jamilah alsaidan, msc. the three consecutive phases of emesis are: emesis nausearetchingvomiting
TRANSCRIPT
Chemotherapy Induced Nausea and VomitingJamilah Alsaidan, Msc
The three consecutive phases of emesis are:
Chemotherapy Induced Nausea and Vomiting
Emesis
Nausea Retching Vomiting
• Inclination to vomit• Feeling in throat or epigastric region alerting
individual vomiting is imminent. Nausea
• Is the labored movement of the abdominal and thoracic muscles before vomitingRetching
• The forceful expulsion of gastric contents through the mouth due to GI retroperistalsisVomiting
Chemotherapy Induced Nausea and Vomiting
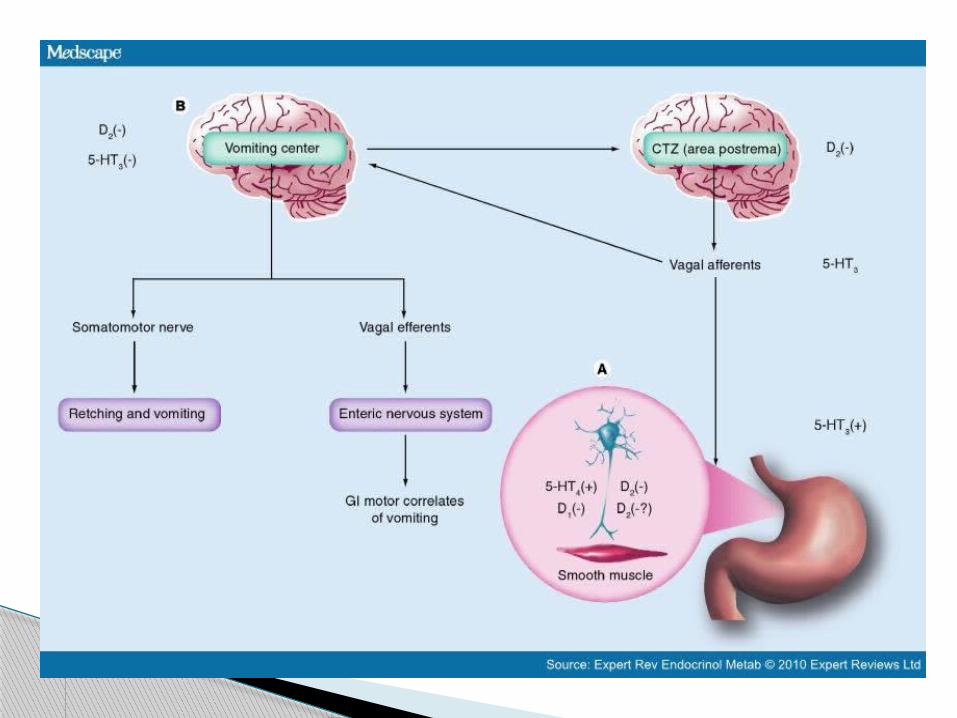
Vomiting is triggered by afferent impulses to the vomiting center, a nucleus of cells in the medulla
Impulses are received from sensory centers, such as:
the chemoreceptor trigger zone (CTZ), Cerebral cortex, visceral afferents from the pharynx and GI
tract
Chemotherapy Induced Nausea and Vomiting- Etiology

Numerous neurotransmitter receptors are located in the vomiting center, CTZ, and GI tract
Cholinergic, histaminic, dopaminergic, opiate, serotonergic, neurokinin, and benzodiazepine receptors
Three main causes of vomiting Stimulation of chemoreceptor trigger zone
in the 4th ventricle Stimulation of the GI tract Sensory input and memory
Chemotherapy Induced Nausea and Vomiting- Etiology
Nausea and or / vomiting may be part of the symptom complex for a variety of gastrointestinal, cardiovascular, infectious, neurologic, metabolic or psychogenic processes
Chemotherapy Induced Nausea and Vomiting
N & V may be a feature of such conditions as pregnancy, may follow operative procedures administration of certain medications such
as those used in cancer chemotherapy or inhalation of noxious odors
Chemotherapy Induced Nausea and Vomiting
General Depending on severity of symptoms, patients
may present in mild to severe distress Symptoms Simple: Self-limiting, resolves spontaneously
and requires only symptomatic therapy Complex: Not relieved after administration of
antiemetics; progressive deterioration of patient secondary to fluid-electrolyte imbalances; usually associated with noxious agents or psychogenic events
