jamie berray loyola university chicago dietetic internship
TRANSCRIPT

Jamie Berray April 9, 2018
Loyola University Chicago Dietetic Internship FONU 423: Clinical Supervised Practice
Case Study

2
NCP Step 1: Nutrition Assessment
Patient Profile Practice Setting in which you are assessing this patient/client
In-patient (821A-General Med/Surgery)
Identifier C.T. Age 59 Gender Female Race/Ethnicity African American Relevant personal data (i.e. language, marital status, lives in a nursing home, socioeconomic status, occupation etc.)
English speaking female, married, daughter present in hospital Non-smoker (never smoked) and never drank alcohol
Admitting diagnosis, chief complaint Pt transfer from St. Anthony hospital for further treatment of newly diagnosed distal esophageal squamous cell carcinoma
Symptoms on presentation Dysphagia, emesis immediately after eating, cough x 2 months
CURRENT Medical Conditions/Diagnoses Distal esophageal squamous cell carcinoma, T2DM, HTN, HLD
PAST Medical Conditions/Diagnoses (previous hospitalizations if pertinent)
Esophageal web, treated with dilation 12 years ago
Medical Test(s) conducted or planned Esophagogastroduodenoscopy (EGD) Medical procedure(s) conducted or planned Laparoscopic J-tube placement
Anthropometric Data: Indicator Value for the patient Assessment of patient
value Height 157 cm Per chart Weight 79.6 kg Per chart, confirmed by
pt Weight change/% change 12 lb wt loss 2 mo / -6% Moderate wt loss UBW/%UBW 85 kg / 94% Pt is 6% below UBW IBW/%IBW 50 kg / 159% Pt is 59% above IBW BMI 32.3 kg/m2 Obese Adjusted Body Weight 57.4 kg Adj BW = 0.25 (Actual
BW – IBW) + IBW
Nutrition Focused Physical Assessment Physical Appearance Obese Muscle and fat wasting Mild temporal wasting Swallowing function Poor Appetite Good Affect (e.g. lethargic, sleeping, coma, energetic, in pain, etc.)
Energetic

3
Food/Nutrition Related History Food Allergies None Chewing and/or Dental Problems None Swallowing Problems Difficulty swallowing related to
esophageal stricture 2/2 esophageal carcinoma
Bowel Habits/Problems Constipation during hospital stay Recent Changes in Eating Habits Unable to tolerate solid foods, eating
softer foods prior to admission Current Appetite Good Food Preferences Softer foods per tolerance Nutrient Malabsorption Problems? None N/V/D/C Vomiting after eating solid foods prior to
admission, tolerating clear liquids during hospital stay without vomiting, Constipation during hospital stay
24 - Hour Recall
Meal Type of Food Portion Breakfast Cherry fruit ice 3 oz Apple juice 4 oz Ensure clear apple 6 oz Liquid protein supplement 1 pouch Chicken broth 3 oz Red gelatin 2 oz Lunch Apple juice 4 oz Ensure clear apple 4 oz Liquid protein supplement 1 pouch Beef broth 2 oz Citrus gelatin 2 oz Dinner Ensure clear apple 2 oz Red gelatin 2 oz
