isokitenic 2015: clinical practice guidelines for muscle injury fc barcelona and aspetar experience
TRANSCRIPT

http://muscletechnetwork.org/proyectos-id/publicaciones/
Clinical Practice Guidelines for Muscle Injury FC Barcelona and Aspetar Experience

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
Clinical Practice Guidelines for Muscle Injury
(2015)
Clinical Practice Guidelines for Muscle Injury
(2009)
Clinical Practice Guidelines for Muscle Injury
(2018)
Previous consensus (2017)

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
(UCL Elite Club Injury Study. 2013/2014 Season Report)

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
11%
28%
61%
43%
25%
32%
0%
10%
20%
30%
40%
50%
60%
70%
Quadriceps Adductor Hamstrings
FCB 1st Team FCB Academy

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
1. Muscle injuries classification 2. Diagnosis and management of muscular injuries 3. Algorithm of rehabilitation 4. Return to play criteria 5. Primary and secondary prevention
CONTENTS

http://muscletechnetwork.org/proyectos-id/publicaciones/
1. Muscle injuries classification 2. Diagnosis and management of muscular injuries 3. Algorithm of rehabilitation 4. Return to play criteria 5. Primary and secondary prevention

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
Introduction
Several grading and classification systems for muscle injuries have been published; indeed, no validated classification system exists.
To classify is necessary to have good epidemiological data, which are basic to find the best therapeutic option for an injury/disease.

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
The Proposal
In our opinion the evaluation of the amount of extracellular matrix (ECM) damaged and its impact in force generation and transmission is a key factor in muscle injuries clinics and prognosis; therefore the classification is based on this concept. We reviewed the literature to select and organize the knowledge about muscle injuries:
• Mechanism. • Clinic and imaging prognosis factors. • Injury relation with MTJ and amount of connective tissue damage (indeed of
function). • Evolution in time.
We organize and resume this concept in a 4 letters acronym structure.
XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
Muscle Injury Mechanism
1. Direct injuries:
• Located in the place of the trauma.
• Size is not well correlated with the functional impairment.
• Different clinical evolution than indirect injuries (shorter time loss).
2. Indirect muscle injuries are located close to a myotendinous junction (MTJ).
Lee J, Mitchell A, and Healy J. Imaging of muscle injury in the elite athlete. British Journal of Radiology 85: 1173-1185, 2012. Thorsson O, Lilja B, Nilsson P, and Westlin N. Immediate external compression in the management of an acute muscle injury. Scandinavian journal of medicine & science in sports 7: 182-190, 1997. Garrett WE, Nikolaou PK, Ribbeck BM, Glisson RR, and Seaber AV. The effect of muscle architecture on the biomechanical failure properties of skeletal muscle under passive extension. The American journal of sports medicine 16: 7-12, 1988.

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
Extracellular matrix (ECM) damage
The evaluation of the amount/severity of ECM damaged is done trough:
• Muscle injury relation with the MTJ (proximal or distal).
• % CSA as reflection of the amount of ECM damaged.
• If there is tendon gap/retraction/loss of tension.
Structure and function of the skeletal muscle extracellular matrix Gillies 2011

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
Mechanism
Location
Grade
Re-injury

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
Mechanism
It describes the mechanism of injury, which could be a direct blow or an indirect strain:
• Direct injuries D
• Indirect injuries I
XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
Location for direct injuries
Is a lowercase regarding the anatomical location:
• p injuries located at the proximal third.
• m injuries located at the middle third.
• d injuries located at the distal third.

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
Is a capital letter followed or not by a lowercase regarding the Location.
It describes the connective tissue damage location, tendon or MTJ.
• J for the injuries at the MTJ.
• T for injuries affecting the tendon: gap/retraction/loss of tension.
• After the T and J, as a sub-index, the proximal and distal location must be specified (p for proximal and d for the distal).
Location for indirect injuries

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
Grade
Is a number from 0 to 4 regarding the Grade. MRI based, is referred to the percentage of the cross sectional area (% CSA) of the affected muscle to total muscle belly, in the axial plane where the injury is greater.
The affected area is considered where there is a hyper-signal change on fat suppressed/STIR images.
If more than one muscle is injured, the muscle with the greater area of signal abnormality or architectural distortion will be considered the primary site of injury and the grading criteria will be taken for that particular muscle.

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
0 Grade 0: clinical suspicion of muscle injury with negative MRI.
1 Grade 1: ≤10% of CSA.
2 Grade 2: 11-25% of CSA.
3 Grade 3: 26-49% of CSA.
4 Grade 4: ≥50% of CSA.
In the future, the architectural distortion, more than the oedema, should be the key in the imaging evaluation to grade the muscle injuries.
Grade

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
Re-injury
Describes the injury chronology (first episode or a re-injury):
R0: First episode, R1: First re-injury, R2: Second re-injury… and so on.
A re-injury is defined as “injury of the same type and at the same site as an index injury occurring no more than 2 months after a player’s return to full participation from the index injury” (Ekstrand 2011). If during the two months period after the RTP a new injury occur in the same muscle but in a different location, it will also considered a re-injury.

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
Proposal
Mechanism Location Grade Reinjury
D (direct)
D p proximal third direct injury
0 negative MRI
1 < 10 % CSA
2 11 – 25 % CSA
3 26 – 49 % CSA
4 >50 % CSA
R0 1st episode
R1 1st reinjury
R2 2nd reinjury
..and so on.
D m medial third direct injury
D d distal third direct injury
I (indirect)
I T p proximal tendon injury
I T d distal tendon injury
I J p proximal MTJ injury
I J d distal MTJ injury

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
• Direct injury located in A: – D-p-G-R0
• Direct injury located in B: – D-m-G-R0
• Direct injury located in C: – D-d-G-R0
A
B
C
Direct Injuries Codification

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
Indirect Injuries Codification
• Indirect injury located in A: – I-Jp-G-R
• Indirect injury located in B: – I-Jd-G-R
A
B

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
Indirect Injuries Codification
• I-Tp-G-R

