january 25, 2015 introduction to pharmacology · january 25, 2015 introduction to pharmacology...
TRANSCRIPT

1
January 25, 2015
Introduction to Pharmacology
Edward Fisher, Ph.D., R.Ph.
Professor and Associate Dean for Academic AffairsDirector MS Clinical Psychopharmacology
University of Hawaii at HiloCollege of [email protected]
Ligands
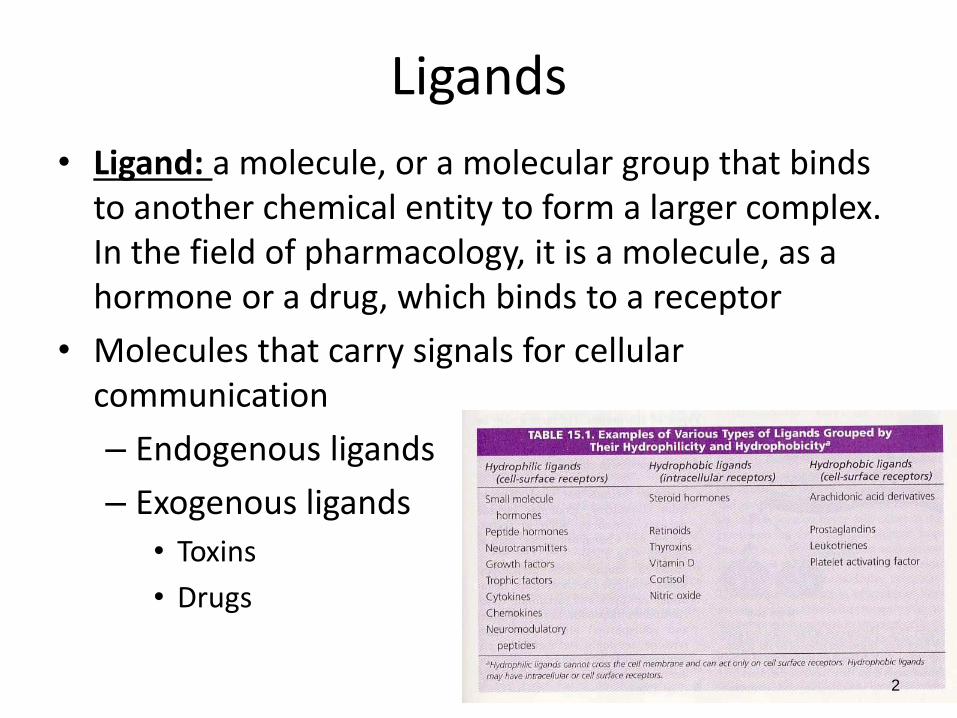
• Ligand: a molecule, or a molecular group that binds to another chemical entity to form a larger complex. In the field of pharmacology, it is a molecule, as a hormone or a drug, which binds to a receptor
• Molecules that carry signals for cellular communication
– Endogenous ligands
– Exogenous ligands
• Toxins
• Drugs
2
Introduction to Pharmacology
3
Pharmacology: the study of substances that interact with living
systems through chemical processes.
Medical pharmacology – therapeutic application
Toxicology – undesirable effects of chemicals on living systems
Pharmacodynamics: the actions of the drug on the body.
Biochemical effects, mechanism of action (MOA)
Drug classification
Pharmacokinetics: the actions of the body on the drug.
Absorption, distribution, metabolism, & excretion
Involved with the time course of the drug in the body
How the drug affects you
How you affect the drug

4
DRUG ADMINISTRATION
PHARMACOKINETICS
1.
2.
PHARMACODYNAMICS3.
Effects of the body on drugs:
• Absorption
• Distribution
• Elimination
• Metabolism
Effects of drugs on the body:
• Receptor-mediated responses

Introduction to Pharmacology
• Receptor: part of an organism or cell (macromolecule) that interacts with a ligand (drug, endogenous molecule) causing a chain of biochemical events leading to an observable response.
Active states vs. inactive states
• Inert Binding Site: a component of the biologic system to which a drug binds without changing any function
5
Introduction to Pharmacology
6
Drug: any substance that brings about a change in biologic
function through its chemical actions.
Endogenous – synthesized in the body (hormones)
Xenobiotics – chemicals not synthesized by the body
Drug: Pharmacy definition: Articles intended for use in the
diagnosis, cure, mitigation, treatment or prevention of disease in
man or other animals
.
7
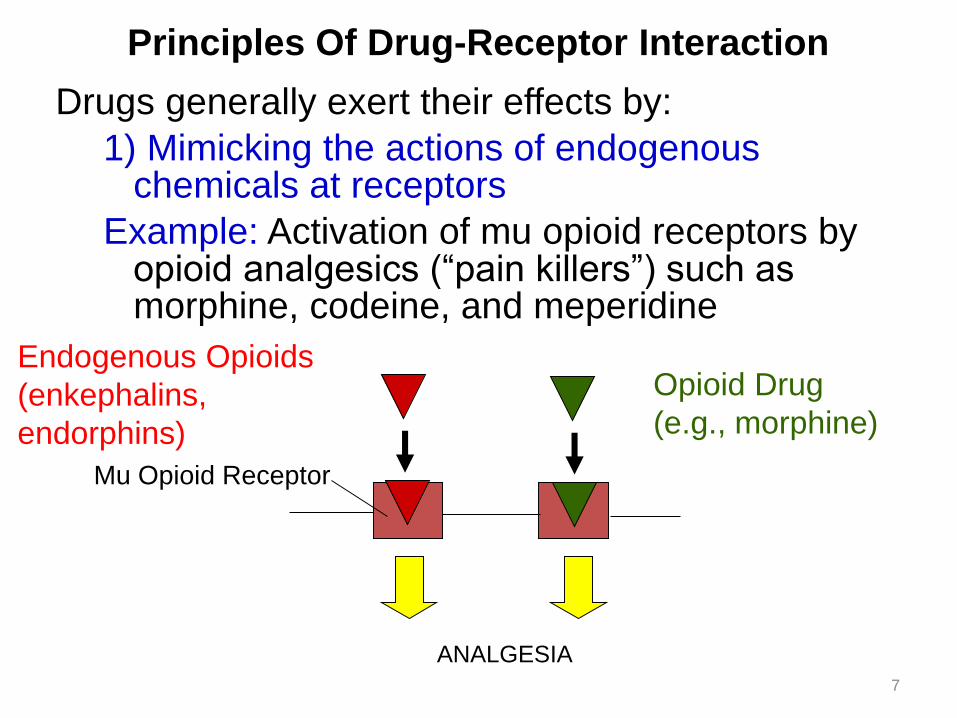
Principles Of Drug-Receptor Interaction
Drugs generally exert their effects by:
1) Mimicking the actions of endogenous chemicals at receptors
Example: Activation of mu opioid receptors by opioid analgesics (“pain killers”) such as morphine, codeine, and meperidine
Mu Opioid Receptor
ANALGESIA
Endogenous Opioids
(enkephalins,
endorphins)
Opioid Drug
(e.g., morphine)
8
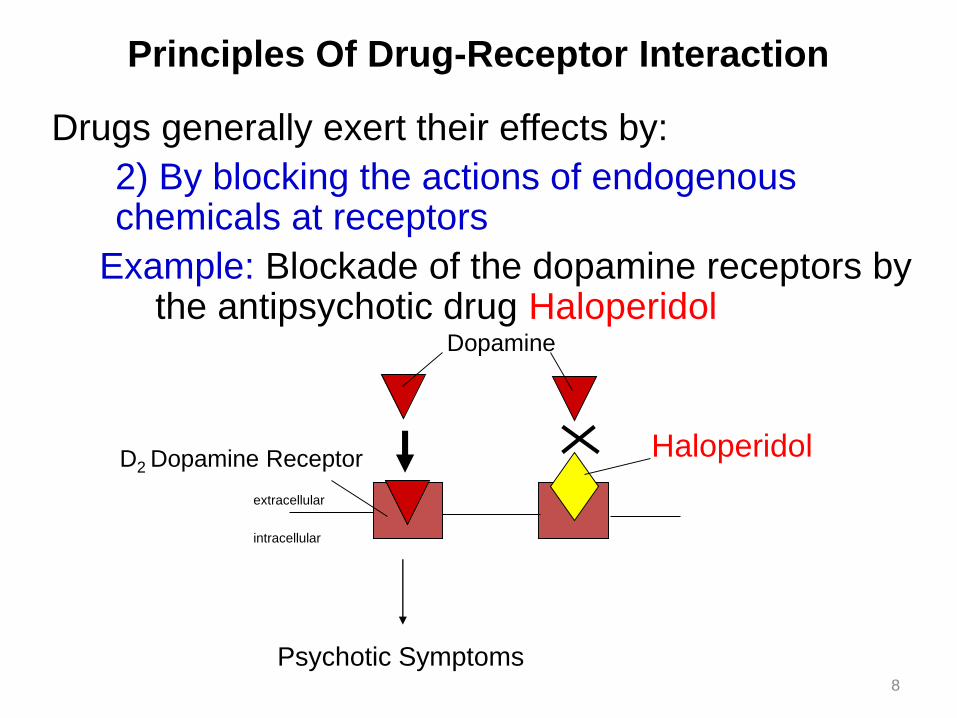
Principles Of Drug-Receptor Interaction
Drugs generally exert their effects by:
2) By blocking the actions of endogenous chemicals at receptors
Example: Blockade of the dopamine receptors by the antipsychotic drug Haloperidol
D2 Dopamine Receptor Haloperidol
Dopamine
extracellular
intracellular
Psychotic Symptoms

