jason zurba bsc rrt supervisor royal columbian...
TRANSCRIPT

Jason Zurba BSc RRT
Supervisor Royal
Columbian Hospital

Outline
• Why we started looking at this
• What our own data has shown us
• What the literature tells us about intubation
• What we have changed
• How this applies to Neonates

Royal Columbian Hospital Airway Committee
Respiratory
Therapists
Physicians:
ICU
Emergency
Anesthesia
Administration
Nursing

Mandate
Leave your ego at
the door
Airway Incidents
Equipment
Protocols
Education

Intubation Data Collection
at Royal Columbian
Hospital



July 2012 to November 2014
582 DOCUMENTED INTUBATIONS

INDICATIONS
RESP FAIL
DEC LOC
SHOCK
OTHER
NO DATA

Urgency

BVM Class

Techniques

Complications
Severe:
SBP <70mmHg if >90 mmHg
O2 Sat’n <80% if >90%
Esophageal intubation
Other: aspiration, dental trauma,
endobronchial intubation, pneumothorax
Cardiac Arrest or Death

Key findings
1. Others Complications: Aspiration, dental trauma, endobronchial intubation,
pneumothorax or any severe complication
2. Severe Complication:
- Hypotension: Systolic blood pressure <70mmHg if >90mmHg prior to attempt
- Hypoxia: oxygen saturation <80% if >90% prior to attempt
-Esophageal intubation
-Cardiac Arrest
-Death within 30 Min of Intubation
1 Attempt (n =224 ) >1 Attempt (n=108)
%
Other Complications 20 44
8.9% vs 41%
Severe Complications 18 32
8.0% vs 30%

Greater than one attempt at ETI was associated
with a 4-fold increase in severe, and a 5-fold
increase in total complications.
Although previous publications found greater
than 2 attempts associated with increased
complications, recent publications found this
association with greater than one attempt,
consistent with our findings.

Should RTs be intubating?
A. Yes, of course
B. No, are you nuts?
Is It just Us? Do we Just Suck at Intubation at RCH ?
Fiberoptic intubation gone horribly wrong

Do we suck at RCH?
A. Yup, you suck
B. Nope, that sounds
normal
C. Nope, you guys are
some kind of A/W
wizards
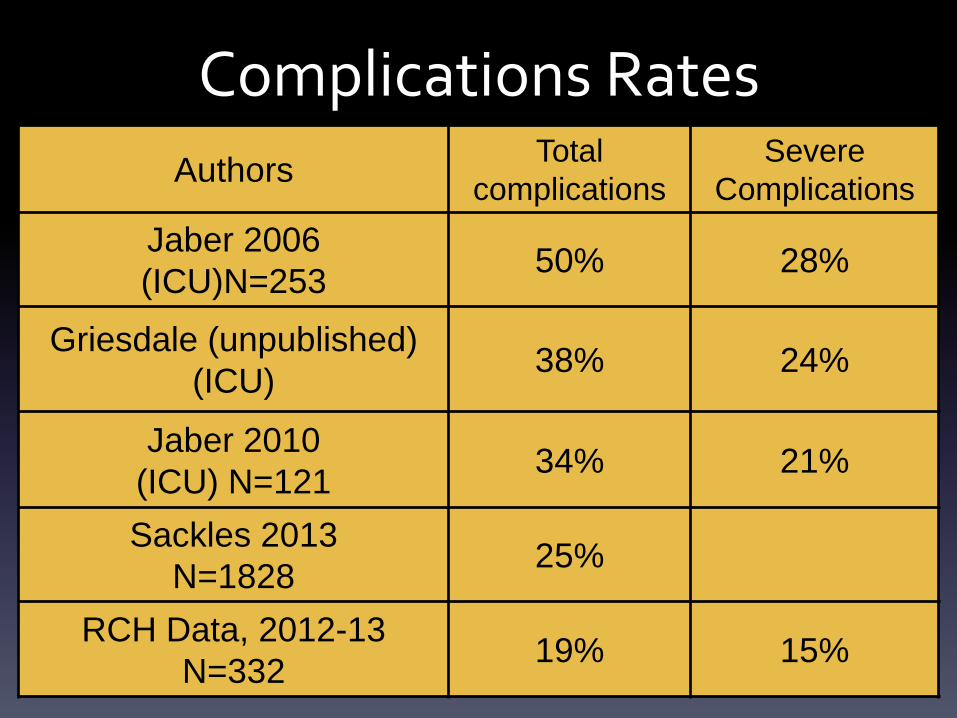
Complications Rates
Authors Total
complications
Severe
Complications
Jaber 2006
(ICU)N=253 50% 28%
Griesdale (unpublished)
(ICU) 38% 24%
Jaber 2010
(ICU) N=121 34% 21%
Sackles 2013
N=1828 25%
RCH Data, 2012-13
N=332 19% 15%

