is intensity of therapy important? dr derick t wade, professor in neurological rehabilitation,...
TRANSCRIPT
Is intensity of therapy important?
Dr Derick T Wade,Professor in Neurological
Rehabilitation,Oxford Centre for Enablement,
Windmill Road, OXFORD OX3 7HE, UKTel: +44-(0)1865-737310Fax: +44-(0)1865-737309
email: [email protected]
Why is intensity of therapy important?
• The questionsdoes rehabilitation alter outcome?how is rehabilitation quantified for
funding?• are translated into
is outcome related to the face-to-face time therapist spends with patient?
how much face-to-face time did the therapist spend treating the patient?
National Clinical Guideline for Stroke. 3rd edition. 2008Recommendation 3.13.1.A
• “Patients should undergo as much therapy appropriate to their needs as they are willing and able to tolerate, and in the early stages they should receive a minimum of 45 minutes daily of each therapy that is required. “
• No comment on time involved in any other activities.

Content
• What is rehabilitation?A process with many activities
• What is therapy (treatment)?Any actions undertaken by therapists?Process of teaching a patient an
activity?• What improves patient function?
Time with the therapist practicing?Other therapist actions/other practice?
Messages
• Rehabilitation is not synonymous with therapy.
• Therapists (team members) do much more than give therapy.
• Rehabilitation process should be separated from rehabilitation actions:In research studies and papersWhen considering resources needed and
used
The clinical context
• Patients present with problems they and/or others attribute to a health problem
• Rehabilitation works within a holistic, biopsychosocial model of illness
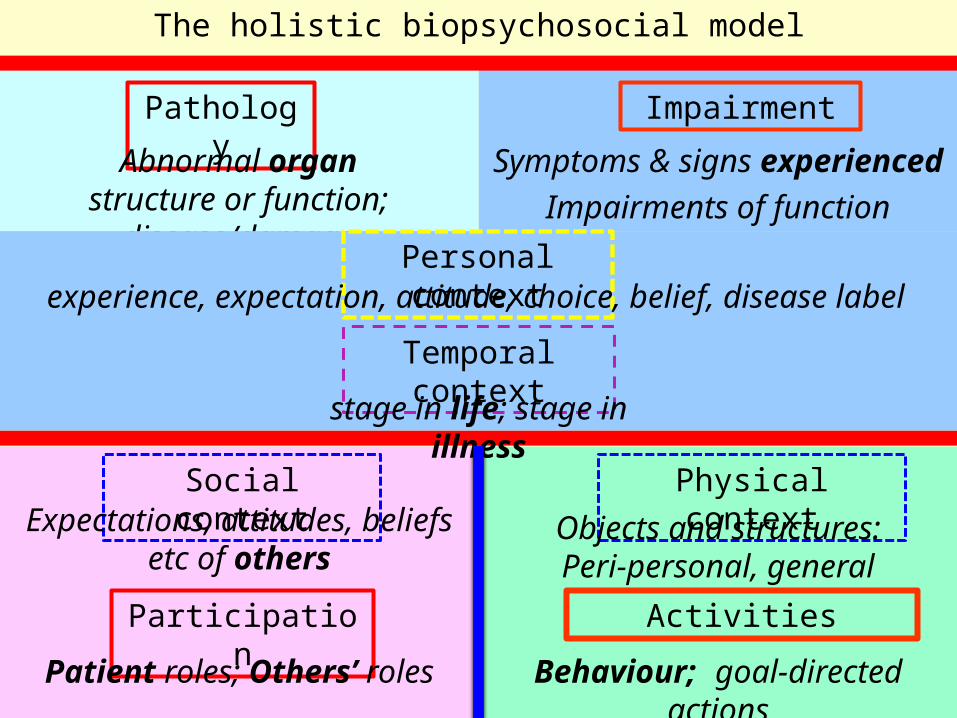
The holistic biopsychosocial model
Pathology
Abnormal organ structure or function;
disease/damage
Impairment
Symptoms & signs experienced
Impairments of function implied
Personal contextexperience, expectation, attitude, choice, belief,
disease label
Social contextExpectations, attitudes,
beliefs etc of others
Participation
Patient roles; Others’ roles
Physical context
Activities
Behaviour; goal-directed actions
Temporal contextstage in life; stage in illness
Objects and structures:Peri-personal, general
Illness is:• A dysfunction within the whole
systemTraditionally secondary to pathology
(disease of or damage to an organ)Better considered secondary to
mismatch between:• Demands made on person
– By self (personal context), others (social context), environment (physical context), bodily needs
• Capacity of person to maintain equilibrium in face of challenge
– Capacity depends on whole person, and may be limited in many ways
Medical approach
• Medical care only considers pathologyDiagnosis, cure/control, implications
• Uses bio-medical model of illnessLow attention to anything other than
• Pathology• Somatic distress (pain)
Not recognise other causes of illnessNot consider importance of other factors
Patient goals usually to:
• Achieve satisfying social functions (roles)
• Be able to respond and adapt to changing circumstances
• Be free of emotional and somatic distress
• Only concerned with pathology as one of many potential limiting factors
Rehabilitation approach
• Considers whole situationUsing holistic biopsychosocial illness
model• Focuses on
Patient problems, wishes etcPatient activities in first instance
• Goals are toOptimise social function, adaptabilityMinimise distress
Rehabilitation: a problem-solving process
Assessment to• Formulate (analyse and understand)
situation• Determine potential goals and actions
Goal setting to:• Set short-, medium-, and log-term goals
Actions to:• Preserve patient safety and well-being
(support)• Change situation (‘treatments’)
Evaluation to:• Compare change against goals• Identify new/altered goals/actions
Rehabilitation activities
• Collecting & analysing data (assessment)
• Setting goals• Undertaking actions to
Preserve safety and well-beingAlter situation / achieve goals
• Monitor change and progressTransfer care to another service/patient
Rehabilitation actions - 1• Two types:
support: care needed to maintain status quo• Often the major resource
treatment: action expected to affect change
• Treatments are multi-focal (i.e. affect several factors)Any level:
• pathology, impairment, activities, participation
Any context:• personal, physical, social
Rehabilitation actions - 2
• Often prolonged in time• May be mutually inter-dependent
Botulinum toxin and physiotherapyGiving wheelchair, adapting house and
teaching how to use it• Order also may be important• Difficult to describe, classify or
quantifyBest by domain of WHO ICF?

