journal of neuroendoscopy -...
TRANSCRIPT

Journal of NeuroendoscopyVolume 1, Number 1 2010
EDITORIAL 1 ORIGINAL PAPERS:
Frameless Free-hand Neuroendoscopic Surgery ─ Development of the Finest Rigid-rod Neuroendoscope Model to cope with the Current Limitations of Neuroendoscopic Surgery─
Shizuo Oi, M.D., Ph.D. 2 REVIEW ARTICLE:
Controversy in Neuroendoscopic Third Ventriculostomy: a Current Status ReviewMasaki Shinoda M.D., Ph.D., Atsushi Murakata M.D., Motoharu Fujii M.D., Ph.D., Ryoichi Ishikawa M.D., Shizuo Oi M.D., Ph.D. 12
NEUROENDOSCOPY On-line Video Technical Education [NEOL: VTE] 19
The Master’s Neurodoscopic Surgical Technique NEOL: VTE No.001 From Basic to Most Advanced Neuroendoscopic Technique with “Oi Handy ProTM”
Shizuo Oi, M.D., Ph.D. 20 NEUROENDOSCOPY On-line Journal Consensus Conference [NEOL: JCC]
NEOL: JCC No.001 Indication for Neuroendoscopic SurgeryPart 1: Arachnoid Cyst 21
My Opinion 23 NEUROENDOSCOPY ESSAY
“Health of Children Worldwide, Seeking God’s Guidance!” Shizuo Oi, M.D., Ph.D. 24
NEUROENDOSCOPY NEWS LETTER
Section I Neuroendoscopy Federations and Societies in the World 35 The History of the GLEN Carlos Gagliardi, M.D. 37 IFNE Interim Meeting: The Neuroendoscopy Masters, 2010 Tokyo Masakazu Miyajima, M.D., Ph.D. 39
Section III Ongoing Neuroendoscopy Studies in the World Worldwide Survey on Pineal Region Tumor Shizuo Oi, M.D., Ph.D. 40 Nationwide investigation on the current status of therapeutic neuroendoscopy for ventricular and paraventricular tumoristic lesions in Japan Nakamasa Hayashi, M.D., Ph.D., Naokatsu Saeki, M.D., Ph.D., Shunro Endo, M.D., Ph.D. 41
Section IV Neuroendoscopy Hands-on Course in the World 43 1. 3rd Minimally-Invasive Neurosurgery Neuroendoscopy Hands-on course Marco A Barajas Romero, M.D. 44 2. 1st Shanghai International Neuroendoscopy Hands-on Workshop [SINEHOW] Jie Ma, M.D., Ph.D., Shizuo Oi, M.D., Ph.D. 45 3. Japanese Society for Neuroendoscopy [JSNE] Hands-on Seminar 2010 Part 1 Takayuki Ohira, M.D., Ph.D. 47
NEUROENDOSCOPY RESEARCH WORLD RECORD RANKING [1950─2010.2]
The list of Top 10 researcher’s papers 49
Journal of Neuroendoscopy

Though not recognized as an independent specialty by international, regional, or national pediatric/adult neurosurgical organizations, Neuroendoscopy Research is de facto recognized as a specific field of research by neurosurgeons, by all other medical and surgical specialties, and by society. The principles of neuroendoscopy surgery are being established, its limits extended and defined, and its practitioners identified. However, even after one hundred years of Neuroendoscopy Research, the various specific indications, pathophysiology in the treatment goal, treatment modalities and outcomes, and fundamental basic science, remain controversial. A journal specific to Neuroendoscopy Research is needed. I chose to undertake this work together with an editorial board including major neuroendoscopy researchers worldwide. The very different national origins and ultimate life goals of the board members form the basis for the truly humanistic group of Neuroendoscopy Research. Still, when all is said and done, how does a journal that hopes to be a humanistic treatment of a scientific discipline, one composed of theoretical and technical elements, come into existence? We are beginning this work with an exhaustive review of the literature over the past century, creating a Neuroendoscopy Research World Record Ranking [NERWRR] as a means of critically analyzing various diagnostic, and therapeutic aspects of neuroendoscopy in the history of Neuroendoscopy Research. In the critical review of nearly 1,000 publications in the NERWRR by the “Masters’ Publications” Review Committee, it was obvious that the Neuroendoscopy technology has been the source to advance the Neuroendoscopy Research. The collaboration with the International Federation of Neuroendoscopy [IFNE] and other international/continental/regional/national societies for neuroendoscopy is essential. It is hoped that this may serve as an ongoing update on Neuroendoscopy Research, while simultaneously stimulating present and future Neuroendoscopy Researchers to advance the present knowledge and treatment modalities in this field, less invasively and more completely to heal the sick patients.
Shizuo Oi, M.D., Ph.D.
Editor-in-Chief Journal of Neuroendoscopy
January 8, 2010
EDITORIAL
Journal of Neuroendoscopy
It is hoped that this “Journal of Neuroendoscopy” may serve as an ongoing update on Neuroendoscopy Research, while simultaneously stimulating present and future Neuroendoscopy Researchers to advance the present knowledge and treatment modalities in this field, less invasivelyand more completely to heal the sick patients.
�J. Neuroendoscopy, Vol. 1, No. 1, 2010

� J. Neuroendoscopy, Vol. 1, No. 1, 2010
Frameless Free-hand Neuroendoscopic Surgery─ Development of the Finest Rigid-rod Neuroendoscope Model to Cope with the Current Limitations of Neuroendoscopic Surgery─Shizuo Oi, M.D., Ph.D. Department of Neurosurgery,The Jikei University School of Medicine [JWCMC], Tokyo JapanInternational Neuroscience Institute [INI], Hannover, Germany
Corresponding Author:Shizuo Oi, M.D., Ph.D.Department of Neurosurgery,The Jikei University School of Medicine3-25-8 Nishi Shinbashi, Minato-ku 105-8461, Tokyo, JapanPhone : + 81- 3-3433-1111Fax : + 81-3-3433-1161E-mail : [email protected]
Key Words: neuroendoscopic surgery; free-hand technique; endoscope-stylet technique; slit-like ventricle
ORIGINAL PAPER
Journal of Neuroendoscopy
The author describes a new and advanced neuroendoscopic surgical technique, “frameless free-hand neuroendoscopic surgery” using a new neuroendoscope that offers improved access to intracranial lesions and maneuverability for various microinstruments during high-resolution imaging. The neuroendoscope has a rigid rod that is 2 mm in diameter and 16.5 cm in length, which is placed in the lower two thirds of an ovoid cannula that is 4.0 × 2.5 mm in diameter. The “gun-butt” holder which the operator grips with his/her left hand, provides stability to the holder and allows the endoscope to be handled with improved control. The surgical route is protected by insertion of a No. 12 or 14 French peel-away sheath. Various microinstruments can be introduced to the operative field via the upper one third of the cannula. These microinstruments are nearly as long as the body of the endoscope, and because these instruments are grasped directly by the surgeon’s right hand, fine neuroendoscopic surgical maneuvering is more readily achieved. The main technical advantage of the free-hand maneuvering of the Handy Small-diameter Rigid-Rod Neuroendoscope is that it can be held comfortably with one hand and instruments can be maneuvered in and out of the filed with the other. The author’s new neuroendoscopic technique, with Endoscope-stylet Technique for a peel-away sheath placement made it possible to deal with intravenicular lesions even in the slit like centricles. It can be concluded that the new and advanced neuroendoscopic surgical technique with “Oi Handi ProTM” has expanded the current concept of the indications for neuroendoscopic surgery.
Summary

