john u doherty, md, facc anticoagulation consortium
TRANSCRIPT
• Expert Consensus Decision Pathway on Peri-Procedural Management of Anticoagulation John U Doherty, MD, FACC Anticoagulation Consortium Roundtable Heart House October 24, 2015

• Peri-Procedural Management of Anticoagulation Consensus Document/Pathway/App Writing Group – John U Doherty, MD, FACC – Ty Gluckman, MD, FACC – William Hucker, MD, PhD, FIT – James Januzzi, MD, FACC – Thomas Ortel, MD – Sherry Saxonhouse, MD, FACC – Sarah Spinler, PharmD, AACC – ACC Staff:
• Lea Binder, • Veronica Wilson

• Peri-Procedural Management of Anticoagulation in Non-Valvular Atrial Fibrillation: The Problem – 35 million prescriptions written annually in the
United States for oral anticoagulation (OAC) – 15-20% have or potentially have interruption of
OAC therapy in a given year placing them at risk of thrombo-embolic events (TE), bleeding, or death
– Management of such patients is spread across providers with poor coordination in decision making across these clinicians.

• Risk stratification in informing such decisions is performed inconsistently (ORBIT-AF)
• Management depends upon patient related factors (risk of TE), procedure related risk of bleeding, education of providers, coordination of care with proceduralists.
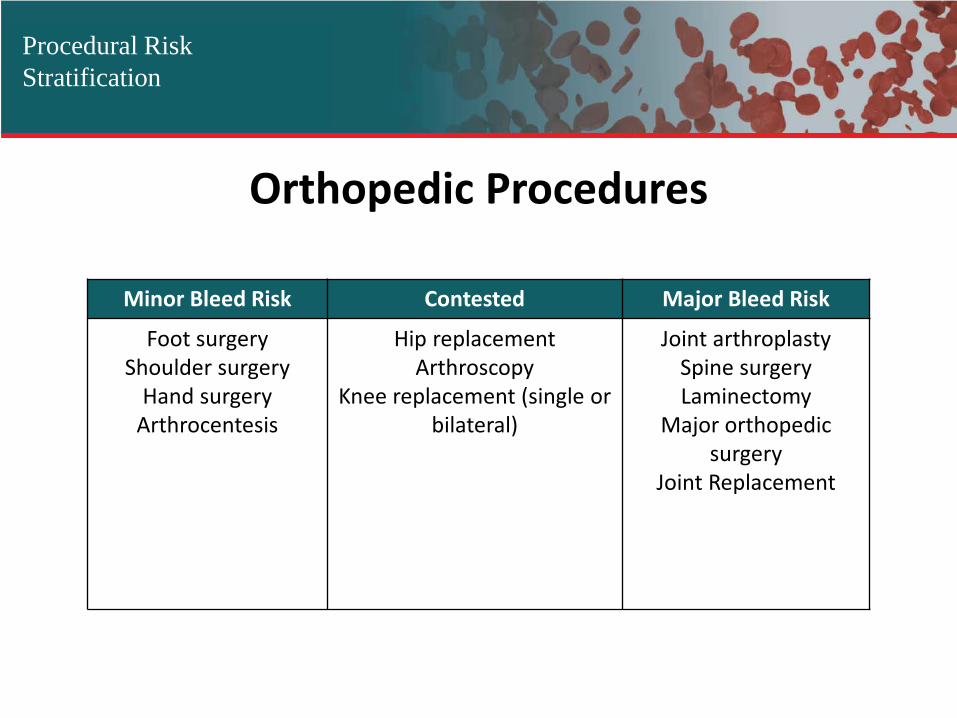
Orthopedic Procedures
Procedural Risk Stratification
Minor Bleed Risk Contested Major Bleed Risk
Foot surgery Shoulder surgery
Hand surgery Arthrocentesis
Hip replacement Arthroscopy
Knee replacement (single or bilateral)
Joint arthroplasty Spine surgery Laminectomy
Major orthopedic surgery
Joint Replacement
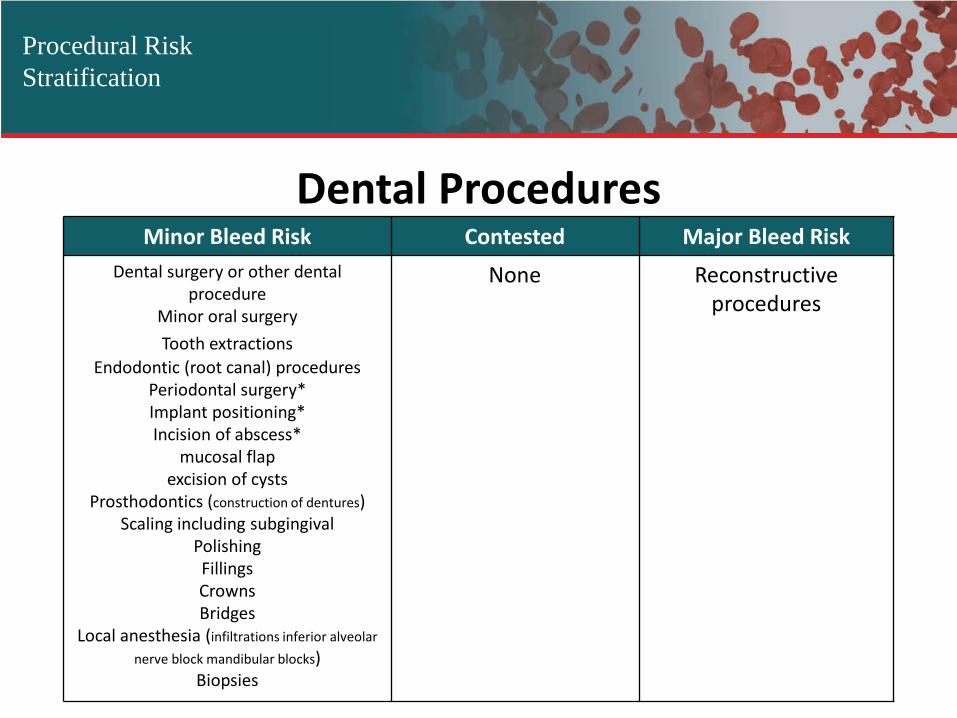
Dental Procedures
Procedural Risk Stratification
Minor Bleed Risk Contested Major Bleed Risk Dental surgery or other dental
procedure Minor oral surgery Tooth extractions
Endodontic (root canal) procedures Periodontal surgery* Implant positioning* Incision of abscess*
mucosal flap excision of cysts
Prosthodontics (construction of dentures) Scaling including subgingival
Polishing Fillings Crowns Bridges
Local anesthesia (infiltrations inferior alveolar nerve block mandibular blocks)
Biopsies
None
Reconstructive procedures

