is highly active antiretroviral therapy (haart) in pregnancy protective against maternal mortality?...
TRANSCRIPT

Is Highly Active Antiretroviral Therapy (HAART) in pregnancy protective against maternal mortality? Results from a large
DREAM cohort in Malawi and Mozambique
Presented by Leonardo Palombi (Italy).
G. Liotta1 , S. Mancinelli1 , E. Gennaro 2, P. Scarcella1, K. Saines-Nielsen3,N. Abdul Magid4, P. Germano5, J. Haswell6, G. Guidotti7 , E.Buonomo1,
A. Doro Altan1, L. Palombi1 , MC. Marazzi8
1 University of Tor Vergata, Public Health Dept., Rome. Italy. 2 University “G. D’Annunzio” , Chieti, Italy 3 UCLA. Pediatrics. Los Angeles, USA4 DREAM Program. Community of S. Egidio, Maputo, Mozambique. 5 DREAM Program. Community of S. Egidio, Rome, Italy. 6 DREAM Program. Community of S. Egidio, Blantyre, Malawi. 7 Pisa University, Italy8 LUMSA University, Rome, Italy
TUAB0201TUAB0201

Background
HIV-1 infection is a major cause of maternal mortality (MM) in resource-limited settings.
The DREAM (Drug Resource Enhancement against AIDS and Malnutrition) Program routinely offers triple ART from pregnancy throughout the postpartum period regardless of maternal CD4 cell count for prevention of mother to child HIV transmission (PMTCT) at clinical centers in sub-saharan Africa.
We evaluated the uptake of triple ART and maternal mortality in our PMTCT cohort at our centers in Malawi and Mozambique.

In prior cohort studies, our group reported a significant association between duration of triple ART in pregnancy and maternal mortality

Methods Study design: Retrospective cohort Records for all HIV+ pregnant women accessing 16
DREAM centers in Malawi and Mozambique from 6/2002 to 6/2010 were reviewed. • Group 1: Women starting triple ART during pre-
natal care, n = 8169.• Group 2: Pregnant women on established triple
ART for their own health, n = 1981 Women identified in pregnancy were offered NVP-
based triple ART at 14 weeks (if required for health) or 25 weeks gestation until 6 months for PMTCT.

Specific Aims
1. To determine risk factors associated with maternal mortality during pregnancy until 6 weeks postpartum.
2. To compare mortality, ART uptake, loss to follow-up and laboratory parameters between women receiving triple ART for PMTCT and women on established ART during pregnancy.
3. To evaluate mortality in women beyond the immediate postpartum period according to duration of triple ART exposure with adjustment for time in medical care and duration of antenatal ART.
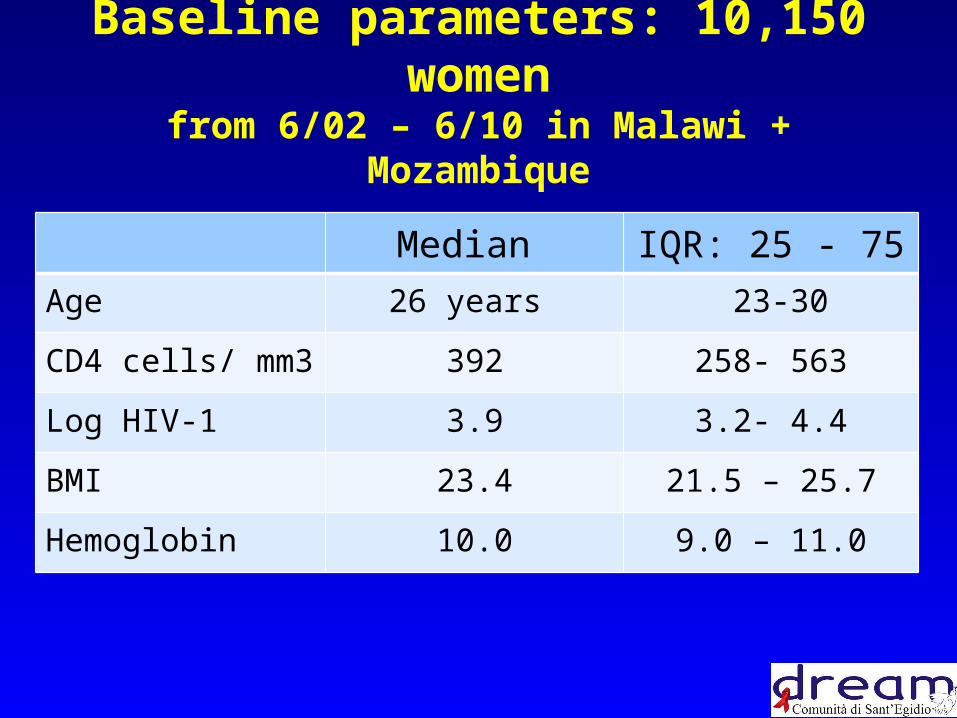
Baseline parameters: 10,150 womenfrom 6/02 – 6/10 in Malawi + Mozambique
Median IQR: 25 - 75
Age 26 years 23-30
CD4 cells/ mm3 392 258- 563
Log HIV-1 3.9 3.2- 4.4
BMI 23.4 21.5 – 25.7
Hemoglobin 10.0 9.0 – 11.0