�J. Neuroendoscopy, Vol. 1, No. 1, 2010
I. Introduction and Background
Intracranial endoscopic surgery (neuroendoscopic surgery) has progressed remarkably over the last
two decades, and various intracranial pathological / pathophysiological conditions are now considered to be treatable with this developing “minimally invasive” neurosurgical procedure [9][10][11][12][13][14][15][16] [17][18][19][20][21][22][23]. The endoscope apparatus used by L’Espinasse [3] played an important part in these first attempts at the treatment of hydrocephalus in 1910. Dandy in 1918 [4], and Putnam in 1934 [16], reported their experiences, which were mainly in endoscopic choroid plexus cauterization. Neuroendoscopic third ventriculostomy was then performed by various neurosurgeons, but it never became a standard technique, largely because the shunt procedure became a generally accepted method for the treatment for hydrocephalus. Although the placement of a shunt became a major therapeutic procedure with the development of silicone in the 1950s [8] and the condition of the majority of hydrocephalus patients was improved with this procedure, the management of hydrocephalus with shunts, regardless of design, is associated with a high incidence of complications. Neuroendoscopic third ventriculostomy (ETV) practices as an alternative to shunting procedures has revolutionized the management of hydrocephalus. Today, ETV is the procedure of choice for patients with non-communicating type of hydrocephalus caused by aqueductal stenosis and other types of ventricular cerebrospinal fluid (CSF) block, with the success rate reaching 60 to 85% in most reported series [1][2][5][6][7]. Wi th t he p rog re s s o f i n s t rumen ta t i ons fo r neuroendoscope, the surgical applications of this neuroendoscopic system expanded not only to lesions related with the CSF circulation but also to management of intracranial tumors and others. The neuroendoscopic system has also come to be applied in micro-neurosurgical procedures, especially skull base surgery, intraventricular surgery and surgery for deep-seated tumors [10]. In dealing with these various pathological / pathopysiological lesions, it became clear that neuroendoscopic surgery requires some categorical differences in procedure corresponding to the nature of each lesion. Moreover, various types of endoscopy for neuroendoscopic surgery are now available, as well as the associated microinstruments. In addition to the flexible / steerable (fiber) type of neuroendoscope, which became less popular because of the limited sterilization method not able to prevent the possibility of prion disease by autoclaue, there have emerged rigid-rod and semi-rigid-
rod endoscope as alternative choices. The author introduces the concepts and design of the “Handy Rigid-rod Neuroendoscope” (Oi Handy ProTM, Karl Storz, Tuttlingen, Germany) with the clinical application for “Frameless Free-Hand Maneuvering”, and discuss the usefulness of this newly developed neuroendoscope and a new concept for neuroendoscopic surgical procedures, consequently to cope with the current limitations of neuroendoscopic surgery.
II. Indicated Diseases for Neuroendoscopic Surgery (Table 1)
The operat ive procedures achieved with this configuration included third ventriculostomies for non-communicating hydrocephalus, fenestration of septation of the hydrocephalic ventricle or septum in isolated ventricles (isolated unilateral ventricle), fenestration of arachnoid cysts and tumors, placement of ventricular tubes in ventricles or intratumoral cystic cavities, biopsies of intraventricular tumors and other advanced techniques. The history of neuroendoscopic surgery is essentially linked to developments in instrumentation. The first attempts at intracranial endoscopic surgery were performed using cystoscopes early in last century. Since then, the rigid type of endoscope had been the main instrument in this field, though many type of flexible viewing devices have been developed, for example those used in the upper and lower gastrointestinal system and upper respiratory tract. The quality of lighting guides and objective lenses has improved and micro-instrumentation has further developed for this rigid type of neuroendoscope. Through the straight working channel this system can accommodate relatively complicated instruments. Operative procedures applied in neuroendoscopic surgery vary in their tissue disruption processes, which include vaporization, coagulation and mechanical manipulation. The former two maneuvers can be achieved by lasers (KTP and YAG fiberoptic lasers), monopolar/ bipolar coagulators, and other devices. Mechanical manipulation can be handle first by the microforceps, which can be passed through the working channel(s), thus facing a certain limitation in the variety and the function of instruments if a flexible endoscope is used. Ventriculostomy for non-communicating and choroids plexus coagulation for communicating hydrocephalus are still debatable on the critical point of whether the postoperative hydrocephalic condition is completely arrested or not. Since there is no definite investigation method by which to estimate preoperatively the postoperative CSF circulation and dynamics with satisfactory alternative CSF pathways and intracranial

� J. Neuroendoscopy, Vol. 1, No. 1, 2010
pressure dynamics, this problem must be studied as one of the future topics of hydrocephalus research. The major concern regarding choroid plexus coagulation in the fact that the human brain requires certain amount of CSF to keep the CSF circulation, essential to maintain homeostasis of the human brain metabolism. The condition of high protein with “waste chemical” of the brain metabolism in the CFS after choroid plexus coagulation is definitely non-physiological and harmful to the brain function. The essential therapeutic goal exists in the condition of arrested hydrocephalus with the CSF circulation maintained physiologically. Shunt manipulation using the semi-rigid-rod endoscope will become more widely recognized as the benefits become more evident. There is room for improvement of the instruments for that purpose. Tissue biopsy and resection are another possibility for this type of neuroendoscopic suregery. Biopsy in
the intraventricular location may be performed less invasively: this may require various forms of instruments, depending on the characteristics and location of the lesion. However, removal of deep-seated intraparenchymal lesions by purely endoscopic maneuvers is debatable. The procedures reported to approach such lesions are just “endoscope-assisted” micro-neurosurgery: the endoscope was merely used for better illuminations and visualization of the operative field in the “open” cannula. “Endoscopic surgery” must be defined as a procedure done in a closed cavity. The future aspects to be developed may, hopefully, include this concept as “micro-endoscopic surgery”.
III. Neuroendoscopy: Fiber Endoscope vs. Rigid-rod Endoscope
1.The past The instrumentation in neuroendoscopic surgery has rapidly improved along with the most recent developments
TABLE 1Future aspects of the research subjects on neuroendoscopic surgery and realistic indications
Possible indications Critical points Future aspects of the researchRealistic indication if confirmed following
Ventriculostomy -> non-communicating hydrocephalus
* Hydrocephalus : completelyarrested postoperatively (?)
* ICP dynamics * Definitely postoperative arrested hydrocephalus
* Subarachnoid CSF dynamics:intact preoperatively (?)
* Preoperative estimation of postoperative CSF circulation
* Definitely postoperative arrested hydrocephalus
* Hydrocephalus completelyarrested postoperatively (?)
Choroid plexus coagulation-> communicating hydrocephalus
* High CSF protein: Harmful to homeostasis of the normal brain metabolism (?)
* CSF formation / absorption rate
* Safety of reduced CSF circulation to the brain metabolism
(not likely acceptable) * Reduction of CSF formation: satisfactory (?)
* Disturbed brain matabolism and development
* Preoperative estimation of postoperative CSF circulation
Shunt manipulation-> shunt placement and / or revision
* Stylet maneuvering shunt placement : best technique (?)
* Brighter operative field and high resolution of image
* Best positioning of shunt tube in the ventricle
Tissue biopsy / resection-> Intraventricular lesions
* Biopsied tissue : enough amount of material for pathological diagnosis. (?)
* Mobility of the instruments of brighter operative field
* Less-invasive tissue diagnosis
Tumor resection-> deep-seated intraparenchymal lesions
* Endoscopy : Just an assistingtool in microsurgery (?)
* Micro-neuro-endoscopic surgery
* Endoscopy-assisting microneurosurgery
Cyst fenestration -> arachnoid cyst
* Long-stauding opening of the fenestrated window with maintained CSF flow (?)
* Prevension of postoperative symptomatic giant subdural hygroma : Selection of transventricular ventriculo-cystostomy route
* Application of the finest neuroendoscopy via small or slit-like ventricle

�J. Neuroendoscopy, Vol. 1, No. 1, 2010
in the application of specific neuroendoscopic techniques. Presently available neuroendoscopic instruments include: 1) There type of neuroendoscope: rigid-rod, semi-rigid-
rod, and steerable-flexible rod endoscopes 2) A halogen light source 3) Viewing equipment, including TV screens and video
recorders 4) Microinstruments such as KTP / YAG lasers,
monopolar coagulators, microforceps (grasping / biopsy), and microballoons
5) Assisting or supporting systems including endoscopic ultrasonography and stereotactic systems
The selection of each component should be based on the specific indication / clinical use of the procedures. The selection should consider the following factors: (1) high image sesolution vs. mobility, for the neuroendoscope; (2) brighter operative field by specific system vs. adaptation of the available light source, for the lighting system; (3) a small but fine image for the video viewing system; (4) anticipated surgical procedures such as fenestration, resection, cutting, and coagulation, for microinstruments; and (5) for the assisting / supporting system, how much the surgeon extends the indication, with considerable understanding for the limitations of neuroendoscopic surgery. There are various aspects that should influence the choice of neuroendoscpe for clinical use. The most salient advantage of the rigid-rod neuroendoscope is its high image of quality, leading the fine morphological analysis with much brighter illumination than its counterparts in comparison with the large size of lens in fiber or video scope. On the other hand, the most important advantage of the steerable-flexible neuroendoscope is its mobility in the ventricle or any other confined space, such as the cystic cavity of the brain parenchyma. The advantages of the semi-rigid-rod neuroendoscope include its fine structure, offering angulations in operative maneuvers, and its possible application as a stylet for shunt placement. The limitation of each type of neuroendoscope must also be understood. The fixed operative field and larger instrument size for the rigid-rod, and the dimmer operative field and limited choice of instrument size for the semi-rigid-rod and flexible / steerable-rod types, and considerable disadvantages. These advantages and disadvantages should be taken into account in the planning of individual procedures. 2.Towards conquering the individual disadvantages We have been involved in development of a flexible-steerable neuroendoscope and advancements in instrumentation and surgical techniques [9][10][11][14] in the last decade of last century. CNS diseases and
pathophysiology as neuroendoscopic surgical targets for these techniques include specific forms of hydrocephalus [13][15], deep-seated tumors, such as pineal region tumors [12], and others [10]. Recent advances in neuroendoscopic instrumentation have provided various types of neuroendoscopy in three major forms described as above. Significant advantages and disadvantages exist for each type. In addition to those technical standpoints of view, the critical disadvantage for fiber scope or video scope have been pointed out in the sterilization method. The fiber scope or video scope cannot be tolerated to the heat of auto clave to prevent prion disease, such as Creutzfeldt-Jacob disease. The mainstream of the neuroendoscopy clinically applied has been created with rigid-rod endoscopy in majority of countries in the world. Following clinical experience using the various types of neuroendoscope, in 1997 we started to design and develop a new type of neuroendoscope combining the individual advantage of the three types, as a cooperative research project with Karl Storz (Tuttlingen, Germany). A prototype was finalized after several revisions of the model in 2003.
IV. Development of A New Neuroendoscope Model [J. Neurosurgery (Pediatrics 1) 102 : 113-118, 2005]
Description of the “Handy Small Diameter Rigid-rod Neuroendoscope with three Working Channels” (Oi Handy ProTM, Karl Storz, Tuttlingen, Germany)The body of the endoscope comprises an oval-shaped outer sheath (3.5 × 2.5 mm maximum diameter and 16.5 mm long), a rigid-rod objective lens (2.0 mm diameter with a 0°or 12°angle), a working channel (upper 1/ 3 of the sheath connected to 3 outlet/inlet orifices), and a handle attachment knob to which a holding handle can
FIG. 1: “Oi Handy ProTM” with the holding handle affixed to a handle attachment konb.

