journal club hallie lee pharmd candidate 2013 mercer university cophs pha 618 geriatrics-continuous...
TRANSCRIPT
Journal ClubHallie LeePharmD Candidate 2013Mercer University COPHSPHA 618 Geriatrics-Continuous Care
Multivitamins in the Prevention of Cardiovascular Disease in Men; The Physicians’ Health
Study II Randomized Controlled Trial

Introduction: The PHS PHS = Physicians’ Health Study II
Multivitamins, the most common supplement taken by US adults, are used to prevent vitamin and mineral deficiency
Perception that they may prevent cardiovascular disease
Observational studies have shown inconsistent associations
There are no long-term clinical trials of their use for CVD
TO DETERMINE WHETHER LONG-TERM MULTIVITAMIN SUPPLEMENTATION DECREASES THE RISK OF MAJOR
CARDIOVASCULAR EVENTS AMONG MEN
(Results for cancer, eye disease, and cognitive decline are to be published separately)
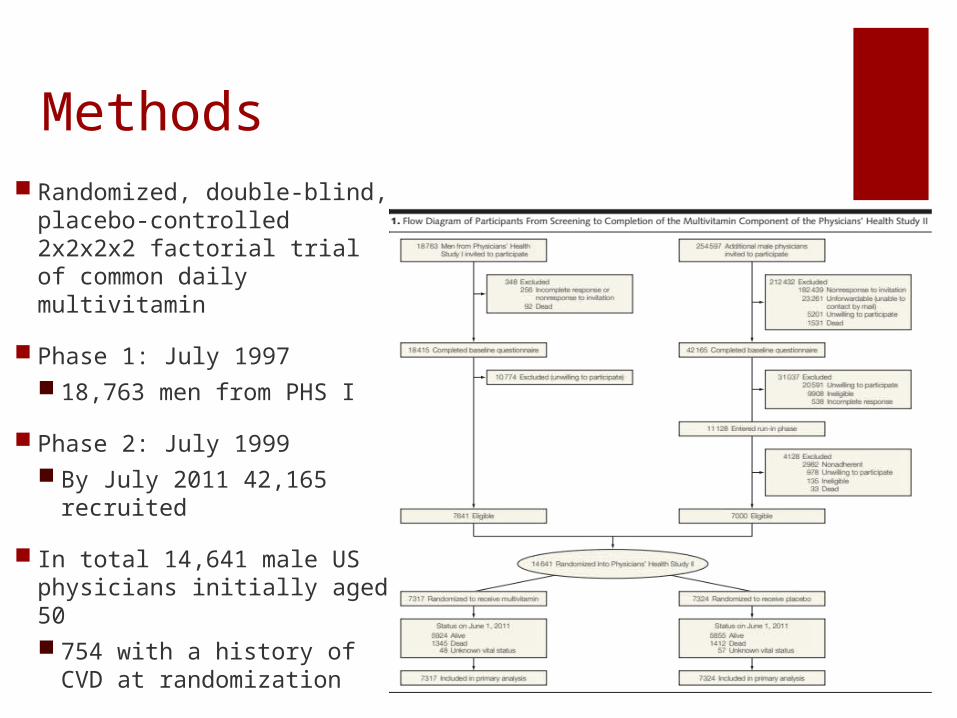
Methods Randomized, double-blind,
placebo-controlled 2x2x2x2 factorial trial of common daily multivitamin
Phase 1: July 1997 18,763 men from PHS I
Phase 2: July 1999 By July 2011 42,165
recruited
In total 14,641 male US physicians initially aged 50 754 with a history of CVD
at randomization

Methods Stratified by age, prior cancer or
CVD, & PHS I assignment
Multivitamin
Vitamin E
Vitamin C
Beta carotene
Exclusion Criteria History of cirrhosis or acute
liver disease Taking anticoagulants Reported serious illness Willing to forgo current use of
multivitamins or supplements with >100% the RDA
Funded by National Institutes of Health, BASF Corp., Pfizer, and DSM Nutritional Products Inc.

Base
line
Chara
cteristics
MethodsPrimary endpoint:
Major cardiovascular events (nonfatal MI, nonfatal stroke, and CVD mortality) Secondary
endpoints:
MI and Stroke individually