Principles Of Drug-Receptor Interaction
9
Drugs generally exert their effects by:
3)By Inhibiting enzymes
• Examples
– Monoamine oxidase inhibitor phenelzine (Nardil®)– COX2 (cyclooxygenase-2) inhibitor – celecoxib –
treatment of inflammatory disorders
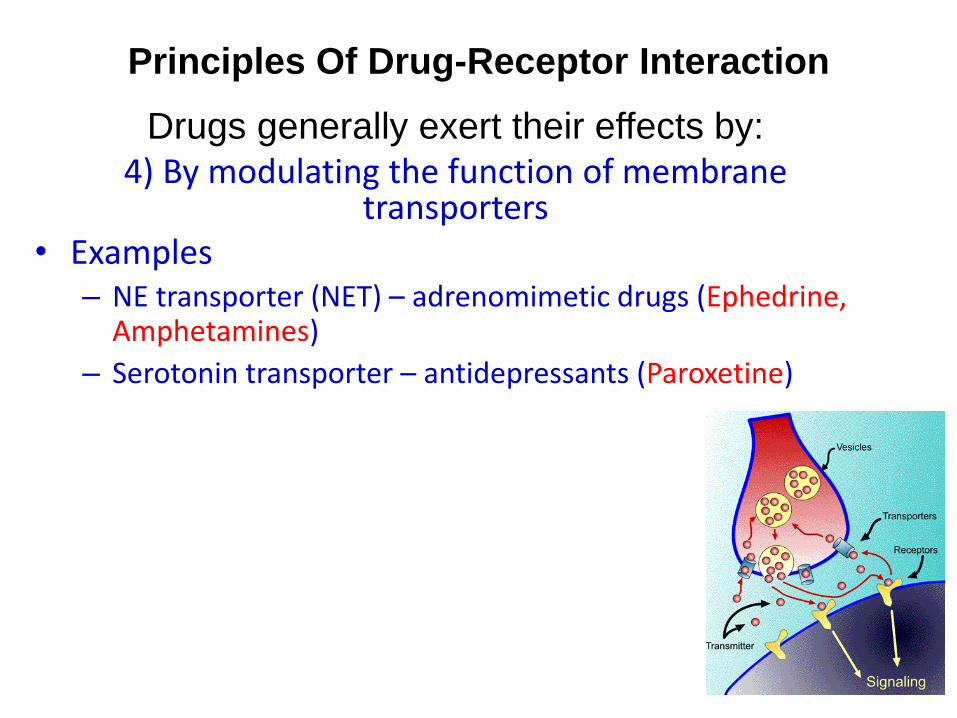
Principles Of Drug-Receptor Interaction
10
Drugs generally exert their effects by:
4) By modulating the function of membrane transporters
• Examples – NE transporter (NET) – adrenomimetic drugs (Ephedrine,
Amphetamines)
– Serotonin transporter – antidepressants (Paroxetine)
11
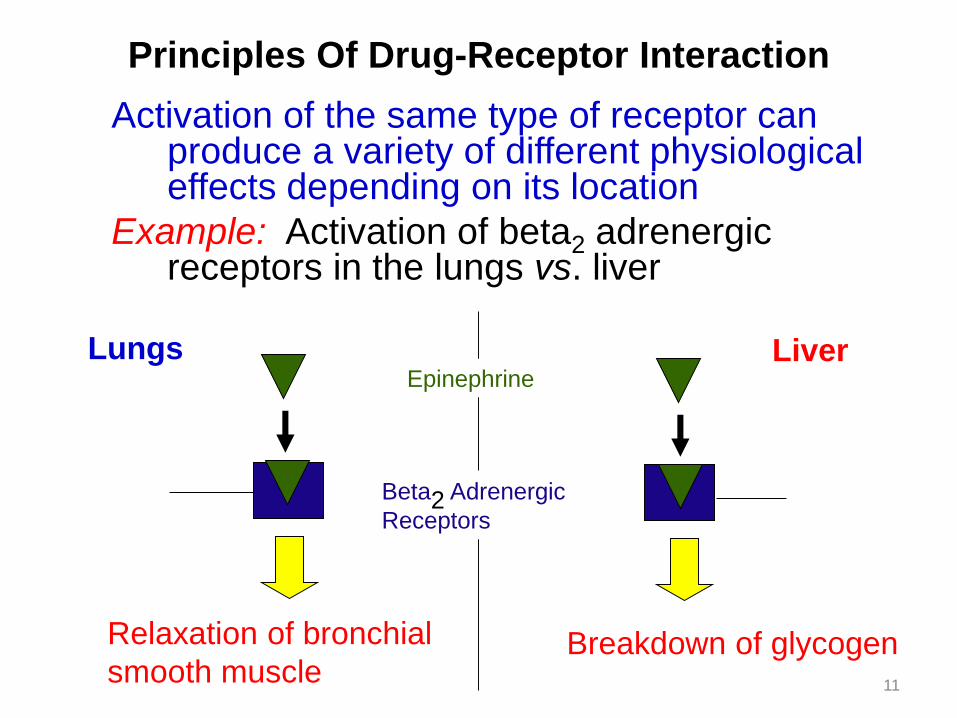
Principles Of Drug-Receptor Interaction
Activation of the same type of receptor can produce a variety of different physiological effects depending on its location
Example: Activation of beta2 adrenergic receptors in the lungs vs. liver
Relaxation of bronchial
smooth muscleBreakdown of glycogen
Beta2 Adrenergic
Receptors
EpinephrineLungs Liver
Principles Of Drug-Receptor Interaction
Inhibition of the same type of receptor can produce a variety of different physiological effects depending on its location
• Example: Haloperidol - Potent D₂ blockade
nigrostriatal causes EPS - Dopamine-mesolimbic treats positive symptoms
12
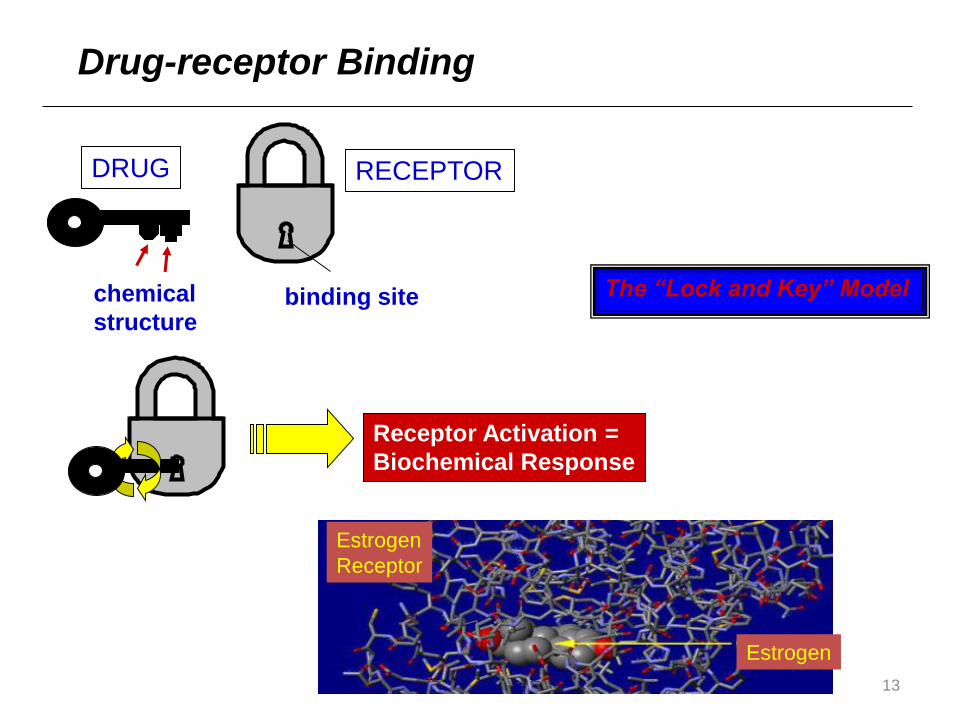
13
Receptor Activation =
Biochemical Response
chemical
structure
DRUG
binding site
RECEPTOR
Estrogen
Estrogen
Receptor
Drug-receptor Binding
The “Lock and Key” Model