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
Take home messages
1. With an acronym we can describe the injury.
2. Allows communication among medical staff.
3. Flexible structure allowing to incorporate
knowledge in the future.
4. Easy to use.

http://muscletechnetwork.org/proyectos-id/publicaciones/
1. Muscle injuries classification 2. Diagnosis and management of muscular injuries 3. Algorithm of rehabilitation 4. Return to play criteria 5. Primary and secondary prevention

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
Background
• Most of them are treated non-surgically. • The clinical appearance is not always clear. • Determining the optimal treatment for any injury can be difficult. NEEDS • Detailed history of the patient and about the injury mechanism. • Careful examination. • Imaging diagnosis:
– Magnetic Resonance Imaging (MRI) – Ultrasound (US)
Critical goal is to differentiate between those patients with injuries possibly requiring surgical treatment from patients with non-surgical injuries

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
1. Appropriate history
About the player:
• Similar injuries before?
• Medications?
• Susceptibility…
About the mechanism of injury:
• Direct blow or indirect strain?
• During training or competition?
• When and how did it start?
About the initial progress:
• Stop or continue playing?
• Normal walk without pain?
XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
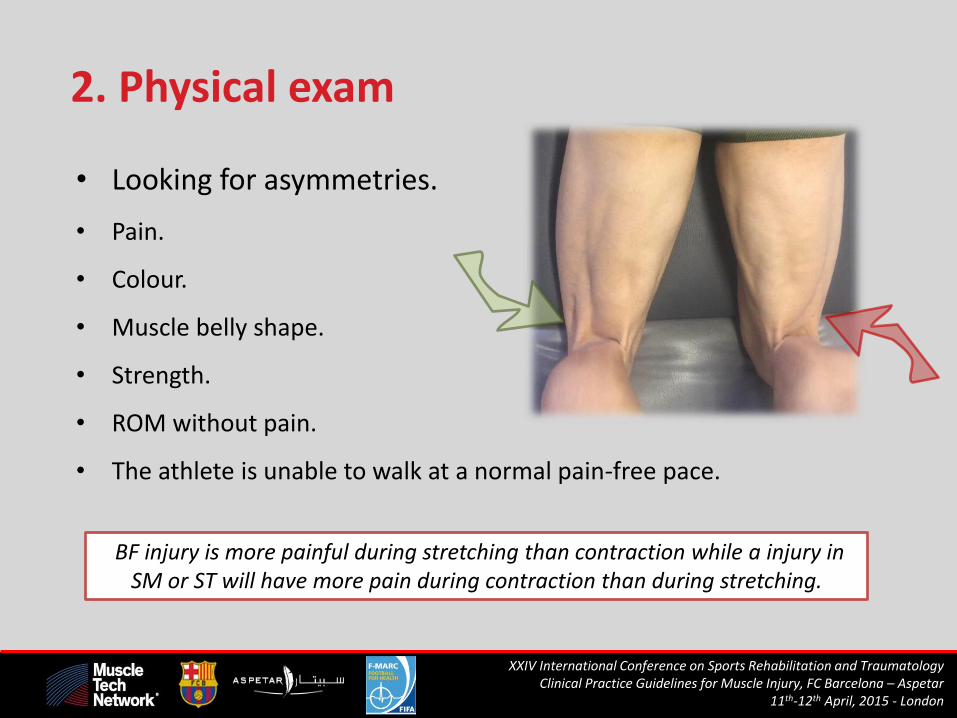
2. Physical exam
• Looking for asymmetries.
• Pain.
• Colour.
• Muscle belly shape.
• Strength.
• ROM without pain.
• The athlete is unable to walk at a normal pain-free pace.
BF injury is more painful during stretching than contraction while a injury in SM or ST will have more pain during contraction than during stretching.

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
3. Imaging of muscle injury
RX: limited value unless an avulsion fracture with bony fragment or apophyseal fracture in a skeletally immature individual.
US and MRI:
• Describe the location (which muscle and tissue).
• The lesion size.
• The lesion nature (oedema/haemorrhage) by echotexture (US) and signal intensity (MRI)

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
3.1 Ultrasound
• Cost effective.
• Radiologist experience dependent.
• Dynamic and interactive process allowing “echopalpation” of painful areas.
• It enables progress monitoring.
• Guide the evacuation of fluid collections.
• Useful in distal hamstring injuries (superficial anatomy).
XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
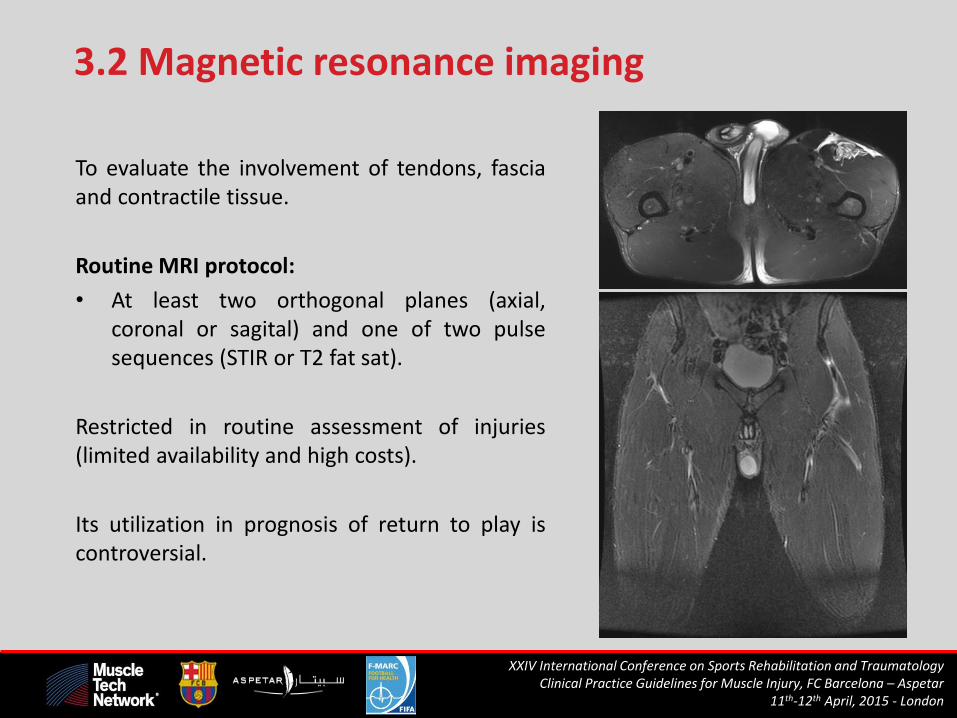
3.2 Magnetic resonance imaging
To evaluate the involvement of tendons, fascia and contractile tissue.
Routine MRI protocol:
• At least two orthogonal planes (axial, coronal or sagital) and one of two pulse sequences (STIR or T2 fat sat).
Restricted in routine assessment of injuries (limited availability and high costs).
Its utilization in prognosis of return to play is controversial.