Food Recall Assessment C.T. was previously admitted to another hospital prior to admission and had been NPO/CLD due to her issues tolerating solid foods. Instead of obtaining a 24 hour recall at the time of initial nutrition assessment, I obtained the information for her intake once her clear liquid diet was initiated and a calorie count was requested to determine the need for enteral feeding recommendations. The USDA nutrient analysis software, Super-Tracker was used to analyze C.T.’s intake. Due to limitations with the food database and inability to input custom food items, the estimations may not be completely accurate. The database did not have an option for the Ensure clear supplements, nor the same liquid protein supplements. However, I chose similar items for her intake log so the results provide an estimation that still provide a good picture of the poor nutrition status that the patient was experiencing with just the clear liquid diet. When the calorie count was initially assessed using the actual numbers for calories and protein from the nutrition supplements along with estimations for the
4
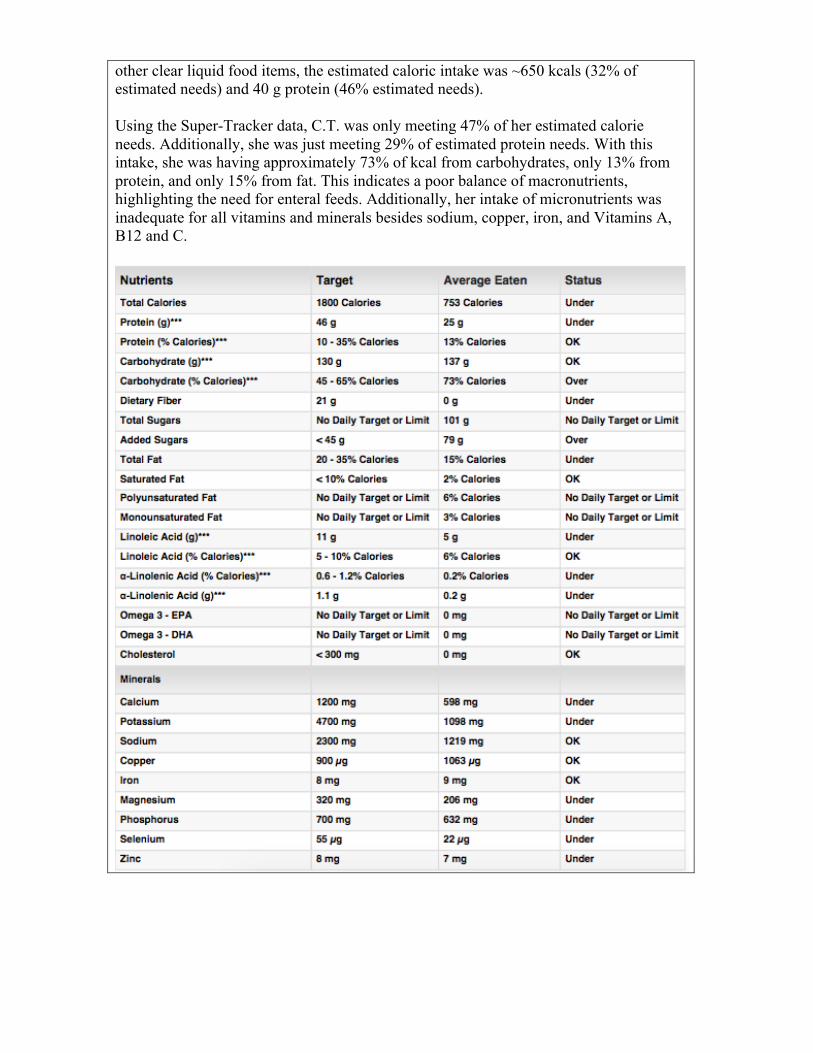
other clear liquid food items, the estimated caloric intake was ~650 kcals (32% of estimated needs) and 40 g protein (46% estimated needs). Using the Super-Tracker data, C.T. was only meeting 47% of her estimated calorie needs. Additionally, she was just meeting 29% of estimated protein needs. With this intake, she was having approximately 73% of kcal from carbohydrates, only 13% from protein, and only 15% from fat. This indicates a poor balance of macronutrients, highlighting the need for enteral feeds. Additionally, her intake of micronutrients was inadequate for all vitamins and minerals besides sodium, copper, iron, and Vitamins A, B12 and C.

5
LABORATORY DATA: Date: 2/28 Date: 3/1 Date: 3/2 Date: 3/3 Date: 3/4 Date: 3/5
Laboratory Test: Normal Values: Values: Values: Values: Values: Values: Values: Diet Order NPO NPO CLD CLD CLD + TF CLD + TF Height 157 cm Weight 79.6 kg Prealbumin 18-38 mg/dL 15.8 ↓ Blood Pressure 120/80 123/76 168/88 140/79 152/82 161/94 140/79 Albumin 3.6-5.1 g/dL 3.6 3.0 ↓ Sodium 135-145 mEq/L 143 143 143 135 143 141 Potassium 3.4-5.1 mEq/L 2.8 ↓ 2.7 ↓ 2.9 ↓ 3.5 3.9 3.2 ↓ Chloride 98-107 101 104 105 107 100 103 BUN 6-20 mg/dL 10 7 6 2 ↓ 3 ↓ 6 Creatinine 0.51-0.95 mg/dL 0.50 ↓ 0.49 ↓ 0.44 ↓ 0.41 ↓ 0.42 ↓ 0.39 ↓ BUN:Creatinine 20 14 14 5 ↓ 7 15 GFR (AA) >90 >90 >90 >90 >90 >90 >90 Calcium 8.4-10.2 mg/dL 10.0 9.2 8.6 8.3 ↓ 8.9 8.7 Magnesium 1.7-2.4 1.6 ↓ 1.9 1.5 ↓ 1.9 1.6 ↓ 1.7 Phosphorus 2.4-4.7 mg/dL 2.9 3.2 2.9 2.2 ↓ 2.8 2.9 Glucose 65-99 mg/dL 104 ↑ 158 ↑ 122 ↑ 167 ↑ 242 ↑ 230 ↑ Hemoglobin 12-15.5 g/dL 12.8 11.6 ↓ 10.5 ↓ 10.8 ↓ 11.4 ↓ 10.7 ↓ Hematocrit 36-46.5% 38.9 34.8 ↓ 32.4 ↓ 32.0 ↓ 35.1↓ 32.5 ↓ RBC 4-5.2 x 106/mm3 4.72 4.27 3.88 ↓ 3.88 ↓ 4.20 3.94 ↓ MCV 78-100 fL 82.4 81.5 83.5 82.5 83.6 82.5 MCH 26-34 pg 27.1 27.2 27.1 27.8 27.1 27.2 MCHC 32-36.5 g/dL 32.9 33.3 32.4 33.8 32.5 32.9

6