Introduction to Pharmacology
14
Drug targets – biomolecules that have a role in the disease
process and are considered to be the site of action for drug
therapy (receptors, enzymes, DNA, ion channels, transport
proteins)

Introduction to Pharmacology
15
Agonist: a drug that binds to and activates a receptor which
brings about an effect.
Albuterol – β2-selective adrenoceptor agonist
Introduction to Pharmacology
16
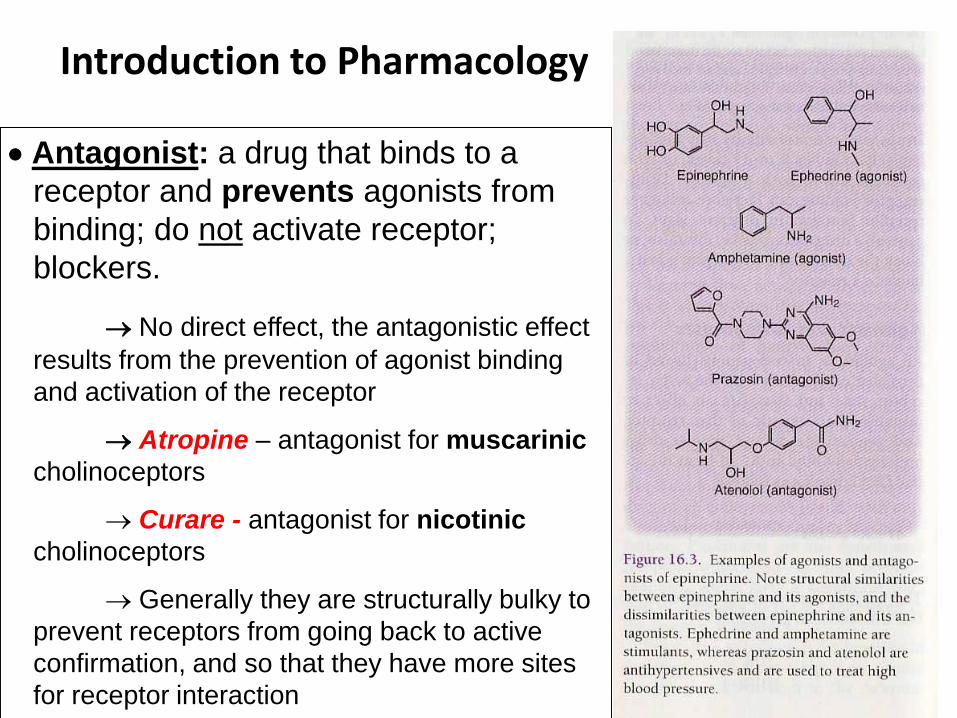
Antagonist: a drug that binds to a
receptor and prevents agonists from
binding; do not activate receptor;
blockers.
No direct effect, the antagonistic effect
results from the prevention of agonist binding
and activation of the receptor
Atropine – antagonist for muscarinic
cholinoceptors
Curare - antagonist for nicotinic
cholinoceptors
Generally they are structurally bulky to
prevent receptors from going back to active
confirmation, and so that they have more sites
for receptor interaction

17
Introduction to Pharmacology
18
Partial Agonist: a drug that binds to a receptor and activates it,
but the effect is not as great as with a full agonist.
Are agonists if no full agonist is present; are antagonists if a full
agonist is present
Pindolol – partial β receptor agonist
Inverse Agonist: a drug that binds to a receptor and stabilizes it
in the inactive conformation.
Constitutively active receptors – active without binding to agonist
Many drugs that act as competitive
antagonists are really partial agonists
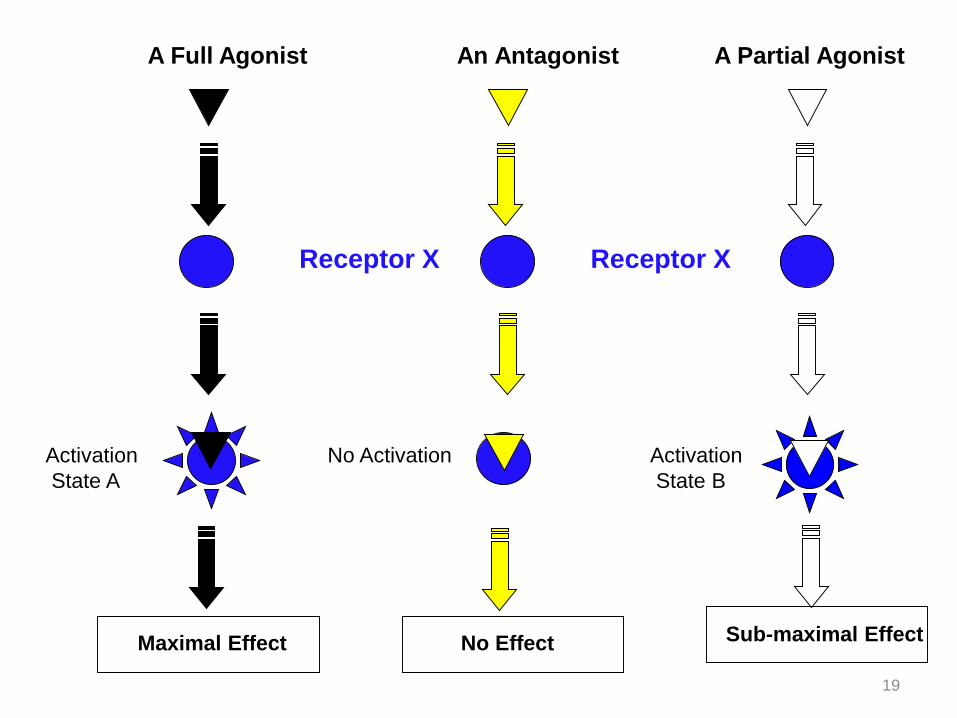
19
An Antagonist
No ActivationActivation
State A
Receptor X
A Full Agonist A Partial Agonist
Activation
State B
Receptor X
Maximal Effect No Effect Sub-maximal Effect
Introduction to Pharmacology
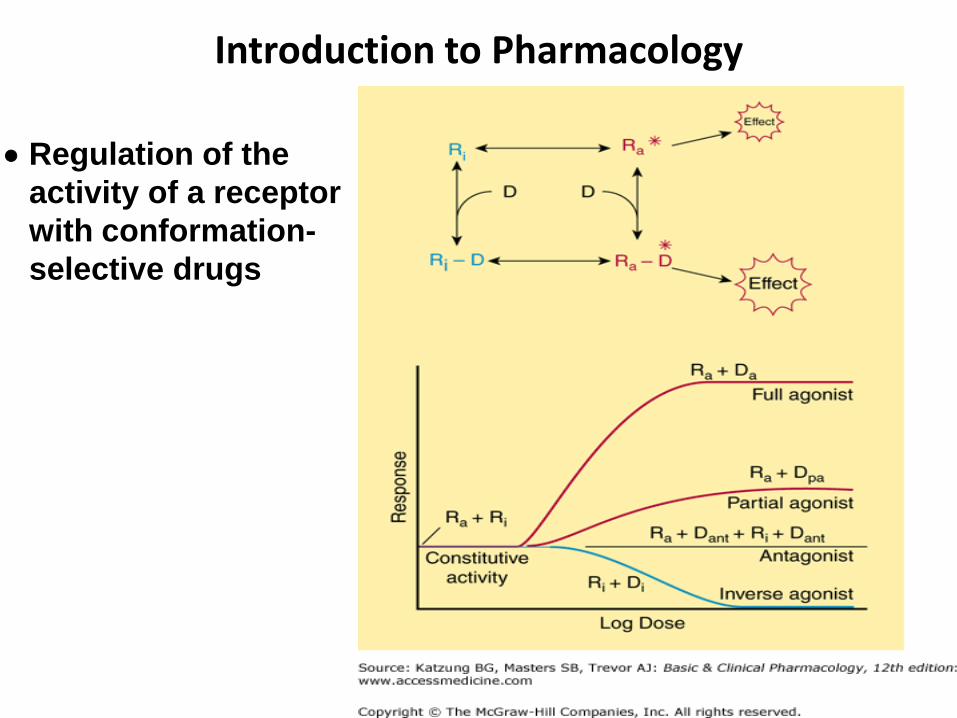
20
Regulation of the
activity of a receptor
with conformation-
selective drugs
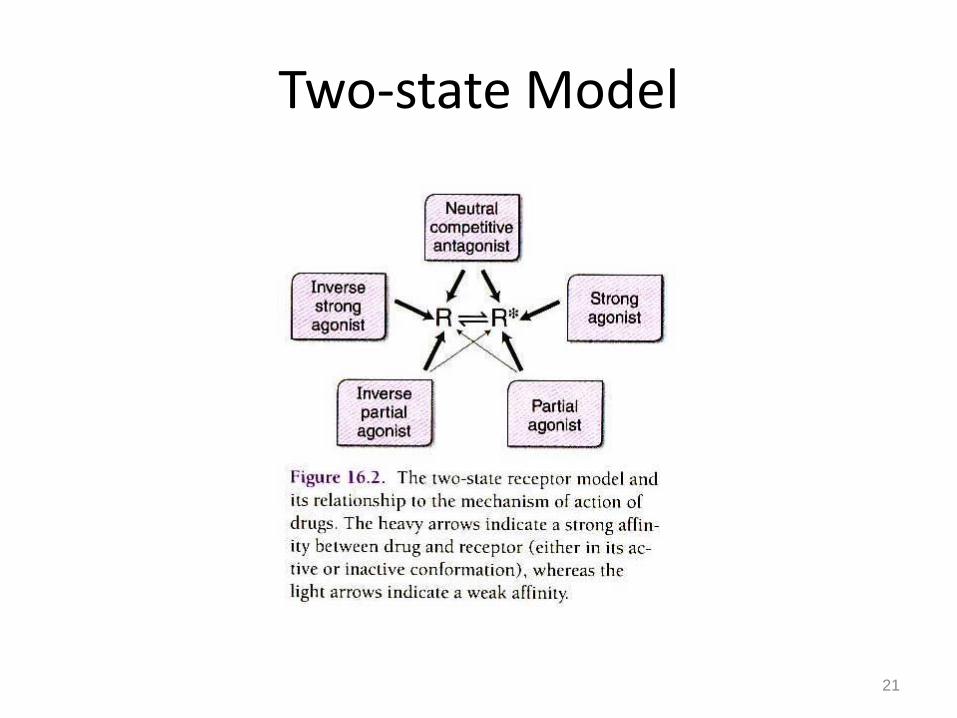
Two-state Model
21
Rinactive Ractive