� J. Neuroendoscopy, Vol. 1, No. 1, 2010
be affixed (Fig. 1). A fixation notch is also present, to which a holder-arm can be applied if the operator wishes to use the system under fixation rather than freehanded, although we have never required fixation procedures in neuroendoscopic surgery. The three-outlet/inlet orifices are used for irrigation (left), suction (center) and micro-instrumentation (right). Irrigation and suction procedures are undertaken by opening either the left or center orifice, respectively. The total weight of the neuroendoscope is 550 g with the endoscope connected to a lighting cable and camera. A number of microinstruments of 1.3-mm diameter are available, including micro-scissors, biopsy forceps, grasping forceps, mono-polar coagulator/cutting rod and bipolar coagulator. These can be introduced through the upper 1/3 of the neuroendoscope lumen (Fig.2 A-E).
V. Frameless Free-hand Technique Model [J. Neurosurgery (Pediatrics 1) 102 : 113-118, 2005]
Through a burr hole, 8 mm in diameter, a 14 French peel-away sheath (“Oi Clear Navi Sheath®”) [19] is passed into the target ventricle. The endoscope is then inserted into the ventricle through the peel-away catheter, and anatomical landmarks are indentified. Steady holding of the endoscope in the surgeon’s left hand over the handle grip at the base allows quick back and forth
movements along the long axis through in a peel-away sheath inserted to the ventricle and with minimally-required side shift of the tip of endoscope to the objective target. Using the right-most inlet/outlet orifice, the short and handy semi-flexible micro-instruments can be guided and controlled by the surgeon’s right hand (Fig. 2 B-D). Irrigation is facilitated by the assistant manually injecting artificial cerebrospinal fluid (CFS). For balloon techniques, a 2 French Forgatti micro-balloon (1.0 mm diameter and 5 mm maximum inflation) can also be manipulated right-handed at the right orifice (Fig. 2 A-H), placing the balloon at the best site for ventriculostomy. Inflation and deflation procedures are controlled by the assistant using manual manipulation of air injection with a 1-ml micro-syringe. Specific techniques for individual neuroendoscopic procedures Third ventriculostomy: Landmarks to guide the endoscope tip to the floor of the third ventricle have been described elsewhere[5][9]. The “Handy Small Diameter Rigid-rod
FIG. 2 B/C: Insertion of the endoscope with both hands’ holding through the peel-away sheath placed.
A
B
FIG. 2: Frameless Free-hand Technique of “Oi Handy ProTM”A: Steady holding of the endoscope in the surgeons left hand.

�J. Neuroendoscopy, Vol. 1, No. 1, 2010
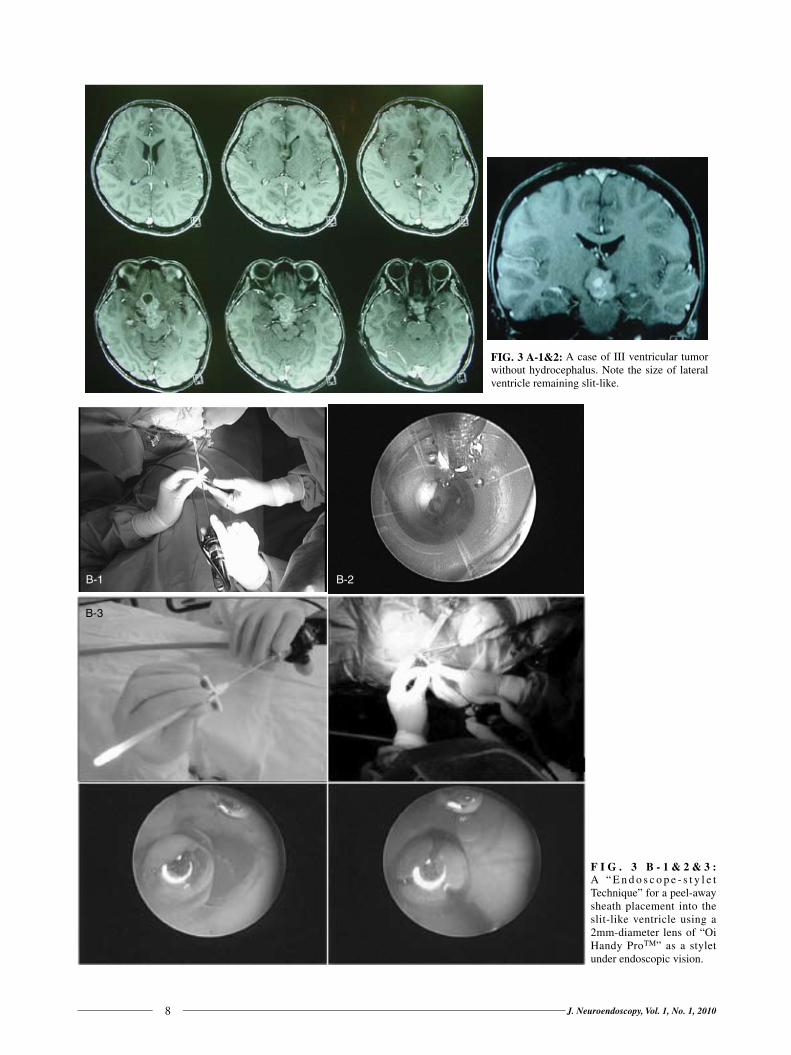
Neuroendoscope” allows passage through a normal-seized foramen of Monro and a wide-angled operative field to discern intraventricular morphology (such as aqueductal stenosis, thinning of the third ventricle floor, etc.) with minimal axial movement of the endoscope sheath (Fig. 2E&F). A small hole is made for the initial opening at the center of the floor of the third ventricle, and can then be enlarged by micro-balloon inflation (2 French, 60 cm and inflated balloon diameter 5 mm). The tip of the “Handy Rigid-rod Neuroendoscope” is then passed through the ventriculostomized window to confirm opening of the Lilliquest membrane and morphology in the prepontine cistern. Tissue biopsy: By inserting the “Handy Small Diameter Rigid-rod Neuroendoscope” through the peel-away sheath towards the lesion in the dilated or normal-sized or even slit-like ventricle (Fig. 3A), the neuroendoscopy trajectory is reserved with “Endoscope-style Technique” for a peel-
away sheath pacement (Fig. 3B&C). Once the tissue is detached from the body of tumor, the entire endoscope is removed through the guide sheath together with the micro-forceps grasping the tissue. The microforceps and accompanying tissue should not be removed though the
FIG. 2 D: Microperceps micro-scissors technique with right hand.
FIG. 2 E: Micro-balloon technique with the surgeon’s right hand positioning and the assistance’s air inflation via Forgatti micro-balloon.
FIG. 2 F: the Forgatti micro-balloon in flated.
FIG. 2 G: Micro-minopolar Coagulator technique
FIG. 2 H: Micro-Scissers technique
� J. Neuroendoscopy, Vol. 1, No. 1, 2010
F I G . 3 B - 1 & 2 & 3 : A “ E n d o s c o p e - s t y l e t Technique” for a peel-away sheath placement into the slit-like ventricle using a 2mm-diameter lens of “Oi Handy ProTM” as a stylet under endoscopic vision.
B-1
B-3
B-2
FIG. 3 A-1&2: A case of III ventricular tumor without hydrocephalus. Note the size of lateral ventricle remaining slit-like.

�J. Neuroendoscopy, Vol. 1, No. 1, 2010
working channel of the endoscope, as the tissue may be damaged or tip of the microgorceps may become caught at the orifice of the endoscope (Fig. 3C&D). It is easy for the surgeon to move the endoscope in this fashion because of the free-handy maneuver.
Fenestration of cyst wall: In cases such as cystic craniopharyngioma, the cyst wall is fenestrated and Ommaya tube placement is endoscopically assisted through the foramen of Monro. This technique using the “Handy Small Diameter Rigid-rod Neuroendoscope” has been described elsewhere. The wall is soft enough to be penetrated by the micro-forceps, and cystic contents are sucked out using the suction function of the neuroendoscope. The Ommaya tube, inserted via a different burr hole, is grasped within the ventricle and guided to the site of penetration of the tumor in the third ventricle under the neuroendoscopic control.Shunt tube placement: In order to place the ventricular tube for ventriculo-peritoneal (V-P) shunt, the lens of the “Handy Small Diameter Rigid-rod Neuroendoscope” is used. After the ventricle is punctured using a manometric ventricular trocar, the inner stylet with CSF pathway is
removed and data regarding intraventricular pressure is obtained. The fine small diameter lens is inserted through the outer sheath of the trocar, and intraventricular morphology is confirmed to determine the best position for placement of the ventricular tube. The outer sheath allows the ventricular tube to be guided into position through the sheath.
VI. Conclusion
In 1991, our newly developed flexible and steerable fiberoptic operative viewing endoscope for the intracranial use was reported and the system was described (The first Symposium on Treatment for Handrocephalus, July 1991, the paper was published in 1992 [9]). The system has been designed to be steered within the angles of +90 to -130 degree with a miniature high-resolution camera, processor and monitor. This flexible viewing fiber has also a working channel (diameter 1 mm) with a lighting guide and objective lens. Through the channel, the system can provide gentle irrigation in the ventricles with irrigation or passage of microinstruments. However, the clinical application to the various intra-cranial lesions has faced to limitations with disadvantages
FIG. 3 C-1&2&3&4: Toward the III ventricle with the choroid plexus as the land mark in the slit-like lateral ventricle.
C-1
C-2
C-3
C-4

