jr pud presentation
TRANSCRIPT

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 1/79
2/5/20112/5/2011 11
The digestive
system
includes the
organs that
ingest food,
transport food,
digest the food into smaller
usable
components,
absorb the
nutr ients, and
expel the waste
products from
the body.

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 2/79
2/5/20112/5/2011 22
Stomach

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 3/79
2/5/20112/5/2011 33
Gastric
ruga
e allowstretching of
the stomach
Note greater and
lesser curvatures

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 4/79
2/5/20112/5/2011 44
GastritisGastritis Acute Gastritis Acute Gastritis is an inflammation of theis an inflammation of thegastric mucosa.gastric mucosa.
GastropathyGastropathy: epithelial or endothelial: epithelial or endothelialdamage without inflammationdamage without inflammation
Gastritis has 3 basic types:Gastritis has 3 basic types: ± ± Acute (erosive/ hemorrhagic) Acute (erosive/ hemorrhagic)
± ± NonNon--erosive, Nonerosive, Non--specific/Chronicspecific/Chronic
± ± Special FormsSpecial Forms

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 5/79
2/5/20112/5/2011 55
Acute Gastritis Acute Gastritis
(Erosive/Hemorrhagic)(Erosive/Hemorrhagic)
Most common causes:Most common causes: ± ± NSAIDS gastric injury by diminishingNSAIDS gastric injury by diminishing
prostaglandin production in stomach andprostaglandin production in stomach and
duodenumduodenum ± ± Alcohol use is the Alcohol use is the leading cause of gastritisleading cause of gastritis
± ± Stress from CNS injury burns, sepsis, surgeryStress from CNS injury burns, sepsis, surgery
± ± Portal hypertension (portal gastropathy)Portal hypertension (portal gastropathy)
Other causes:Other causes:
± ± ingestioningestion
± ± radiationradiation

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 6/79
2/5/20112/5/2011 66
Chronic GastritisChronic Gastritis
Nonerosive/nonspecificNonerosive/nonspecificInfectious gastritis Type B:Infectious gastritis Type B: H Pylori H Pylori ± ± Involves antrum and body of stomachInvolves antrum and body of stomach
majority of patients asymptomaticmajority of patients asymptomatic
± ± Strong association with PUDStrong association with PUD ± ± 2 to 6 fold risks of gastric adenocarcinoma and also2 to 6 fold risks of gastric adenocarcinoma and alsogastric lymphomagastric lymphoma
Autoimmune gastritis Type A: Pernicious anemia Autoimmune gastritis Type A: Pernicious anemia ± ± Body and fundus, It usually spares the antrum & affectsBody and fundus, It usually spares the antrum & affects
the parietal cells.the parietal cells. ± ± Pernicious anemia caused by impaired absorption of Pernicious anemia caused by impaired absorption of
vitamin Bvitamin B--1212 occurs due to lack of intrinsic factor fromoccurs due to lack of intrinsic factor fromparietal cells and decrease in acid productionparietal cells and decrease in acid production
± ± Increased risk of adenocarcinomaIncreased risk of adenocarcinoma

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 7/79
2/5/20112/5/2011 77
Special forms of GastritisSpecial forms of Gastritis
Infectious (Phlegmonous or necrotizing gastritis)Infectious (Phlegmonous or necrotizing gastritis) ± ± Emergency gastric resection, and Abx therapyEmergency gastric resection, and Abx therapy
± ± CMV, candidal (fungal) in immunocompromised pt¶sCMV, candidal (fungal) in immunocompromised pt¶s
± ± Larvae ingestion requires endoscopic removalLarvae ingestion requires endoscopic removal
Eosinophilic GastritisEosinophilic Gastritis
Giant Cell (Menetrier¶s disease) (HypertrophicGiant Cell (Menetrier¶s disease) (HypertrophicGastropathy)Gastropathy) ± ± only found on biopsyonly found on biopsy
Lymphocytic GastritisLymphocytic Gastritis
Granulomatous GastritisGranulomatous Gastritis ± ± TuberculosisTuberculosis
± ± SyphilisSyphilis
± ± FungalFungal
± ± SarcoidSarcoid
± ± Crohn¶sCrohn¶s

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 8/79

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 9/79
2/5/20112/5/2011 99
GastritisGastritisLab:Lab: ± ± Endoscopy c/ biopsy is the gold standardEndoscopy c/ biopsy is the gold standard
± ± A urea breath test A urea breath test
± ± Specific test for underlying conditions (e.g) B12 and CBC for Specific test for underlying conditions (e.g) B12 and CBC for pernicious anemiapernicious anemia
Differential Diagnosis:Differential Diagnosis: ± ± 1. Peptic ulcer 1. Peptic ulcer 2. Gastroparesis2. Gastroparesis
± ± 3. Gastric carcinoma3. Gastric carcinoma 4. GERD4. GERD
± ± 5. Pancreatitis5. Pancreatitis 6. Lymphoma6. Lymphoma
Treatment:Treatment: (same as duodenal ulcers)(same as duodenal ulcers)
± ± Remove irritantRemove irritant
± ± Treat for H pyloriTreat for H pylori
± ± Antacids & H2 blockers Antacids & H2 blockers
± ± Avoid smoking & alcohol Avoid smoking & alcohol

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 10/79
2/5/20112/5/2011 1010
Peptic Ulcer DiseasePeptic Ulcer Disease
DefinitionDefinition: PUD is describes: PUD is describesany ulcer of the upperany ulcer of the upperdigestive tract.digestive tract. (duodenal #(duodenal #1)1)
and stomachand stomach (gastric #2)(gastric #2)Break in the duodenal orBreak in the duodenal or
gastric mucosa extendinggastric mucosa extendingthrough the muscularisthrough the muscularis
mucosae, and are usuallymucosae, and are usually5mm5mm--1cm.1cm.

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 11/79
2/5/20112/5/2011 1111
R ead about peptic ulcers
in the clinical view in the
text

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 12/79
2/5/20112/5/2011 1212
Zollinger Zollinger--Ellison SyndromeEllison Syndrome
UlcersUlcers--associatedassociated
with thewith the Zollinger Zollinger--
Ellison (ZE)Ellison (ZE)Syndrome (#3Syndrome (#3) are) are
caused by gastrincaused by gastrin--
releasing islet cellreleasing islet cell
tumors (gastrinomas),tumors (gastrinomas),
& are also considered& are also considered
a form of peptic ulcer.a form of peptic ulcer.
8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 13/79
2/5/20112/5/2011 1313
Zollinger Zollinger--Ellison SyndromeEllison Syndrome A tumor of the pancreas that secretes gastrin A tumor of the pancreas that secretes gastrin
((Gastrinoma)Gastrinoma)
Usually found in head of pancreas but can alsoUsually found in head of pancreas but can alsobe found in duodenum, liver & lungbe found in duodenum, liver & lung
7575--80% of ulcers produced develop in the80% of ulcers produced develop in theduodenal bulbduodenal bulb
Suspect in any patient with:Suspect in any patient with: ± ± Multiple or recurring duodenal ulcersMultiple or recurring duodenal ulcers
± ± Post bulbar or jejunal ulcersPost bulbar or jejunal ulcers
± ± Ulcers associated with diarrheaUlcers associated with diarrhea
± ± Elevated serum gastrin levelsElevated serum gastrin levels
Usually only tested when suspect ZE syndromeUsually only tested when suspect ZE syndrome