DISCUSSION of Laboratory Data Upon evaluation of her laboratory data, C.T. presented with several indicators of poor nutrition status. However, because of the increased stress and inflammation her body was experiencing with her recent diagnosis of esophageal cancer and the tests and procedures she was undergoing during her stay, some of the lab values may not be completely indicative of poor nutrition status/malnutrition. For example, prealbumin, when low, may be an indicator of malnutrition. However, it is also decreased in times of stress and inflammation in the body, which could be the explanation in this case. Similarly, C.T.’s albumin was low, likely due to the acute stress. In addition to acute stress, medications and fluid status can have a great impact of nutritional laboratory data as well. Potassium can be decreased with the use of the medications Lisinopril and Insulin Lispro, which C.T. was receiving during her hospital stay. Magnesium can be decreased with the use of insulin and Docusate Senna medications. Both of these laboratory values could have also been low due to increased fluid loss from the frequent vomiting the pt had been experiencing. Low phosphorus can be sign of refeeding syndrome during the initiation of nutrition support. However, C.T.’s phosphorus levels were monitored and only decreased during one day of her admission. Blood urea nitrogen, or BUN, when high is indicative of renal dysfunction. However, it can be decreased with a low protein and high carbohydrate diet. Given C.T.’s poor intake prior to admission and clear liquid diet with ~70% of calories from carbohydrates for the beginning of her stay, this may have been true of her situation. However, BUN is sensitive to fluid status and may have fluctuated due to administration of fluids with her enteral feedings. Creatinine is interpreted in conjunction with BUN to assess renal function. Unlike BUN, it is not significantly affected by dehydration or malnutrition. When decreased, it is a sign of decreased muscle mass or muscular dystrophy which tends to decrease with age. C.T.’s elevated glucose throughout her stay can be attributed not only to her type 2 Diabetes, but also the acute stress response of her disease state. C.T. shows to have low hemoglobin, low hematocrit, low RBC, normal MCV, MCH, and MCHC. These labs could indicate that C.T. has normocytic anemia, or anemia of chronic disease. This type of anemia could be an indicator of decreased protein as well as malnutrition. Due to lack of lipid panel laboratory data, I was unable to assess C.T.’s hyperlipidemia status. However, she is prescribed a HMG-CoA reductase inhibitor to control this.

7
MEDICATIONS: Medication: Dosage: Purpose or Function: Significant Nutritional Implications: Lisinopril
5 mg, 1 tab, oral, daily Angiotensin converting enzyme (ACE) inhibitor Blood pressure control
Avoid salt substitutes, may increase serum potassium, hold if K is greater than 5.2
Metformin 500 mg, 1 tab, oral, BID Blood sugar control May cause diarrhea, low appetite.
Glipizide 5 mg , 1 tab, oral, daily, 30 tab
Blood sugar control Nausea, vomiting, low appetite, diarrhea, constipation, headache, weight gain.
Pravastatin 10 mg, 1 tab, oral, Q Bedtime
HMG-CoA reductase inhibitor Hyperlipidemia control
Risk of hyperglycemia.
Heparin 1 mL, injection, Q12H Anticoagulant May cause hyperkalemia, metabolic acidosis, contains sodium-avoid on salt-restricted diet or with chronic heart failure.
