ischemia at the crossroads?
TRANSCRIPT

Cardiovascular Drugs and Therapy 2: 9-15, 1988 © Kluwer Academic Publishers. Printed in the U.S.A.
ISCHEMIA AT THE CROSSROADS?
SUMMARY. Understanding and control l ing the consequences of myocardial i schemia requires us to acknowledge that w e are deal ing wi th a complex, dynamic, and highly variable process. The severity and progression of ischemic injury is not solely determined by the extent of oxygen deprivation, but by many other factors, including the accumulat ion of toxic metabolites. It may not be justified to assume that in- jury to the myocyte necessari ly determines the survival of the organ; other components, such as the endothel ium and the conduct ing system, may play a crucial role. Many factors can influence the severity and evolution of iscbemic injury, perhaps the most important being the extent of residual (or collateral) f low to the affected tissue. I f the ischemia is relat ively mild, then the myocardium may survive for some long time, and drugs and other interventions may be used to further extend this period. However, reperfusion and the es- tabl ishment of an adequate level of coronary flow is an ab- solute prerequisite for sustained t issue survival. The more severe the ischemia, the earlier must be the reperfusion. However, reperfusion of previously ischemic t i ssue is not without hazard, and it may precipitate potential ly lethal events such as arrhythmias. Reperfusion may possibly result in the death of cells that were potential ly viable in the moments before reflow was established, and there is good evidence that manipulat ion of reperfusion conditions may accelerate and possibly enhance recovery from ischemia. Much remains to be learned about myocardial ischemia and reperfusion, and in doing this we should perhaps put some of the older, yet wel l established, concepts behind us.
KEY WORDS. ischemia, myocardial metabolism, oxygen im- balance, reperfusion
The Imbalance of Supply And Demand: A Variable and Dynamic Condition
Through their choice of the title: "Modern concepts in the Trea tment of Ischemic Hear t Disease," the editors of this symposium have, perhaps by intention, cast a shadow of doubt over the validity of some established concepts relating to myocardial ischemia and its man- agement. Have our concepts changed, should they change, or could it be that we are rediscovering old problems, but this t ime giving them glamorous and credible names? The "stunned cardiologist" [1] of the 1980s has suffered from a barrage of terminology (silent ischemia, stuttering ischemia, stunned myo- cardium, jeopardized myocardium, blighted myocar- dium, hibernating myocardium, condemned myocar- dium, infarct size limitation, and reperfusion- induced injury, to mention a few) and might be forgiven for seeking reassurance and/or clarification.
David J. Hearse The Rayne Institute St Thomas' Hospital London, UK
Fortunately, the cornerstone of our understanding of ischemia remains more or less intact [2, 3]. Thus, ischemia involves an imbalance between the needs of the tissue for life-sustaining blood and the ability of the vasculature to respond adequately to this require- ment. In recent years, however, our understanding of the origins of this condition has become considerably more sophisticated. I t is now acknowledged tha t it is not invariably a simple thrombotic occlusion that generates a zone of potentially lethal ischemia, but other factors, such as progressive atherosclerosis, plaque rupture, coronary spasm, and adverse drug-in- duced effects may also initiate the event. From this broader view of ischemia and its origins, has come the important recognition that the phenomenon is by no means static, but is highly dynamic (such that the af- fected tissue may experience waves of ischemia of varying severity and duration) and involves other im- portant factors in addition to supply and demand. As will be discussed later, the impairment of washout may be of equal or even greater importance than defi- cient supply.
Since traditional definitions of ischemia can be flawed on at least two counts, (1) they fail to take ac- count of the dynamic state of the cell and the ischemic process and (2) they fail to take account of problems of washout as well as supply, it may be appropriate to define ischemia as it will be used in the context of this article.
Ischemia arises when coronary blood flow is inade- quate to maintain steady state metabolism. This will result in the development of an anerobic metabolism and an intensifying metabolic imbalance, a condition that will be expressed in a number or ways, e.g., the
Address for correspondence and reprint requests: Professor D. J. Hearse, Director of Cardiovascular Research, The Rayne Institute, St. Thomas' Hospital, London, SE1 7EH, United Kingdom

10 Hearse
net degradation of the adenine nucleotide pool, which occurs as a consequence of an inadequate ability to support a sufficient rate of ATP turnover. Unless halted, this deterioration of metabolic imbalance will culminate in cell death, a process that may be has- tened by failure of washout as well as supply.