Chemotherapy Induced Nausea and Vomiting- Clinical Presentation
Signs Simple: Patient complaint of queasiness or
discomfort Complex: Weight loss; fever; abdominal
pain Laboratory tests Simple: None Complex: Serum electrolyte concentrations;
upper/lower GI evaluation
Chemotherapy Induced Nausea and Vomiting- Clinical Presentation
Chemotherapy Induced Nausea and Vomiting- Clinical Presentation Other information Fluid input and output Medication history Recent history of behavioral or visual
changes, headache, pain, or stress Family history positive for psychogenic
vomiting
Gastrointestinal mechanisms Mechanical obstruction- e.g. Gastric outlet
obstruction, Small bowel obstruction Functional gastrointestinal disorders-
e.g.Gastroparesis, Nonulcer dyspepsia, Chronic intestinal pseudoobstruction, Irritable bowel syndrome
Organic gastrointestinal disorders e.g Peptic ulcer disease,Pancreatitis, Pyelonephritis, Cholecystitis ,Cholangitis, Hepatitis
Acute gastroenteritis ( Viral, Bacterial)
Chemotherapy Induced Nausea and Vomiting- Specific etiologies

Cardiovascular diseases Acute myocardial infarction
Miscellaneous causes Pregnancy Noxious odors Operative procedures
Neurologic processes Migraine headache Vestibular disorders
Chemotherapy Induced Nausea and Vomiting- Specific etiologies
Chemotherapy Induced Nausea and Vomiting- Specific etiologies Metabolic disorders Diabetes mellitus
(diabetic ketoacidosis) Renal disease
(uremia) Psychiatric causes Anxiety disorders Anorexia nervosa Drug withdrawal Opiates Benzodiazepines
Therapy-induced causes
Cytotoxic chemotherapy
Radiation therapy Anticonvulsant
preparations Opiates Antibiotics
Emetogenic potential of chemotherapy agents
HighModerateLowMinimal
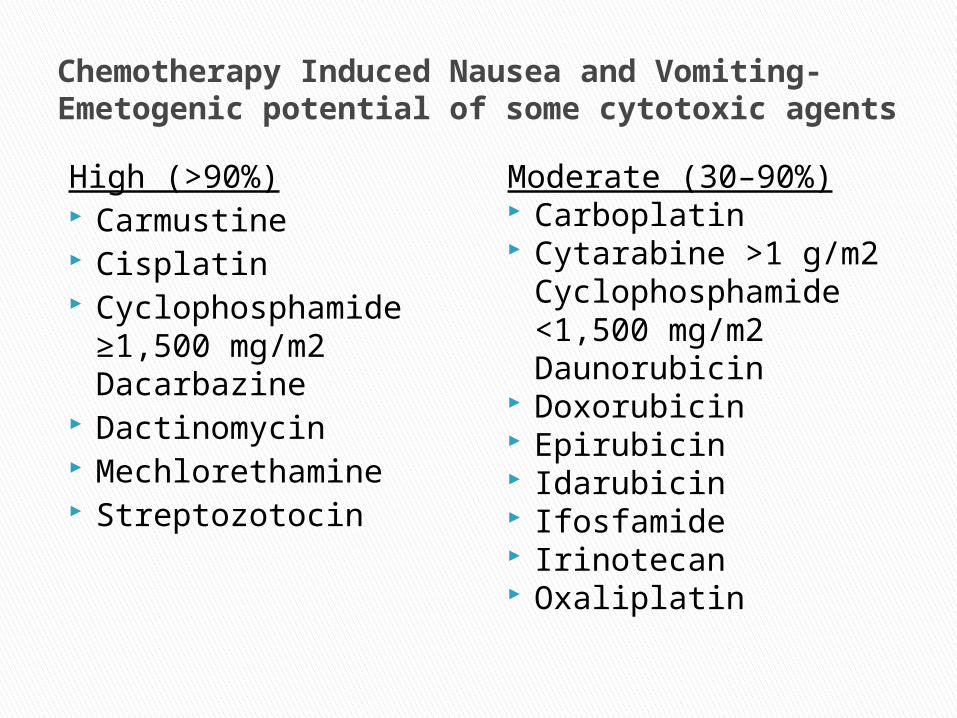
Chemotherapy Induced Nausea and Vomiting- Emetogenic potential of some cytotoxic agents
High (>90%) Carmustine Cisplatin Cyclophosphamide
≥1,500 mg/m2 Dacarbazine
Dactinomycin Mechlorethamine Streptozotocin
Moderate (30–90%) Carboplatin Cytarabine >1 g/m2
Cyclophosphamide <1,500 mg/m2 Daunorubicin
Doxorubicin Epirubicin Idarubicin Ifosfamide Irinotecan Oxaliplatin
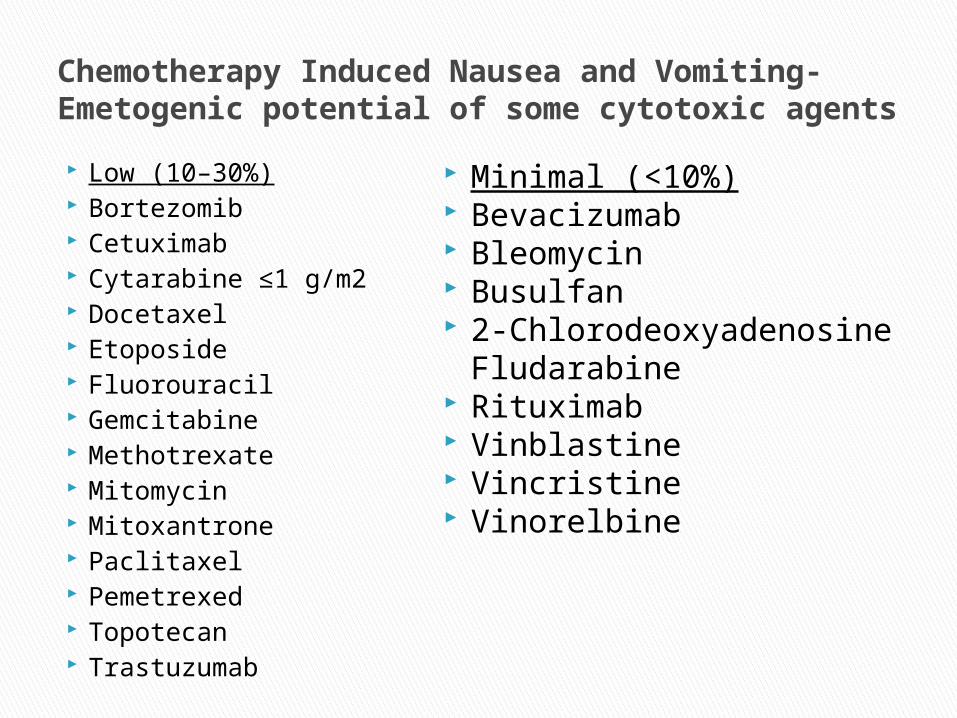
Chemotherapy Induced Nausea and Vomiting- Emetogenic potential of some cytotoxic agents