How do we measure up to others

Authors
Absolute
Risk of Adverse
Event
Griesdale 2008
n=136 18% 38%
Sackles 2013
n=1828 14% 53%
RCH Data
n=332 8% 41%
Complications Increase with >1 Attempt

• Prospective cohort study of pts intubated by ICU
team
• N=136
• Excluded Cardiac arrest pts
• >1 attempt associated with ↑ risk of severe
complications OR 3.31 (95% CI:1.30,8.40, p=0.01)

• Retrospective analysis of 4 years of QI data
• N=1828
• 1 attempt complications 14.2% (95% CI12.4%-16.2%
• >1 attempt complications 47.2%(95% CI 41.8%-52.7%)


What are some things we can fix?

• First pass success
– PGY-1 38%
– PGY-2 52%
– PGY-3 66%
– Anesthesia Resident 85%
• Higher year of training RR .74 95%[CI] .54-.93 P<.01
• Anesthesia Resident RR .52 95%[CI] .2-1 P=.03

Lessons
• People with more experience have better
success

• N=322
• Anesthesia Residents out of OR intubations
– Complications decreased with attending
Supervision
– 21.7% vs 6.1% P=.0001

Lesson
• Anesthetists are the experts

So….. How many intubations does it take to become good?

How many Intubations should you do to show competency
A. 5
B. 10
C. 20
D. 30
E. >30

• 57 successful intubations to have 90% success rate
• Still improving into the 80s

• 472 intubations by 20 trainees (msi, RT, EMT)
• All pts prescreened to be easy intubations
• Analysis of data predicted 90% success after 47 intubations
• “existing Direct laryngoscope intubation training…..is
inadequate for non-anaesthesia healthcare workers”
• “Emphasis should be placed on effective ventilation and
oxygenation using BVM”

• Small number of ER residents (3)
• 342 intubations over 2 years
• 74.7 intubations to achieve 90% successful
intubation (95% CI 62.0-87.3)

Lesson
• RT intubation competency programs are
probably not adequate.
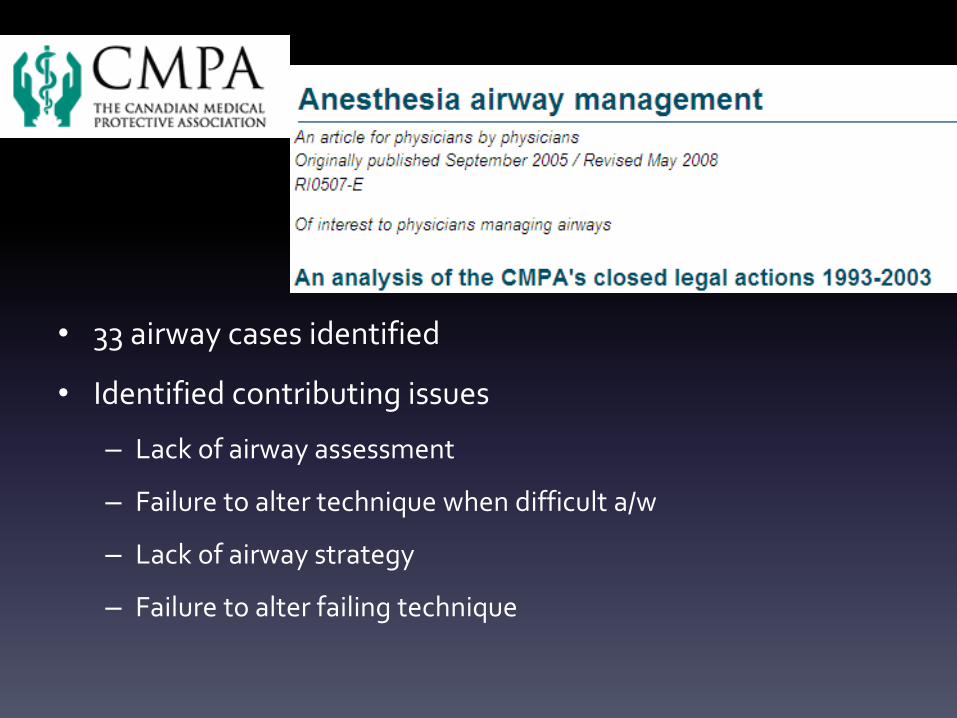
• 33 airway cases identified
• Identified contributing issues
– Lack of airway assessment
– Failure to alter technique when difficult a/w
– Lack of airway strategy
– Failure to alter failing technique