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
MRI advantages
• To measure the size of injury (length and cross-sectional area).
• Proximal hamstring injuries.
• Groin area injuries.
• In assessing the tendon retraction (preoperative planning).
• In highlighting subtle edema.
• In evaluating injuries to deep injuries of muscles.
• In evaluating injuries when a previous injury is present (residual scarring).
• Discovering concomitant image.

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
Management of a muscle injury
Clinical history
Physical exam
US MRI Treatment
Immediate X X
Could be made
anytime
Rest
Ice
Compression
Elevation
Analgesia
12 hours X X
24 hours X X
48 hours X X
Functional tests
1st week Monitorize
players feelings
X x To evaluate how the
progression of loads are assumed
Rehabilitation
progressive protocol
Weekly X X
Return to play X X
For follow-up the functional recovery and sometimes to help to decide return to play: • Muscle: Tensiomyography, electromyography and strength tests. • Player: GPS, HR and self administered scales during and after the rehabilitation sessions on field.
Initial acute phase
Subacute and
functional phase

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
Muscle injuries heal conservatively.
Indications of surgical treatment: • Total or subtotal (>50%) rupture with few or no agonist muscles.
• Large intramuscular hematoma.
• Complains of chronic pain (>4-6 months) in a previously injured muscle, specially with ROM deficit.
Surgical procedure: • Anatomic restoration when is possible.
• Surgical release of adhesions from the nerve and scar debridement in
chronic cases.
Surgical treatment

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
Bony avulsions
Muscle Part of muscle Tendon Treatment
Quadriceps
Proximal ASIS AIIS
Conservative; unless > 2cm
Distal Patellar avulsion Surgical; (except non
displaced)
Hamstrings
Proximal Ischial tuberosity Gap < 2cm conservative
Bigger gaps: surgical
Distal All (rare)
( BF – SM ) Surgical reattachment must
be considered

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
Proximal
Distal
Rectus femoris

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
Tendon-bone disinsertions
Muscle Localization Tendon Treatment
Quadriceps
Rectus Femoris Proximal
Direct head Surgical reattachment
Indirect head Little gap: Conservative
Big gap: Surgical
Direct + Indirect head Surgical
Hamstrings Proximal
Biceps Femoris Long Head and/or Semitendinosus
Surgical
Semimembranosus
Conservative. If there were symptoms after 4 months: surgical reattachment
must be considered
Distal All (rare) Surgical reattachment must be
considered

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
Ischion
Central Tendon

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
Reattached

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
Comin J, Malliaras P, Baquie P, Barbour T, Connell D. Return to competitive play after hamstring injuries involving disruption of the central tendon. Am J Sports Med. 2013;41(1):111-115.
• Long recovery times.
• Worse results.
• Biceps femoris 45%
• Recurrent injury.
New surgical indication for hamstring?

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
DISTAL
PROXIMAL
Proximal end of Central
Tendon
Distal end of Central
Tendon

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
Central Tendon injuries
MTJ injuries, when the Central Rectus Femoris Tendon or Common Hamstring Tendon is involved with loss of tension
Muscle Part of muscle-tendon Treatment
Quadriceps and
Hamstrings
< 2 cm from bone insertion Reattachment to the
bone and reduce tension at MTJ
More than 2 cm to bone insertion
Surgical treatment: Anatomical repair
with minimally invasive approach

http://muscletechnetwork.org/proyectos-id/publicaciones/
Take home messages
1. Clinical expertise in muscle injuries.
2. US and MRI to confirm diagnosis.
3. Surgical treatment when tendon is
affected.

http://muscletechnetwork.org/proyectos-id/publicaciones/
1. Muscle injuries classification 2. Diagnosis and management of muscular injuries 3. Algorithm of rehabilitation 4. Return to play criteria 5. Primary and secondary prevention

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
Rehabilitation Program
LITERATURE
SEARCH
SCIENTIFIC
EVIDENCE
EXPERIENCE
CONSENSUS
THERAPEUTIC

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
Proposal of Algorithm
ALLPARAMETERSDIAGNOSTICPHASE ACUTEPHASE SUBACUTEPHASE FUNCTIONALPHASE PHASETORTP
ANDCONTROLTEST DESTRUCTION REPAIR REMODELLING
PHISICALTHERAPY X X X
MANUALTHERAPY X X X
FLEXIBILITYANDROM X X X
PROPIOCEPTION X X X
CORE X X X
NEUROM-CONTROL X X X X
STRENGTH X X X
POWER X X
FITNESS X X
PAIN/FATIGUE X X X X X
BIOMECANICHS X X X X X
IMAGE X X X X X