�0 J. Neuroendoscopy, Vol. 1, No. 1, 2010
of the flexible-steerable (fiber) neuroendoscope, i.e. possibility of prion disease, poor quality of imaging compared by size, disorientation, limited instrumentations etc. To conquer these limitations of fiber endoscope, the authors have developed a new type of neuroendoscope, offering improved access to intracranial lesions and maneuverability for various micro-instruments under high-resolution imaging during neuroendoscopic surgery. The endoscope used in this model is a rigid-rod of 2.0 mm diameter with an ovoid cannula of 4.0 mm diameter. The “gun-butt” holder incorporated to the neuroendoscope for use with operator’s left hand provides stability to the holder and allows the endoscope to be handled with improved control. The surgical route is protected by insertion of a 14 French peel-away sheath. Various micro-instruments can be introduced to the operative field through the upper 1/3 of the cannula. These micro-instruments are almost as long as the body of the endoscope, so that direct handling by the right hand of the surgeon allows fine neuroendoscopic surgical maneuvering to be much more readily achieved. The main technical advance with this “Free-hand Maneuver” of the “Handy Small Diameter Rigid-rod Neuroendoscope is one’s ability to hold the endoscope comfortably with one hand and maneuver instruments in and out the field with the other. The results of early clinical experiences, with 0% mortality and morbidity, indicate the utility of these new concepts in both neuroendoscope and neuroendoscopic surgery. [J. Neurosurg (Pediatrics 1) 120: 113 ─ 118, 2005].
Acknowledgement The author is grateful for the technological work by
Mr. Phillip Barger, Karl Storz, Tuttlingen, Germany, and outstanding research works by fellows of “Sami-Oi Scholarship” [sponsored by Karl Storz]: Dr. Nakamasa Hayashi, Dr. Yuichiro Nonaka, Dr. Hideo Hamada, Dr. Shigeki Ono, Dr.Sadahiro Nomura, Dr.Tomoru Miwa, Dr.Kenichi Nishiyama (Japan), Dr. Barback Babapour (Germany), Dr. Federico Di Rocoo (Italy), Dr. Saad H. Abdullah (Jordan), Dr. Senta Kurschel (Austria), Dr. Chen Ge (China), Dr.Nidal Hayel Khasawneh(Amman, Jordan), Dr. Enchev Yovor (Yugoslavia), Dr.Nigel Peter Symss (Chennai, India), Dr. Sang-Dae Kim (Korea) and Dr. John Boor (Kenya).
References
1. Brockmeyer D, Abtin K, Carey L, Walker ML: Endoscopic third ventriculostomy: an outcome analysis. Pediatr Neurosurg. 28 (5): 236─240, 1998
2. Cinalli G, Sainte-Rose C, Chumas P, Zerah M, Brunelle F, Lot G, Pierre-Kahn A, Renier D: Failure of third ventriculostomy in the treatment of aqueductal stenosis in children. J Neurosurg. 90 (3): 448─454, 1999
3. Davis 1: Neurological surgery, Lea & Febiger, Philadelhia, 1936
4. Dandy WE: Extirpation of the choroid plexus of the lateral ventricle in communicating hydrocephalus. Ann Surg: 68: 569─579, 1918
5. Jones RF, Stening WA, Brydon M: Endoscopic third ventriculostomy. Neurosurgery. 26 (1): 86─92, 1990
6. Jones RF, Stening WA, Kwok BC, Stands TM: Third ventriculostomy for shunt infections in children. Neurosurgery. 32 (5): 855─860, 1993
7. Hopf NJ, Grunert P, Fries G, Resch KD, Perneczky A: Endoscopic third ventriculostomy: outcome analysis of 100 consecutive procedures Neurosurgery. 44 (4): 795 ─806, 1999
8. Marzoni FA, Upchurch SE, Lambert CJ: An experimental study of silicone as soft tissue substitute. Plast Reconstr Surg. 24: 600─608, 1959
9. Oi, S, Tominaga S, Yamada H, Shose Y, Urui S, Tamaki N, Yamaguchi, M, Matsumoto S: Neuro-Endoscopic Surgery (Part-1) A newly developed flexible and steerable fiberoptic operative viewing system. Current Treatment for Hydrocephalus (Tokyo) 2: 83─87, 1992
10. Oi S: Recent Advance in Neuroendoscopic Surgery: ─ Realistic indications and clinical achievement─ Critical Reviews of Neurosurgery 6: 64─72, 1996
11. Oi, S, Hidaka M, Tago K, Matsumae M, Takei F, Sato O, Abe H, Tachiiwa M, Sasaki H, Sato Y, Suga K: Neuro-Endoscopic Surgery (Part-3) Characteristics of Rigid, Semi-rigid and Flexible/Steerable Endoscopy: Analysis in Cadaver Dissection, Experimental Animal Model and Clinical Application. Current Tr Hyd (Tokyo) 1995; 5: 57─66, 1996
12. Oi, S, Shibata M, Tominaga J, Honda Y, Shinoda M, Takei F, Tsugane R, Matsuzawa K, Sato O: Efficacy of Neuroendoscopic Procedures in “Minimally-invasive” Preferential Management of Pineal Region Tumors ─ A Prospective Study ─ J. Neurosurg 93: 245─253, 2000
13. Oi S, Shimoda M, Shibata M, Honda Y, Togo K, Shinoda
Fig. 4.D The histological fundings of the biopsied tissue: germ cell tumor.
FIG. 4: The histological fundings of the biopsied tissue: germ cell tumor.

��J. Neuroendoscopy, Vol. 1, No. 1, 2010
M, Tugane R, Sato O: Pathophysiology of Long-standing Overt Ventriculomegaly in Adults. J Neurosurg 92: 933─940, 2000
14. Oi S, Togo K, Matsumae M, Takei F, Hidaka M, Honda Y, Sato O, Iwaki K, Tachiiwa M, Ito M, Suga K: Neuro-Endoscopic Surgery (Part-2) Development and clinical use of microforceps for steerable and flexible Neuro-Endoscope. Current Treatment for Hydrocephalus (Tokyo) 1994 4: 48─53, 1994
15. Oi S, Hidaka M, Honda Y, Togo K. Shinoda M, Shimoda M, Tsugane R, Sato: Neuroendoscopic Surgery for Specific Forms of Hydrocephalus. Child’s Nerv Syst 15: 56─68, 1999
16. Oi S; Kamio, M; Joki, T; Abe, T: Neuroendoscopic anatomy and surgery in pineal region tumors: role of neuroendoscopic procedure in the ‘minimally-invasive preferental’ management. J. Neurosurg 54 (3): 277─286, 2001
17. Oi, S; Abbott, R: Loculated ventricles and isolated compartments in hydrocephalus: their pathophysiology and the efficacy of neuroendoscopic surgery. Neurosurg.
Clin.N.Am. 15 (1): 77─87, 2004 18. O i , S ; S a m i i , A ; S a m i i , M : F r a m e l e s s f r e e -
hand maneuvering of a small-diameter rigid-rod neuroendoscope with a working channel used during high-resolution imaging. Technical note. J. Neurosurg 102 (1) suppl: 113─118, 2005
19. Oi, S; Abdullah, SH : New transparent peel-away sheath with neuroendoscopic orientation markers. Technical note. J. Neurosurg 107 (6): 1244─1247, 2007
20. Oi, S; Enchev, Y: Neuroendoscopic foraminal plasty of foramen of Monro. Childs Nerv. Syst. 24 (8): 933─942, 2008
21. Putnam TH: Treatment of hydrocephalus by endoscopic coagulation of the choroid plexus Description of a new instrument and preliminary report of results. N Engl J Med 210: 1373─1376, 1934
22. Vr ies JK: An endoscopic technique for th i rd ventriculostomy. Surg Neurol. 9 (3): 165─168, 1978
23. Walker ML, Carey L, Brochmeyer DL: The Neuro-Navigational 1.2-mm Neuroview Neuroendoscope. Neurosurgery. 36 (3): 617─618, 1995