Lessons • Assess
• Plan and communicate an airway strategy
• If it looks tough, do something different
• If something isn’t working, don’t do it again

• With anticipated DTI 70% anesthetists didn’t
change technique
– > 60% progressed to CICV
• SGA regularly rescued failed intubation
• Transtracheal jet high complications rate of
death when used as rescue

Lesson
• Change technique for difficult A/W
• Don’t use transtracheal jet
• SGAs are pretty cool

How many of you regularly see DL fail during intubation and the second attempt is DL again?

• When first attempt DL unsuccessful, repeated
DL 80% failure rate.
• Recommend identification and detailing difficult
A/W details

Lesson
• If it isnt working, don’t keep doing it no matter how
tempting
• Clearly identify Difficult A/W

• Previous difficult intubation (DTI) 6 times more likely to be DTI again
• Previous failed intubation 22 times more likely to fail again.
• As a result of findings Denmark created database

Lesson • Clearly identify people with difficult A/W
• Listen if someone says it was difficult

But I Gotta Intubate! It’s an Emerrrrrrgency!
They Can Usually Wait
• Less than 1/3 of our pts were “Emergent”
• Intubations of Critically ill are usually urgent,
not emergent (Griesdale 2011)

• N=649,359
• Favourable Neurological outcome;
– Intubation
– SGA
– BVM

• N=649,359
• Favourable Neurological outcome;
– Intubation 1.0% (95% CI 0.9%-1.1%)
– SGA 1.1% (95% CI 1.1%-1.2%)
– BVM 2.9%(95% CI 2.9%-3.0%)

Lesson
• It may be better to use BVM than intubate (at
least in cardiac arrest)

But what if I can’t manually ventilate them?

• 4 year observational study
• N=53,041
• 77 cases of impossible mask ventilation
• Only 19 of these were difficult a/w

Lesson • Impossible mask ventilation is extremely rare.
• Even if you do meet them, they will probably be easy to intubate

• N=128
• Apneic oxygenation Decreased desaturation during
intubation absolute risk reduction 16.7% P=0.016

Lesson
• Apneic oxygenation may further decrease
your risk of desaturation during intubation

What if you put it all together?

• Two phase Multi-center
• Use of Intubation Bundle – Preoxygenation, 2 operators, RSI, Cricoid, EtCO2,
Protective ventilation, Fluid loading
• N=244 (123 before, 121 after) – ↓life threatening complications 34%-21%
– ↓other complications 21%-9%

Griesdale et al 2011 (unpublished) Use of a checklist
Serious
Complication

Lesson
• Use a checklist, they work!

307 Hospitals
4 Countries
1 year
Prospective
ICU, ED, OR
Airway Cases:
Death
Brain Damage
Unexpected ICU

NAP 4
• 4 Common themes identified
– 1) Lack of airway assessment
– 2) Lack of airway strategy
– 3) Avoidance of awake techniques
– 4) The failure to plan for Failure: repeated
attempts using the same people/equipment
NAP 4 • 98/133 no documented airway exam
• 66 ‘may be difficult’-1 change in airway strategy
• needle Cricothyrotomy: 64% (16/25) Failure
Rate
• Failure to use capnography implicated in 82% of
ICU airway deaths and brain damage

NAP4 Recommendations • Develop a checklist for intubation
• Standardize Difficult A/W equipment
• Including SGA and Aintree catheters
• Do more awake FOB intubations
• Investigate A/W critical incidents
• Appoint an A/W lead anesthetist in all institutions.
• Capnography is mandatory

NAP4 Reccomendations
• Identify Difficult A/W patients
• Establish good communication between ICU,
ER, and Anesthesia
• Establish clear lines of communication to
escalate A/W events to individuals with
appropriate skills.