Comparison between groups
7
Baseline parameters Group 1N=8,169
Mean (SD)
Group 2N =1,982
Mean (SD)
p
HAART in days 832 (586) 1459 (621) <0.001
CD4 cell count 431 (275) 354 (366) <0.001
Viral load cps/ml 3.6 (1.3) 3.8 (1.5) <0.001
Body Mass Index 23.8 (3.6) 22.0 (3.8) <0.001
Hemoglobin 9.9 (3.4) 10.1 (1.9) 0.26
Refusal/Loss to follow up
9.8 3.9 <0.001
Maternal Mortality 1.1 0.7 0.17

Maternal mortality (MM)
Deaths up to 42 days postpartum: 101 (0.99%)• Group 1 (ART during PMTCT): 87/ 8169 (1.1%)• Group 2 (established ART): 14/1981 (0.7%)• Deaths by CD4 cell count strata:
• < 350 cells/ mm3: 1.3%• > 350 cells/ mm3: 0.7%
• Deaths by triple ART exposure:• < 30 days of antenatal ART: 22/ 991 (2.2%) • > 90 days of antenatal ART: 35/ 5260 (0.7%)
Mozambique MMR 520 (0.52%) Unicef 2009
Malawi MMR 1100 (1.1%) Unicef 2009

Multivariate analysis of Maternal Mortality: logistic regression forward stepwise model
Outcome variable Maternal Death
OR 95% CL p
Shorter ART exposure 1.72 1.36 – 2.17 0.001
Baseline Viral Load 0.84 0.61 – 1.17 0.3
Baseline CD4 count 1.57 1.19 – 2.06 < 0.001
Baseline Hemoglobin 1.42 1.06– 1.91 0.02
Baseline BMI 1.98 1.47 – 2.64 < 0.001
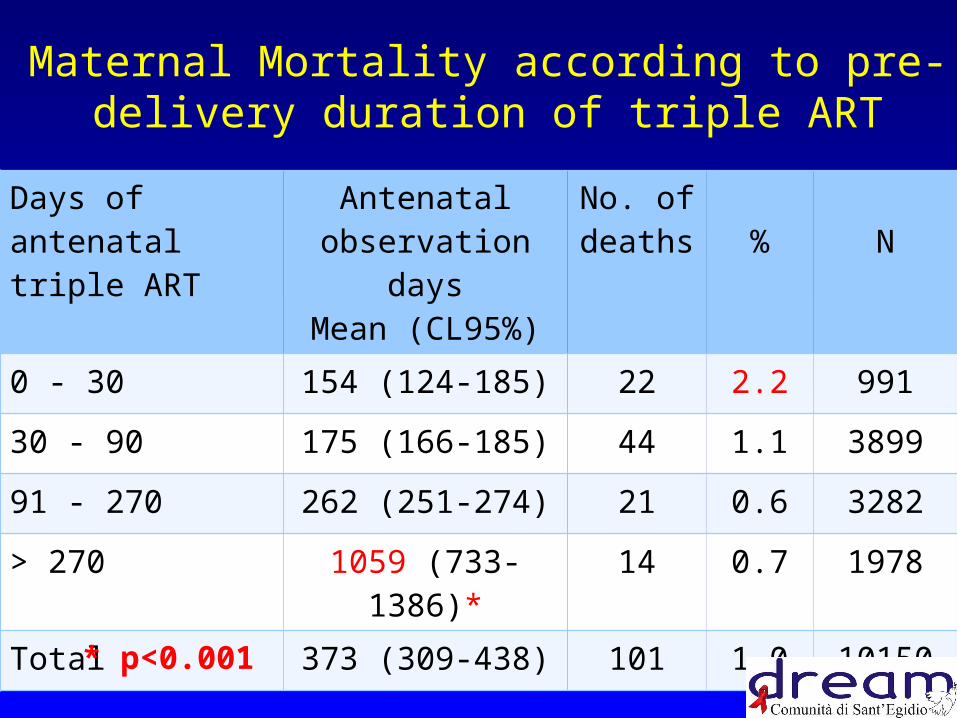
Maternal Mortality according to pre-delivery duration of triple ART
10
Days of antenatal triple ART
Antenatal observation daysMean (CL95%)
No. of deaths % N
0 - 30 154 (124-185) 22 2.2 991
30 - 90 175 (166-185) 44 1.1 3899
91 - 270 262 (251-274) 21 0.6 3282
> 270 1059 (733-1386)* 14 0.7 1978
Total 373 (309-438) 101 1.0 10150
* p<0.001