�� J. Neuroendoscopy, Vol. 1, No. 1, 2010
Controversy in Neuroendoscopic Third Ventriculostomy: a Current Status Review
Masaki Shinoda M.D.1, Ph.D., Atsushi Murakata M.D.1,Motoharu Fujii M.D., Ph.D.1, Ryoichi Ishikawa M.D.1,Shizuo Oi M.D., Ph.D2. 1Department of Neurosurgery, St. Luke’s International Hospital, Tokyo, Japan2Department of Neurosurgery, Jikei University, Tokyo, Japan
Corresponding Author: Masaki Shinoda M.D., Ph.D.Department of Neurosurgery, St. Luke’s International Hospital9-1 Akashi-cho, Chuo, Tokyo 104-8560, JapanTel: +81-3-3541-5151; Fax: +81-3-3544-0649E mail: [email protected]; ETV, endoscopic third ventriculostomy; VP shunt, ventriculo peritoneal shunt; GCS, Glasgow Coma Scale.
Over 85 years have passed since the first clinical trials of endoscopic ventriculostomy for hydrocephalic patients. Indications for endoscopic third ventriculostomy (ETV) have been expanded to the treatment of not only obstructive hydrocephalus, but also some types of communicating hydrocephalus. While successful results have clearly been obtained for non-communicating hydrocephalus in recent clinical research, the pathological states which for ETV is effective remain enigmatic. ETV has also developed with advances in equipment and techniques. Following the evolution of ETV, complications have also changed and reduced in number. Many authors have reported age limitations for ETV in pediatric populations. This review therefore examined the literature on pathological indications for ETV, age limitations to ETV and complications to date.
Summary
Key Words: endoscopic third ventriculostomy; hydrocephalus; pediatric
Introduction
Many reports have examined the effectiveness and indications of third ventriculostomy for so-
called obstructive hydrocephalus. Third ventriculostomy is one of the most classical treatments for hydrocephalic patients20, 22.Dandy reported the first third ventriculostomy using a subfrontal approach in 192213. Amazingly, Mixter performed the first endoscopic third ventriculostomy the following year43, using a urethroscope to successfully
treat a pediatric hydrocephalic patient. Given the bulky equipment used in endoscopy, several attempts for modified third ventriculostomy were developed. Hoffman et al. reported stereotaxic third ventriculostomy with intraoperative ventriculography using a special apparatus30. Kelly et al. performed CT-guided stereotaxic third ventriculostomy with a ventriculoscope canule35. All cases recovered without shunting. With the development of a neuroendoscopy apparatus, larger numbers of series were reported in the 1990s33, 58, 60.Herein we review the pathological indications and age
REVIEW ARTICLE
Journal of Neuroendoscopy

��J. Neuroendoscopy, Vol. 1, No. 1, 2010
limitations for endoscopic third ventriculostomy (ETV), along with complications encountered to date.
What types of hydrocephalus should be indicated?
Posterior fossa tumor should have one of the best indications for ETV. Fritsch et al. reported that in 23 pediatric patients with hydrocephalus due to posterior fossa tumors, only six patients (11.5%) required permanent treatment for hydrocephalus (VP shunt, n = 4; EVD, n = 223). No pathological differences in outcome were identified23. Al-Tamimi et al. reported on 12 patients under 18 years old who had presented with pineal region tumor and undergone ETV and tumor biopsies2. Eight cases underwent endoscopic biopsy during ETV. Diagnostic sensitivity for endoscopic biopsy is 75%2. In another article on pediatric hydrocephalus with posterior fossa tumors, 107 patients were treated with early posterior fossa surgery (Group 1)45. In that group, 93 patients underwent total or subtotal tumor resection associated with external ventricular drainage (Group 1A), and 14 underwent stereotactic biopsy associated with ETV (Group 1B)45. The 53 remaining patients underwent elective posterior fossa surgery (Group 2)45. Early tumor resection (Group 1A) successfully resolved hydrocephalus in 85 patients (91%), whereas ETV resolved intracranial hypertension in 11 patients (12% of Group 1B)45. In Group 1, persistent hydrocephalus affected 10% of the 107 patients, seven of whom had symptoms and were treated (shunts, n = 3; ETVs, n = 4). Persistent hydrocephalus was more frequent in children with severe preoperative hydrocephalus and with medulloblastomas45. Sainte-Rose reviewed cases of posterior fossa tumors and hydrocephalus divided into three groups: Group A, 67 patients with hydrocephalus present on admission in whom endoscopic third ventriculostomy was performed prior to tumor removal and midline tumor occupied 67 cases (100%); Group B, 82 patients with hydrocephalus who did not undergo preliminary third ventriculostomy but instead received conventional treatment and midline tumor presented on 56 cases (68%); and Group C, 47 patients in whom no ventricular dilation was present on admission and midline tumor appeared in 21 cases (45%)53. There were no significant differences between patients in Group A or B with respect to the following variables: age at presentation, evidence of metastatic disease, extent of tumor resection, or follow-up duration. In patients in Group A, however, more severe hydrocephalus was demonstrated; the patients in Group C were in this respect different from those in the other two groups53. These results mean that ETV was more frequently required prior to tumorectomy with midline tumors53.
Obstructive hydrocephalus shows various causes. Ba ldauf e t a l . r epor ted on ETV for occ lus ive hydrocephalus caused by massive cerebellar infarction5. Ten patients with a mean age of 61.8 years underwent emergency ETV for cerebellar infarction5. Two cases required additional ETV and one case required suboccipital decompression5. Nine of 10 patients showed better GCS after the operation5. Takahashi reported on the use of ETV in patients under 9 months old with obstructive hydrocephalus, classified into three groups based on MRI findings. Group I comprised six patients in whom the frontal horns of the lateral ventricles were enlarged and the cerebral cortical morphology was normal. Group II was made up of 13 patients in whom the entire lateral ventricle was enlarged bilaterally and the cerebral cortical morphology was relatively normal. Group III was composed of six patients in whom the lateral ventricle was markedly enlarged bilaterally and periventricular leakage of cerebrospinal fluid was evident57. Grade I patients showed virtually normal development as of 4 years old57. In Group II, development was still delayed in six patients at 1 year after ETV, and two of these patients underwent shunting. However, all patients in this group showed near-normal development at 5-6 years old57. In Group III, all patients underwent shunting within 1 year after ETV because no appreciable improvement of development was apparent at 6 months after the initial procedure57. Non-communicating hydrocephalus must be a good indication for ETV. A retrospective review from seven international medical centers reported endoscopic third venctriculostomy for pediatric hydrocephalic patients55. No particular discrepancies were seen in the success rates of each institute. Success rates for treating subarachnoid hemorrhage or intraventricular hemorrhage (IVH), cerebrospinal fluid (CSF) infection or a combination of both pathologies were 60.9%, 64.3%, and 23.1%, respectively55. The success rate for the whole group was 60.9%. Among patients ≤15 years old, the success rate was 49.3%, whereas the success rate for adult patients was 78.6%55. A total of 22 technically successful ETV procedures were performed. The ETV success rate for controlling hydrocephalus was 81% and the rate of severe complications was 9%55. O’Brien et al. reported on 170 patients who underwent primary ETV and 63 patients who underwent ETV for VP shunt malfunction, with ETV success rates were 74% and 70%, respectively48. In the primary ETV group, patients with a history of IVH and meningitis as a cause for hydrocephalus showed poor success rates of 27% and 0%, respectively48. O’Brien et al. also reported on the application of ETV and endoscopic tumor biopsy (ETB) in 41 cases with

�� J. Neuroendoscopy, Vol. 1, No. 1, 2010
pediatric midline tumor (pineal, n = 24; tectal plate, n = 9; midbrain, n = 3; thalamus, n = 3)47. ETV success rates of these patients were 68% and no correlation was seen between ETV success rates and prognosis47. Histological examination of biopsy specimens was nondiagnostic in eight cases in which ETB was performed47. Seven of these cases involved pineal region tumors and one involved a tectal plate tumor, and stereotaxic biopsy was added in four cases and craniotomy in one case for diagnosis47. Another article described ETV and ETB in 20 cases with pineal tumor, with pathological confirmation of diagnosis in 15 cases, but lack of verification for the remaining five patients51.Fourth ventricular outlet obstruction (FVOO) is an uncommon cause of obstructive hydrocephalus, most commonly associated with prior IVH or intraventricular infection in children. Mohanty et al. reported 22 FVOO patients, with ETV performed for 10 <2 years old, six between 2 and 18 years old, and six >18 years old42. They classified four groups based on operative findings at basal cisterns: Grade I (clear subarachnoid space, few or no strands) in six patients; Grade II (clear subarachnoid space, few strands) in eight patients; Grade III (mildly hazy space, moderate strands, basilar artery and neural structures still discernible) in three patients; and Grade IV (dense arachnoid strands, no discernible delineation) in three patients42. ETV failed in all infants <6 months old, whereas the success rate was 93% in patients >2 years old (P = 0.0074). A striking correlation was noted between outcome and status of the basal cisterns, with failed procedures in five of six Grade III or IV patients42. In terms of correlating the status of basal cisterns with age, although older children and adults showed relatively clear basal cisterns, whereas arachnoid scarring was more predominant in infants and children <2 years old, the difference did not reach statistical significance42. Thickness of the third ventricular floor observed at surgery and correlations to overall outcome were also not statistically significant, although the procedure failed in five of the nine patients with a non-translucent floor.Decq et al. reported that five young adults with hydrocephalus and showing Chiari type I malformation were treated by endoscopic third venctriculostomy without posterior fossa decompression14. Good results were seen in four cases. Oi et al. reported various types of non-communicating ventricular dilatations, particularly long-standing overt ventriculomegaly in adulthood (LOVA)49, 50, 52. In an early report for seven LOVA patients who underwent ETV and aqueductoplasty, 57% of patients showed excellent results49. Two patients with LOVA needed VP shunt
because it was thought that the endoscopically opened route had been obliterated by the clot or CSF circulation was still poor in the subarachnoid space49. ETV failure may be abrupt in onset, causing a potentially life-threatening increase in intracranial pressure (ICP)4. Aquilina et al. reported the usefulness of a ventricular reservoir as follows: diagnosis of recurrent hydrocephalus by pressure assessment in 19 cases; diagnostic cerebrospinal fluid aspiration in five cases; postoperative external ventricular drainage in four cases; emergency ventricular access for acute recurrence of hydrocephalus in two cases; and diagnosis and management of ventriculitis in two cases (as complications of reservoir operation)4. In cases with ventricular dilatations and adjacent cystic components, neuroendoscopic transventricular ventriculocystostomy was applicable16. Size reduction was achieved for 10 adjacent cysts16. Idiopathic normal pressure hydrocephalus (iNPH) can be difficult to diagnose accurately, and CSF shunt remains the first-choice surgical treatment9. Improvement rates in several recent studies were in 65 ─ 80%36. Gangemi et al. reported that 25 ETVs were performed for patients with iNPH25. Overall rate of neurological improvement after ETV in our series was 72%25. Improvement of gait disturbance was significantly higher (73%) as compared with that of dementia (16%) or urinary incontinence (31%) 25. Gangemi et al. also reported in an ETV multicenter study for iNPH that the rate of neurological improvement was higher in patients with shorter clinical history, better preoperative neurological score, and clinical onset with gait disturbances26. Intraoperative findings of the sudden reappearance of normal cerebral pulsations and significant downward and upward movements of the third ventricular floor after ETV were also correlated with good outcomes for iNPH26.
How young can ETV become applicable?
In recent articles, ETV success rate in adults was 83%, including for tumor, long-standing overt ventriculomegaly, Chiari malformation Types I, II, aqueduct stenosis and IVH32. In the secondary group (shunt malfunction), ETV was successful in 67%32.According to a study of ETV in children <6 months old, ETV was successful in 57% of patients who experienced regression of signs of intracranial hypertension40. Balthasar et al. reported that optimal timing should be ≥ 4 months after birth for ETV from the analysis of 12 cases7. Gorayeb et al. reported that in patients <1 year old (mean, 4.7 months), the success rate was 64% and complications mainly involved meningitis27.