What have we done so far
Difficult Airway Recognition • Blue wrist band
• Blue sign for HOB
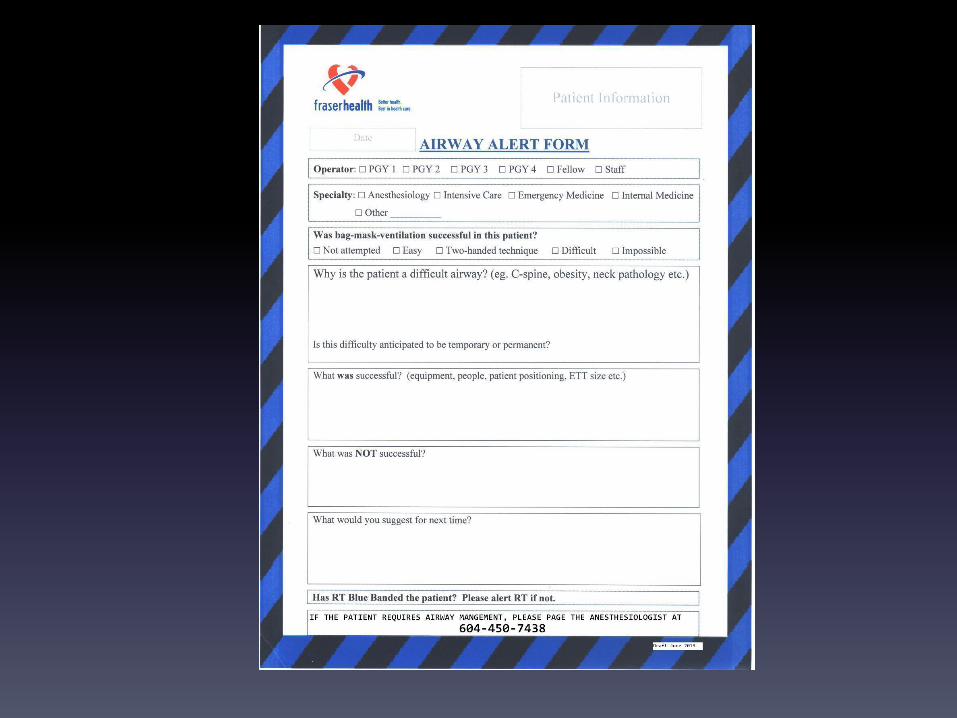
• Airway Alert form

• 24 hour a day response from a rover
Anesthesiologist for difficult airways
• Empowered any member of team to
escalate airway emergencies

• ETCO2 monitoring at every
intubation
• Standardize difficult intubation
equipment
• Standardize intubation procedure
– Preprinted orders

Date (dd/mm/yyyy) Time Prescriber Signature Printed Name or College ID#
Pre-printed Orders:
Intubation Royal Columbian Hospital (trial)
Form ID: Rev: April 10th 2014 Page: 1 of 1
DRUG & FOOD ALLERGIES
l Mandatory o Optional: Prescriber check (P) to initiate, cross out and initial any orders not indicated.
1. PREPARATION- PRE-INTUBATION
· Airway Competent MD, RT and RN present · Airway equipment present and consideration for adjuncts discussed · Planned strategy for intubation verbally communicated to all team members (see back)
Airway assessment and positioning completed: · Assess for contraindications prior to positioning (e.g. any cervical spine instability?)
· Sniffing position required? (e.g. Troop pillow, flannels/pillows) · Potential for difficult airway discussed with team
Breathing and Pre-oxygenation
· Apneic oxygenation (15lpm nasal prongs) · Assisted Bag Valve Mask
¨ Non-Invasive Ventilation (NIV) as ordered by MD
Circulation:
· RN to ensure patent IV and all medications are prepared prior to start.
· IV 500 mL SODIUM CHLORIDE 0.9% bolus over 15 mins
· Monitor BP Q 3 min during and for 20 min post intubation medications and until stable
o NOREPINEPHRINE Infusion at 5 mcg/min if MAP less than 60 mmHg
o PHENYLEPHRINE 50 to 100 mcg IV PRN
2. INTUBATION (consider standardized medications):
o Rapid Sequence Induction (RSI) Patient weight:
Induction / Analgesia Agents:
¨ ETOMIDATE 0.3 mg/kg IV (Prepare 20mg in syringe) ¨ KETAMINE 1.5 to 2.0 mg/kg IV (Prepare 200 mg in syringe)
¨ Fentanyl 1 to 2 mcg/kg (Prepare 250mcg in syringe) ¨ Other:
Neuromuscular Blockade: o SUCCINYLOCHOLINE 1.5 mg/kg IV Prepare: mg IV
o ROCURONIUM 1 mg/kg IV Prepare: mg IV
o Awake Intubation
¨ GLYCOPYRROLATE 0.4 mg IV
· Topicalization with Lidocaine 5ml/kg o KETAMINE 0.25 to 0.5 mg/kg IV PRN Prepare: mg IV PRN ¨ MIDAZOLAM 0.05 mg/kg IV PRN Prepare: mg IV PRN
3. POST- INTUBATION
· Confirm placement with waveform CO2 and auscultation · CXR
· Was this a difficult Airway? If yes, RT to ensure Difficult Airway Bundle implemented
Psychiatric consultant: Time Notified:
Diagnosis: Psychiatric
Medical
DRAFT