Gastrointestinal Procedures
Procedural Risk Stratification
Minor Bleed Risk Contested Major Bleed Risk Gastrointestinal endoscopy +/- biopsy
Endoscopy ultrasound (EUS) without fine-needle aspiration (FNA)
Capsule endoscopy Endoscopy without surgery*
Upper and lower endoscopy without biopsy Endoscopic retrograde
cholangiopancreatography (ERCP) without sphincterotomy
Diagnostic endoscopic retrograde cholangiopancreatography (ERCP)
Luminal self-expanding stent placement (controversial)
Biliary/pancreatic stent without sphincterotomy
Enteral stent deployment (without dilation) Colonoscopy with or without biopsy
Diagnostic procedures +/- biopsy Diagnostic esophagogastroduodenoscopy
(EGD) with or without biopsy Flexible sigmoidoscopy with or without
biopsy Nonthermal (cold) snare removal of small
Enteroscopy Therapeutic balloon-assisted
enteroscopy Endoscopy (including balloon enteroscopy) with or without
mucosal biopsy Enteroscopy and diagnostic
balloon-assisted enteroscopy Colonic polyp resection
Colonic polyp resection < cm safe without bridging
Resection of large colon polyp (>- cm)
Catheter exchange through well formed tracts (e.g.
gastrostomy nephrostomy cholecystostomy tubes)
Gastrostomy tube placement (initial)
Percutaneous endoscopic gastrostomy
Treatment of esophageal/gastric varices Treatment of varices
Variceal band ligation (controversial) Coagulation or ablation of tumors or vascular lesions
Tumor ablation by any technique Endoscopic sphincterotomy (.-% risk of bleeding)
Biliary sphincterotomy Pancreatic sphincterotomy
Endoscopic retrograde cholangiopancreatography (ERCP) with sphincterotomy
Abdominal procedure Polypectomy
Polypectomy (> cm) Colonoscopic polypectomy (-.% risk of bleeding)
Gastric polypectomy (% risk of bleeding) Endoscopic mucosal or submucosal dissection
Percutaneous liver biopsy Endosonographic (EUS) guided fine needle aspiration
Endoscopy ultrasound (EUS) with fine-needle aspiration (FNA) or needle biopsy Endoscopic hemostasis
Cystogastrostomy Endoscopic mucosal resection