Low (10–30%) Bortezomib Cetuximab Cytarabine ≤1 g/m2 Docetaxel Etoposide Fluorouracil Gemcitabine Methotrexate Mitomycin Mitoxantrone Paclitaxel Pemetrexed Topotecan Trastuzumab
Minimal (<10%) Bevacizumab Bleomycin Busulfan 2-Chlorodeoxyadenosine
Fludarabine Rituximab Vinblastine Vincristine Vinorelbine
Non-Chemotherapy Etiologies of Nausea and vomiting in cancer patients
Fluid and electrolyte abnormalities Hypercalcemia Volume depletion Adrenocortical insufficiency Drug Induced Opiates Antifungals Antibiotics
Chemotherapy Induced Nausea and Vomiting
Other Uremia Metastases Gastrointestinal obstruction Increased intracranial pressure Peritonitis Radiation Therapy
Chemotherapy Induced Nausea and Vomiting
The overall goal of antiemetic therapy is to prevent or eliminate nausea and vomiting
This should be accomplished without adverse events or with clinically acceptable adverse effects
Simple nausea and vomiting prevention is achieved easily with treatment
Patients with more complex problems require greater assistance
Chemotherapy Induced Nausea and Vomiting- Desired outcome of treatment
General Approach to Treatment
Non drug Modalities Medication
Chemotherapy Induced Nausea and Vomiting- Treatment Modalities
The treatment choice depends on severity of the NV and associated conditions
The management of psychogenic vomiting is greatly dependent on psychological intervention
Underlying problems are complex and must be addressed
Treatment of underlying psychological disorder with its appropriate medications
E.g. Bulimia nervosa
Chemotherapy Induced Nausea and Vomiting
Non drug modalities include Dietary, Psychological, or physical changes
Simple complaints- Avoid or intake in moderation troublesome food, beverage or odor
Behavioral interventions include relaxation, biofeedback, self hypnosis, cognitive distraction, guided imagery, and systematic desensitization
Chemotherapy Induced Nausea and Vomiting- Non Drug Modalities
Antiemetic drugs- both non-prescription and prescription are recommended
The treatment of simple nausea and vomiting usually requires minimal therapy. Drugs are usually effective in small, infrequently administered doses.