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 14/79
2/5/20112/5/2011 1414
Peptic Ulcer Disease (PUD)Peptic Ulcer Disease (PUD)
Men 3 : 1 WomenMen 3 : 1 Women
Most commonly occur inMost commonly occur in::
± ± #1 Duodenum (Duodenal)#1 Duodenum (Duodenal)
± ± #2 Stomach (Gastric)#2 Stomach (Gastric)
± ± EsophagusEsophagus
± ± GastroentericGastroentericanastomosesanastomoses
± ± Meckel¶s DiverticulumMeckel¶s Diverticulum

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 15/79
2/5/20112/5/2011 1515
PUDPUDThe spectrum of the disease is broad from mild mucosalThe spectrum of the disease is broad from mild mucosalinjury to frank ulcerations.injury to frank ulcerations.
Symptoms vary and are not related to the severity of Symptoms vary and are not related to the severity of tissue damage.tissue damage.
11--2% of population have an ulcer at the present time2% of population have an ulcer at the present time
10% of population will have ulcer in their lifetime10% of population will have ulcer in their lifetime
Gastric and Duodenal ulcers tend to recur in the sameGastric and Duodenal ulcers tend to recur in the same
location.location.
Recurrent hemorrhage occurs in 50% of patients whoRecurrent hemorrhage occurs in 50% of patients whohave had a prior bleed.have had a prior bleed.

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 16/79
2/5/20112/5/2011 1616
Duodenal Ulcer vs. Gastric Ulcer Duodenal Ulcer vs. Gastric Ulcer
DuodenalDuodenal ± ± Increased acidIncreased acid
productionproduction
± ± H. pyloriH. pylori
± ± relieved by foodrelieved by food &&
typically awakenstypically awakens
patient around 1:00ampatient around 1:00am
GastricGastric ± ± Normal or decreasedNormal or decreased
acid productionacid production
± ± Decreased mucosalDecreased mucosal
resistanceresistance
± ± H. pyloriH. pylori
± ± NSAIDSNSAIDS
± ± worsened by foodworsened by food

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 17/79
2/5/20112/5/2011 1717
Duodenal Vs. Gastric (cont)Duodenal Vs. Gastric (cont)DuodenalDuodenal
± ± Onset more common age 25Onset more common age 25to 55to 55
± ± never malignantnever malignant
± ± mostly located in the duodenalmostly located in the duodenal
bulb or immediately post bulbar.bulb or immediately post bulbar. ± ± Ulcers distal to the duodenalUlcers distal to the duodenalbulb should raise suspicion for bulb should raise suspicion for Zollinger Zollinger--Ellison SyndromeEllison Syndrome(also c/ multiple frequently(also c/ multiple frequentlyoccurring duodenal ulcers.)occurring duodenal ulcers.)
± ± Men 3:1 WomenMen 3:1 Women
± ± Duodenal 5 times moreDuodenal 5 times morecommon than gastriccommon than gastric
± ± 6060--80% have recurrence within80% have recurrence withinone year.one year.
GastricGastric ± ± Onset more common ageOnset more common age
40 to 7040 to 70
± ± BenignBenign more likely @more likely @lesser curvature/lesser curvature/ antrumantrum
± ± Gastric ulcers are moreGastric ulcers are morecommon @ lesser common @ lesser curvaturecurvature
± ± Malignancies more likelyMalignancies more likely
@ greater curvature@ greater curvature
± ± 11--3% occur in carcinomas3% occur in carcinomas

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 18/79
2/5/20112/5/2011 1818
PUD EtiologiesPUD Etiologies
1.1. Helicobacter pylori (H. pylori) infection: (#1 cause)Helicobacter pylori (H. pylori) infection: (#1 cause)
± ± A. Associated c/ 70 A. Associated c/ 70--95% of Peptic ulcers.95% of Peptic ulcers.
± ± B. Treatment of H. pylori improves healing rate & markedlyB. Treatment of H. pylori improves healing rate & markedly
decreases the recurrence rate.decreases the recurrence rate.
2.2. NSAIDS: (#2 cause)NSAIDS: (#2 cause) (inhibit prostaglandins which normally(inhibit prostaglandins which normally
stimulate production of mucous secretions & bicarb.)stimulate production of mucous secretions & bicarb.)
± ± A. may cause gastric or duodenal ulcers (steroids also) A. may cause gastric or duodenal ulcers (steroids also)
± ± B. accounts for the majority of non H. pylori ulcersB. accounts for the majority of non H. pylori ulcers

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 19/79
2/5/20112/5/2011 1919
PUD Etiologies (cont)PUD Etiologies (cont)
3.3.H
ypersecretion states: (#3 althoughH
ypersecretion states: (#3 althoughuncommon)uncommon) ± ± Gastrinomas (Zollinger Gastrinomas (Zollinger--Ellison Syndrome)Ellison Syndrome)
± ± Multiple endocrine neoplasia (MENMultiple endocrine neoplasia (MEN--1)1)
4. Stress:4. Stress: physiologic stressphysiologic stress (eg. Burns,(eg. Burns,surgery, & severe medical conditions)surgery, & severe medical conditions)
5. Rare causes: viral, radiation, vascular insuff.5. Rare causes: viral, radiation, vascular insuff.
Diseases assoc. c/ peptic ulcers:Diseases assoc. c/ peptic ulcers: ± ± Cirrhosis, renal failure, pulmonary ds.Cirrhosis, renal failure, pulmonary ds.
Any pt. c/ systemic ds. (COPD, renal failure, cirrhosis of liver) Any pt. c/ systemic ds. (COPD, renal failure, cirrhosis of liver)are prone to ulcers so should be started on H2 blockers.are prone to ulcers so should be started on H2 blockers.