��J. Neuroendoscopy, Vol. 1, No. 1, 2010
Patients with Chiari II malformation and aqueduct stenosis showed lower success rates (45%, 55%) compared with other forms of obstructive hydrocephalus (86%)27. Even infantile ETV patients showed varying success rate between the 1st semester (52%) and 2nd semester (85%)27. A series of ETV in patients <2 years old reported that failed procedures were more frequent in patients <6 months old, and idiopathic aqueductal stenosis with associated hydrocephalus showed a good outcome in 50% of the patients6. Patients older than 1.5 years showed a good success rate6. From an article on ETV performed at <1 year old, median age was 206 days (range, 82 ─311 days) in successful cases and 94 days (range, 8─299 days) in unsuccessful cases37. Navarro et al. identified several significant factors influencing the late ETV failure rate: age <12 months; hydrocephalus without expansive lesions; placement of an external ventricular drain (EVD) after ETV; and development of early complications46. In a series of 18 infantile ETV cases, Infants with obstructive hydrocephalus had a 100% success rate (four of four), and infants with communicating hydrocephalus had a 10% success rate (one of 10). In infants with hydrocephalus related to myelomeningocele, the success rate was 50% (two of four)24. Because of the poor results of ETVs in such cases, they recommend VP shunt for infants with communicating hydrocephalus secondary to IVH or meningitis24. Drake et al. reported that one-year complication –free survival after ETV were less than CSF shun in infant and neonatal periods19. Age is a major determinant of outcome from CSF diversion, with worse outcomes in young patients19. Kadrian et al. reported a retrospective analysis of 181 ETV cases from a single institution and analyzed the long-term reliability of ETV34. The statistical model predicted the following reliability at 1 year after insertion: at 0 ─ 1 month old, 31%; at 1 ─ 6 months old, 50%; at 6 ─ 24 months old, 71%; and at >24 months old, 84%34. Drake et al. combined patients from nine pediatric neurosurgery centers across Canada to obtain a better estimate of outcomes and identify factors affecting the success of ETV18. In the 368 patients, mean age was 6.5 years, and aqueduct stenosis and tumors were the most common etiology18. The 1- and 5-year success rates were 65% and 52%, respectively18. The 5-year success rate in patients <1 month old was 28%, compared with 68% in patients >10 years old18. Multivariate analysis only showed age as having a significant effect on outcome, with younger patients showing higher failure rates, particularly in neonates and infants18. In a series of 275 ETVs, 66 procedures were performed in children <2 years old8. The overall success
rate of ETVs in patients <2 years old in our cohort of patients was 53%8. However, success rates differed markedly between different etiologies of hydrocephalus, varying between 27% in patients with hydrocephalus in association with meningomyelocele with no previous shunting and 87% in patients with aqueductal stenosis8. The success rate in every age group mainly depended on the etiology of hydrocephalus, not on the age of the patient8. A similar conclusion has been reported, that selective use of ETV as the primary treatment for hydrocephalic infants is safe and can lead to an up to 21% reduction in the shunted population of all newly diagnosed patients, and that success of ETV is dependent on etiology, not age31
How to prevent complications?
Late rapid deter iorat ion af ter ETV is a rare complication, but is often fatal17. Seven reports and nine international e-mail interviews have described 16 pediatric cases showing late rapid deterioration after ETV, with fatal outcomes in 13 cases and ETV occlusions in almost all cases17. This phenomenon occurred 1.4 ─ 84 months after ETV (mean, 2.5 years)17. The fatal complication occurs seems to be around 1 in 200 ─ 250 ETVs. Tuli et al. reported that in pediatric CSF shunt mortality rate was 10 deaths per 907 cases, the patients with neoplasms were excluded because their deaths were predominantly related to the tumor59.Whether to use ETV or CSF shunt as the surgical procedure in patients with hydrocephalus remains controversial10, 15, 36, 57. Bilginer et al. reported that ETV for VP shunt malfunction patients, overall success rate for ETV after shunt malfunction was 80% (36 patients) and failure rate was 20% (9 patients)10. Injury to the basilar artery or related branches is a rare but severe complication of ETV1,15,54. Incidence is nearly 1%, practically equivalent to that of the mortality linked to the surgical procedure15. According to Schroeder et al., 22 of 193 patients with ETV experienced complications, comprising 15 adults and seven pediatric patients54. Almost all recovered well, but two patients died (severe meningitis, n = 1; subarachnoid hemorrhage with torn basilar perforators, n = 1)54. They reported complications were more common in the 1990s and became more rare in the 2000s54. CSF leakage is sometimes an intractable complication after ETV. Costa Val reported that in babies within the first 24 months of life with an open anterior fontanel, a curved scalp incision was made over the anterior fontanel12. The fontanel and lateral edge of the frontal bone were exposed and osteoplastic minicraniotomy