Results Rates of major CV events:
11.0 per 1000 person-years in the multivitamin group
10.8 per 1000 person-years in the placebo group
Men taking a daily multivitamin experienced no benefit for the primary end point of major CV events (HR, 1.01; 95% CI, 0.91- 1.10; P = .91)
Lack of significant benefit for the secondary end points
Total MI (3.9 and 4.2 events per 1000 person-years for multivitamin and placebo, respectively; HR, 0.93; 95% CI, 0.80-1.09; P = .39)
Total stroke (4.1 and 3.9 events per 1000 person-years; HR, 1.06; 95% CI, 0.91-1.23; P = .48) compared to placebo
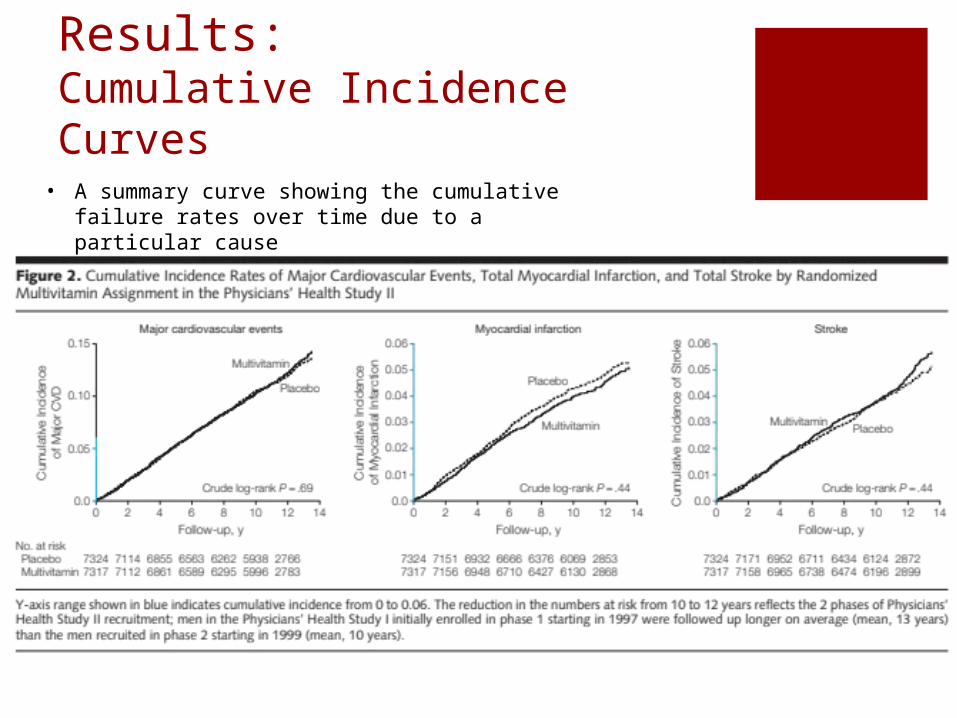
Results: Cumulative Incidence Curves • A summary curve showing the cumulative failure
rates over time due to a particular cause

Results
Subgroup analyses examined whether baseline clinical, lifestyle, familial, biochemical, and dietary risk factors for CVD, along with the other randomized PHS II interventions, modified the effect of a daily multivitamin on major cardiovascular events
Suggestion of a differential effect across age groups with possible differences among men aged 50 to 59 years and men 70 years or older
No other evidence was found of effect modification by baseline risk factors on major CV events

Sta
tistics The PHS II was estimated to have 80%
power to detect a 12% reduction in the primary end point of major CV events
Primary analyses were based on the intention-to-treat principle
All analyses performed using SAS version 9.2 (SAS Institute Inc) and S-Plus (Insightful Corp), with statistical significance set at P < .05 using 2-sided tests
Cox proportional hazards models estimated hazard ratios (HRs) and 95% CIs
Each pre-specified end point stratified on the presence of CVD at randomization and adjusted for PHS II study design variables, including age, PHS cohort (original PHS I participant, new PHS II participant), and randomized vitamin E, vitamin C, and beta carotene assignments
Statistics Relative Risk/Hazard Ratio
(876/7317) / (856/7324) = 1.01
Relative Risk Reduction 1- 1.01 = 0.01
Absolute Risk Reduction (856/7324) – (876/7317) = 0.003
Number Needed to Treat 1/0.003 = 333.33
Odds Ratio (876/6441) / (856/6468) = 1.03

Statistics: A look at “Power” Power is defined by beta ()
Indicates the probability of the statistical test detecting significant differences when they exist
Analogous to sensitivity
Defined as 1 - Power of 80% is minimal Power of 90% is ideal
A power of 80% means there is a 20% chance of a type II error To falsely conclude that no significant difference exists
between populations/samples
Due to chance or small sample size

Power• Higher power is achieved by increasing the sample size• Often overlooked by researchers• Tabulated values and formulas are available for calculating the
required sample size• The smaller the difference between two interventions, the larger
the sample size needed

Conclu
sion
DAILY MULTIVITAMIN SUPPLEMENTATION DID NOT REDUCE THE RISK OF MAJOR CARDIOVASCULAR EVENTS
Whether to take a daily multivitamin requires consideration of an individual’s nutritional status, because the aim of supplementation is to prevent vitamin and mineral deficiency, plus consideration of other potential effects, including a modest reduction in cancer and other important outcomes in PHS II that will be reported separately

Discussion Limitations
Only one multivitamin formulation Study population was confined to middle-aged and
older, predominantly white, male physicians Long-term multivitamin use may be more effective
when initiated earlier in life to counter the initiation and progression of atherosclerosis that often begins at an earlier age
No recommendation or change in practice should be made based on the information found in this trial
Additional trials are necessary
Class Ib level of evidence
References Sesso H., Christen W., Bubes V., et al. Multivitamins
in the Prevention of Cardiovascular Disease in Men; The Physicians’ Health Study II Randomized Controlled Trial. JAMA November 7, 2012; 308(17):1751-1760.