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 20/79
2/5/20112/5/2011 2020
The pathogenesis of PUD is related to theThe pathogenesis of PUD is related to the
imbalance between normal protective factors andimbalance between normal protective factors and
injurious factorsinjurious factorsNo Ulcer No Ulcer
± ± NormalNormal
Ulcer Ulcer
Aggressive forces Aggressive forces ± ± Gastric acidGastric acid
± ± Digestive enzymesDigestive enzymes
Vs.Vs.
Defensive forcesDefensive forces ± ± MucusMucus
± ± BicarbBicarb
± ± ProstaglandinsProstaglandins
± ± Epithelial regenerationEpithelial regeneration

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 21/79
2/5/20112/5/2011 2121
Ulcers result from:Ulcers result from:
1. Increased aggression1. Increased aggression
± ± H. pylori infectionH. pylori infection
± ± NSAIDSNSAIDS
± ± CigarettesCigarettes
Or Or
2. Impaired Defense2. Impaired Defense ± ± IschemiaIschemia
± ± Prostaglandin Inhibition (NSAIDS)Prostaglandin Inhibition (NSAIDS)
± ± Delayed gastric emptyingDelayed gastric emptying

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 22/79
2/5/20112/5/2011 2222
PUDPUD
ADVERSE EFFECTS OF SMOKING ADVERSE EFFECTS OF SMOKING
± ± 1. Interferes c/ action of H2 antagonists1. Interferes c/ action of H2 antagonists
± ± 2. Increases rate of gastric emptying2. Increases rate of gastric emptying ± ± 3. Increases duodenogastric reflux3. Increases duodenogastric reflux
± ± 4. Decreases pancreatic bicarb secretion4. Decreases pancreatic bicarb secretion
± ± 5. Decreases mucosal blood flow5. Decreases mucosal blood flow
± ± 6. Depresses gastric mucosal prostaglandin6. Depresses gastric mucosal prostaglandin
synthesissynthesis

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 23/79
2/5/20112/5/2011 2323

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 24/79
2/5/20112/5/2011 2424
Peptic Ulcer Disease FactsPeptic Ulcer Disease FactsMost ulcers are caused by H. pyloriMost ulcers are caused by H. pylori
inf ection, not spicy food, acid or stress.infection, not spicy food, acid or stress.
You can test for You can test for H. pylori H. pylori infection.infection.
H. pylori H. pylori / ulcers can be tx¶d c/ antibiotics./ ulcers can be tx¶d c/ antibiotics.
Complications:Complications:
± ± A Major complication is bleeding & perforation A Major complication is bleeding & perforation
± ± Erosion of a small vessel at the base of theErosion of a small vessel at the base of theulcer is the cause of the bleedingulcer is the cause of the bleeding
± ± Perforation is usually catastrophic causingPerforation is usually catastrophic causingperitonitisperitonitis

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 25/79
2/5/20112/5/2011 2525
What is H. pyloriWhat is H. pylori
Helicobacter pylori Helicobacter pylori ((H. pylori H. pylori ) is a) is agram negative spiralgram negative spiral--shaped bacillusshaped bacillusfound in the gastric mucous layer or found in the gastric mucous layer or
adherent to the epithelial lining of theadherent to the epithelial lining of thestomach.stomach.
H. pylori H. pylori causes more than 90% of causes more than 90% of duodenal ulcers and up to 80% of duodenal ulcers and up to 80% of gastric ulcers.gastric ulcers.

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 26/79
2/5/20112/5/2011 2626
How do people get infected withHow do people get infected with
H. pylori H. pylori ??
It is not known howIt is not known how H. pylori H. pylori is transmitted or is transmitted or why some patients become symptomatic whilewhy some patients become symptomatic whileothers do not.others do not.
The bacteria are most likely spread from personThe bacteria are most likely spread from personto person through fecalto person through fecal--oral or oraloral or oral--oral routes.oral routes.
Possible environmental reservoirs include:Possible environmental reservoirs include: ± ± contaminated water sourcescontaminated water sources
± ± Iatrogenic spread through contaminated endoscopesIatrogenic spread through contaminated endoscopeshas been documented but can be preventedhas been documented but can be prevented

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 27/79
2/5/20112/5/2011 2727
What can people do to preventWhat can people do to prevent H.H.
pylori pylori infection? infection?
Since the source of Since the source of H. pylori H. pylori is not yet known,is not yet known,
recommendations for avoiding infection haverecommendations for avoiding infection have
not been made.not been made.
In general, it is always wise for persons to washIn general, it is always wise for persons to wash
hands thoroughly, to eat food that has beenhands thoroughly, to eat food that has been
properly prepared, and to drink water from aproperly prepared, and to drink water from a
safe, clean source.safe, clean source.

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 28/79
2/5/20112/5/2011 2828
H. pylori H. pylori infectioninfectionBefore this bacterium was discovered, spicyBefore this bacterium was discovered, spicy
food, acid, stress, and lifestyle were consideredfood, acid, stress, and lifestyle were consideredthe major causes of ulcers.the major causes of ulcers.
The majority of patients were given longThe majority of patients were given long--termterm
medications, such as H2 blockers, and moremedications, such as H2 blockers, and morerecently, proton pump inhibitors, without arecently, proton pump inhibitors, without achance for permanent cure.chance for permanent cure.
These medications relieve ulcer These medications relieve ulcer--relatedrelatedsymptoms, heal gastric mucosal inflammation,symptoms, heal gastric mucosal inflammation,and may heal the ulcer, but they do NOT treatand may heal the ulcer, but they do NOT treatthe infection.the infection.

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 29/79
2/5/20112/5/2011 2929
H. Pylori H. Pylori infectioninfection
When acid suppression is removed, the majorityWhen acid suppression is removed, the majorityof ulcers, particularly those caused byof ulcers, particularly those caused by H. pylori H. pylori ,,recur.recur.
Since we now know that most ulcers are causedSince we now know that most ulcers are causedbyby H. pylori H. pylori , appropriate antibiotic regimens can, appropriate antibiotic regimens cansuccessfully eradicate the infection in mostsuccessfully eradicate the infection in most
patients, with complete resolution of mucosalpatients, with complete resolution of mucosalinflammation and a minimal chance for inflammation and a minimal chance for recurrence of ulcers.recurrence of ulcers.

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 30/79
2/5/20112/5/2011 3030
What illnesses doesWhat illnesses does H. pylori H. pylori
cause?cause?Most persons who are infected with H. pylori never suffer Most persons who are infected with H. pylori never suffer any symptoms related to the infection; however,any symptoms related to the infection; however, H. pylori H. pylori causes chronic active, chronic persistent, and atrophiccauses chronic active, chronic persistent, and atrophicgastritis in adults and children.gastritis in adults and children.
Infection withInfection with H. pylori H. pylori also causes duodenal and gastricalso causes duodenal and gastriculcers. Infected persons have a 2ulcers. Infected persons have a 2-- to 6to 6--fold increasedfold increasedrisk of developing gastric cancer and mucosalrisk of developing gastric cancer and mucosal--associatedassociated--lymphoidlymphoid--type (MALT) lymphoma comparedtype (MALT) lymphoma compared
with their uninfected counterparts.with their uninfected counterparts.
The role of The role of H. pylori H. pylori in nonin non--ulcer dyspepsia remainsulcer dyspepsia remainsunclear.unclear.