�� J. Neuroendoscopy, Vol. 1, No. 1, 2010
was performed12. No cases with CSF leakage and/or complications were encountered12. Kombogiorgas and Sgouros measured sizes of 32 ETV stomas as the distance from the basilar artery to the posterior clinoid process, finding a mean stoma size of 37%38. In patients without previous shunt (n = 17), stoma size >30% associated with ETV success (p = 0.088) 38. CSF leak was adversely associated with ETV success and mean stoma size was 41.3% for successful ETV and 27.8% for unsuccessful ETV38. In patients without previous shunt, stoma size may correlate with success and CSF leak appears strongly associated with failure38. In a study of 155 patients and 173 ETVs, overall complication rate per procedure was 18%21. Cases were divided into three categories showing: intraoperative complications; early postoperative complications (≤1 month); and late complications (>1 month)21. Early postoperative CSF leakage was the most common complication, followed by late postoperative restenosis of stoma21. Complication rate varied significantly with the etiology of hydrocephalus, with patients showing Chiari type I malformation and tumor displaying no or very low complication rates21. The risk of complications was significantly higher for repeat endoscopic procedures (55.5%) than for the first procedure (10%; P = 0.0001)21. Cinalli et al. reported on alterations in ICP after ETV in non-communicating hydrocephalus in pediatric patients11. ICP was continuously recorded for an average of 7 days in 64 children who underwent 68 ETVs for obstructive triventricular hydrocephalus of various etiologies11. After 31 procedures (45.6%), ICP remained normal (<20 mmHg) for the entire duration of monitoring11. After 37 procedures (54.5%), ICP was persistently high on Day 1 (mean, 29.7 mmHg) and decreased very slowly in subsequent days, remaining high for 2-9 days (mean, 4.5 days)11. In 13 patients (19.1%), ETV failed and a ventriculoperitoneal shunt was implanted. After four procedures, the stoma became obstructed and the patients were treated to reopen the stoma11. Postoperative ICP was not significantly higher in patients in whom ETV failed11. Post-ETV infection is one of the most awful complications, occurring in 8.08% / ETV41. This complication usually occurs within the first 2 weeks after ETV41. In an article on ETV with previous shunt operation, a total of 131 patients were identified as comprising 86 patients who underwent ETV as a primary procedure and 45 patients who received ETV at the time of shunt malfunction28. Serious complications after ETV occurred more frequently in patients who presented with shunt malfunction (14 of 45 patients, 31%) compared with patients who underwent primary ETV (7 of 86
patients, 8%)28. Previously shunted patients with a history of two or more revisions and who experienced serious complications at the time of ETV were more likely to require shunt replacement28. In a case of complex shaped hydrocephalus, identifying anatomical structures is sometimes difficult. Hayashi et al. reported a transparent sheath composed of a thin polypropylene outer tube and an obturator29. The sheath measures 10 cm in length, 5.2 mm in outer diameter, and 4.7 mm in inner diameter29. It provides excellent visibility without troublesome bleeding from tissues surrounding the foramen of Monro during rigid endoscopic procedures29.In response to ETV, ventricular volume falls to a value lower than preoperatively, but higher than the normalized value for age and sex56. All patients appeared to have supranormal volumes in the long term, with volume stabilizing at 3─6 months56. Constructive interference in steady-state, 3-dimensional, Fourier transformation (CISS) magnetic resonance imaging in the endoscopic management for 11 of 15 procedures provided better brain tissue/cerebrospinal fluid contrast, allowing better understanding of the cause of hydrocephalus and the nature of the cysts3. CISS is useful to determine the results for ETV3. ETV malfunction can be diagnosed by detecting flow void from the stoma on MRI with T2 sagittal fast spin echo (FSE)44.
Acknowledgements This article was supported by St Luke’s Life Science Institute Research Grant for Clinical Epidemiology Research 2007.
References
1. Abtin K, Thompson BG, Walker ML: Basilar artery perforation as a complication of endoscopic third ventriculostomy. Pediatr Neurosurg 28: 35─41, 1998
2. Al-Tamimi YZ, Bhargava D, Surash S, Ramirez RE, Novegno F, Crimmins DW, et al: Endoscopic biopsy during third ventriculostomy in paediatric pineal region tumours. Childs Nerv Syst 24: 1323─1326, 2008
3. Aleman J, Jokura H, Higano S, Akabane A, Shirane R, Yoshimoto T: Value of constructive interference in steady-state, three-dimensional, Fourier transformation magnetic resonance imaging for the neuroendoscopic treatment of hydrocephalus and intracranial cysts. Neurosurgery 48: 1291─1296, 2001
4. Aquilina K, Edwards RJ, Pople IK: Routine placement of a ventricular reservoir at endoscopic third ventriculo-stomy. Neurosurgery 53: 91─96; discussion 96─97, 2003
5. Baldauf J, Oertel J, Gaab MR, Schroeder HW: Endoscopic third ventriculostomy for occlusive hydrocephalus caused by cerebellar infarction. Neurosurgery 59:539─544; discussion 539─544, 2006
6. Baldauf J, Oertel J, Gaab MR, Schroeder HW:

��J. Neuroendoscopy, Vol. 1, No. 1, 2010
Endoscopic third ventriculostomy in children younger than 2 years of age. Childs Nerv Syst 23: 623─626, 2007
7. Balthasar AJ, Kort H, Cornips EM, Beuls EA, Weber JW, Vles JS: Analysis of the success and failure of endoscopic third ventriculostomy in infants less than 1 year of age. Childs Nerv Syst 23: 151─155, 2007
8. Beems T, Grotenhuis JA: Is the success rate of endoscopic third ventriculostomy age-dependent? An analysis of the results of endoscopic third ventriculostomy in young children. Childs Nerv Syst 18: 605─608, 2002
9. Bergsneider M, Black PM, Klinge P, Marmarou A, Relkin N: Surgical management of idiopathic normal-pressure hydrocephalus. Neurosurgery 57: 29─39, 2005
10. Bilginer B, Oguz KK, Akalan N: Endoscopic third ventriculostomy for malfunction in previously shunted infants. Childs Nerv Syst 25: 683─688, 2009
11. Cinalli G, Spennato P, Ruggiero C, Aliberti F, Zerah M, Trischitta V, et al: Intracranial pressure monitoring and lumbar puncture after endoscopic third ventriculostomy in children. Neurosurgery 58: 126─136; discussion 126─136, 2006
12. Costa Val JA: Minicraniotomy for endoscopic third ventriculostomy in babies: technical note with a 7-year-segment analysis. Childs Nerv Syst 25: 357─359, 2009
13. Dandy WE: An operative procedure for hydrocephalus. Johns Hopkins Hosp Bull 33: 189─190, 1922
14. Decq P, Le Guerinel C, Sol J-C, Brugieres P, Djindjian M, Nguyen J-P: Chiari I malformation: a rare cause of noncommunicating hydrocephalus treated by third ventriculostomy. J Neurosurg 95: 783─790, 2001
15. Di Rocco C, Massimi L, Tamburrini G: Shunts vs endoscopic third ventriculostomy in infants: are there different types and/or rates of complications? A review. Childs Nerv Syst 22: 1573─1589, 2006
16. Di Rocco F, Yoshino M, Oi S: Neuroendoscopic transventricular ventriculocystostomy in treatment for intracranial cysts. J Neurosurg 103: 54─60, 2005
17. Drake J, Chumas P, Kestle J, Pierre-Kahn A, Vinchon M, Brown J, et al: Late rapid deterioration after endoscopic third ventriculostomy: additional cases and review of the literature. J Neurosurg 105: 118─126, 2006
18. Drake JM: Endoscopic third ventriculostomy in pediatric patients: the Canadian experience. Neurosurgery 60: 881─886; discussion 881─886, 2007
19. Drake JM, Kulkarni AV, Kestle J: Endoscopic third ventriculostomy versus ventriculoperitoneal shunt in pediatric patients: a decision analysis. Childs Nerv Syst 25: 467─472, 2009
20. Enchev Y, Oi S: Historical trends of neuroendoscopic surgical techniques in the treatment of hydrocephalus. Neurosurg Rev 31: 249─262, 2008
21. Ersahin Y, Arslan D: Complications of endoscopic third ventriculostomy. Childs Nerv Syst 24: 943─948, 2008
22. Farin A, Aryan HE, Ozgur BM, Parsa AT, Levy ML: Endoscopic third ventriculostomy. J Clin Neurosci 13: 763─770, 2006
23. Fritsch MJ, Doerner L, Kienke S, Mehdorn HM: Hydrocephalus in children with posterior fossa tumors: role of endoscopic third ventriculostomy. J Neurosurg 103: 40─42, 2005
24. Fritsch MJ, Kienke S, Ankermann T, Padoin M, Mehdorn
HM: Endoscopic third ventriculostomy in infants. J Neurosurg 103: 50─53, 2005
25. Gangemi M, Maiuri F, Buonamassa S, Colella G, de Divitiis E: Endoscopic third ventriculostomy in idiopathic normal pressure hydrocephalus. Neurosurgery 55: 129─134; discussion 134, 2004
26. Gangemi M, Maiuri F, Naddeo M, Godano U, Mascari C, Broggi G, et al: Endoscopic third ventriculostomy in idiopathic normal pressure hydrocephalus: an Italian multicenter study. Neurosurgery 63: 62 ─ 67; discussion 67-69, 2008
27. Gorayeb RP, Cavalheiro S, Zymberg ST: Endoscopic third ventriculostomy in children younger than 1 year of age. J Neurosurg (Pediatrics 5) 100: 427─429, 2004
28. Hader WJ, Walker RL, Myles ST, Hamilton M: Complications of endoscopic third ventriculostomy in previously shunted patients. Neurosurgery 63: ONS168─174; discussion ONS174─165, 2008
29. Hayashi N, Hamada H, Umemura K, Kurosaki K, Kurimoto M, Endo S: Transparent endoscopic sheath and rigid-rod endoscope used in endoscopic third ventriculostomy for hydrocephalus in the presence of deformed ventricular anatomy. J Neurosurg 104: 321 ─325, 2006
30. H o ff m a n H J , H a r wo o d - N a s h D , G i l d a y D L : Percutaneous third ventriculostomy in the management of noncommunicating hydrocephalus. Neurosurgery 7: 313─321, 1980
31. Javadpour M, Mallucci C, Brodbelt A, Golash A, May P: The Impact of Endoscopic Third Ventriculostomy on the Management of Newly Diagnosed Hydrocephalus in Infants. Pediatr Neurosurg 35, 2001
32. Jenkinson MD, Hayhurst C, Al-Jumaily M, Kandasamy J, Clark S, Mallucci CL: The role of endoscopic third ventriculostomy in adult patients with hydrocephalus. J Neurosurg 110: 861─866, 2009
33. Jones RF, Stening WA, Brydon M: Endoscopic third ventriculostomy. Neurosurgery 26: 86─91; discussion 91─82, 1990
34. Kadrian D, van Gelder J, Florida D, Jones R, Vonau M, Teo C, et al: Long-term reliability of endoscopic third ventriculostomy. Neurosurgery 56: 1271 ─ 1278; discussion 1278, 2005
35. Kelly PJ, Goerss S, Kall BA, Kispert DB: Computed tomography-based stereotaxic third venctriculostomy: technical note. Neurosurgery 18: 791─794, 1986
36. Klinge P, Marmarou A, Bergsneider M, Relkin N, Black PM: Outcome of shunting in idiopathic normal pressure hydrocephalus and the value of outcome assessment shunted patients. Neurosurgery 57: 40─52, 2005
37. Koch D, Wagner W: Endoscopic third ventriculostomy in infants of less than 1 year of age: which factors influence the outcome? Childs Nerv Syst 20: 405─411, 2004
38. Kombogiorgas D, Sgouros S: Assessment of the influence of operative factors in the success of endoscopic third ventriculostomy in children. Childs Nerv Syst 22: 1256─1262, 2006
39. Kurschel S, Ono S, Oi S: Risk reduction of subdural collections following endoscopic third ventriculostomy. Childs Nerv Syst 23: 521─526, 2007
40. Lipina R, Reguli Š, Doležilová V, Kuncíková M, Podešvová H: Endoscopic third ventriculostomy for