Ischemia and the Extent of Flow Reduction
Although ischemia is often studied in its most severe form (sustained zero coronary flow), it is important to appreciate that total cessation or even marked de- ficiency of blood flow is not a prerequisite for myocar- dial ischemia. Tissue can suffer significant ischemic injury when blood flow is still substantial. It can even be argued that tissue with a relatively normal blood flow at rest may become ischemic under conditions of increased demand for energy because of the failure of its vasculature to respond sufficiently to the require- ment of an increased cardiac output.
The Crucial Role of the Collateral Circulation
Besides our appreciation tha t the occlusion of a cor- onary artery need not be total for ischemia to ensue (such that myocardial infarction might well occur in the absence of occlusion [4]), we have also realized that even in the presence of complete obstruction, cor- onary flow may not fall to zero. Collateral flow [5-9] from cardiac and extracardiac sources can provide a lifeline to tissue that has been deprived of its more usual source of blood [6, 10]. Thus in dogs [6] and many patients with coronary artery disease, extensive artery-to-artery anastomoses are found between ad- joining coronary perfusion beds. These collateral con- nections may supply the equivalent of a third or more of the normal blood flow and may explain why, despite t ransmural zones of ischemia, only a subendocardial infarct may develop. Thus, residual or collateral flow to an ischemic zone may well result in the salvage of a significant amount of tissue. Younger patients, and species such as the pig [6] and baboon, are normally devoid of collateral vessels, and in them coronary oc- clusion results in the rapid development of a fully transmural infarct. The guinea pig [6] is blessed with a totally collateralized coronary anatomy and as such is naturally resistant to ischemia and infarction.
The Severity of Ischemia
Although the extent of residual or collateral flow to an area of regional ischemia is the single most important determinant of the severity of that ischemia, and hence the fate of the tissue, other factors such as heart rate, inotropic state, myocardial oxygen consumption (MVO2), and coexisting diseases such as diabetes mellitus, hypertension, and thyroid disorders all act to reduce or intensify the severity (and hence affect the outcome) of an ischemic episode [10, 11]. Unfor- tunately some of these factors, particularly coexisting disease, are difficult to reproduce in the laboratory, a consideration that has significantly limited our un- derstanding of human myocardial ischemia.
Surprisingly, the crucial relationships between the extent and duration of ischemia and its outcome are rather poorly defined. We know, for example, that myocytes can survive very severe ischemia (zero flow) only for short times (perhaps 30 to 40 minutes) but may survive moderate deprivation of flow lasting several hours. In this connection, we [12, 13] have sug- gested that ischemia be designated tolerable, critical, or lethal. In a dog study [13], we observed that reduc- tions of coronary flow up to approximately 50% had relatively little effect upon the tissue content of high- energy phosphates, even if the reduction in flow was maintained for as long as 2 hours. In this state of toler- able ischemia, tissue energy balance is probably main- tained by a combination of increased oxygen consump- tion per unit flow, reduced contractile performance, and more efficient utilization of substrate (for exam- ple, switching from fat ty acid to glucose utilization). Thus, although contractility may be reduced, tissue in this state should remain free of major metabolic or morphological injury for long or indefinite periods. It should not become infarcted (unless excessively stim- ulated) and thus represents a tolerably but chronically ischemic tissue mass, which may respond well to metabolic or pharmacological interventions designed to make the most of the energy supply/energy demand status. Drugs such as coronary vasodilators might af- ford real protection to such tissue with a sustained im- provement in, or even a normalization of, contrac- tile performance.