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
Progression of exercises

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
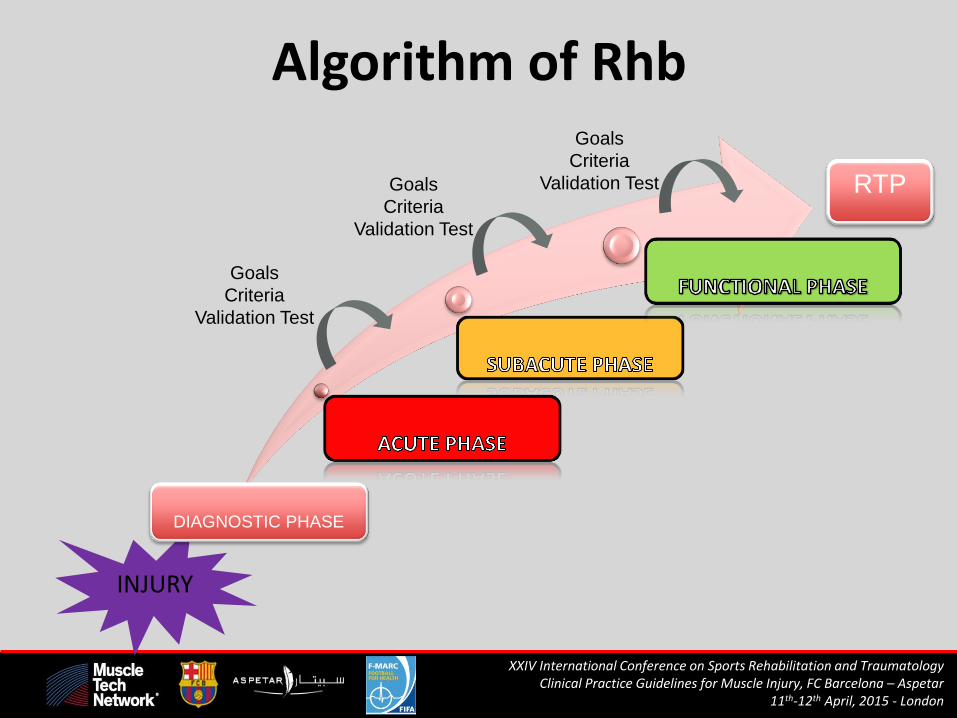
Algorithm of Rhb
INJURY
DIAGNOSTIC PHASE
Goals
Criteria
Validation Test
Goals
Criteria
Validation Test
Goals
Criteria
Validation Test RTP

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
Diagnostic Phase
Kerkhoffs, G., et al. "Diagnosis and prognosis of acute hamstring injuries in athletes”, 2013
INJURY !!!
• PRESSION (together with Cryotherapy 3 times/day, every 3h, 20’-30’)
• REST (sporting, not total)
• ICE (Cryotherapy 3 times/day, every 3h., 20’-30’)
• IMMOBILISATION (3-4 days, every 3-4h, between 15-20’)
• ELEVATION (upper the heart level and different positions)
• ANAMNESIS (Injury analysis, antecedents,...)
• COMPLEMENTARY PROOFS (RN, ECO, ...)
• GENERAL TESTS (Assessment muscular, articular,...)
• SPECIFIC TESTS (types of pain, localisation, function)
• PSICOLOGIC SUPPORT OF PLAYER
• DIFFERENTIAL DIAGNOSTIC
• FINAL DIAGNOSTIC

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
Algorithm of Rhb
INJURY
DIAGNOSTIC PHASE
Goals
Criteria
Validation Test
Goals
Criteria
Validation Test
Goals
Criteria
Validation Test
RTP

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
Acute Phase

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
Goals and Criteria
Acute Phase
- NO PAIN or discomfort during exercises
- During exercises to maintain neutral spine in static position to Bosu or Board
- To work from Low to Moderate Intensity
- Isometric knee flexion 15º, decubitus prono (ISOM)/(CONC)/(ECC)
- Work with flexion knee to 45° and hip 0°>50% (CKC) / (OKC)
- Uninjured leg (dynamometer or similar 50%.)
- (SBET) with 30º Flexion Knee +(SLS) +(ESH) <70 avoiding pain
- Walk/Run to treadmill until 70% -3% (ESH) decrease
CKC: Close Kinetic Chain, OKC: Open Kinetic Chain, ISOM: Isometric, CONC: Concentric, ECC: Eccentric, ROM: Range of Motion; ESH
(Elongation Stress on Hamstrings.). DST: (Deep squat test). SLS: Single leg squat. RPT: Runner post test. AKET: Active Knee Ext Test:

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
Algorithm of Rhb
INJURY
DIAGNOSTIC PHASE
Goals
Criteria
Validation Test
Goals
Criteria
Validation Test
Goals
Criteria
Validation Test RTP

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
Subacute Phase

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
Goals and Criteria
Subacute Phase
- NO PAIN or discomfort during exercises.
- Not tilting the pelvis or flattening the spine during dynamic exercises
- To work from Moderate to High Intensity
- Isometric knee flexion strength decubitus supine knee flexion 25°
- hip flexion 45°, less than 10% asymmetry (OKC)/(CKC)
- Work uninjured leg (dynamometer or similar 70%.)
- Isometric hip extension strength, knee 0º, Hip 70º less than 10%
- (ESH) Stretch < 70 +(SLS) +(DST) painless
- Start Walking on the treadmill to <8 km/h 5% (ESH)
CKC: Close Kinetic Chain, OKC: Open Kinetic Chain, ISOM: Isometric, CONC: Concentric, ECC: Eccentric, ROM: Range of Motion; ESH (Elongation Stress on Hamstrings.). DST: (Deep squat test). SLS: Single leg squat. RPT: Runner post test. AKET: Active Knee Ext Test:

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
Algorithm of Rhb
INJURY
DIAGNOSTIC PHASE
Goals
Criteria
Validation Test
Goals
Criteria
Validation Test
Goals
Criteria
Validation Test RTP