Treatment - pathology• Pathology
Changing neural plasticity/ability to learn• Increase – e.g. ?use amphetamines• Decrease – e.g. avoid sedative and similar
drugsAltering neural structures
• Nerve growth factors etc
• Also noteMaking the correct diagnosis (or new
one)Giving or monitoring disease therapy
Treatment - impairment
• Treatments to alter impairments:Directly (e.g. pain, spasticity)Indirectly
• Prostheses (replace a lost part/skill)• Orthoses (support a lost skill)
• Note: impairments may change:SpontaneouslySecondary to other treatments
• E.g. increased activity
Treatment - activities
• To be discussed
Treatment - participation
• Most interventions to alter social participation are at other levelsAn important supra-ordinal goal for
other goals• May:
Help patient to adjust social role expectations
Help person move out of sick role (being a patient)
Role change is important“The kindest thing anyone could have done for me would have been to look me square in the eye and say this clearly:
‘Reynolds Price is dead. Who will you be now? Who can you be now and how can you get there double-time’”
Reynolds Price. A whole new life: an illness and a healing.
New York Atheneum 1994
Treatment – physical context
• This involves altering the physical environmentPeri-personal (clothing, small aids etc)Personal (wheelchairs etc)Within home (adaptations to stairs etc)Within other personal settings (e.g. workplace)Further afield (public transport etc)
Treatment – social context
• May wish to act on/alter attitudes, expectations, behaviours etc of: Personal others (family, friends, work
colleagues)Others met (e.g. healthcare staff)
• Also consider:Broader societal attitudesLaws, rights, responsibilitiesCulture of organisations & systems
Treatment – personal context
• May try to alter or influence:Expectations, beliefs, attitudesSelf-efficacy, confidence etc
• Involves actions such as:Providing informationCognitive behavioural therapyContacting others in similar situation
System analysis
• Rehabilitation is a systemInvolves many peopleIncludes many activitiesAll spread over time
• SystemsAre, to an extent, resistant to
‘degradation’• Someone else can take over
But deliver an outcome that is greater than the sum of its parts
At present
• We know that the system works• We do not know
Which bits are criticalThe extent to which one intervention
may affect the outcome of another
Changing activities
• Depends primarily on learning:How to manage despite impairment
• Techniques• Strategies etc
Use of equipmentWhat is possibleHow to overcome difficulties
Activities (behaviour)
• Learning (a behaviour) depends upon:Having adequate skills (i.e. impairment
not too severe)Goals (motivation of patient)
• Patient must see connection to wanted goalsConfidence/self efficacy
• Belief it can be achievedFeedback on performance

Change in behaviour
• This depends primarily on amount of practice:Repetition (100s of times)May secondarily alter impairment
• E.g. increase fitness or strength
• AlsoFeedback on achievement/failureVarying situations
Roles of rehabilitation team
• To optimise environmentStructuresPeople (staff, family)
• To ensure practice isSafeAppropriate to abilities
• To teach techniques, strategies etc• To encourage practice in different
settings

In a session a therapist may:
Facilitate practice of an activity directlyProvide support (emotional, social)Provide information, new knowledgePractice other activities, indirectly
• E.g. communicationTeach how to use equipmentTeach others how to facilitate safe
practiceOrganise actions by othersCollect data, set goals etc

Rehabilitation
• Helps patientSelect the most appropriate destinationTravel along best pathwayMake best selection at any junctions
• Makes pathwaysafe & easy to followHave emergency support network
Therapists
• Participate in team toSelect and adjust pathwayProvide safety net
• Help patientOvercome particular obstacles safelyNavigate parts of the pathwayLearn new skills to manage travel

Conclusions• Intensity of practice determines
extent of change in specific, targeted activitiesTherapist has a role in facilitating safe
practice• Therapists have many other tasks
beyond practice• Relationship between rehabilitation
input and outcome unclearExtent (quantity) probably low
relationshipExpertise (quality) likely to be more
related
Is intensity of therapy important?
Dr Derick T Wade,Professor in Neurological
Rehabilitation,Oxford Centre for Enablement,
Windmill Road, OXFORD OX3 7HE, UKTel: +44-(0)1865-737310Fax: +44-(0)1865-737309
email: [email protected]
*** NOT VERY IMPORTANT ***