In our second proposed state of ischemic injury, reductions in flow of about 60%-80% in the dog heart caused the tissue energy levels to decline. The greater the reduction in flow, or the greater the duration of ischemia, the greater was the energy imbalance. In this phase, designated as critical ischemia [12], small changes in flow or in duration of ischemia could result in large changes in tissue energy status. It is possible that tissue in this state could be appropriately iden-

Ischemia at the Crossroads? 11
tiffed as jeopardized, since a small improvement in flow might halt the t ime-dependent decline of energy reserves and so push the tissue over the survival threshold into the time-independent state of tolerable ischemia. It may well be that in this relatively narrow range of reduced flow, pharmacological interventions could be used to delay very considerably the onset of irreversible injury. However, the time dependency of this phase necessitates that interventions be made as soon after the onset of ischemia as possible, perhaps within 1 to 2 hours with say an 80% reduction, and 6 to 12 hours with say a 60% reduction, in flow.
The third state of injury, designated as lethal ischemia, is associated with reductions in flow of greater than 80%. In this phase, we suggested that in- jury develops very rapidly and has a complex time dependency such that tissue energy stores fall rapidly with time up to about 45 minutes. With increasing durations of ischemia, residual energy supplies decline more slowly, since the tissue is probably in a state of ir- reversible injury. Thus, with reductions in flow of 80% or more, it is probably more appropriate to call the tissue condemned rather than jeopardized since, without early reperfusion, there is little likelihood of the tissue being salvaged by any pharmacological intervention.
The preceding discussion on the relationship be- tween the degree of flow deprivation and the nature and extent of injury was derived from, and applies to, the dog. However, it would not seem unreasonable to apply the principle to other species, particularly when correction is made for heart rate and metabolic rate. In recent studies [14] with the rat heart, we have drawn very similar conclusions about a critical threshold for flow, below which tissue survival is unlikely.
Is The Myocyte the Victim?
Traditionally the myocyte, as the quantitatively dom- inant cell type of the heart, has been assumed to be the primary victim of ischemia, and thus its response is the determinant of organ survival or death. As our un- derstanding of ischemia and its consequences im- proves, it is becoming clear that other cell types (for example, the conducting tissue, the vascular smooth muscle, and, particularly, the vascular endothelium) can play an important role in determining the out- come of an episode of myocardial ischemia. Some of these cell types, for example, the endothelium, may exhibit significant functional impairment after very brief periods of ischemia. There is little doubt that a
better understanding of the consequences of myocar- dial ischemia in these relatively neglected cells could contribute much to the effective management of ischemia and myocardial infarction.
The Natural History of Myocardial Ischemia
In the past quarter of a century we have accumulated a detailed understanding of the metabolic, functional, electrophysiological, and morphological consequences of myocardial ischemia. It is not the objective of this article to discuss these changes in detail; there are, however, many excellent reviews on the subject (see, for example, reference 16). As illustrated by the scheme shown in Figure 1, myocardial ischemia is an enormously complex process, the characteristics of which differ greatly from heart to heart and even from cell to cell within the same heart [15]. Indeed, the heterogeneity of ischemia-induced cellular changes is probably a very important determinant of the outcome of an ischemic episode. As shown in Figure 1, the tem- poral characteristics of ischemia are also of great im- portance. Thus, ischemia initiates a progression of cellular changes, which, unless halted, may continue to cell death and tissue necrosis, as has been so clearly described by Jennings and colleagues [2, 3]. Initially, ischemia-induced injury is fully reversible, such that the restoration of adequate flow results in an almost immediate recovery of normal metabolic and contrac- tile activity. As the duration or severity of the ischemia increases, restoration may not result in the immediate return of normal contractile function, al- though in time a full recovery is observed. This slow recovery may take several hours or days and represents the phenomenon of the stunned myocardium. Beyond a certain point, injury becomes so severe that reperfu- sion cannot restore function. In this state of irrevers- ible injury, reperfusion may even trigger an extension or acceleration of damage.