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 31/79
2/5/20112/5/2011 3131
Peptic Ulcer Disease SymptomsPeptic Ulcer Disease Symptoms
#1. Epigastric Pain#1. Epigastric Pain
± ± BurningBurning
± ± Occurs 1Occurs 1--3 hrs p/ meals3 hrs p/ meals
± ± Relieved by foodRelieved by food
± ± May occur @ nightMay occur @ night ± ± May radiate to back or May radiate to back or
shoulders if perforatedshoulders if perforated
NauseaNausea
VomitingVomiting
± ± May be related to partial or May be related to partial or
complete gastric outletcomplete gastric outlet
obstructionobstruction
DyspepsiaDyspepsia
± ± Belching/ BloatingBelching/ Bloating
HeartburnHeartburnChest DiscomfortChest Discomfort
Anorexia Anorexia
Weight lossWeight loss ± ± In gastric ulcers (also inIn gastric ulcers (also in
pancreatic ds.)pancreatic ds.)Weight gainWeight gain ± ± In duodenal ulcersIn duodenal ulcers
Hematemesis or melenaHematemesis or melena ± ± Due to GI bleedingDue to GI bleeding
± ± If severe = hematocheziaIf severe = hematochezia

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 32/79
2/5/20112/5/2011 3232
Who should be tested andWho should be tested and
treated for treated for H. pylori H. pylori ??
Persons with active gastric or duodenalPersons with active gastric or duodenalulcers or documented history of ulcersulcers or documented history of ulcers
should be tested for should be tested for H. pylori H. pylori , and if found, and if foundto be infected, they should be treated.to be infected, they should be treated.
To date, there has been no conclusiveTo date, there has been no conclusiveevidence that treatment of evidence that treatment of H. pylori H. pylori infection in patients with noninfection in patients with non--ulcer ulcer dyspepsia is warranted.dyspepsia is warranted.

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 33/79
2/5/20112/5/2011 3333
PUD TestsPUD Tests
Laboratory Test:Laboratory Test: ± ± Routine tests are of little importance. Having a CBC isRoutine tests are of little importance. Having a CBC is
helpful.helpful.
Upper GI endoscopy c/ biopsy*Upper GI endoscopy c/ biopsy*
Upper GI series (barium) (limited today)Upper GI series (barium) (limited today)Serum TestSerum Test ± ± Amylase Amylase
± ± ElectrolytesElectrolytes
± ± Serum Gastrin level if ZE syndrome is suspectedSerum Gastrin level if ZE syndrome is suspectedFrequently occurring duodenal ulcers or multipleFrequently occurring duodenal ulcers or multipleDuodenal Ulcers*Duodenal Ulcers*

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 34/79
2/5/20112/5/2011 3434
How isHow is H. pylori H. pylori infection diagnosed?infection diagnosed?Several methods may be used to diagnoseSeveral methods may be used to diagnose H. pylori H. pylori
infection.infection.Serological testsSerological tests that measure specificthat measure specific H. pylori H. pylori IgGIgGantibodies can determine if a person has been infected.antibodies can determine if a person has been infected. ± ± The sensitivity and specificity of these assays around 80%The sensitivity and specificity of these assays around 80%
Fecal Antigen AssayFecal Antigen Assay
Urea Breath testUrea Breath test ± ± In this test, the patient is given either 13CIn this test, the patient is given either 13C-- or 14Cor 14C--labeled urea tolabeled urea to
drink.drink.
± ± H. pylori H. pylori metabolizes the urea rapidly, and the labeled carbon ismetabolizes the urea rapidly, and the labeled carbon is
absorbed.absorbed. ± ± This labeled carbon can then be measured as CO2 in the patient'sThis labeled carbon can then be measured as CO2 in the patient's
expired breath to determine whether expired breath to determine whether H. pylori H. pylori is present.is present.
± ± The sensitivity and specificity of the breath test ranges from 94%The sensitivity and specificity of the breath test ranges from 94%to 98%.to 98%.

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 35/79
2/5/20112/5/2011 3535
How isHow is H. pylori H. pylori infection in PUDinfection in PUD
diagnosed? diagnosed?
Upper Upper endoscopyendoscopy(esophagogastroduodenal) is(esophagogastroduodenal) is
considered the reference method of considered the reference method of
diagnosis.diagnosis.

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 36/79
2/5/20112/5/2011 3636
Dx of Dx of H. pylori H. pylori by Endoscopyby Endoscopy
During endoscopy, biopsy specimens of theDuring endoscopy, biopsy specimens of thestomach and duodenum are obtained and thestomach and duodenum are obtained and thediagnosis of diagnosis of H. pylori H. pylori can be made by severalcan be made by severalmethods:methods:
± ± The biopsy urease testThe biopsy urease test -- a colorimetric test based ona colorimetric test based onthe ability of the ability of H. pylori H. pylori to produce urease; it providesto produce urease; it providesrapid testing at the time of biopsy.rapid testing at the time of biopsy.
± ± Histologic identification of organismsHistologic identification of organisms -- considered theconsidered the
gold standard of diagnostic tests.gold standard of diagnostic tests. ± ± Culture of biopsy specimens for Culture of biopsy specimens for H. pylori,H. pylori, whichwhich
requires an experienced laboratory and is necessaryrequires an experienced laboratory and is necessarywhen antimicrobial susceptibility testing is desiredwhen antimicrobial susceptibility testing is desired

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 37/79
2/5/20112/5/2011 3737
Peptic Ulcer Disease TherapyPeptic Ulcer Disease TherapyNonNon--PharmacologicalPharmacological
± ± Diet change is of no valueDiet change is of no value
± ± Smoking CessationSmoking CessationSmoking delays healingSmoking delays healing
± ± DC medications that enhance the progressionDC medications that enhance the progression
NSAIDSNSAIDSPharmacological TherapyPharmacological Therapy ± ± Inhibit secretion of acidInhibit secretion of acid
± ± Neutralizing gastric acidsNeutralizing gastric acids
± ± Augmentation of protection of mucosa Augmentation of protection of mucosa ± ± Antibiotics prn Antibiotics prn
Maintenance TherapyMaintenance Therapy ± ± Prevention c/ colloid bismuthPrevention c/ colloid bismuth
± ± Bedtime dosage of H2 blockersBedtime dosage of H2 blockers

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 38/79
2/5/20112/5/2011 3838
Peptic Ulcer Disease TherapyPeptic Ulcer Disease Therapy
Pharmacological TherapyPharmacological Therapy
± ± Inhibition of acidInhibition of acid
H2 blockersH2 blockers
Antacids Antacids
Proton pump inhibitorsProton pump inhibitors
Anticholinergics Anticholinergics
ProstaglandinsProstaglandins
Augmentation protection Augmentation protection