Insulin Lispro (HumaLOG)
Medium dose, injection, Q6H
Recombinant Human Insulin Analog Control high blood sugar
Hypoglycemia, hyperglycemia, hypokalemia, fluid retention.
Docusate Senna 100 mg, 1 cap, oral, BID, PRN
Stool softener, stimulant laxative
Risk of hypomagnesemia, GI cramping, nausea, diarrhea.
Acetaminophen-hydrocodone
1 tab, oral, Q6H, PRN Combination opiod/non-opioid pain reliever
May decrease bowel mobility, hypokalemia, hyperglycemia.
Ondansetron (Zofran) 4 mg, Q6H, PRN Selective 5-HT3 receptor antagonist Nausea & vomiting
Increase bowel transit time.
Glucagon 1 mg, PRN Give if pt’s blood pressure is less than 7
May cause nausea, vomiting,
DISCUSSION of Medications Constipation: During her admission, C.T. experienced constipation with no bowel movement for two days. This symptom may have been a side effect of acetaminophen-hydrocodone or glipizide medications. Hypomagnesemia: Docusate carries a low risk of hypomagnesemia, which could have contributed to the fluctuations in C.T.’s magnesium levels. Hypokalemia: Low potassium levels have been associated with Heparin, Lisinopril or Insulin Lispro. Insulin Lispro may cause a shift in potassium from extracellular to intracellular space leading to hypokalemia

8
NCP Step 2: Nutrition Diagnosis
PATHOPHYSIOLOGY (CURRENT Medical Conditions) Esophageal squamous cell carcinoma The epithelium, the innermost lining of the esophagus, is made up of flat, thin cells called squamous cells. Cancer that originates in these cells, called squamous cell carcinoma, begins in this inner lining and grows outward through the submucosa and muscle layers. This growth leads to obstructions, or strictures, that block the passage of foods and liquids through the esophagus, leading to dysphagia in most patients (shown in the image below). Surgical intervention is often required for treatment of esophageal cancer, including the partial or total removal of the esophagus and partial removal of the stomach. Early placement of feeding jejunostomy tubes is often indicated for patients with esophageal cancer to allow for early postoperative tube feeds and to provide adequate nutrition while dysphagia occurs with the strictures.
Type 2 Diabetes Mellitus Type 2 Diabetes Mellitus is characterized by a combination of beta-cell failure and insulin resistance, resulting in hyperglycemia. Insulin resistance is initially demonstrated in target tissues such as muscle, liver and adipose tissue. The pancreas is unable to produce adequate insulin relative to the elevated glucose levels in the blood after meals. As insulin secretion decreases, hepatic glucose production increases causing an increase in fasting blood glucose. The beta-cell function progressively decreases causing T2DM patients to require more medication over time, and eventually exogenous insulin, to maintain same level of glycemic control. Stress-induced hyperglycemia, such as during illness, injury, or surgery, may require insulin for control during these periods as well.

9
Hypertension Hypertension is characterized by elevated blood pressure, with a systolic reading above 130 or diastolic reading above 80. Blood pressure, the resistance to the flow of blood in the blood vessels, is the product of cardiac output and peripheral resistance. Blood pressure is affected by the diameter of the blood vessels, therefore, Atherosclerosis which decreases the diameter of blood vessels can lead to hypertension. Factors that contribute to the development of hypertension include genetics, obesity, increased dietary salt intake, and the activation of the sympathetic nervous system and renin-angiotensin-aldosterone system. The kidney is both the contributing and target organ for the hypertensive process and is involved with multiple organ systems in the pathways of blood pressure control. Hypertension can progress and contribute to complications which can damage the aorta, heart, kidneys, retina and central nervous system. Hyperlipidemia Hyperlipidemia is the condition characterized by abnormally high lipids present in the blood, specifically cholesterol and triglycerides. The accumulation of these lipids can contribute to the development of atherosclerosis which can lead to hypertension, stroke, and heart attack. Hyperlipidemia is associated with obesity, excessive consumption of saturated fats, Type 2 Diabetes.