The management of complex nausea and vomiting, for example, in patients who are receiving cytotoxic chemotherapy, may require combination therapy.
Chemotherapy Induced Nausea and Vomiting- Pharmacologic Therapy
Many treatment options for clinician to choose from
Factors that enable a clinician to discriminate between medication options:
A) The suspected etiology of the symptoms B) The frequency, duration, and severity of the
episodes C) The ability of the patient to use oral, rectal,
injectable, or transdermal medications D) The success of previous antiemetic
medication
Chemotherapy Induced Nausea and Vomiting
In relation to chemotherapy administration; Nausea or vomiting that occurs:
within 24 hours: Acute Intensity peaks after 5-6 hours after 24 hours: Delayed before chemo given: Anticipatory
Chemotherapy Induced Nausea and Vomiting
The distinction between acute and delayed symptoms becomes blurred with respect to time of onset after several doses and for several consecutive days
Delayed symptoms are best described with cisplatin
Chemotherapy Induced Nausea and Vomiting

Breakthrough vomiting occurs despite prophylactic treatment and /or requires additional rescue medications
Refractory emesis refers to emesis that occurs during treatment cycles when antiemetic prophylaxis and / or rescue therapy has failed in previous cycles
Chemotherapy Induced Nausea and Vomiting
Factors to consider when selecting an antiemetic for CINV include the following:
1) The emetic risk of the chemotherapy agent or regimen
2) Patient specific factors3) Patterns of emesis after administration of
specific chemotherapy agents or regimens
Chemotherapy Induced Nausea and Vomiting- Factors to consider
The emetic risk of the agent is the most important and primary factor to consider when deciding IF you will administer prophylactic agents and WHICH antiemetic agent to select
The combination of metoclopramide and dexamethasone was the most common regimen to prevent delayed nausea and vomiting before the availability of aprepitant
The combination is still used when aprepitant has not been incorporated into the initial regimen for CINV
Single agent phenothiazaine butytophenone, or steroids are used for mildly to moderately emetogenic regimens and for “as needed” use for prolonged symptoms ( breakthrough symptoms)
Chemotherapy Induced Nausea and Vomiting- Factors to consider
Patients receiving chemotherapy classified to be high risk should receive a combination antiemetic regimen containing three drugs on the day of chemotherapy administration (Day one)
A serotonin 5-HT3 inhibitor (e.g. Dolasetron, Granisetron, Ondansetron, Palonosetron, ) + dexamethasone plus NK1 inhibitor ( e.g. aprepitant)
Chemotherapy Induced Nausea and Vomiting
Patients receiving regimens that are classified as being of moderate emetic risk should receive a combination antiemetic regimen containing an serotonin 5-HT3 inhibitor plus dexamethasone on day 1.
The exception to this is patients receiving an anthracycline and cyclophosphamide should receive the triple regimen described for high emetic risk regimens