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 39/79
2/5/20112/5/2011 3939
Peptic Ulcer Disease TherapyPeptic Ulcer Disease Therapy
Antacids Antacids (magnesium, aluminum, & calcium based)(magnesium, aluminum, & calcium based)
± ± cause diarrheacause diarrhea
Moderate to high doses of H2 blockers result inModerate to high doses of H2 blockers result inimproved healing ratesimproved healing rates
± ± Used 1 hr PC & HS for 6Used 1 hr PC & HS for 6--8 wks8 wks
± ± Side effects:Side effects:Hypermagnesemia (careful in renal patients)Hypermagnesemia (careful in renal patients)
Aluminum causes phosphate depletion & osteoporosis Aluminum causes phosphate depletion & osteoporosis
Sodium overload in CHFSodium overload in CHF
Hypercalcium causing Milk alkali syndromeHypercalcium causing Milk alkali syndrome
Inhibits absorption of antibiotics, digoxin, warfarinInhibits absorption of antibiotics, digoxin, warfarin

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 40/79
2/5/20112/5/2011 4040
PUD Therapy (cont)PUD Therapy (cont)
Proton Pump Inhibitors:Proton Pump Inhibitors:
± ± Inhibit the H,KInhibit the H,K--ATPase pump ATPase pump
± ± Healing rate 80Healing rate 80--100%100%
± ± Prilosec (Omeprazole)Prilosec (Omeprazole)
Anticholinergics: reduce acid by 50% and Anticholinergics: reduce acid by 50% and
cause blurred visioncause blurred vision ± ± pupil dilation, consider pt¶s occupation or driving restrictionpupil dilation, consider pt¶s occupation or driving restriction

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 41/79
2/5/20112/5/2011 4141
PUD Therapies (cont)PUD Therapies (cont)
Prostaglandins (Do not use in pregnancy)Prostaglandins (Do not use in pregnancy) ± ± Inhibit the parietal cell cyclic AMP function inInhibit the parietal cell cyclic AMP function in
response to histamineresponse to histamine
± ± Healing rate are equal to H2 blockersHealing rate are equal to H2 blockers
± ± Primary role is to be used as a prophylactic agent toPrimary role is to be used as a prophylactic agent toprevent NSAID induced ulcers. Not used as aprevent NSAID induced ulcers. Not used as aprimary therapyprimary therapy
± ± Mosoprostol (Cytotec)Mosoprostol (Cytotec)
Sucralfate (Carafate) its action is unknownSucralfate (Carafate) its action is unknown ± ± It forms a viscous shield over the mucosaIt forms a viscous shield over the mucosa
± ± Absorbs bile & pepsin Absorbs bile & pepsin
8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 42/79
2/5/20112/5/2011 4242
What ar the tr eat ent r egi ens sed f r What ar e the tr eat ent r egi ens sed f r
H . l ri H . l ri er adi ati n?er adi ati n?
Curr ent ther apy f r Curr ent ther apy f r H
. l ri H
. l ri inf ecti n consists of inf ection consists of 10 days to 2 weeks of one or two eff ective 10 days to 2 weeks of one or two eff ective antibiotics,antibiotics, ± ± amoxicillin,amoxicillin,
± ± tetracyclinetetracycline
not to be used for children <12 yrsnot to be used for children <12 yrs ± ± metronidazole, or metronidazole, or
± ± clarithromycin,clarithromycin,
Plus either Plus either ± ± ranitidine bismuth citrate (H2 blocker),ranitidine bismuth citrate (H2 blocker),
± ± bismuth subsalicylate (peptobismuth subsalicylate (pepto--bismol),bismol),
± ± or proton pump inhibitor . or proton pump inhibitor .

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 43/79
2/5/20112/5/2011 4343
PUD Therapies (cont)PUD Therapies (cont)
Acid suppression by the H2 blocker or Acid suppression by the H2 blocker or
proton pump inhibitor in conjunction withproton pump inhibitor in conjunction with
the antibiotics helpsthe antibiotics helps
± ± alleviate ulcer alleviate ulcer--related symptoms (i.e.,related symptoms (i.e.,
abdominal pain, nausea),abdominal pain, nausea),
± ± helps heal gastric mucosal inflammation,helps heal gastric mucosal inflammation,
± ± and may enhance efficacy of the antibioticsand may enhance efficacy of the antibioticsagainstagainst H. pylori H. pylori at the gastric mucosalat the gastric mucosal
surface.surface.

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 44/79
2/5/20112/5/2011 4444
H. Pylori TxH. Pylori Tx
Currently, eightCurrently, eight H. pylori H. pylori treatment regimens aretreatment regimens areapproved by the Food and Drug Administrationapproved by the Food and Drug Administration(FDA); however, several other combinations(FDA); however, several other combinationshave been used successfully.have been used successfully.
Antibiotic resistance and patient noncompliance Antibiotic resistance and patient noncomplianceare the two major reasons for treatment failure.are the two major reasons for treatment failure.
Overall, triple therapy regimens have shownOverall, triple therapy regimens have shownbetter eradication rates than dual therapy. better eradication rates than dual therapy. Longer length of treatment (14 days versus 10Longer length of treatment (14 days versus 10days) results in better eradication rates.days) results in better eradication rates.

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 45/79
2/5/20112/5/2011 4545
FDAFDA--approved treatment optionsapproved treatment options
1. Omeprazole 40 mg QD + clarithromycin 500 mg TID x1. Omeprazole 40 mg QD + clarithromycin 500 mg TID x
2 wks, then omeprazole 20 mg QD x 2 wks2 wks, then omeprazole 20 mg QD x 2 wks--OROR--
2. (Zantac) Ranitidine bismuth citrate (RBC) 400 mg BID2. (Zantac) Ranitidine bismuth citrate (RBC) 400 mg BID
+ clarithromycin 500 mg TID x 2 wks, then RBC 400 mg+ clarithromycin 500 mg TID x 2 wks, then RBC 400 mg
BID x 2 wksBID x 2 wks--OROR--
3. Bismuth subsalicylate (Pepto Bismol®) 525 mg QID +3. Bismuth subsalicylate (Pepto Bismol®) 525 mg QID +
metronidazole 250 mg QID + tetracycline 500 mg QID* xmetronidazole 250 mg QID + tetracycline 500 mg QID* x
2 wks + H2 receptor antagonist therapy as directed x 42 wks + H2 receptor antagonist therapy as directed x 4
wkswks
--OROR--
4. Lansoprazole 30 mg BID + amoxicillin 1 g BID +4. Lansoprazole 30 mg BID + amoxicillin 1 g BID +
clarithromycin 500 mg TID x 10 daysclarithromycin 500 mg TID x 10 days