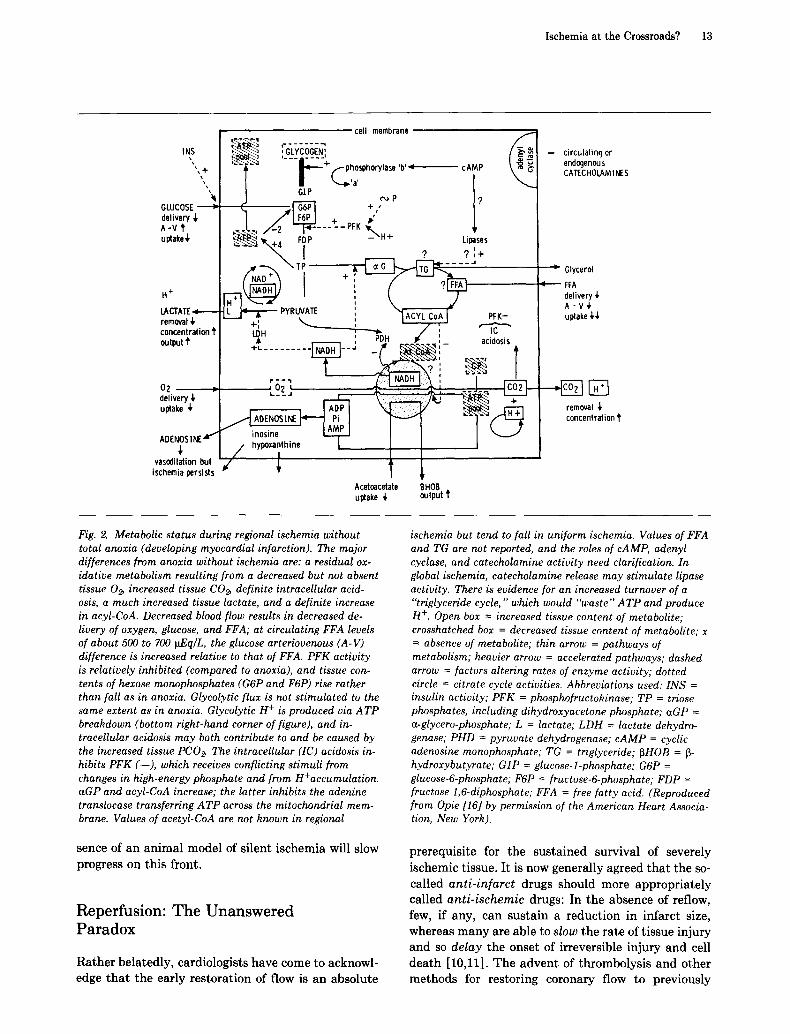
Detailed studies of many aspects of the changes shown in Figure 1 have been reported, and consider- able information is now available concerning the molecular characteristics of ischemic injury. An ex- cellent example is illustrated in Figure 2, which is re- produced from the work of Opie [16] and shows the ef- fect of ischemia upon substrate utilization and energy metabolism. Detailed knowledge such as this is in- valuable in improving our ability to manage myocar- dial ischemia.

12 Hearse
Ah ?
ONSET OF SEVERE ISCHEMIA
Reduced oxygen avadabdlly Disturbances of transmembrane =onlc balance Utilization of dissolved oxygen Cyanos~s ReduCllOn of mdocnondrlal aChvlty and ox~dat,ve metabolism Reduced ATP produchon Reducllon of creaflrte phosphafe stores Reduchon ot 4mphtude and durahon of acDon polenhal Leakage of potassium ST segment changes Accumulation Ot SOdBUm and chlonde ions Catecholamlne release Stimulation of adenyl cyclase Cyclic AMP medlaleo actwat~on of phosphorylase Stlmulallon of glycogenolysls Net UllllZatlon O~ high energy phosphates Accumulat=on of protons cardon dioxide and inorgamc phosphate StlmWatlon of phosphoftuclokmase acllvlty Increase of glycolytE flux Oevelopmenl ot intracellular aCldOSpS Reduction or blockage of ml{ocnonor,a~ electron transport Repression of fatty acid o, ldahon Utdlzatlon Of glyCOgen Leakage ol Jnorganfc phosphate AccumuFatlon of NADH Increasect laclale dehyOrogenase and ,, glycerophosphale dehydrogenase actlw/y Accumulahon of laclate and.-giycerodnosphate Leakage of laclale AccumuJat~bn of laity acyl CoA denvalwes Depletion of creatme phosphate LeaKage of adenosine ~nosJne an~ olher melaPohtes VasodllalJon Inhibition of adenine nucleohde Iransferase activity Possible Stlmulahon of trlglycerlde synlheSls and degradation Increasing cellular actdOSlS Repression of phospnotruclok,nase and glyceraldenycte-3-phosphale
dehydrogenase actlvlly Slowing of glycolytlc flux Increasing depletion of energy slores Cell swelhng Increase tn cytoplasmic *omzed cabcrum content Leakage of magnesium cons PosslbJe exhaustion ol glycogen reserves Development of mltochondr~al damage Inhiot~lon of glycolysJs Severe reduction of ATP Minor ultraslructural changes e g mJtochondrlal swelling Poss,ble onset of contracture
ONSET OF IRREVERSIBLE DAMAGE ~
Lysosomal cPanges and actlvahon Ot hydroJases Actwahon of hDOproceln hpases Increaslrg cellular edema LOSS of mltOChOndnal resplralory control Nonspeclhc eleCtrocard=ographlc changes Ultrastructural changes in mtlOChondna and myoflbnls Complele depletion of energy reserves MetaOollc dlsrupllOn Loss of mltochondnal components Leakage of macromolecules to mterstdlal space and lymph Sevece ullraslruclural damage and membrane detenOtahon Cellular dlSrUplaon Extens*ve enzyme leakage DISrUptIOn Of mltochondrla DlSlnlegtallon of myolibnls Disruption ol cell membranes Cellular autolysis
CELL DEATH AND TISSUE NECROSIS