�� J. Neuroendoscopy, Vol. 1, No. 1, 2010
obstructive hydrocephalus in children younger than 6 months of age: is it a first-choice method? Childs Nerv Syst 24: 1021─1027, 2008
41. Lozier AP, Sciacca RR, Romagnoli MF, Connolly ES: Ventriculostomy-related infections: a critical review of the literature. Neurosurgery 51: 170 ─ 182, 2002
42. Mahanty A, Biswas A, Satish S, Vollmer DG: Efficacy of endoscopic third venctriculostomy in fourth ventricular outlet obstruction. Neurosurgey 63: 905 ─ 914, 2008
43. Mixter WJ: Ventriculostomy and puncture of the floor of the third ventricle. Boston Med Surg J 188: 277 ─ 278, 1923
44. Mohanty A, Vasudev MK, Sampath S, Radhesh S, Sastry Kolluri VR: Failed endoscopic third ventriculostomy in children: management options. Pediatr Neurosurg 37: 304 ─ 309, 2002
45. Morelli D, Pirotte B, Lubansu A, Detemmerman D, Aeby A, Fricx C, et al: Persistent hydrocephalus after early surgical management of posterior fossa tumors in children: is routine preoperative endoscopic third ventriculostomy justified? J Neurosurg 103: 247 ─ 252, 2005
46. Navarro R, Gil-Parra R, Reitman AJ, Olavarria G, Grant JA, Tomita T: Endoscopic third ventriculostomy in children: early and late complications and their avoidance. Childs Nerv Syst 22: 506 ─ 513, 2006
47. O'Brien DF, Hayhurst C, Pizer B, Mallucci CL: Outcomes in patients undergoing single-trajectory endoscopic third ventriculostomy and endoscopic biopsy for midline tumors presenting with obstructive hydrocephalus. J Neurosurg 105: 219 ─ 226, 2006
48. O’Brien DF, Javadpour M, Collins DR, Spennato P, Mallucci CL: Endoscopic third ventriculostomy: an outcome analysis of primary cases and procedures performed after ventriculoperitoneal shunt malfunction. J Neurosurg 103: 393 ─ 400, 2005
49. Oi S, Hidaka M, Honda Y, Togo K, Shinoda M, Shimoda M, et al: Neuroendoscopic surgery for specific forms of hydrocephalus. Childs Nerv Syst 15: 56 ─ 68, 1999
50. Oi S, Sato O, Matsumoto S: Neurological and medico-social problems of spina bifida patients in adolescence
and adulthood. Childs Nerv Syst 12: 181 ─ 187, 1996 51. Oi S, Shibata M, Tominaga J, Honda Y, Shinoda M,
Takei F, et al: Efficacy of neuroendoscopic procedures in minimally invasive preferential management of pineal region tumors: a prospective study. J Neurosurg 93: 245 ─253, 2000
52. Oi S, Shimoda M, Shibata M, Honda Y, Togo K, Shinoda M, et al: Pathophysiology of long-standing overt ventriculomegaly in adults. J Neurosurg 92: 933 ─ 940, 2000
53. Sainte-Rose C, Cinalli G, Roux FE, Maixner R, Chumas PD, Mansour M, et al: Management of hydrocephalus in pediatric patients with posterior fossa tumors: the role of endoscopic third ventriculostomy. J Neurosurg 95: 791 ─797, 2001
54. Schroeder HW, Niendorf WR, Gaab MR: Complications of endoscopic third ventriculostomy. J Neurosurg 96: 1032 ─ 1040, 2002
55. Siomin V, Cinalli G, Grotenhuis A, Golash A, Oi S, Kothbauer K, et al: Endoscopic third ventriculostomy in patients with cerebrospinal fluid infection and/or hemorrhage. J Neurosurg 97: 519 ─ 524, 2002
56. St George E, Natarajan K, Sgouros S: Changes in ventricular volume in hydrocephalic children following successful endoscopic third ventriculostomy. Childs Nerv Syst 20: 834 ─ 838, 2004
57. Takahashi Y: Long-term outcome and neurologic development after endoscopic third ventriculostomy versus shunting during infancy. Childs Nerv Syst 22: 1591 ─ 1602, 2006
58. Teo C, Jones R: Management of hydrocephalus by endoscopic third ventriculostomy in patients with myelomeningocele. Pediatr Neurosurg 25: 57 ─ 63; discussion 63, 1996
59. Tuli S, Tuli J, Drake J, Spears J: Predictors of death in pediatric patients requiring cerebrospinal fluid shunts. J Neurosurg (5 Suppl Pediatrics) 100: 442 ─ 446, 2004
60. Wong TT, Lee LS: A method of enlarging the opening of the third ventricular floor for flexible endoscopic third ventriculostomy. Childs Nerv Syst 12: 396 ─ 398, 1996

��J. Neuroendoscopy, Vol. 1, No. 1, 2010
[NEOL: VTE]
NEOL: VTE No.001
From Basic to Most Advanced Neuroendoscopic Technique with “Oi Handy ProTM”
Prof. Shizuo OI, M.D., Ph.D.
NEUROENDOSCOPY
On-line Video Technical Education
16
NEUROENDOSCOPY Online Video Technical Education
No.001
From Basic to Most Advanced Neuroendoscopic
Technique with “Oi Handy ProTM”
Prof. Shizuo OI, M.D., Ph.D
Journal of Neuroendoscopy

�0 J. Neuroendoscopy, Vol. 1, No. 1, 2010
NEUROENDOSCOPIC SURGERY On-line Video Technical Education
NEOL: VTE No.001
From Basic to Most Advanced Neuroendoscopic Technique with “Oi Handy ProTM”
Prof. Shizuo OI, M.D., Ph.D. Head, Divisions of Pediatric Neurosurgery, Professor, Departments of Neurosurgery, The Jikei University of Medicine (JWCMC), Tokyo, JapanDirector and Professor of Pediatric Neurosurgery,International Neuroscience Institute (INI), Hannover, Germany
SummaryConcept of “Oi Handy ProTM” NeuroendoscopeThe “Oi HandyProTM” endoscope is the result of several years of neuroenoscopy invention. The author’s experience, as well as that of other colleagues, has formed the basis for the design of a new device with potential for improving certain features of the endoscope used in the neurosurgical field. It is a handy rigid-shaft neuroendoscope that combines several major advantages; high-resolution imaging with right illumination, mobile manipulation with “frameless free-hand maneuvering,” and a lightweight body with fine surgical instruments. This new instrument is presented and its unique features as they relate to neurosurgery are described.
On-line Access: www.karlstorz.com
©08/2007The contents of this presentation may be presented to third parties exclusively for scientific purposes, upon condition that the author is mentioned upon presentation.Any copies or extracts require explicit permission.KARL STORZ GmbH & Co. KGMillelstresse8 78532 Tuttlingen - GermanyPostbox230 78503 Tuttlingen - GermanyTel: +49 (0) 7461 708-0 Fax: +49 (0) 7461 708-105E-mail: [email protected]
The Master’s Neurodoscopic Surgical Technique.

��J. Neuroendoscopy, Vol. 1, No. 1, 2010
[NEOL: JCC]
NEOL: JCC No.001
Indication for Neuroendoscopic Surgery
Part 1: Arachnoid Cyst
NEUROENDOSCOPY
On-line Journal Consensus Conference
Journal of Neuroendoscopy

�� J. Neuroendoscopy, Vol. 1, No. 1, 2010
NEOL: JCC No.001 Indication for Neuroendoscopic SurgeryPart 1: Arachnoid Cyst
Case No.1 A 7-year- old-male with Left Middle Fossa Arachnoid Cyst
History: The patient underwent CT study with an episode of minor head injury. The CT demonstrated a giant size of arachnoid cyst in left middle fossa extending to left cerebral convexity. He is right- handed but has no specific symptom.
Neurological Examination:The neurological examination revealed no neurological deficit. His intelligence quotient (IQ) was 147 [performance 157, verbal 137].
Neuroimaging: (CT scan)
Our Dicision Making: Absolutely no surgical indication. Just follow up.
QUESTION No.1 What is your opinion?No.2 How would you approach, if indicated for surgery?

��J. Neuroendoscopy, Vol. 1, No. 1, 2010
Journal of Neuroendoscopy
“My Opinion”[ ]Fax: 0081-3-3235-9377 [ ]e-mail: [email protected]
NEUROENDOSCOPY On-line Journal Consensus Conference [NEOLJCC]
on NEOLJCC No.
[ ] I agree! [ ] I disagree!
How would you approach, if indicated for surgery?[ ] Open Surgery [ ] Neuroendoscopic ApproachComment
Name: ,M.D.Institute: City: ,Country[ ] I permit the above opinion and comment to be published with my name andinstitute/country in “Journal of Neuroendoscopy”.[ ] e-mail address: @