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 46/79
2/5/20112/5/2011 4646
FDAFDA--approved treatment optionsapproved treatment options
(cont.)(cont.)
5.5. --OROR-- Lansoprazole 30 mg TID + amoxicillin 1 g TID xLansoprazole 30 mg TID + amoxicillin 1 g TID x2 wks**2 wks**
6.6. --OROR-- Rantidine bismuth citrate 400 mg BID +Rantidine bismuth citrate 400 mg BID +clarithromycin 500 mg BID x 2 wks, then RBC 400 mgclarithromycin 500 mg BID x 2 wks, then RBC 400 mgBID x 2 wksBID x 2 wks
7.7. --OROR-- Omeprazole 20 mg BID + clarithromycin 500 mgOmeprazole 20 mg BID + clarithromycin 500 mg
BID + amoxicillin 1 g BID x 10 daysBID + amoxicillin 1 g BID x 10 days
8.8. --OROR-- Lansoprazole 30 mg BID + clarithromycin 500Lansoprazole 30 mg BID + clarithromycin 500mg BID + amoxicillin 1 g BID x 10 daysmg BID + amoxicillin 1 g BID x 10 days
LongLong term consequences ofterm consequences of HH
8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 47/79
2/5/20112/5/2011 4747
LongLong--term consequences of term consequences of H.H.
pylori pylori infection? infection?
Recent studies have shown an associationRecent studies have shown an associationbetween longbetween long--term infection withterm infection with H. pylori H. pylori andandthe development of the development of gastric cancer gastric cancer..
Gastric cancer is the second most commonGastric cancer is the second most commoncancer cancer worldwideworldwide; it is most common in; it is most common incountries such as Colombia and China, wherecountries such as Colombia and China, whereH. pylori H. pylori infects over half the population in earlyinfects over half the population in early
childhood.childhood.
In the United States, whereIn the United States, where H. pylori H. pylori is lessis lesscommon in young people, gastric cancer ratescommon in young people, gastric cancer rates
have decreased.have decreased.
8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 48/79
2/5/20112/5/2011 4848
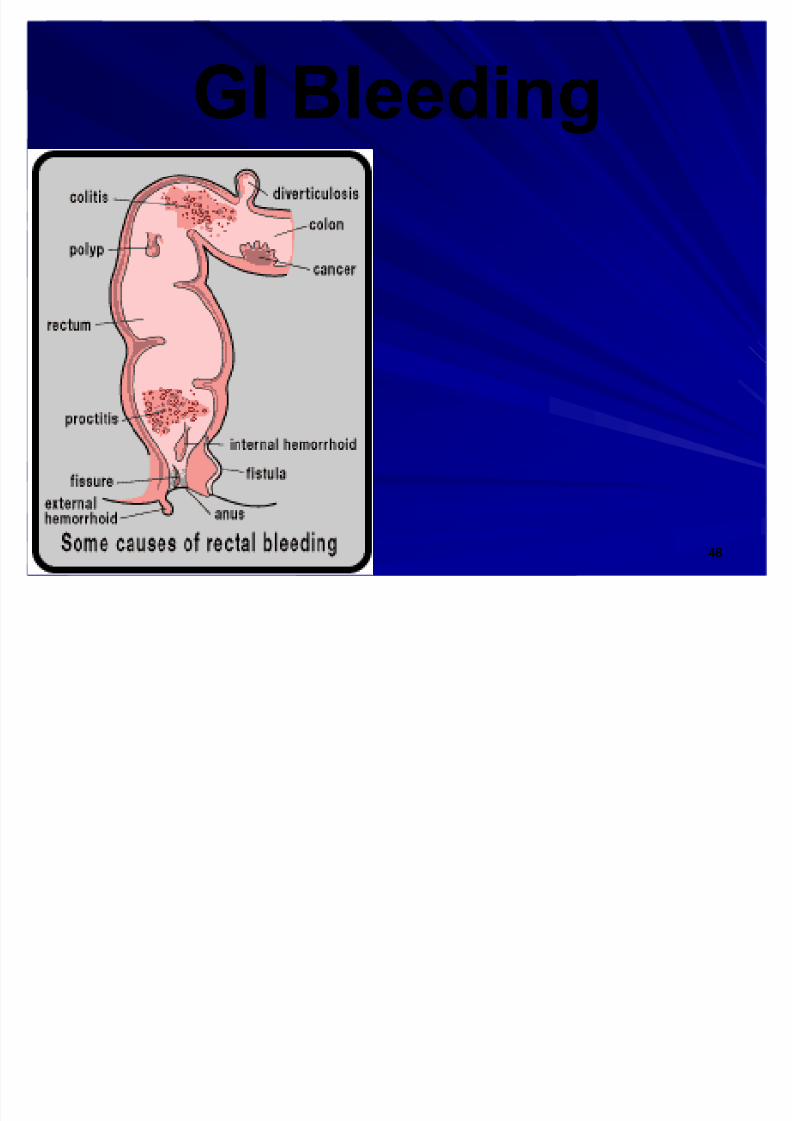
GI BleedingGI Bleeding

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 49/79
2/5/20112/5/2011 4949
Gastrointestinal BleedingGastrointestinal Bleeding
May present as:May present as:
± ± Occult blood (not visualized)Occult blood (not visualized)
± ± Melena (black stool)Melena (black stool)
± ± Hematemesis (vomiting blood)Hematemesis (vomiting blood)
± ± Hematochezia (passage in stool)Hematochezia (passage in stool)

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 50/79
2/5/20112/5/2011 5050
Kinds of GI BleedingKinds of GI Bleeding
HematemesisHematemesis ± ± Rapid bleed: vomiting bright red bloodRapid bleed: vomiting bright red blood
± ± Slow bleed: ³coffeeSlow bleed: ³coffee--grounds´grounds´
MelenaMelena ± ± Black tarry stoolBlack tarry stool
± ± Source:Source:Upper GIUpper GI
Or lower GI to right colonOr lower GI to right colon
HematocheziaHematochezia ± ± Bright red blood in stoolBright red blood in stool
± ± Source:Source:Lower GILower GI
Or Upper GI if massiveOr Upper GI if massive

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 51/79
2/5/20112/5/2011 5151
Occult bloodOccult blood
Hemacult/Guiaic is the most commonly used testHemacult/Guiaic is the most commonly used testFalse positives <2%False positives <2%
Obtain 2 different samples from 2 stools over a 3 dayObtain 2 different samples from 2 stools over a 3 dayperiodperiod
Laxatives alter results causing both falseLaxatives alter results causing both false--positive andpositive andfalsefalse--negative resultsnegative results
False positive results from food rich in peroxidaseFalse positive results from food rich in peroxidase ± ± Bloody meatsBloody meats
± ± BroccoliBroccoli
± ± TurnipsTurnips ± ± Cauliflower Cauliflower
False negatives from taking Vit. C or food containingFalse negatives from taking Vit. C or food containingvitamin Cvitamin C
Neoplasms is #1 cause of occult blood lossNeoplasms is #1 cause of occult blood loss

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 52/79
2/5/20112/5/2011 5252
Guiaic/ HemoccultGuiaic/ Hemoccult