Mortality in women over 4 years adjusted for observation time under triple ART
Days of antenatal triple ART
Total Observation time - days
mean (CL95%)
No. of deaths % N
0-30 779 (738-821) 45 4.5 991
31-90 817 (799-835) 92 2.4 3899
91-270 865 (846-885) 58 1.8 3282
> 270 1459 (1431-1486) 39 2.0 1978
Total 954 (942-967) 234 2.3 10150

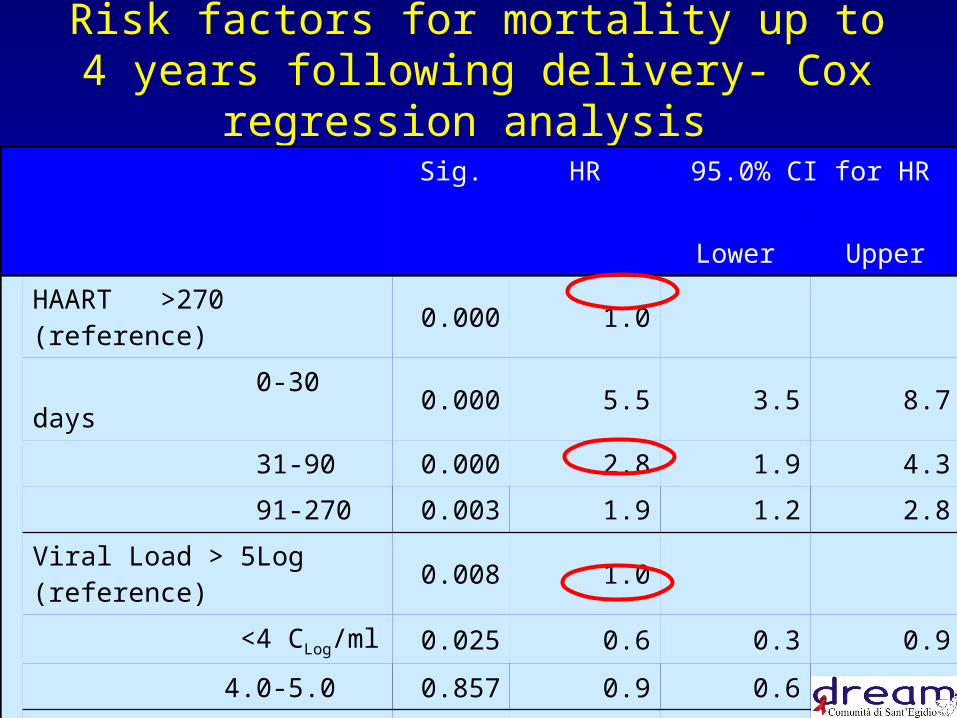
Risk factors for mortality up to 4 years following delivery- Cox regression analysis
13
Sig. HR 95.0% CI for HR
Lower Upper
HAART >270 (reference) 0.000 1.0
0-30 days 0.000 5.5 3.5 8.7
31-90 0.000 2.8 1.9 4.3
91-270 0.003 1.9 1.2 2.8
Viral Load > 5Log (reference) 0.008 1.0
<4 CLog/ml 0.025 0.6 0.3 0.9
4.0-5.0 0.857 0.9 0.6 1.4
CD4 >350 0.000 1.0
< 200 Cell/microL 0.000 1.9 1.3 2.7
200-350 0.001 1.7 1.2 2.3

Sig. HR 95.0% CI for HR
Lower Upper
BMI >20.0 (reference) 0.000 1.0
<18.5 0.000 2.7 1.8 4.0
18.5-20.0 0.012 1.7 1.1 2.5
Hb >10.0 (reference) 0.019 1.0
8.0-10.0 gr/100cc 0.017 1.6 1.1 2.4
<8.0 0.016 1.4 1.1 1.9
Risk factors for mortality up to 4 years following delivery- Cox regression analysis
(2)

CD4
Viral Load

Hemoglobin
BMI

Summary Maternal mortality is significantly associated with
duration of triple ART, baseline CD4 cell count, BMI and degree of anemia.
Women on established ART while pregnant, women with CD4 counts > 350 and women with > 90 days of antenatal ART have a lower mortality risk during pregnancy and immediate postpartum period.
Women with extended antenatal ART (beyond 270 days prior to delivery) have the highest four year survival benefit.

Summary Provision of triple ART in pregnancy carries a significant
survival benefit and renders maternal mortality in HIV+ women (1%) equivalent or lower to population country-wide statistics and significantly lower than the mortality of untreated HIV+ mothers in Malawi (6%). Lettow 2011
Women who present to medical care late in pregnancy and receive shorter courses of triple ART (lowest triple ART exposure in absolute terms) have a higher mortality risk over 4 years.
18

Conclusions Triple ART for PMTCT purposes have a
significant impact on maternal mortality in resource-limited settings.
Extended triple ART carries a survival benefit extensive to all women regardless of CD4 cell strata.
Provision of triple ART to all HIV-infected women significantly decreases the risk of maternal death in the short and medium term. 19

Grazie!
• To our patients• To our sponsors• To the members of
the DREAM Program