Fig. 1. Cellular consequences of myocardial ischemia. Some of the cellular events thought to occur following the onset of severe myocardial ischemia. This figure, which is highly spec- ulative, is not intended to convey that the events occur in a strict sequence or in the exact order listed. The progression of changes is a dynamic process, and only the onset of some changes is indicated. In general, the early changes are revers- ible, but, with increasing durations of ischemia, they progress to irreversible damage. The exact point of the transition is unknown. (Reproduced with permission from Hearse et hi. [15].)
Ischemia: Not Simply a Problem of Supply
Thus far, this article has concentrated on the problems of inadequate supply . However, as pointed out by Jen- nings [2], it must be stressed that a reduction in blood
supply also limits the r emova l from the tissue of potentially toxic intermediates (for example, protons and lactate). Some investigators convincingly argue [17] that it is the inadequate w a s h o u t and accumula- tion of such intermediates (the formation of some, for instance lactate, actually being enhanced in ischemia) that might have greater responsibility for inducing severe metabolic injury and possibly even for the onset of irreversible injury [14]. Certainly, the absence of washout can be used to explain many of the differences between the myocardial consequences of ischemia and hypoxia, the latter being characterized by normal, or even enhanced, coronary flow rates.
Silent Ischemia: Making Itself Heard
As stated so appropriately by Beamish in a recent issue of the C a n a d i a n Journa l of Cardiology [18] s i lent ischemia is making itself heard. To date, the seductive naming of the phenomenon has probably done more to establish silent ischemia as a discrete condition than have all of the clinical and experi- mental studies of its manifestation. Despite the recent rash of articles and symposia devoted to this topic, this writer remains confused and cautious. Unanswered questions abound: Is "silent" ischemia a precursor of "noisy" ischemia--a mild, asymptomatic ischemia that may deteriorate to angina? Therefore, is silent ischemia more a reflection of our inadequacy to detect the symptoms of mild ischemia than an indication of the occurrence of a distinct disease process? What is the prognosis for silent ischemia and how is this prog- nosis altered for those patients currently being "treated" for the condition? It could be argued that at present it is the electrocardiogram that is being treated rather than the disease. While normalization of an abnormal ECG is most likely a reflection of cellular benefit, we should not forget the limitations of the interpretation of the ECG and the fact that drugs can alter the nature of the ECG without necessarily improving the metabolism of the cell. It is not that many years ago that changes in ST segments lead to false optimism about our ability to reduce the size of an evolving infarct.