PATHOPHYSIOLOGY (PAST Medical Conditions) Esophageal web Esophageal webs, often referred to as esophageal rings, are thin membranes of normal esophageal tissue, consisting of three layers of mucosa, submucosa and muscle, that cause partial obstructions of the esophagus. The true pathophysiology of esophageal webs remains controversial; proposed theories for include congenital origin, inflammation, iron deficiency, developmental abnormality, and autoimmunity. Esophageal webs are most commonly observed in the presence of Plummer-Vinson Syndrome. This syndrome is viewed as an autoimmune phenomenon associated with a classical triad of dysphagia, iron deficiency anemia and esophageal webs. The etiology and pathophysiology are unknown, but proposed theoretic causes include iron deficiency, genetic predisposition, malnutrition, or autoimmune process. Cases can often be treated effectively with iron supplementation. However, in cases of significant esophageal obstruction, Plummer-Vinson syndrome is treated with rupture and dilation of the web. Although the electronic medical record did not contain information about C.T.’s exact diagnosis related to her esophageal web 12 years ago, this syndrome could potentially have been the etiology.

10
Medical Conditions/Diagnoses INTER-RELATIONSHIPS Esophageal web and esophageal squamous cell carcinoma Esophageal webs caused by Plummer-Vinson syndrome are extremely prone to the development of esophageal squamous cell carcinoma. The explanation for this strong relationship is due to the presence of iron deficiency anemia. Anemia can lead to the epithelial atrophy, which changes cell kinetics, decreasing the ability of repair for the mucosa. This decreased repair capacity allows carcinogens to act aggressively on the mucosa, predisposing the area to malignancy.
Plummer-‐‑Vinson
Syndrome
Esophagealweb, iron deficiency anemia, dysphagia
Decreased repair capacity of esophagealmucosa
Carcinogenic attack on
esophageal cells
Esophageal squamous cell carcinoma
11
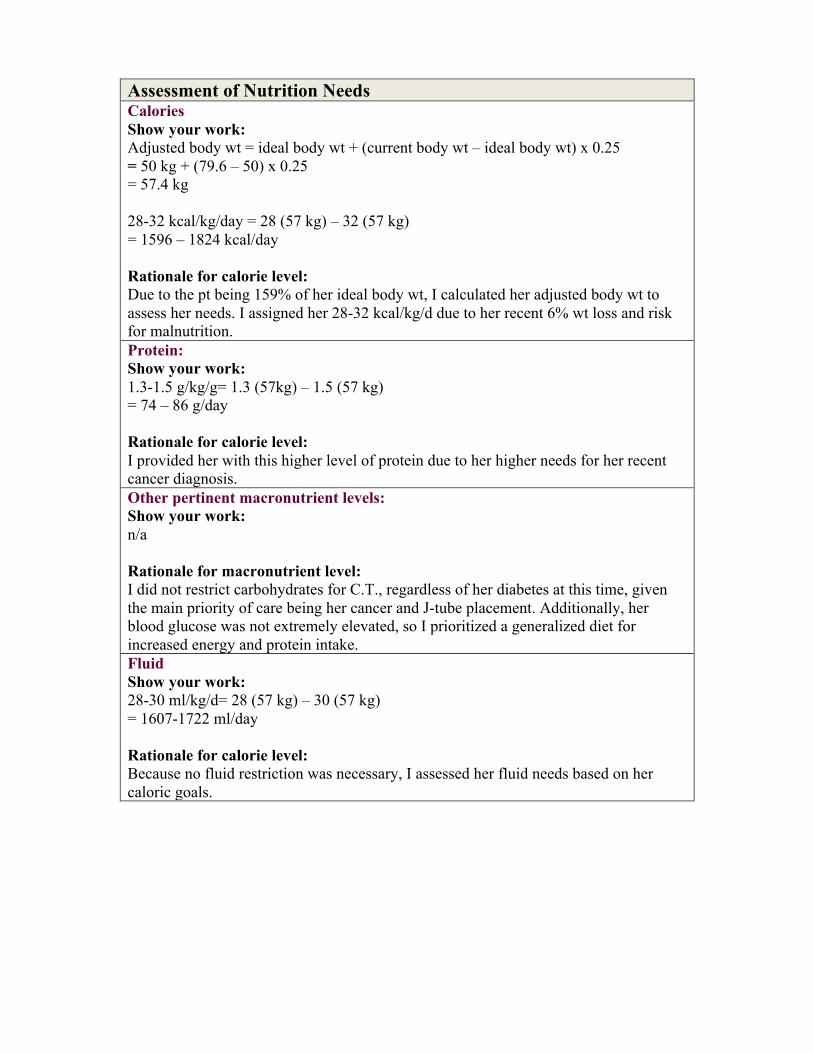
Assessment of Nutrition Needs Calories Show your work: Adjusted body wt = ideal body wt + (current body wt – ideal body wt) x 0.25 = 50 kg + (79.6 – 50) x 0.25 = 57.4 kg 28-32 kcal/kg/day = 28 (57 kg) – 32 (57 kg) = 1596 – 1824 kcal/day Rationale for calorie level: Due to the pt being 159% of her ideal body wt, I calculated her adjusted body wt to assess her needs. I assigned her 28-32 kcal/kg/d due to her recent 6% wt loss and risk for malnutrition. Protein: Show your work: 1.3-1.5 g/kg/g= 1.3 (57kg) – 1.5 (57 kg) = 74 – 86 g/day Rationale for calorie level: I provided her with this higher level of protein due to her higher needs for her recent cancer diagnosis. Other pertinent macronutrient levels: Show your work: n/a Rationale for macronutrient level: I did not restrict carbohydrates for C.T., regardless of her diabetes at this time, given the main priority of care being her cancer and J-tube placement. Additionally, her blood glucose was not extremely elevated, so I prioritized a generalized diet for increased energy and protein intake. Fluid Show your work: 28-30 ml/kg/d= 28 (57 kg) – 30 (57 kg) = 1607-1722 ml/day Rationale for calorie level: Because no fluid restriction was necessary, I assessed her fluid needs based on her caloric goals.