10 Rinactive 10 Ractive

10 Rinactive 10 Ractive
Add 8 INVERSE AGONISTS that bind to
inactive receptor molecule and stabilize it
2 Rinactive 10 Ractive
New equation
6 Rinactive 6 Ractive
4 Active Receptors are converted to 4 inactive
6 Rinactive 6 Ractive
Fewer active receptors with constitutive activity
A Little Background on Drugs
28
A drug is a substance that brings about a change
in biologic function through its chemical actions.
Sources
Endogenous
Exogenous (xenobiotics)
States
Solids
Liquids
Gases
Size
Vast majority of drugs have a MW between 100 – 1000
MW 100 helps achieve selective receptor binding
MW 1000 inhibits diffusion-mediated distribution
= Chemicals foreign to the biological
system in question
Drugs do not create effects they modulate
function

Drug Receptors & Pharmacodynamics
29
Receptors:
1.) Determine the quantitative relations between dose or
concentration of drug and pharmacologic effects
receptor number in various target tissues
2.) Are responsible for selectivity of drug action
Affinity – determined by chemical forces that cause drug
to bind to the receptor
Efficacy – change in confirmation toward the active state
Intrinsic activity – ability to evoke maximal effect after
binding
3.) Mediate the actions of both pharmacologic agonists and
antagonists
receptor classes, subtype, and isoforms
Receptor:
Class α β
Subtype α1 α2
Isoforms α1a α1b
30
31
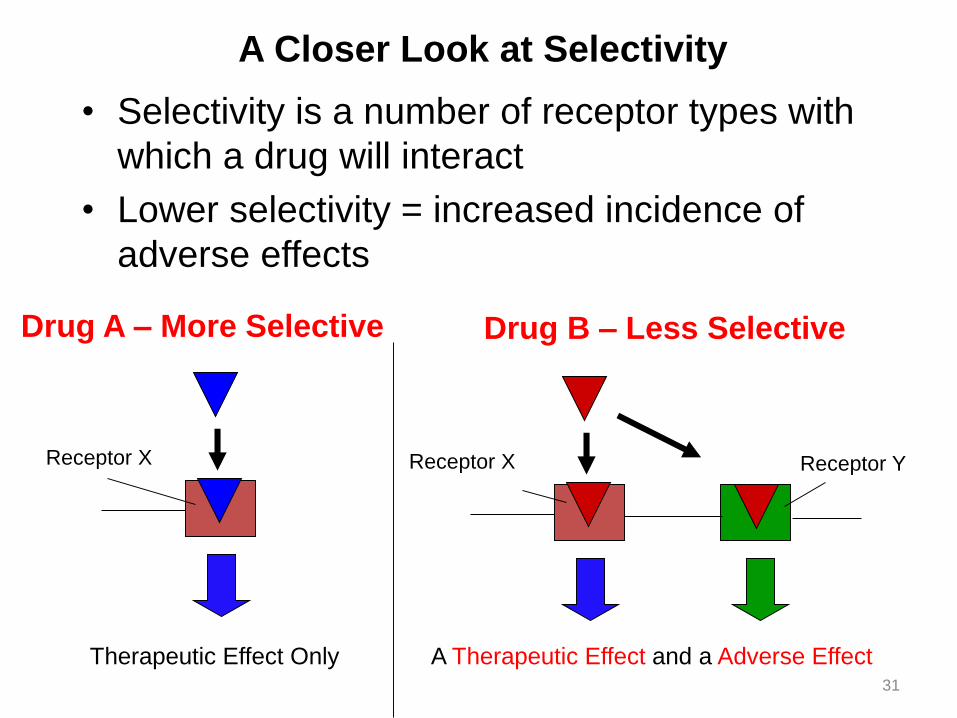
A Closer Look at Selectivity
• Selectivity is a number of receptor types with
which a drug will interact
• Lower selectivity = increased incidence of
adverse effects
A Therapeutic Effect and a Adverse EffectTherapeutic Effect Only
Drug A – More Selective
Receptor X Receptor X Receptor Y
Drug B – Less Selective
32
A Closer Look At Affinity
• The affinity of a drug for a receptor describes
how readily and tightly that drug binds to its
receptor
– High affinity = good drug-receptor interaction;
LESS drug needed to produce a response
– Low affinity = poor drug receptor interaction;
MORE drug needed to produce a response
Example:
Affinity for mu opioid receptor:
fentanyl > morphine > meperidine
Dose typically used for analgesia:
fentanyl: 0.1 mg; morphine: 10 mg; meperidine: 100 mg