It would seem that the greatest barrier to our better understanding of silent ischemia (and hence our abil- ity to put it in an appropriate clinical perspective and monitor the efficacy of its treatment) is the absence of a highly sensitive and reliable marker of mild ischemic injury. Perhaps the time has come for biochemists to re-examine the characteristics of mild ischemic injury in the hope that better markers than lactate or po- tassium leakage can be found. Unfortunately, the ab-
Ischemia at the Crossroads? 13
I cell membrane
",+ I ~'~'~ I'~'--":-:+fphosprlorylase'b ' , cAMP \ ~ ~'1
• GIP I GLUCOSE ~ ,~ _ I-~'~ + ,' l delivery ,i, I . ~ I F6P I + p ~' I A-V i' ~ZL.~ / / - 2 ~ . . . . . FK ~ . uptake& ~ ~K.+4 FDP - H+ Lipases
LACTATE: L I~ & PYRUVATE ' , ~ . . - ~ . , IACYLCoAI PFK- removal ,~ .~., ~ , ~
concentrationi' LI)H ~ i ~ . . . . / i " IC to ~' & ~ , rup • ., acidosis ou.ut + . . . . . . . . . . INAOH]__ = _(, ~ : -
• I I
o, , ,"6;~ L-I NA°H I~. ', I r6~Tb_ de'ii.ry ~, =_~-~ ~ = +-I
ADE N~,S ~ ~ ? 0 I~ 'a='' inosine ~ . ~
vasodilation but =/6 I ; I ischemia persists " • l
Acetoacetate BHOB . uptake ~. output ?
-- circulating or endogenous CATECHOLAM I NE S
Glycerol • FFA
delivery ~, /~ -V,~ uptake ~
removal ~. concentration 't
Fig. 2. Metabolic status during regional ischemia without total anoxia (developing myocardial infarction). The major differences from anoxia without ischemia are: a residual ox- idative metabolism resulting from a decreased but not absent tissue 02, increased tissue CO~ definite intracellular acid- osis, a much increased tissue lactate, and a definite increase in acyl-CoA. Decreased blood flow results in decreased de- livery of oxygen, glucose, and FFA; at circulating FFA levels of about 500 to 700 ~Eq/L, the glucose arteriovenous (A-V) difference is increased relative to that of FFA. P F K activity is relatively inhibited (compared to anoxia), and tissue con- tents of hexose monophosphates (G6P and F6P) rise rather than fall as in anoxia. Glycolytic f lux is not st imulated to the same extent as in anoxia. Glycolytic H + is produced via A T P breakdown (bottom right-hand corner of figure), and in- tracellular acidosis may both contribute to and be caused by the increased tissue PCO~ The intraceUular (IC) acidosis in- hibits PFK (--), which receives conflicting stimuli from changes in high-energy phosphate and from H+ accumulation. aGP and acyl-CoA increase; the latter inhibits the adenine translocase transferring A T P across the mitochondrial mem- brane. Values of acetyl-CoA are not known in regional
sence of an animal model of silent ischemia will slow progress on this front.
Reperfusion: The Unanswered Paradox
Rather belatedly, cardiologists have come to acknowl- edge tha t the early restoration of flow is an absolute
ischemia but tend to fall in uniform ischemia. Values of FFA and TG are not reported, and the roles of cAMP, adenyl cyclase, and catecholamine activity need clarification. In global ischemia, catecholamine release may stimulate lipase activity. There is evidence for an increased turnover of a "triglyceride cycle," which would "waste" A T P and produce H +. Open box = increased tissue content of metabolite; crosshatched box = decreased tissue content of metabolite; x = absence of metabolite; thin arrow = pathways of metabolism; heavier arrow = accelerated pathways; dashed arrow = factors altering rates of enzyme activity; dotted circle = citrate cycle activities. Abbreviations used: INS = insulin activity; PFK = phosphofructokinase; TP = triose phosphates, including dihydroxyacetone phosphate; aGP = a-glycero-phosphate; L = lactate; LDH = lactate dehydro- genase; PHD = pyruvate dehydrogenase; cAMP = cyclic adenosine monophosphate; TG = triglyceride; ~HOB = ~- hydroxybutyrate; GIP = glucose-l-phosphate; G6P = glucose-6-phosphate; F6P = fructose-6-phosphate; FDP = fructose 1,6-diphosphate; FFA = free fa t ty acid. (Reproduced from Opie [16] by permission of the American Heart Associa- tion, New York).
prerequisite for the sustained survival of severely ischemic tissue. It is now generally agreed tha t the so- called a n t i - i n f a r c t drugs should more appropriately called a n t i - i s c h e m i c drugs: In the absence of reflow, few, if any, can sustain a reduction in infarct size, whereas many are able to s low the rate of tissue injury and so d e l a y the onset of irreversible injury and cell death [10,11]. The advent of thrombolysis and other methods for restoring coronary flow to previously

14 Hearse
ischemic tissue has put much emphasis on reperfusion and its consequences.