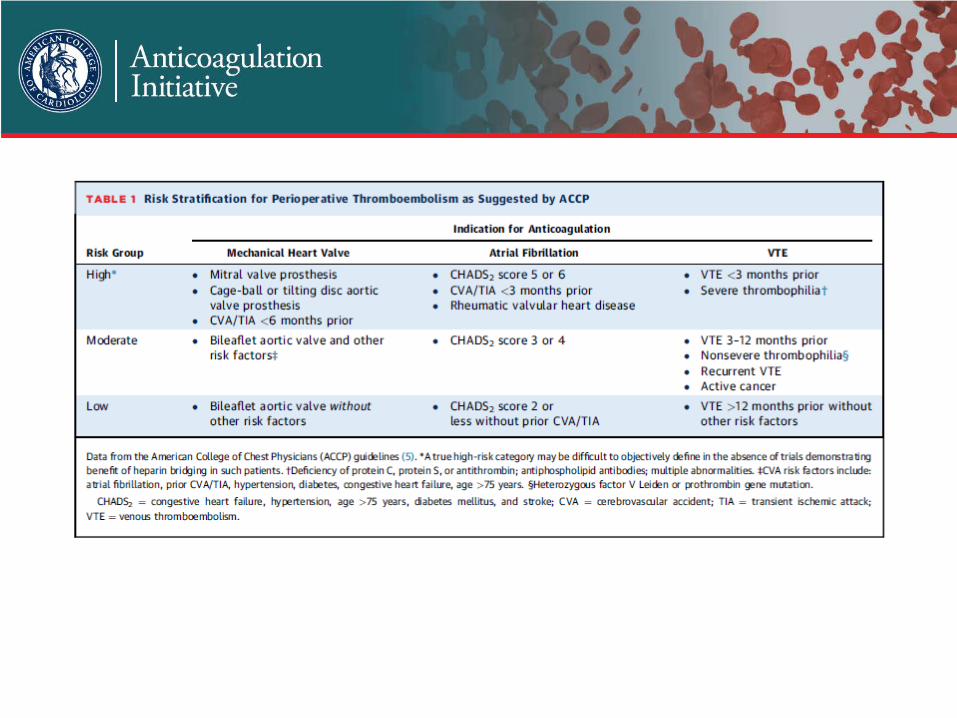
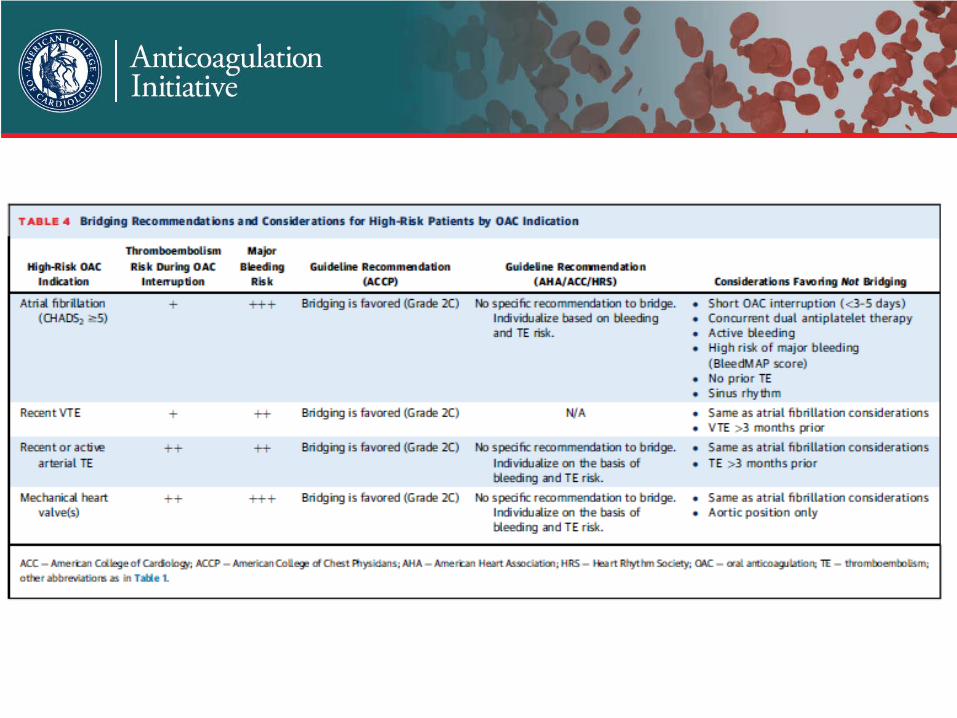
• What We Know and What We Don’t – Guidelines are limited: ACCP and ACC/AHA AF
Guidelines suggest continuation of anticoagulation for procedures with low bleeding risk, bridging for patients at high risk of TE that require interruption, and clinical judgment for those at intermediate risk.
– For certain procedures, continuation of warfarin is associated with lower risk of bleeding and equivalent TE risk to interruption with bridging (BRUISE Control)
• What We Know and What We Don’t – How Should DOACs Be Managed Peri-
Procedurally? • Not informed with RCTs. Europace article provides
practical recommendations for managing DOACs peri-procedurally