33
Intrinsic activity describes the ability of a drug to activate a receptor and produce a physiological response when it binds to a receptor
•Agonists: bind to the receptor and activate it, producing a physiological response
–Have intrinsic activity•Antagonists: Receptor antagonists bind to the receptor but do not change its function. However, they prevent activation by endogenous chemicals or other drugs
–Do not have intrinsic activity
A Closer Look At Intrinsic Activity
Some drug’s MOA do not involve receptors:
antacids, osmotic diuretics
34
Types of Receptors
35
Regulatory Proteins:
Mediate actions of most drugs and endogenous chemicals
(neurotransmitters, hormones, autocoids)
Best characterized
Enzymes:
Usually through inhibition
Methotrexate inhibits dihydrofolate reductase
Transport Proteins:
Digoxin inhibits Na+, K+ ATPase
Structural Proteins:
Colchicine inhibits tubulinPrevents polymerization of microtubules
Aspects of Drug Receptor Function
36
Relationship between drug concentration (dose) &
pharmacologic response
Relationship Between Dose & Response
37
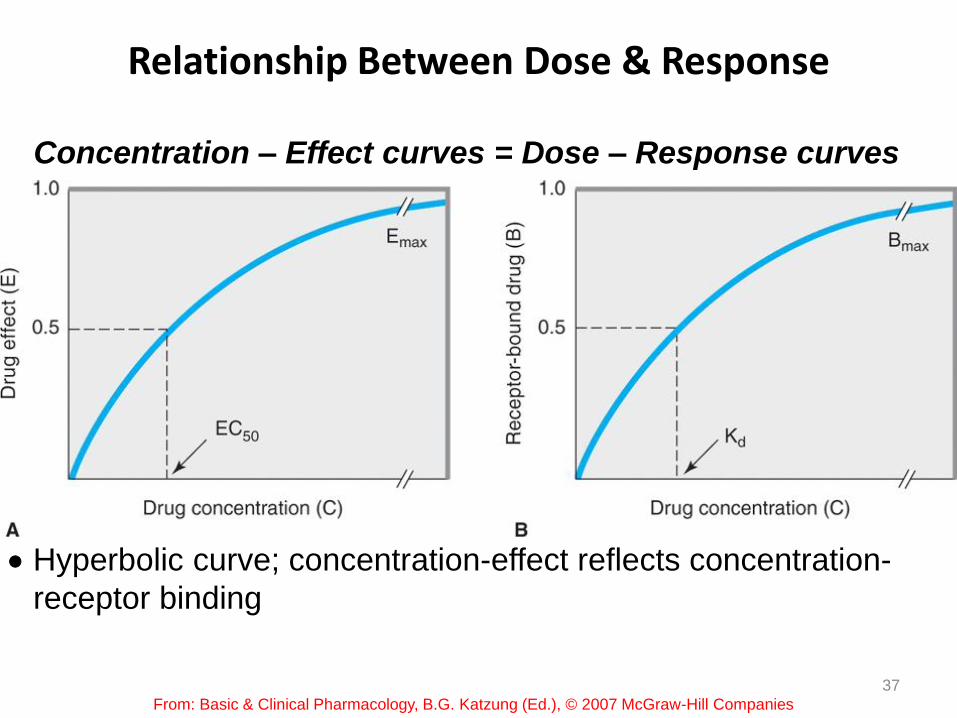
Concentration – Effect curves = Dose – Response curves
From: Basic & Clinical Pharmacology, B.G. Katzung (Ed.), © 2007 McGraw-Hill Companies
Hyperbolic curve; concentration-effect reflects concentration-
receptor binding

Occupation theory
Magnitude of pharmacological effect is proportional to percentage of
receptors occupied
38
Relationship Between Dose & Response
39
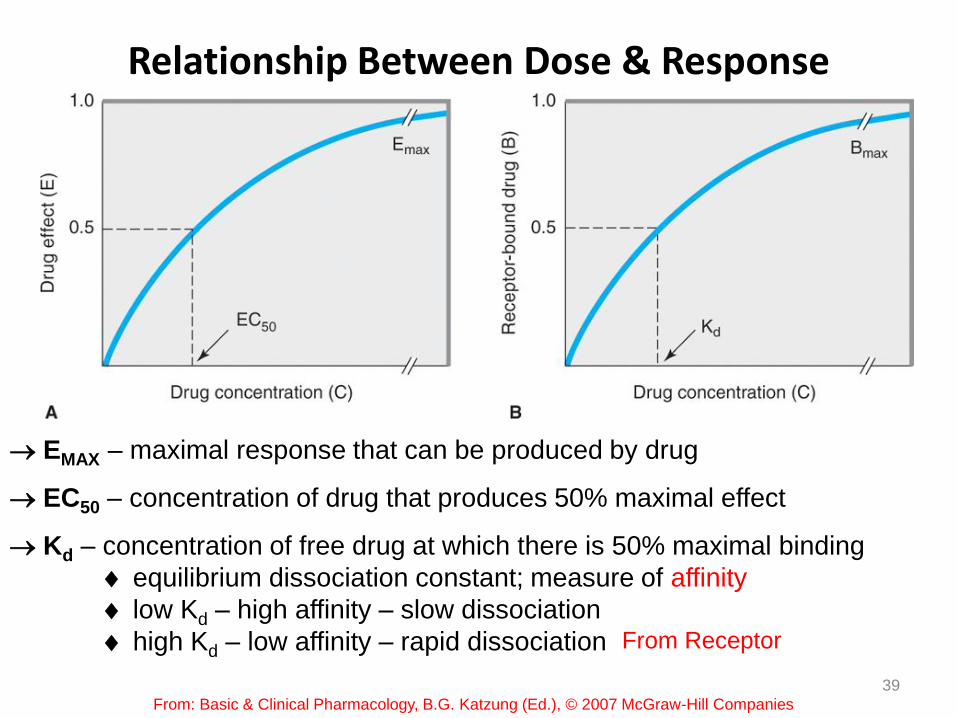
EMAX – maximal response that can be produced by drug
EC50 – concentration of drug that produces 50% maximal effect
Kd – concentration of free drug at which there is 50% maximal binding
equilibrium dissociation constant; measure of affinity
low Kd – high affinity – slow dissociation
high Kd – low affinity – rapid dissociation
From: Basic & Clinical Pharmacology, B.G. Katzung (Ed.), © 2007 McGraw-Hill Companies
From Receptor
Relationship Between Dose & Response
40
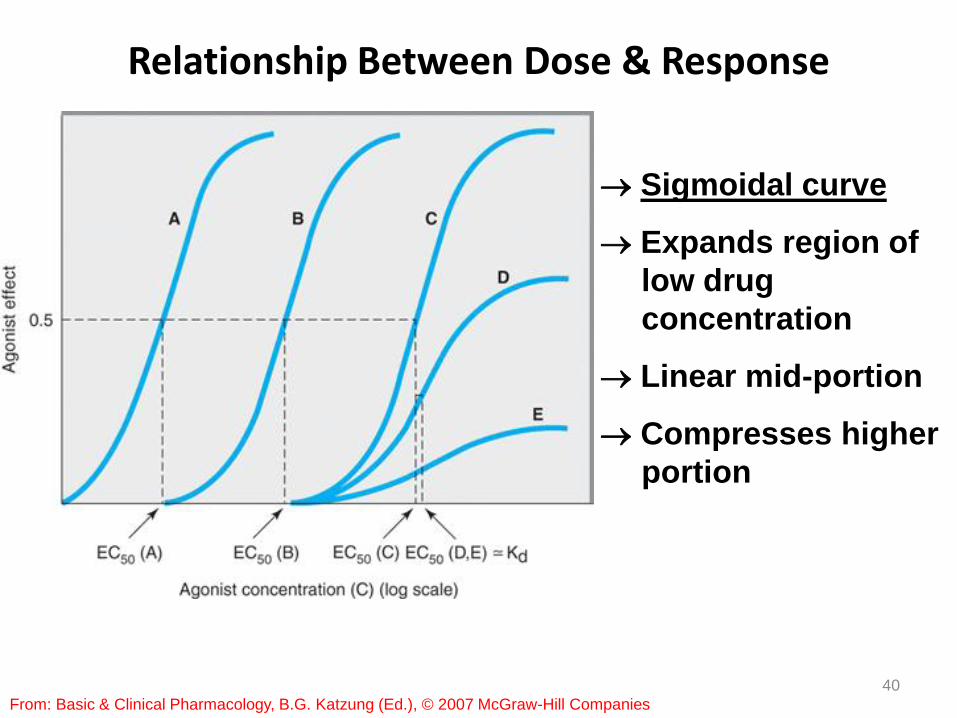
From: Basic & Clinical Pharmacology, B.G. Katzung (Ed.), © 2007 McGraw-Hill Companies
Sigmoidal curve
Expands region of
low drug
concentration
Linear mid-portion
Compresses higher
portion