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
Functional Phase

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
Goals and Criteria
Functional Phase
- No PAIN or discomfort during exercises.
- Correct spine control and strength transfer during exercises
- To work from High to Explosive Intensity
- Integrate strength, neuromuscular and proprioceptive work
- Achieved in contralateral leg no asymmetry (dynamometer/encoder 100%)
- Uninjured leg (Encoder or isokinetic 100%.)
- Isokinetic criteria: We should avoid differences higher than 20%
- (RPT)+(AHFT)+(AKET) No asymmetry
- Test of the feed and games
CKC: Close Kinetic Chain, OKC: Open Kinetic Chain, ISOM: Isometric, CONC: Concentric, ECC: Eccentric, ROM: Range of Motion; ESH
(Elongation Stress on Hamstrings.). DST: (Deep squat test). SLS: Single leg squat. RPT: Runner post test. AKET: Active Knee Ext Test:
XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
Algorithm of Rhb
INJURY
DIAGNOSTIC PHASE
Goals
Criteria
Validation Test
Goals
Criteria
Validation Test
Goals
Criteria
Validation Test RTP

Criteria-based progression
Development of an approach
XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
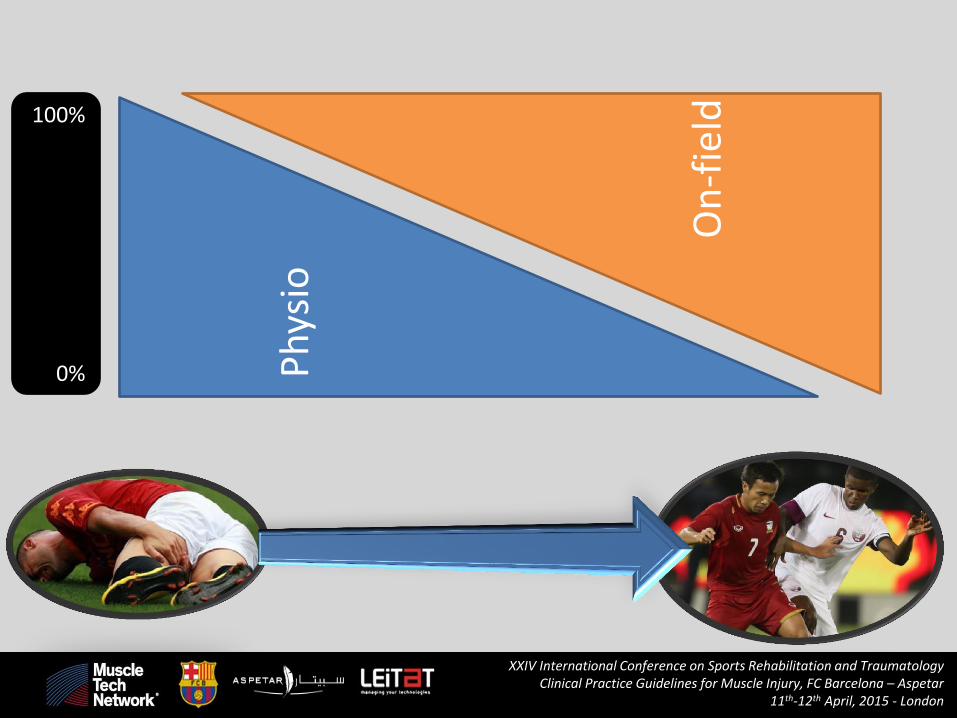
Ph
ysio
On
-fie
ld
100%
0%
XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London

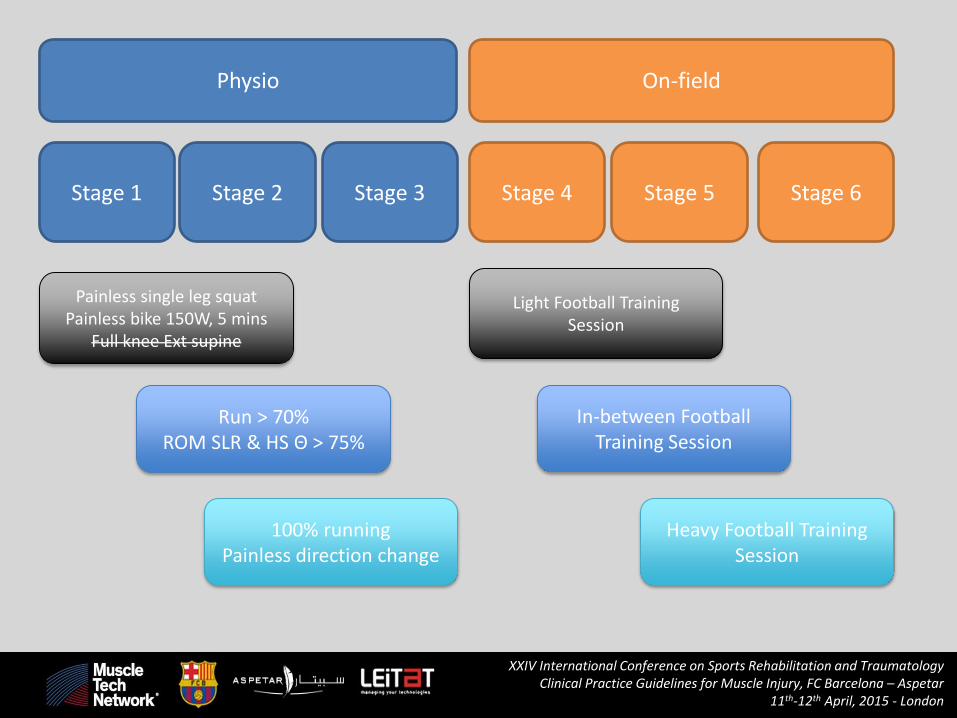
Physio On-field
Stage 1 Stage 2 Stage 3 Stage 4 Stage 5 Stage 6
Painless single leg squat Painless bike 150W, 5 mins
Full knee Ext supine
Run > 70% ROM SLR & HS Θ > 75%
100% running Painless direction change
Light Football Training Session
In-between Football Training Session
Heavy Football Training Session
XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London

Passive movement
Massage – no pain
Massage - discomfort
Active range of motion
Eccentric outer range
Slow run Concentric
through range Fast run
Direction change Isometric – inner
range Eccentric inner
range Outer range
ballistic
Stretching Trunk control Cardio (bike) Isometric outer
range
Painless single leg squat Painless bike 1.5*BW, 5 mins
Full knee Ext supine
Run > 70% ROM SLR & HS Θ > 75%
100% running Painless direction change
XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London