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 53/79
2/5/20112/5/2011 5353
Causes of GI bleeding by locationCauses of GI bleeding by location
Upper GIUpper GI ± ± #1 PUD#1 PUD
DuodenalDuodenal
GastricGastric
± ± Esophageal varicesEsophageal varices(Secondary to portal HTN)(Secondary to portal HTN)
± ± MalloryMallory--Weiss tear Weiss tear (Mucosal laceration @ EG(Mucosal laceration @ EG
junction) junction)
± ± GastritisGastritis
Lower GILower GI ± ± #1 Hemorrhoids#1 Hemorrhoids
± ± #2 Anal Fissure#2 Anal Fissure
± ± DiverticulosisDiverticulosis ± ± IntussusceptionIntussusception
Upper & Lower GIUpper & Lower GI
± ± NeoplasmsNeoplasms ± ± Angiodysplasias Angiodysplasias(Osler¶s disease)(Osler¶s disease)

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 54/79
2/5/20112/5/2011 5454
GI BleedGI Bleed
GI bleeding is a powerful laxativeGI bleeding is a powerful laxativeGI bleeding may be life threateningGI bleeding may be life threatening
GI bleeding may be acute or chronicGI bleeding may be acute or chronic
Adult anemia is secondary to GI bleeding Adult anemia is secondary to GI bleedinguntil proven otherwiseuntil proven otherwise
GI bleeding is secondary to GI bleeding is secondary to
cancer until proven otherwise cancer until proven otherwise

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 55/79
2/5/20112/5/2011 5555
GI BleedGI Bleed
Nature & duration helps with evaluationNature & duration helps with evaluationPresence of pain is importantPresence of pain is important
Watch for associated symptoms: fever, weight lossWatch for associated symptoms: fever, weight loss
Medication and past surgery historyMedication and past surgery history
The initial step is assessment of hemodynamic status.The initial step is assessment of hemodynamic status.
A systolic BP <100mm Hg is high risk c/ acute A systolic BP <100mm Hg is high risk c/ acute
bleeding.bleeding.
CAN BE MASSIVE AND DEADLYCAN BE MASSIVE AND DEADLY
MUST BE TREATED RAPIDILY AND AGGRESSIVELYMUST BE TREATED RAPIDILY AND AGGRESSIVELY
ALWAYS R/O CANCER ALWAYS R/O CANCER

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 56/79
2/5/20112/5/2011 5656
Upper GI bleedUpper GI bleed
4x more common than lower GI4x more common than lower GI
bleedbleed
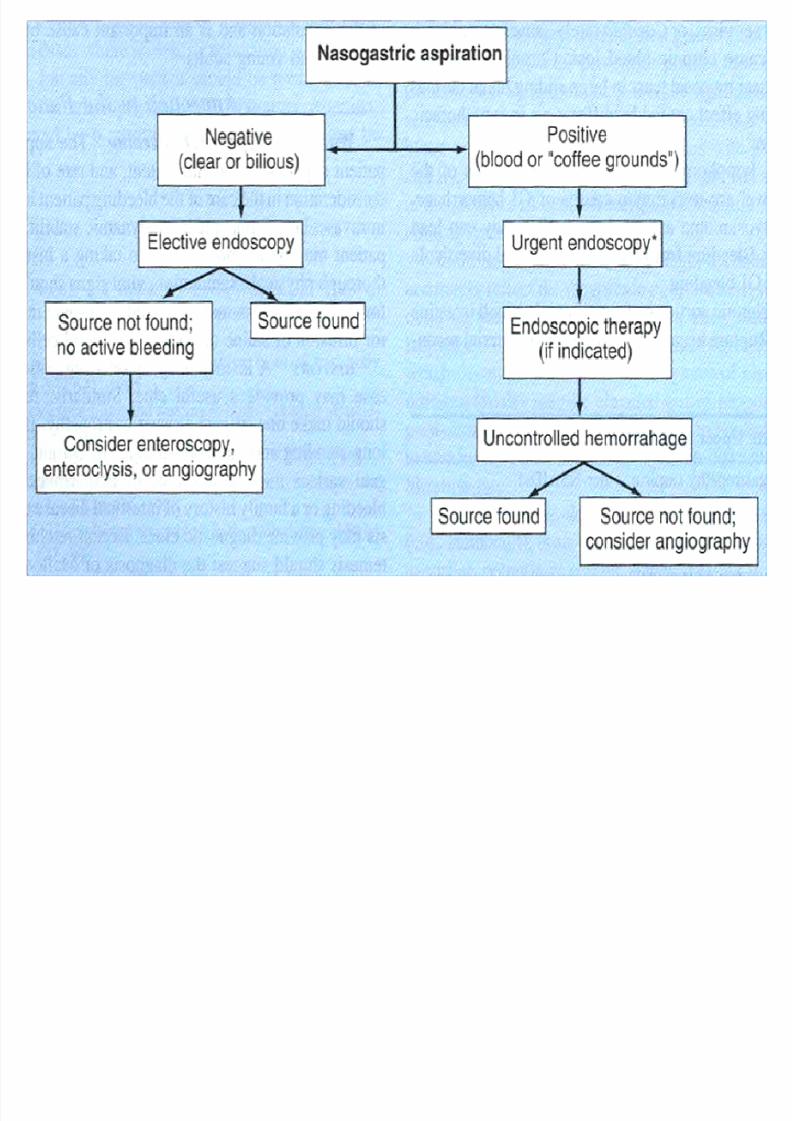
R/O upper GI source by NG tubeR/O upper GI source by NG tube
aspirateaspirate

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 57/79
2/5/20112/5/2011 5757
Upper GI Differential Dx aidsUpper GI Differential Dx aids
Signs of chronic liver diseaseSigns of chronic liver disease
implicates bleeding due to portal HTN.implicates bleeding due to portal HTN.
A hx of dyspepsia, NSAID use, or PUD,A hx of dyspepsia, NSAID use, or PUD,
suggests Peptic Ulcer .suggests Peptic Ulcer .
Acute bleeding after heavy alcoholAcute bleeding after heavy alcohol
ingestion or retching suggests aingestion or retching suggests a
MalloryMallory--Weiss tear .Weiss tear .
8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 58/79
2/5/20112/5/2011 5858
Lower GI bleedsLower GI bleeds
HematocheziaHematochezia
± ± (however, 10% is from upper GI source)(however, 10% is from upper GI source)
Defined as below ligament of TreitzDefined as below ligament of Treitz ± ± (divides duodenum/ jejunum)(divides duodenum/ jejunum)
95% from Colon95% from Colon
Less likely than Upper GI bleed to presentLess likely than Upper GI bleed to presentin shock, or require transfusionin shock, or require transfusion
85% spontaneous cessation85% spontaneous cessation