Relationship Between Dose & Response
• Receptor-Effector Coupling: Transduction process between occupancy & drug response
Coupling efficiency based on
1.) extent of conformational change (full agonist-full response, partial agonist-partial response) and
2.) biochemical events that transduce occupancy into response
41
Relationship Between Dose & Response
42From: Basic & Clinical Pharmacology, B.G. Katzung (Ed.),
© 2007 McGraw-Hill Companies
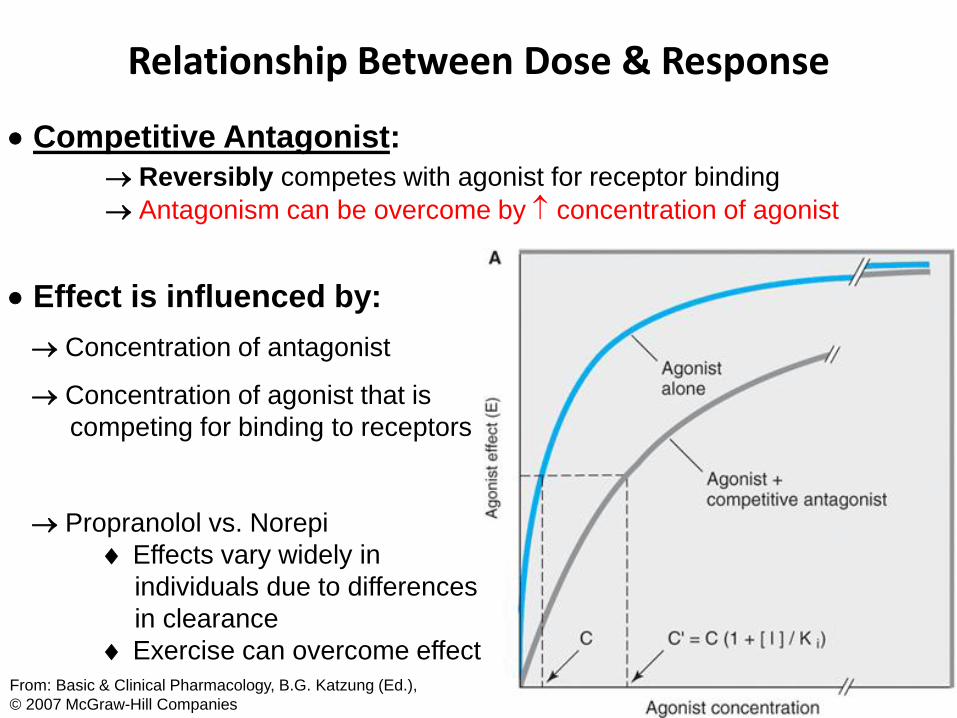
Competitive Antagonist:
Reversibly competes with agonist for receptor binding
Antagonism can be overcome by concentration of agonist
Effect is influenced by:
Concentration of antagonist
Concentration of agonist that is
competing for binding to receptors
Propranolol vs. Norepi
Effects vary widely in
individuals due to differences
in clearance
Exercise can overcome effect
Relationship Between Dose & Response
43From: Basic & Clinical Pharmacology, B.G. Katzung (Ed.),
© 2007 McGraw-Hill Companies
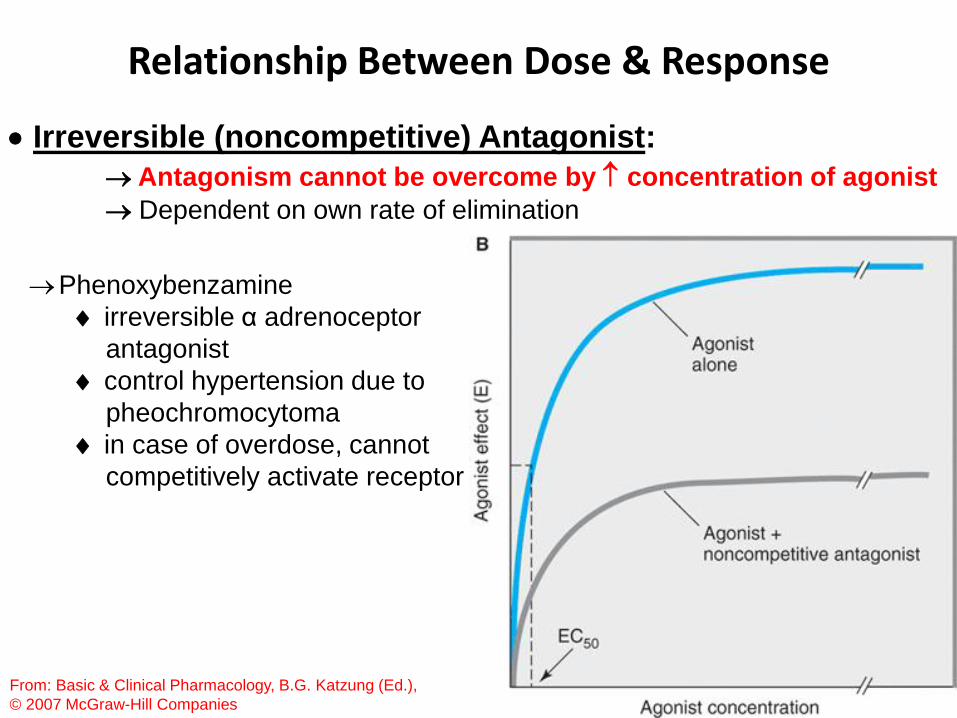
Irreversible (noncompetitive) Antagonist:
Antagonism cannot be overcome by concentration of agonist
Dependent on own rate of elimination
Phenoxybenzamine
irreversible α adrenoceptor
antagonist
control hypertension due to
pheochromocytoma
in case of overdose, cannot
competitively activate receptor

Relationship Between Dose & Response
44
From: Basic & Clinical Pharmacology, B.G. Katzung (Ed.), © 2007 McGraw-Hill Companies
Full agonist at
single
concentration
Full agonist at
single
concentration
Relationship Between Dose & Response
45
Allosteric Antagonist:
Binds to another part of the molecule
Chemical Antagonist:
A drug may bind to and inactivate another drug
Protamine used to counteract heparin
Desferrioxamine chelates iron
Physiological Antagonist:
One type of functional antagonism – agonists that oppose via action
on a different receptor or system
Use of a separate endogenous regulatory pathway
Glucocorticoids vs. insulin in controlling blood glucose
Effects are less specific & more difficult to control