Gait
• Walk
• Jog
• Run
• Triple extension
• Late swing (“A drill”)
• Direction change
4 laps =8 ‘sprints’ X 3 sets ~ 700m 11s → 3.1 s 10% → 100%
3 reps 12s → 9s 60% → 100%
XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
Physio On-field
Stage 1 Stage 2 Stage 3 Stage 4 Stage 5 Stage 6
Painless single leg squat Painless bike 150W, 5 mins
Full knee Ext supine
Run > 70% ROM SLR & HS Θ > 75%
100% running Painless direction change
Light Football Training Session
In-between Football Training Session
Heavy Football Training Session
XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London

0
20
40
60
80
100
120
140Pe
rcen
t o
f u
nin
jure
d s
ide
Inner range
Mid range
Outer range

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London

http://muscletechnetwork.org/proyectos-id/publicaciones/
Take home messages
1. Sequential and progressive.
2. Dynamic and open.
3. Adaptable to each player.
4. Criteria-based progression
5. Based on knowledge and experience.

http://muscletechnetwork.org/proyectos-id/publicaciones/
1. Muscle injuries classification 2. Diagnosis and management of muscular injuries 3. Algorithm of rehabilitation 4. Return to play criteria 5. Primary and secondary prevention

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
The decision-making process of returning an injured or ill player to competition

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
All clear to play
Huge reinjury risk (14-16%)
Criteria
1. Clinical/ Anatomical 2. Imaging (US) 3. Functional
Specific Physical Test
High workloads Highest competition level No reinjury
HEALTHY INDIVIDUALS
WHEN?

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
Return to play
Anatomical, imaging and functional CRITERIA have to be taken into
consideration in order to provide:
Personalized return to play:
1. Injury location/connective tissue involved
2. Anatomical variability
3. Imaging
4. Player position/GPS

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
1. Injury location/connective tissue

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
Return to play
Anatomical, imaging and functional CRITERIA have to be taken into
consideration in order to provide:
Personalized return to play:
1. Injury location/connective tissue involved
2. Anatomical variability
3. Imaging
4. Player position/GPS

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
2. Anatomical variability

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
A
B
C
Semimembranosus injuries

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
Return to play
Anatomical, imaging and functional CRITERIA have to be taken into
consideration in order to provide:
Personalized return to play:
1. Injury location/connective tissue involved
2. Anatomical variability
3. Imaging
4. Player position/GPS

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
3. Imaging

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
Return to play
Anatomical, imaging and functional CRITERIA have to be taken into
consideration in order to provide:
Personalized return to play:
1. Injury location/connective tissue involved
2. Anatomical variability
3. Imaging
4. Player position/GPS

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
4. Player position / GPS

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
COMPARISON THE PLAYERS SAME POSITION WITH THE PLAYER INJURED
0 50 100 150 200 250 300
AVE HSR SET 5PLAYER INJURY
AVE HSR SET 6PLAYER INJURY
AVE SPRINT SET 5PLAYER INJURY
AVE SPRINTS SET 6PLAYER INJURY
AVE ACEL SET 5PLAYER INJURY
AVE ACEL SET 6PLAYER INJURY
AVE DEC SET5PLAYER INJURY
AVE DEC SET 6PLAYER INJURY
AVE VEL.MAX SET5PLAYER INJURY
AVE VEL.MAX SET6PLAYER INJURY
SUMMARY
DA
TA W
EEK
S 5
/6
Comparision with the same players injured player position return to train with the group

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
COMPARED TO OTHER DEFENDER SAME POSITION DURING 60’ MINUTS THE FRIENDLY MATCH
43 51 32 37 38
55
49 45 45 44 42
59
020406080
100120
HIGH ACEL/DESA <3mts/s
DESA.MAXIMES
ACEL.MAXIMES202,91 211,5
290,59 303,53 292,24
542,61
0
100
200
300
400
500
600
DEFENDER 1DEFENDER 2DEFENDER 3DEFENDER 4DEFENDER 5 PLAYERINJURED
HSR DISTANCE <21K/h
15
20 21
15
19
25
0
5
10
15
20
25
30
DEFENDER 1 DEFENDER 2 DEFENDER 3 DEFENDER 4 DEFENDER 5 PLAYERINJURED
TOTAL SPRINTS
29,88 30,38
29,12
34,31
31,68 32,73
26
28
30
32
34
36
DEFENDER 1 DEFENDER 2 DEFENDER 3 DEFENDER 4 DEFENDER 5 PLAYERINJURED
PEAK SPEED MAX

http://muscletechnetwork.org/proyectos-id/publicaciones/
Take home messages
1. Personalized.
2. Technology and experience.
3. Six training sessions.
4. Friendly matches.

http://muscletechnetwork.org/proyectos-id/publicaciones/
1. Muscle injuries classification 2. Diagnosis and management of muscular injuries 3. Algorithm of rehabilitation 4. Return to play criteria 5. Primary and secondary prevention

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
PRIMARY PREVENTION
Prevent the onset of muscle injury
Addressing risk factors Enhancing resistance to exposure
Part of the general football training (all players)

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
Avoidance of a new muscle injury when the player has suffered a previous injury
SECONDARY PREVENTION
Individual, personalized, specific program

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
PREVENTION “SNAPSHOT”
PLAYER INDIVIDUAL STRENGTH PROGRAMME
SQUAD PREVENTION PROGRAMME (SPECIFIC EXERCISES)
WARM UPS PREVENTION OBJECTIVES DAILY
STRENGTH CIRCUITS
FOOTBALL CIRCUITS
GYM
GY
M
P
ITC
H
SMALL GROUPS CIRCUITS
PITCH