12
Nutrition Diagnosis Which of the following domains is the patient/client presenting with:
DOMAIN Check (ü) if patient presents with this
characteristic
If checked, explain evidence to support this
decision INTAKE Energy Balance ü Inadequate energy intake-
need for NPO and CLD status for ~5 days
Oral or Nutrition Support Intake
ü Inadequate oral intake- need for enteral feeds
Fluid Intake Bioactive Substance Intake Nutrient Intake ü Increased protein needs-
due to cancer diagnosis CLINICAL Functional ü Swallowing difficulty-
emesis after eating solid foods due to esophageal stricture
Biochemical Weight ü Obese, Class I- BMI of 32
Unintended wt loss- 12 lb wt loss in past 2 months (6%)
BEHAVIORAL-ENVIRONMENTAL Knowledge and Beliefs Physical Activity & Function
Food Safety and Access What is the Nutrition Diagnosis for this client/patient?
Diagnosis or Problem
Etiology Signs and/or Symptoms
Inadequate caloric intake
Related to Altered GI function, difficulty swallowing, GI surgery
Related to Need for NPO status and enteral feeding
Inadequate protein intake
Related to Altered GI function, difficulty swallowing, GI surgery
Related to Need for CLD and enteral feeding
13
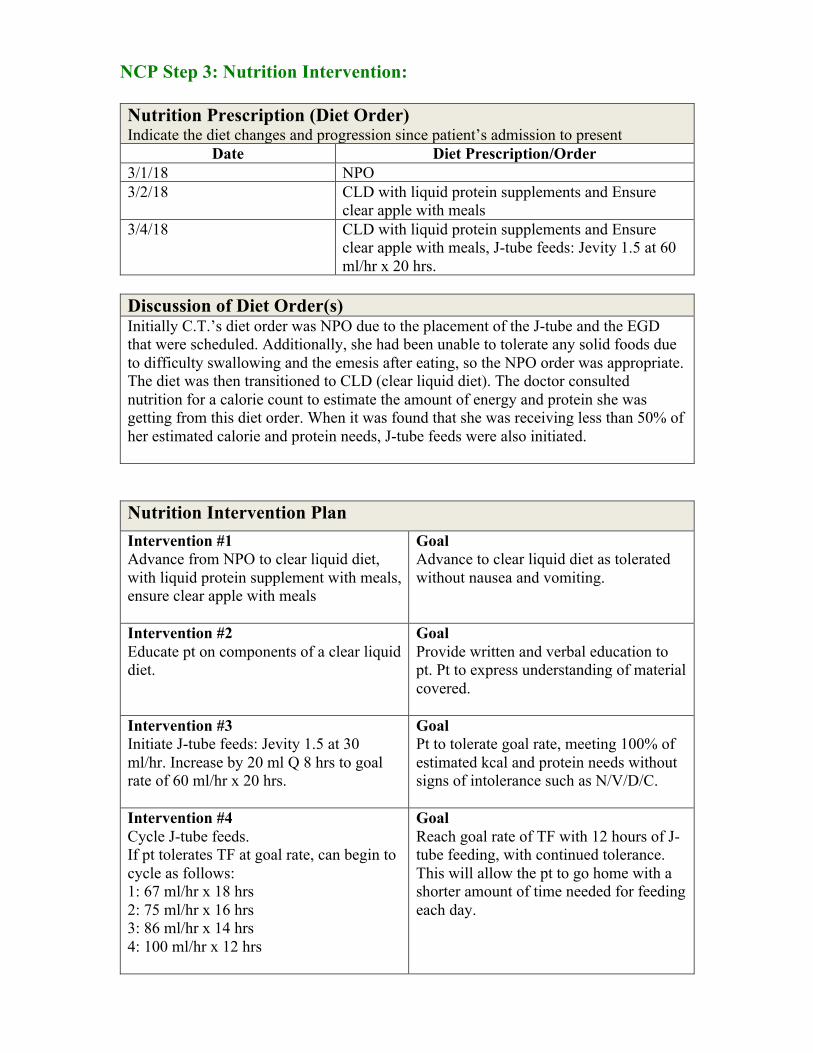
NCP Step 3: Nutrition Intervention: Nutrition Prescription (Diet Order) Indicate the diet changes and progression since patient’s admission to present
Date Diet Prescription/Order 3/1/18 NPO 3/2/18 CLD with liquid protein supplements and Ensure
clear apple with meals 3/4/18 CLD with liquid protein supplements and Ensure
clear apple with meals, J-tube feeds: Jevity 1.5 at 60 ml/hr x 20 hrs.