46
Aspects of Drug Receptor Function
47
Relationship between dose and clinical response
Relationship Between Dose & Clinical Response
48
Maximal benefit with minimal toxicity
Graded dose-response relationship:
Potency – EC50 or ED50 (dose needed for 50% of drug’s maximal
effect)
Dependent on affinity (Kd) and
Efficiency of coupling response
Maximal efficacy – limit of the dose-response relationship;
important for clinical effectiveness
Dependent on ability to reach relevant receptors
Route of administration, absorption, site of action
Relationship Between Dose & Clinical Response
49From: Basic & Clinical Pharmacology, B.G. Katzung (Ed.), ©
2007 McGraw-Hill Companies
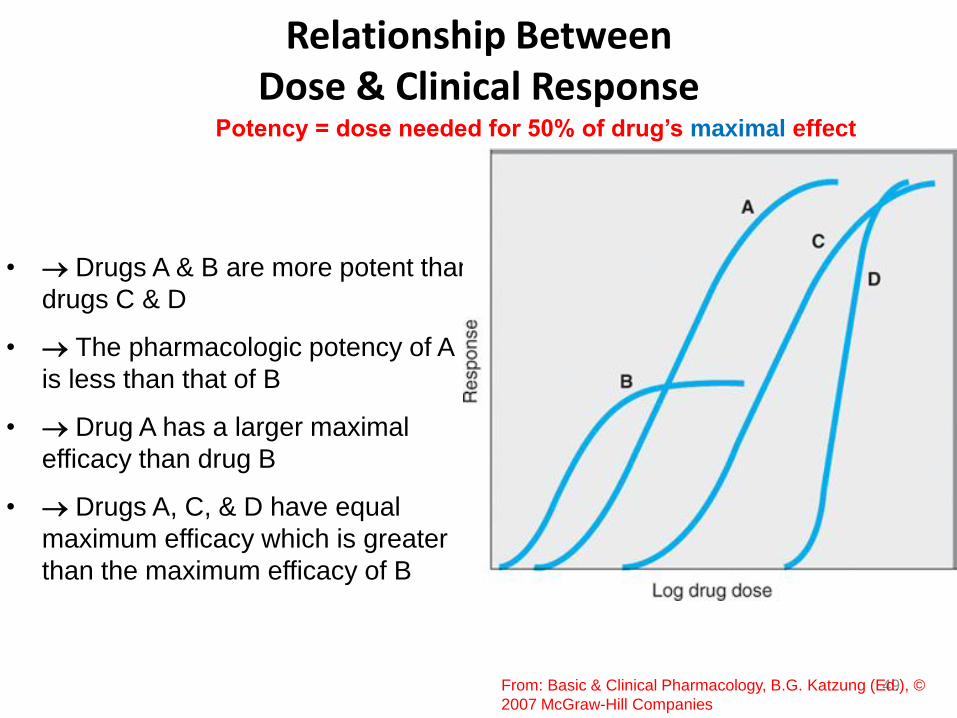
• Drugs A & B are more potent than
drugs C & D
• The pharmacologic potency of A
is less than that of B
• Drug A has a larger maximal
efficacy than drug B
• Drugs A, C, & D have equal
maximum efficacy which is greater
than the maximum efficacy of B
Potency = dose needed for 50% of drug’s maximal effect
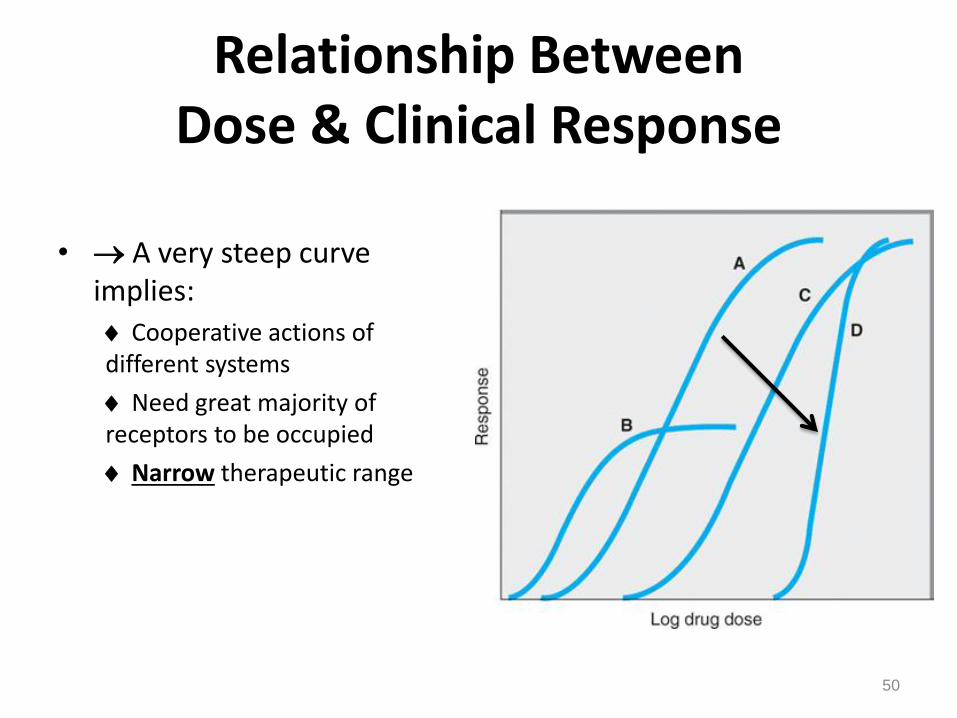
Relationship Between Dose & Clinical Response
• A very steep curve implies:
Cooperative actions of different systems
Need great majority of receptors to be occupied
Narrow therapeutic range
50
51
More
potent
Less
potent
More Less
Log dose
Inte
nsit
y o
f re
sp
on
se
50%
1 100
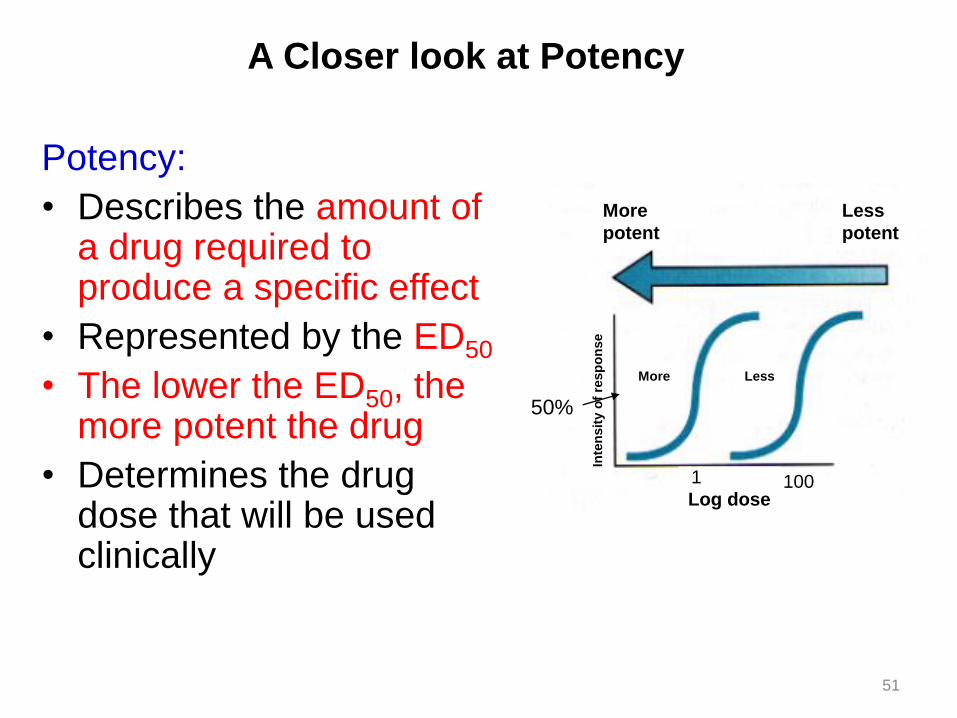
A Closer look at Potency
Potency:
• Describes the amount of a drug required to produce a specific effect
• Represented by the ED50
• The lower the ED50, the more potent the drug
• Determines the drug dose that will be used clinically
52
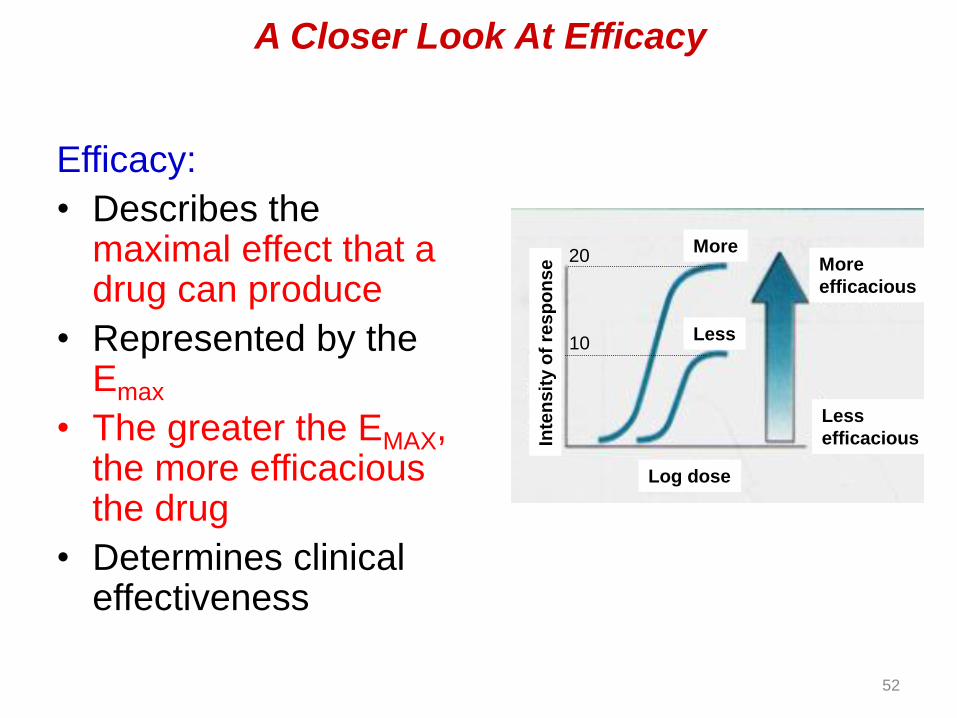
Efficacy:
• Describes the maximal effect that a drug can produce
• Represented by the Emax
• The greater the EMAX, the more efficacious the drug
• Determines clinical effectiveness
1
Inte
ns
ity o
f re
sp
on
se
Log dose
More
Less
More
efficacious
Less
efficacious
20
10
A Closer Look At Efficacy