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
PRIMARY PREVENTION
PLAYER INDIVIDUAL STRENGTH PROGRAMME
SQUAD PREVENTION PROGRAMME (SPECIFIC EXERCISES) GY
M
strength training
of the hamstringsImage Code Description weight Ser/Repet weight Ser/Repet frequency When
Musculador belt STh1
Eccentric working with variants in dop:
drop with rotation, different angles of
flexion..
body weight or body
weight with 3kg3x4
body weight or body
weight with 3kg 3x8
1x7 (1 competition)/10
days( 2 competitions)
Before or afther 48
hours to match
Splits with body
flexionSTh2 Work hamstring body weight 4 repetitions body weight 8 repetitions once or twice a week
Alternate days ,
never before or
afther to match
Angel STh3 Work hamstring body weight 4 repetitions body weight 8 repetitions once or twice a week
Alternate days ,
never before or
afther to match
minimum stimulus maximum stimulus
StrengthTraining
PrimaryPrevention

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
PRIMARY PREVENTION
DAY -4. ECCENTRIC STRENGHT.
TIRANTE MUSCULADOR
DAY -3. RUNNING
TECHNIQUE & PROPIOCEPTION
EXERCISES.
DAY -2. AGILITY AND
COORDINATION SKILLS.
DAY -1. SPEED REACTION
AND FEET WORK…
PLAYER INDIVIDUAL STRENGTH PROGRAMME
SQUAD PREVENTION PROGRAMME (SPECIFIC EXERCISES) GY
M
WARM UPS PREVENTION OBJECTIVES DAILY
P
ITC
H

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
PRIMARY PREVENTION
DAY -4. ECCENTRIC STRENGHT.
TIRANTE MUSCULADOR

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
PRIMARY PREVENTION
DAY -2. AGILITY AND
COORDINATION SKILLS.

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
PRIMARY PREVENTION
W/O BALL
BOXES
PASSING DRILLS
POSSESSION GAMES
HAMSTRINGS QUADRICEPS
ADDUCTOR MUSCLES CORE STABILITY
COORDINATION / AGILITY PROPIOCEPTION
UPPER BODY
PLAYER INDIVIDUAL STRENGTH PROGRAMME
SQUAD PREVENTION PROGRAMME (SPECIFIC EXERCISES)
WARM UPS PREVENTION OBJECTIVES DAILY
STRENGTH CIRCUITS
GY
M
P
ITC
H
XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
PRIMARY PREVENTION
MULTISTATIONS WITHOUT BALL
MULTISTATIONS WITH BOXES
MULTISTATIONS WITH PASSING
DRILLS
MULTISTATIONS WITH POSSESSION
GAMES
HAMSTRINGS QUADRICEPS
ADDUCTOR MUSCLES CORE STABILITY
COORDINATION / AGILITY PROPIOCEPTION
UPPER BODY
STRENGTH CIRCUITS ON THE FIELD

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
PRIMARY PREVENTION
STRENGTH CIRCUITS ON THE FIELD
MULTISTATIONS WITHOUT BALL
MULTISTATIONS WITH BOXES
MULTISTATIONS WITH PASSING
DRILLS
MULTISTATIONS WITH POSSESSION
GAMES
HAMSTRINGS QUADRICEPS
ADDUCTOR MUSCLES CORE STABILITY
COORDINATION / AGILITY PROPIOCEPTION
UPPER BODY

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
PRIMARY PREVENTION
STRENGTH CIRCUITS ON THE FIELD
MULTISTATIONS WITHOUT BALL
MULTISTATIONS WITH BOXES
MULTISTATIONS WITH PASSING
DRILLS
MULTISTATIONS WITH POSSESSION
GAMES
HAMSTRINGS QUADRICEPS
ADDUCTOR MUSCLES CORE STABILITY
COORDINATION / AGILITY PROPIOCEPTION
UPPER BODY

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
PRIMARY PREVENTION
STRENGTH CIRCUITS ON THE FIELD
MULTISTATIONS WITHOUT BALL
MULTISTATIONS WITH BOXES
MULTISTATIONS WITH PASSING
DRILLS
MULTISTATIONS WITH POSSESSION
GAMES
HAMSTRINGS QUADRICEPS
ADDUCTOR MUSCLES CORE STABILITY
COORDINATION / AGILITY PROPIOCEPTION
UPPER BODY

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
PLAYER INDIVIDUAL STRENGTH PROGRAMME
SQUAD PREVENTION PROGRAMME (SPECIFIC EXERCISES)
WARM UPS PREVENTION OBJECTIVES DAILY
STRENGTH CIRCUITS
FOOTBALL CIRCUITS
GY
M
P
ITC
H
PRIMARY PREVENTION