Discussion of Diet Order(s) Initially C.T.’s diet order was NPO due to the placement of the J-tube and the EGD that were scheduled. Additionally, she had been unable to tolerate any solid foods due to difficulty swallowing and the emesis after eating, so the NPO order was appropriate. The diet was then transitioned to CLD (clear liquid diet). The doctor consulted nutrition for a calorie count to estimate the amount of energy and protein she was getting from this diet order. When it was found that she was receiving less than 50% of her estimated calorie and protein needs, J-tube feeds were also initiated.
Nutrition Intervention Plan Intervention #1 Advance from NPO to clear liquid diet, with liquid protein supplement with meals, ensure clear apple with meals
Goal Advance to clear liquid diet as tolerated without nausea and vomiting.
Intervention #2 Educate pt on components of a clear liquid diet.
Goal Provide written and verbal education to pt. Pt to express understanding of material covered.
Intervention #3 Initiate J-tube feeds: Jevity 1.5 at 30 ml/hr. Increase by 20 ml Q 8 hrs to goal rate of 60 ml/hr x 20 hrs.
Goal Pt to tolerate goal rate, meeting 100% of estimated kcal and protein needs without signs of intolerance such as N/V/D/C.
Intervention #4 Cycle J-tube feeds. If pt tolerates TF at goal rate, can begin to cycle as follows: 1: 67 ml/hr x 18 hrs 2: 75 ml/hr x 16 hrs 3: 86 ml/hr x 14 hrs 4: 100 ml/hr x 12 hrs
Goal Reach goal rate of TF with 12 hours of J-tube feeding, with continued tolerance. This will allow the pt to go home with a shorter amount of time needed for feeding each day.

14
Nutrition Intervention Plan Nutrition Prescription
Current order: NPO Your Recommendation: CLD and Jevity 1.5
Which goal is the priority at this time? Meet 100% of calorie and protein needs through J-tube feeds.
If instruction was given, who did you instruct?
I instructed the pt and her daughter on the components of a clear liquid diet.
What instructional materials did you use? Where they effective? Why or why not?
I used the clear liquid diet patient education materials from the nutrition care manual. This was effective because it had an entire listing of liquids that were acceptable and it made things more clear for the patient.
If patient has been education, what is their motivation/compliance level at this time?
She was very motivated and willing to stick to this plan.
Does the patient have any barriers to compliance to the interventions?
None that I found.
NCP Step 4: Monitoring and Evaluation Health Care Outcomes Based on your Nutrition Intervention indicate below what outcome measurements you will use to monitor progress and success of the interventions. Intervention
Health & Disease Outcomes
Cost Outcomes
Patient Outcomes
Initiate J-tube feeds of Jevity 1.5
Prevention of malnutrition
Minimize unnecessary financial costs
Pt to meet goal of 100% of energy and protein needs via enteral support
Provide education on clear liquid diet
Patient compliance Minimize unnecessary financial costs
Pt was discharged with continued recommendation of clear liquid diet

15
Monitoring and Evaluation Question to Consider Answer/Reflection
What indices are you using to determine success of your intervention?