53
Relationship Between Dose & Clinical Response
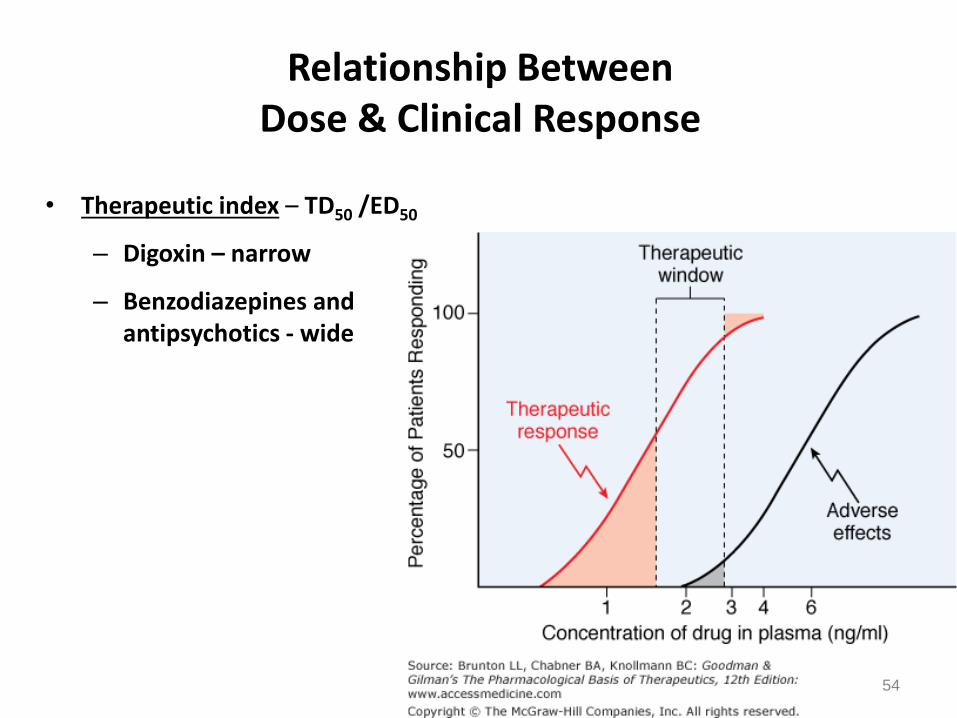
• Therapeutic index – TD50 /ED50
– Digoxin – narrow
– Benzodiazepines and antipsychotics - wide
54

Cumulative Quantal Dose-response Curve and Drug Safety Indices
• Therapeutic window – the range of doses of a
drug or of its concentration in a bodily system
that provides safe and effective therapy
55
Narrow vs. wide therapeutic
window

The clinically acceptable risk of toxicity depends critically on the
severity of the disease being treated
56
Relationship Between Dose & Clinical Response
57
Variation in drug responsiveness:
Clinical response in individual patients
Idiosyncratic – infrequently observed in most patients
Genetic differences in metabolism
Immunological differences
Hypersensitivity – true allergy (uncommon)
Hyperreactive – intensity of effect is increased vs. that in most
individuals
Hyporeactive – intensity of effect is decreased vs. that in most
individuals
Tolerance – responsiveness decreases as a consequence of
continued drug administration
Tachyphylaxis – decreased responsiveness that occurs rapidly
after administration of a drug

Relationship Between Dose & Clinical Response
58
Four mechanisms contribute to
variation in drug responsiveness
1.) Alteration in concentration of drug that reaches receptor
2.) Variation in concentration of endogenous receptor ligand
3.) Alteration in number or function of receptors
4.) Change in responsiveness distal to receptor
1.) Alteration in concentration of drug that reaches receptor
Dose
ADME
59
2.) Variation in concentration of endogenous receptor ligand
• Saralasin – weak partial agonist at angiotensin II receptors
• Angiotensin II is a potent vasoconstrictor– What would be its effect on blood pressure up or down?
• What would be the effect on blood pressure of giving saralasin to a patient with high levels of angiotensin?
• What would be the effect on blood pressure of giving saralasin to a patient with low levels of angiotensin?
60

3.) Alteration in number or function of receptors
• Up-regulation (thyroid hormone increases receptors in heart; antagonists like -blockers also do this)
– Stop antagonist – increase in receptor number - response to endogenous ligand (need to wean)
• Down-regulation
– Stop agonist – may have too few receptors to get effective stimulation
61
3.) Alteration in number or function of receptors
Pharmacogenomics (or pharmacogenetics) is the study of the genetic variations that cause differences in drug response among individuals or populations. Future clinicians may screen every patient for a variety of such differences before prescribing a drug.
62
4.) Change in responsiveness distal to receptor
• Largest and most important class of mechanisms that cause variation in responsiveness to drug therapy
• Age
• General health
• Severity & pathophysiology of disease
• Wrong diagnosis
• Compensatory mechanisms - (baroreceptor reflex after administration of an anti-hypertensive agent)
63
Relationship Between Dose & Clinical Response
64
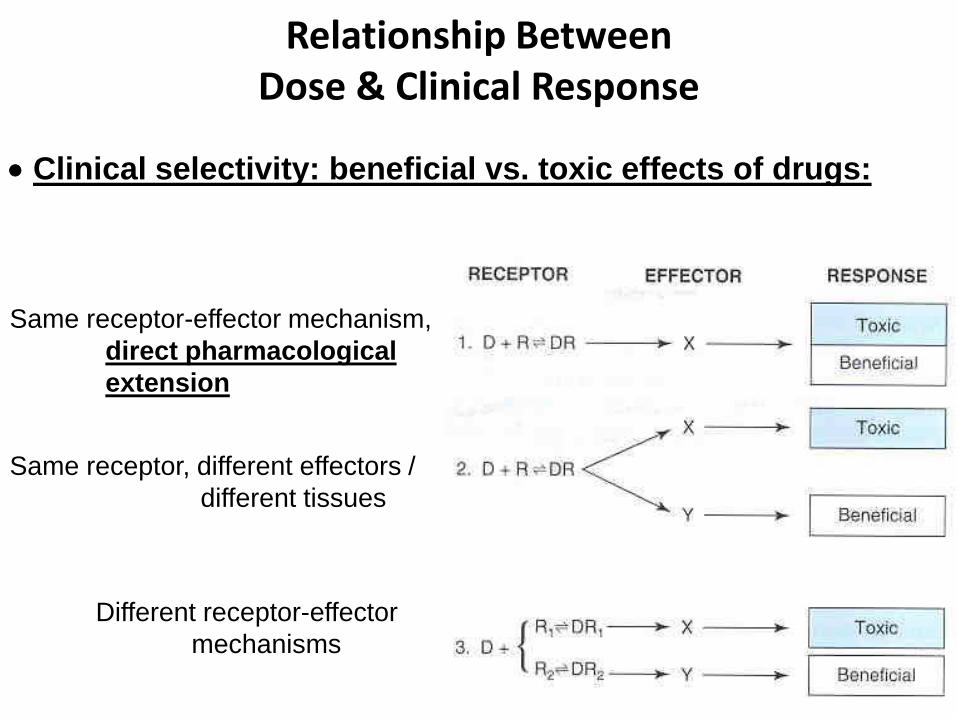
Clinical selectivity: beneficial vs. toxic effects of drugs:
Same receptor-effector mechanism,
direct pharmacological
extension
Same receptor, different effectors /
different tissues
Different receptor-effector
mechanisms
Relationship Between Dose & Clinical Response
65
Strategies for lowering adverse effects:
Use lowest dose possible
Add an adjunctive drug that acts on a different receptor mechanism
Anatomical selectivity – refine administration to get more drug to site
of action
No drug causes only a single, specific effect
66

Drugs are selective, not specific
67