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
RELATIONSHIP BETWEEN TECHNICAL, TACTICAL AND CONDITIONING CIRCUITS.
CONDITIONING OR PREVENTION STATION PREVIOUS TO THE
FOOTBALL ACTION.
DECISSION MAKING + MULTIPLE OPTIONS
CLOSER TO OUR STYLE OF PLAY/
GAME PLAN
PRIMARY PREVENTION
XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
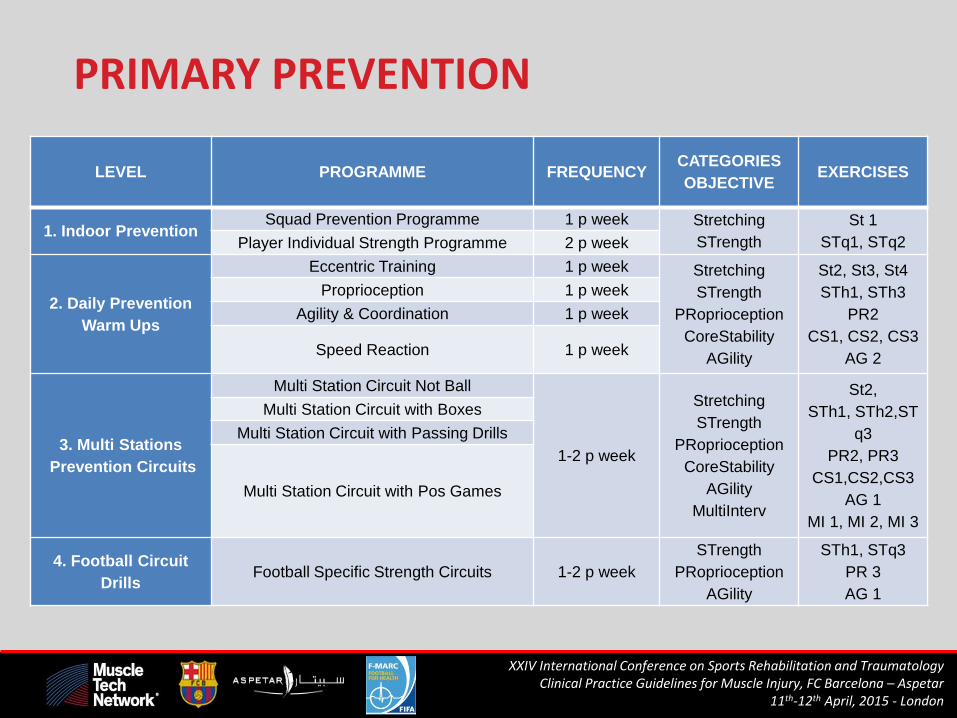
LEVEL
PROGRAMME FREQUENCY CATEGORIES
OBJECTIVE EXERCISES
1. Indoor Prevention Squad Prevention Programme 1 p week Stretching
STrength
St 1
STq1, STq2 Player Individual Strength Programme 2 p week
2. Daily Prevention
Warm Ups
Eccentric Training 1 p week Stretching
STrength
PRoprioception
CoreStability
AGility
St2, St3, St4
STh1, STh3
PR2
CS1, CS2, CS3
AG 2
Proprioception 1 p week
Agility & Coordination 1 p week
Speed Reaction 1 p week
3. Multi Stations
Prevention Circuits
Multi Station Circuit Not Ball
1-2 p week
Stretching
STrength
PRoprioception
CoreStability
AGility
MultiInterv
St2,
STh1, STh2,ST
q3
PR2, PR3
CS1,CS2,CS3
AG 1
MI 1, MI 2, MI 3
Multi Station Circuit with Boxes
Multi Station Circuit with Passing Drills
Multi Station Circuit with Pos Games
4. Football Circuit
Drills Football Specific Strength Circuits 1-2 p week
STrength
PRoprioception
AGility
STh1, STq3
PR 3
AG 1
PRIMARY PREVENTION

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
SECONDARY PREVENTION
PLAYER INDIVIDUAL STRENGTH PROGRAMME
SQUAD PREVENTION PROGRAMME (SPECIFIC EXERCISES)
WARM UPS PREVENTION OBJECTIVES DAILY
STRENGTH CIRCUITS
FOOTBALL CIRCUITS
GYM 2
PITCH 2
GY
M
P
ITC
H

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
Hamstrings injury prevention
Seated eccentric knee flexor stretch (Seated Straight-Leg Raise)
XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
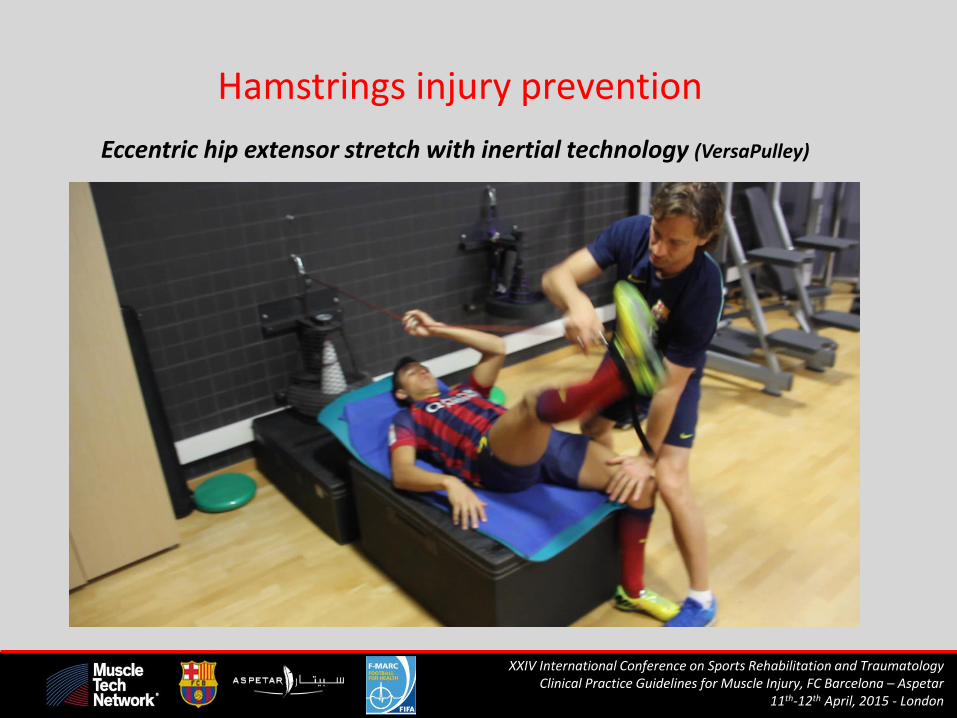
Hamstrings injury prevention
Eccentric hip extensor stretch with inertial technology (VersaPulley)

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
Hamstrings injury prevention
Eccentric knee flexor extension with inertial technology (Yo-Yo Knee Extension)

http://muscletechnetwork.org/proyectos-id/publicaciones/
Take home messages
1. Evolving knowledge.
2. Primary prevention linked with
training.
3. Secondary prevention: personalized.

http://muscletechnetwork.org/proyectos-id/publicaciones/

XXIV International Conference on Sports Rehabilitation and Traumatology Clinical Practice Guidelines for Muscle Injury, FC Barcelona – Aspetar
11th-12th April, 2015 - London
…It has been demonstrated that hamstring injuries typically occur at this musculotendinous junction: either at the proximal or distal ‘‘free’’ ends or, more commonly, at
the central intramuscular tendon... Comin et al. Am J Sports Med. 2013;41(1):111-115