Tolerance of tube feed regimen- no signs of N/V/D/C
Did the intervention work? Explain Yes, the patient was able to tolerate the feeds at goal rate without any digestive issues.
If the intervention is not working, indicate what follow up action you took.
n/a
What are the causes of initial interventions that did not work?
n/a
How will you monitor success of your follow up interventions?
If the pt would have stayed in the hospital longer, I would have liked to monitor her tolerance of cycling her tube feeding down to a goal of 12 hours.
CONCLUSION
1. Brief concluding remarks. How did the case end in terms of your involvement?
In terms of my involvement, C.T. was discharged shortly after tolerating the goal rate of TF of 60 ml/hr over a time period of 20 hours. If the patient would have stayed in the hospital for a few more days, I would have recommended her J-tube feeds be cycled down to 12 hours so that we could monitor tolerance of feeding at 12 hours/day so that she would have to spend less time each day getting her feedings.
2. What did you learn from this case that you feel you can use for future practice?
Through this experience I learned about the complexity of esophageal squamous cell carcinoma and the complications that arise with esophageal webs/strictures. I learned about the importance of early initiation of enteral feeding in a medical condition where removal of part of the esophagus and stomach is anticipated.
DOCUMENTATION Attach all initial and follow up notes for this patient/client to this report. Be sure to delete any data that may identify the patient such as name or room number.
REFERENCES 1.) Novacek, G. (2006). Plummer-Vinson syndrome. Orphanet Journal of Rare Diseases. 2.) Samad, A. (2005).Oral Manifestations of Plummer-Vinson Syndrome: A Classic Report with Literature Review. Journal of International Oral Health. 3.) What Is Cancer of the Esophagus? (n.d.). Retrieved from https://www.cancer.org/cancer/esophagus-cancer/about/what-is-cancer-of-the-

16
esophagus.html 4.) Mahan, L. Kathleen; Raymond, Janice L (2016-05-17). Krause's Food & the Nutrition Care Process (Krause's Food & Nutrition Therapy) Elsevier Health Sciences. 5.) Heparin (Porcine): Uses, Side Effects, Interactions, Pictures, Warnings & Dosing. (n.d.). Retrieved from https://www.webmd.com/drugs/2/drug-3918/heparin-porcine-injection/details 6.) Humalog Pen Subcutaneous : Uses, Side Effects, Interactions, Pictures, Warnings & Dosing. (n.d.). Retrieved from https://www.webmd.com/drugs/2/drug-16875/humalog-pen-subcutaneous/details 7.) Lisinopril Oral : Uses, Side Effects, Interactions, Pictures, Warnings & Dosing. (n.d.). Retrieved from https://www.webmd.com/drugs/2/drug-6873-9371/lisinopril-oral/lisinopril-oral/detailshttps://www.webmd.com/drugs/2/drug-6989/pravastatin-oral/details 9.) Glipizide Oral : Uses, Side Effects, Interactions, Pictures, Warnings & Dosing. (n.d.). Retrieved from https://www.webmd.com/drugs/2/drug-10094-9061/glipizide-oral/glipizide-tablet-oral/details 10.) Senna With Docusate Sodium Oral : Uses, Side Effects, Interactions, Pictures, Warnings & Dosing. (n.d.). Retrieved from https://www.webmd.com/drugs/2/drug-146747/senna-with-docusate-sodium-oral/details 11.) New ACC/AHA High Blood Pressure Guidelines Lower Definition of Hypertension. (n.d.). Retrieved from http://www.acc.org/latest-in-cardiology/articles/2017/11/08/11/47/mon-5pm-bp-guideline-aha-2017 12.) Pathophysiology of Hypertension . (2017, May 18). Retrieved from https://emedicine.medscape.com/article/1937383-overview?pa=AxiDOxg/0weOeiM1QQrZNae38t78ho81Rl5m7rgCLsC9PKTW0FAI5qXvGyvMsT5GX8MwC0EECwzp432Skuf9qw== 13.) Hyperlipidemia in Patients with Type 2 Diabetes. (1999, March 15). Retrieved from https://www.aafp.org/afp/1999/0315/p1666.html 14.) Vergès, B. (2015). Pathophysiology of diabetic dyslipidaemia: Where are we? Diabetologia, 58(5), 886-899. 15.) Esophageal Webs and Rings. (2017, January 06). Retrieved from https://emedicine.medscape.com/article/186561-overview#a2 16.) Esophageal Cancer. (2018, March 22). Retrieved from https://emedicine.medscape.com/article/277930-overview#a5