• Defining the Algorithm – Assumptions:
• An area of clinical variability and incomplete knowledge • Common problem with care across many providers with
variable knowledge • Proceeding without interruption often not considered • Use of a parenteral agent probably too frequent • DOACs, if dosed properly, seldom need to be bridged • Peri-procedural management with DOACs needs to
follow a different path than warfarin

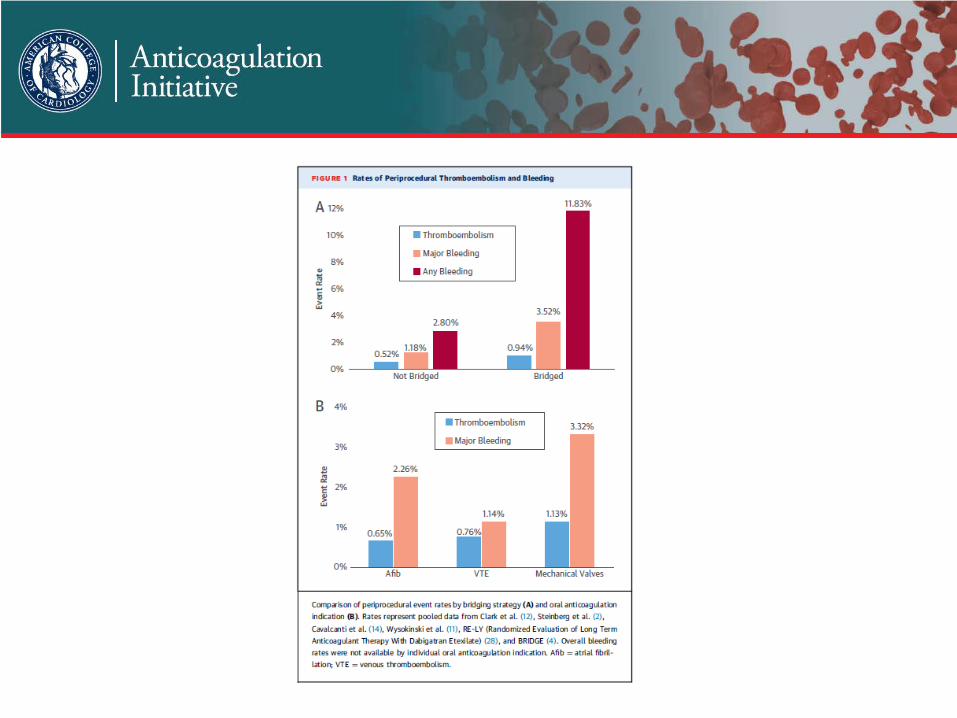
– The risk of a TE with an interruption averages 0.52% for interruption without bridging and 0.94% for those interrupted and bridged based on pooled data (0.4% and 0.3% respectively in BRIDGE trial)



• The Process – Should the patient be anti-coagulated in the first
place? – Assess TE risk of interruption (patient specific) – Assess risk of bleeding (procedure specific) – Are some procedures such low risk that clinicians
can fast track decision not to interrupt – Are there procedures of sufficient bleeding risk
that we would always interrupt?

• The Process • Recognize that there are instances where clinical
judgement needs to prevail • Attempt to give guidance that is procedure-specific
• When to restart anticoagulant? It’s Not Just 1 Decision! – Decide to stop – Decide when to stop informed by labs, creatinine
clearance – Use a parenteral agent prior to procedure – Use a parenteral agent post-procedure: when and
what dose – When to stop parenteral agent