For prophylaxis prior to administration of regimens classified as low emetogenic risk dexamethasone alone is recommended
Chemotherapy Induced Nausea and Vomiting
High Emetic risk Serotonin 5-HT3 inhibitor + dexamethasone +
aprepitantModerate Emetic risk Anthracycline + cyclophosphamide:Serotonin 5-HT3 inhibitor + dexamethasone + aprepitant All other regimens of moderate emetic risk:Serotonin 5-HT3 inhibitor + dexamethasone
Low Emetic Risk DexamethasoneMinimal riskNo medication
Chemotherapy Induced Nausea and Vomiting- Prophylaxis of Acute Phase of CINV on Day of Chemotherapy Administration (Day 1)
High Emetic Risk Serotonin 5-HT3 inhibitor : Dolasetron 100 mg po or 100 mg IV or 1.8
mg/kg IV Granisetron 2 mg po or 1 mg IV or 0.01 mg/kg
IV Ondansetron 24 mg po or 8 mg IV or 0.15
mg/kg IV Palonosetron 0.25 mg IV AND Dexamethasone 12 mg po AND Aprepitant 125 mg po
Chemotherapy Induced Nausea and Vomiting- Prophylaxis of Acute Phase of CINV on Day of Chemotherapy Administration (Day 1) DOSES
Moderate emetic risk Anthracycline and cyclophosphamide- as before,
as high emetic risk All other regimens of moderate emetic risk: Dolasetron 100 mg po or 100 mg IV or 1.8
mg/kg IV Granisetron 2 mg po or 1 mg IV or 0.01 mg/kg IV Ondansetron 24 mg po or 8 mg IV or 0.15 mg/kg
IV Palonosetron 0.25 mg IV AND Dexamethasone 8mg IV
Chemotherapy Induced Nausea and Vomiting- Prophylaxis of Acute Phase of CINV on Day of Chemotherapy Administration (Day 1)

Low Risk Dexamethasone 8mg IV
Minimal Risk None
Chemotherapy Induced Nausea and Vomiting- Prophylaxis of Acute Phase of CINV on Day of Chemotherapy Administration (Day 1)
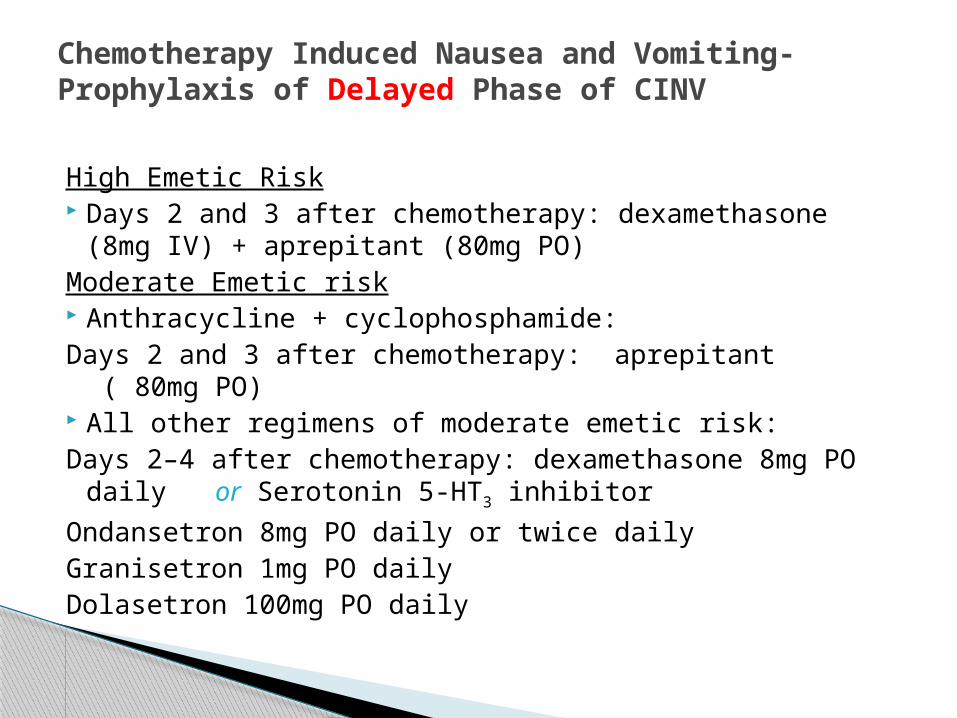
High Emetic Risk Days 2 and 3 after chemotherapy: dexamethasone (8mg
IV) + aprepitant (80mg PO)Moderate Emetic risk Anthracycline + cyclophosphamide:Days 2 and 3 after chemotherapy: aprepitant ( 80mg
PO) All other regimens of moderate emetic risk:Days 2–4 after chemotherapy: dexamethasone 8mg PO
daily or Serotonin 5-HT3 inhibitor
Ondansetron 8mg PO daily or twice dailyGranisetron 1mg PO dailyDolasetron 100mg PO daily
Chemotherapy Induced Nausea and Vomiting- Prophylaxis of Delayed Phase of CINV
Low Emetic Risk- None
Minimal Emetic Risk- None
Chemotherapy Induced Nausea and Vomiting- Prophylaxis of Delayed Phase of CINV

The best strategy to prevent delayed CINV is to control acute CINV
Aprepitant, dexamethasone and metoclopramide have demonstrated efficacy in preventing delayed CINV
Patients receiving cisplatin and other agents are at highest risk to experience delayed NV
The management of delayed CINV caused by high risk emetogenic regimens is more well defined than moderate emetic risk regimens
Chemotherapy Induced Nausea and Vomiting
Cannabinoids are used after the failure of other regimens or to stimulate appetite
Consider using an H2 blocker or proton pump inhibitor to prevent dyspepsia ( may mimic nausea)
Not FDA approved indications therefore doses not recommended
Chemotherapy Induced Nausea and Vomiting