So…. Should RTs be intubating ?
• If our competency programs are inadequate
• We often don’t do enough intubations to maintain
competency
• Dealing with failed A/W is beyond our scope
• We are unable to do awake fiberoptic intubations
• Open cricothyrotomy is beyond our scope
• Greater than one attempt significantly increases severe
complications

So…..Should RTs intubate?
A. Yes
B. No
How have the initiatives worked so far?

Difficult airway identification system
• Has been huge success.
• Every difficult airway (?) is being labelled and
documented
• FHA is adopting system

Extubation of Difficult A/W
• Empowered RTs to refuse orders to extubate
difficult airways
• Identified difficult A/W require anesthetist to
be present for extubation

So, how has the order set worked?
• In 11 months we have had 17 uses of the order
set
• Approx 10% usage

What about babies? Maybe RTs should intubate babies?

Neonatal ETI
• Data collection cards now kept in NICU
• Overall complication rates 54%
• Complication rates with 1st pass success 29%
• Complication rates increase to 83% thereafter

Complications with Intubation

Maybe we suck at intubating babies?

• 5 level 3 NICUs
• One year study 2011
• 455 ETI attempts 203 patients

• Neonatal ETI Low frequency, High-stakes events
• Success rates poor (at best 72%)
• 60% decompensation+esophageal
• Providers with more experience more successful


Going to get worse
• No routine intubations for meconium
• No longer ethical to practice after death
• Working hours for DRs reduced
• Reduction in invasive ventilation

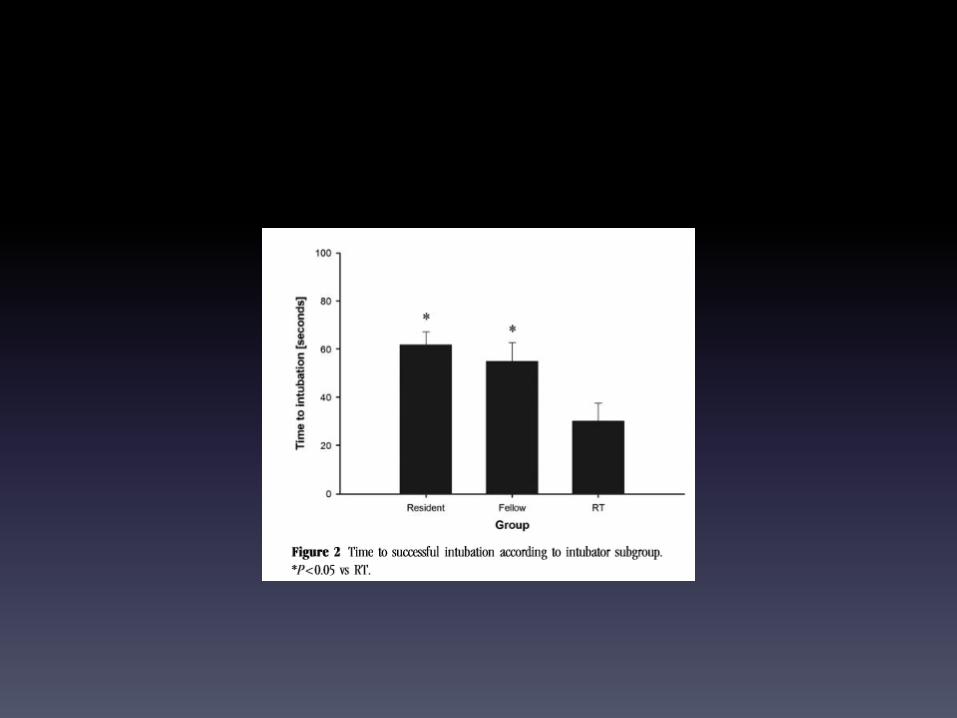
• 50 ETI assessed
• Residents (25), NICU Fellows (13), RTs (12)


Why difference Adult to Neo
• Difficult airway uncommon
• Limited techniques and adjuncts
• Uncommon procedure even for Attending
Physicians

What do you do if you cant intubate a neonate???

• Telephone survey of all 59 level 3 NICU in UK
• 7% had CICV algorithm


Cautious Maybe
• Smaller, dedicated staff
• Take on the dedicated role
• Reasonable competency program