In 1973 we reported [19] the first of a series of, studies [19-21] demonstrating that after a period of severe oxygen deprivation, reperfusion or reoxygena- tion can result in a sudden increase in the leakage of enzymes, the onset of contracture, and the rapid development of severe ultrastructural injury. This ef- fect(the oxygen paradox) [20] was directly attr ibuted to the readmission of molecular oxygen which, as has been shown, can produce highly cytotoxic free radicals [22]. During the past 10 years, reper fus ion- induced in jury has become the focus of much interest and debate, but its exact nature remains elusive and con- troversial [11]. While there is no doubt that reperfu- sion can precipitate the occurrence or expression of a number of unfavorable events, it is possible that these events would have occurred in any case, but perhaps over a longer t ime scale. Thus, some would argue that reperfusion-induced injury is merely the acceleration, by reperfusion, of the expression of pre-existing injury and tha t severe reperfusion-induced injury only occurs in tissue that is already in a state of irreversible injury. Certainly, there is evidence in support of this view- point; however, others argue that reperfusion, when carried out inappropriately, can cause damage in its own right. This view is supported by studies [23-26] which show tha t modification of reperfusion con- ditions (for example, transient reduction of calcium or selective provision of substrates) can enhance re- covery, an effect that has been attr ibuted to overcom- ing reperfusion-induced injury. At the present time, arguments for reperfusion-induced injury are limited by the failure of most studies to distinguish between the ability of an intervention (for example, selective provision of glutamate during early reperfusion) to en- hance the absolute ex t en t of recovery as opposed to improving the rate of recovery [11, 27]. The phenome- non of the stunned myocardium requires that such dis- tinctions be made days after the onset of reperfusion, rather than only minutes or hours later.
While we await definitive evidence that reperfusion can induce irreversible injury in cells that were in a state of reversible injury in the seconds before reperfu- sion, it seems that, on balance, reperfusion-induced injury is likely to be a real phenomenon. One aspect of reperfusion tha t undoubtedly exists and is potentially detrimental is the ability of reflow to trigger severe arrhythmias [28, 29]. Reperfusion-induced ventricular fibrillation frequently occurs within seconds of the onset of reperfusion in both experimental and clinical circumstances, and better understanding of the events responsible for the induction of these serious threaten-
ing arrhythmias should assist greatly in our ability to control the ravages of ischemia.
Future Developments
Undoubtedly we will learn more about the mech- anisms underlying ischemia, reperfusion, and their control. Undoubtedly, too, new and imaginative names will continue to be coined for both new and old phenomena, and it is to be hoped that we will see major (and much needed) developments in our ability to detec t and quan t i f y ischemic injury. Armed with improved methodologies, a continuously expanding knowledge of molecular mechanisms of injury, and a more critical approach to the interpretation of experi- mental and clinical studies, in the 1990s we should witness some major advances in our ability to manage myocardial ischemia in its many forms.
References
1. Donato L. Concluding remarks: The "stunned"cardiologist. Can J. Cardiol 1986;Suppl A:260-262.
2. Jennings RB. Myocardial ischemia--observations, defini- tions and speculations. J Mol Cell Cardiol 1970;1:345-349.
3. Jennings RB, Ganote CE, Reimer KA. Ischemic tissue in- jury. Am J Pathol 1975;81:179-198.
4. Harris P. A theory concerning the course of events in angina and myocardial infarction. Eur J Cardiol 1975;3:157-163.
5. Newman PE. The coronary collateral circulation: Deter- mination and functional significance in ischemic heart dis- ease. Am Heart J 1981;102:431-445.
6. Schaper W. Experimental infarcts and the microcirculation. In: Hearse DJ, Yellon DM, eds. Therapeutic Approaches to Myocardial Infarct Size Limitation. New York: Raven Press, 1984:79-90.
7. Brazier J, Hottentott C, Buckberg GD. Noncoronary col- lateral myocardial blood flow. Annals Thorac Surg 1975; 19:426-435.
8. Schaper W. The Collateral Circulation of the Heart. Am- sterdam: North Holland, 1971.
9. Bloor CM. Functional significance of the coronary collateral circulation. Am J Pathol 1974;76:562-587.
10. Hearse D J, Yellon DM. eds. Therapeutic Approaches to Myocardial Infarct Size Limitation. New York: Raven Press, 1984.
11. Hearse DJ. The protection of the ischemic myocardium: Surgical success versus clinical failure. Prog Cardiovasc Dis, in press.
12. Hearse DJ. Critical distinctions in the modification of myocardial cell injury. In: Opie LH, ed. Calcium An- tagonists and Cardiovascular Disease. New York: Raven Press, 1984:129-145.
13. Hearse DJ, Crome R, Yellon DM, Wyse RK. Metabolic and flow correlates of myocardial ischemia. Cardiovasc Res 1983;17:452-458.

Ischemia at the Crossroads? 15
14. Maxwell MP, Hearse DJ, Yellon DM. The critical threshold of residual flow for cell survival during ischaemia studies in the isolated rat heart. J Molec Cell Cardiol, in press.
15. Hearse DJ, Braimbridge MV, Jynge P. Protection of the Ischemic Myocardium: Cardioplegia. New York: Raven Press, 1981.
16. Opie LH. Effects of regional ischemia on metabolism of glucose and fatty acids. Relative rates of aerobic and anaerobic energy production during myocardial infarction and comparison with effects of anoxia. Circ Res 1976;38 (Suppl 1}:52-74.
17. Neely JR, Grotyohann LW. Role of glycolytic products in damage to ischemic myocardium. Circ Res 1984;55:816- 824.
18. Beamish RE. Silent ischemia makes itself heard. Canad J Cardiol 1987;3:51.
19. Hearse DJ, Humphrey SM, Chain EB. Abrupt reoxygena- tion of the anoxic potassium arrested perfused rat heart: A study of myocardial enzyme release. J Molec Cell Cardiol 1973;5:395-407.
20. Hearse DJ, Humphrey SM, Bullock GR. The oxygen para- dox and the calcium paradox: Two facets of the same prob- lem? J Molec Cell Cardiol 1978;10:641-668.
21. Hearse DJ. Reperfusion of the ischemic myocardium. J Molec Cell Cardiol 1977;9:605-616.
22. Hess ML, Manson NH. Molecular oxygen: Friend or foe? J Mol Cell Cardiol 1984;16:969-985.
23. Rau EE, Shine K, Gervais A, Douglas AM, Amos EC. En- hanced mechanical recovery of anoxic and ischemic myocar- dium by amino acid perfusion. Am JPhysiol 1979;236:H873- H879.
24. Follette DM, Buckberg GD. Reducing post-ischemic myo- cardial injury during cardiopulmonary bypass by temporary initial reperfusate modification. Clin Res 1984;4:25-28.
25. Allen BS, Okamoto F, Buckberg GD et al. Studies of con- trolled reperfusion after ischemia IX. Reperfusate composi- tion: Benefits of marked hypocalcemia and diltiazem on regional recovery. J Thorac Cardiovasc Surg 1986;92:564- 572.
26. Kuroda H, Ishigiero S, Mori T. Optimal calcium concentra- tion in the initial reperfusate for post ischemic myocardial performance (calcium concentration during reperfusion). J Molec Cell Cardiol 1986;18:625-633.
27. Hearse DJ, Yellon DM. Why are we still in doubt about in- farct size limitation? The experimentalist's viewpoint. In: Hearse DJ, Yellon DM, eds. Therapeutic Approaches to Myocardial Infarct Size Limitation. New York: Raven Press, 1984:17-41.
28. Hearse DJ, Manning AS, Janse MJ, eds. Life Threatening Arrhythmias in Ischemia and Infarction. New York: Raven Press, 1987.
29. Manning AS, Hearse DJ. Reperfusion-induced arrhyth- mias: Mechanisms and prevention. J Molec Cell Cardiol 1984;16:497-518.