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 59/79
2/5/20112/5/2011 5959
Complications of GI bleedComplications of GI bleed
DIC from both massive blood loss &DIC from both massive blood loss &
coagulationcoagulation
MultiMulti--organ failureorgan failure
Hemodynamic collapseHemodynamic collapse
Hyper Hyper--ammonia toxicityammonia toxicity
Hepatorenal failureHepatorenal failureEncephalopathyEncephalopathy

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 60/79
2/5/20112/5/2011 6060
8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 61/79
2/5/20112/5/2011 6161

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 62/79
2/5/20112/5/2011 6262
8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 63/79
2/5/20112/5/2011 6363
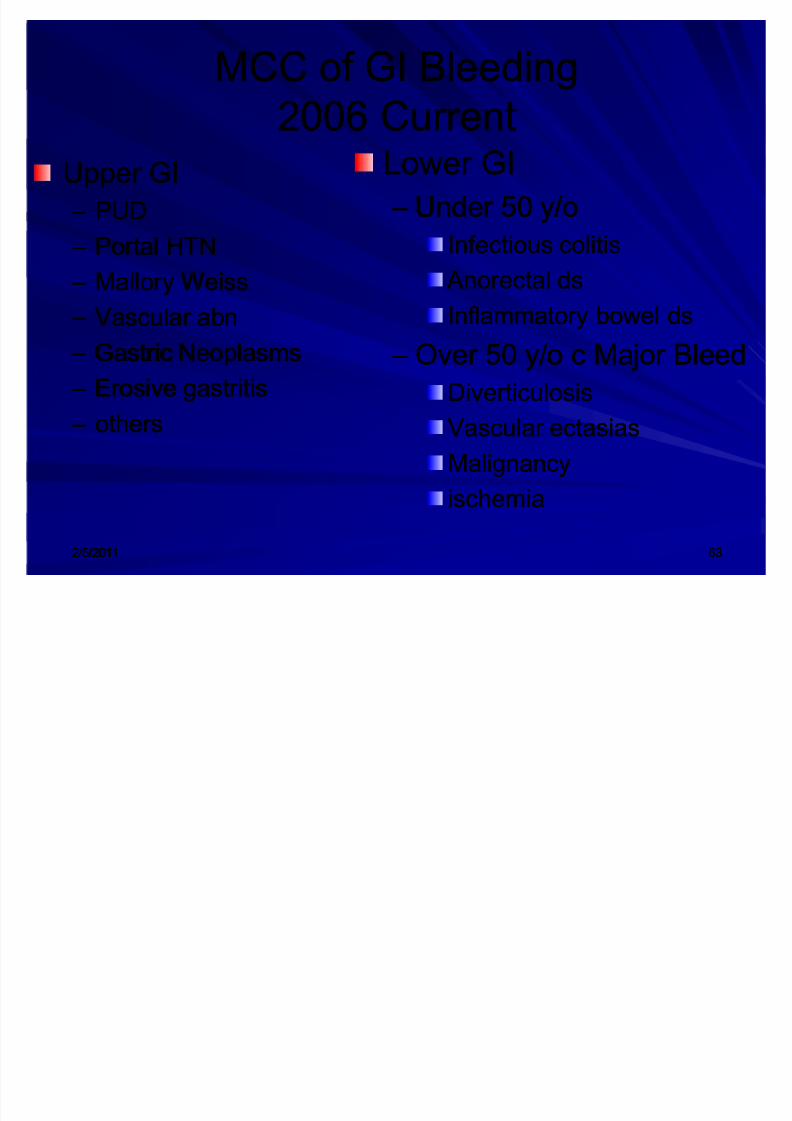
MCC of GI BleedingMCC of GI Bleeding
2006 Current2006 Current
Upper GIUpper GI
± ± PUDPUD
± ± Portal HTNPortal HTN
± ± Mallory WeissMallory Weiss ± ± Vascular abnVascular abn
± ± Gastric NeoplasmsGastric Neoplasms
± ± Erosive gastritisErosive gastritis
± ± othersothers
Lower GILower GI
± ± Under 50 y/oUnder 50 y/o
Infectious colitisInfectious colitis
Anorectal ds Anorectal dsInflammatory bowel dsInflammatory bowel ds
± ± Over 50 y/o c Major BleedOver 50 y/o c Major Bleed
DiverticulosisDiverticulosis
Vascular ectasiasVascular ectasias
MalignancyMalignancy
ischemiaischemia

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 64/79
2/5/20112/5/2011 6464
GI BLEED

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 65/79
2/5/20112/5/2011 6565
LABS
1.CBC
1.PT/PTT/Thrombin time- DIC panel (FSPfibrin split products, fibrinogen, FDPfibrin degradation products, clottingtime, D dimer assay)
2.Electrolytes/BUN/creatinine
3.Blood Type and Cross match
4.CXR/ AXR rarely helpful only if perforated
GI BLEED

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 66/79
2/5/20112/5/2011 6666
Anoscopy/ Sigmoidoscopy VS. Anoscopy/ Sigmoidoscopy VS.
ColonoscopyColonoscopy
Anoscopy/Anoscopy/
SigmoidoscopySigmoidoscopy
± ± Acceptable in <45 yo Acceptable in <45 yo
otherwise healthy tootherwise healthy toevaluate for:evaluate for:
Anorectal ds. Anorectal ds.
Inflammatory bowel ds.Inflammatory bowel ds.
Infectious colitisInfectious colitis
± ± If lesion found, noIf lesion found, no
further eval neededfurther eval needed
ColonscopyColonscopy
± ± Used DiagnosticallyUsed Diagnostically
and Therapeuticallyand Therapeutically
± ± All >40 All >40--45 yo c/ +45 yo c/ +guiaic or Fe+guiaic or Fe+
deficiency anemiadeficiency anemia

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 67/79
2/5/20112/5/2011 6767
Flex SigFlex Sig

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 68/79
2/5/20112/5/2011 6868
Anoscopy/ Rigid Sigmoidoscopy Anoscopy/ Rigid Sigmoidoscopy

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 69/79
2/5/20112/5/2011 6969
Super Duper Pooper Scooper Super Duper Pooper Scooper

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 70/79
2/5/20112/5/2011 7070
ColonoscopyColonoscopy

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 71/79
2/5/20112/5/2011 7171
8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 72/79
2/5/20112/5/2011 7272

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 73/79
2/5/20112/5/2011 7373

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 74/79
2/5/20112/5/2011 7474
U t t f U GIU t t f U GI

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 75/79
2/5/20112/5/2011 7575
Urgent management of Upper GIUrgent management of Upper GI
bleedsbleeds2 Large bore IV lines need started c/ colloid solution2 Large bore IV lines need started c/ colloid solutionstarted until PRBC can be infused, if needed.started until PRBC can be infused, if needed.
OctreotideOctreotide-- Decreases portal HTN (it is administeredDecreases portal HTN (it is administeredpromptly to all patients with active upper GI bleeds,promptly to all patients with active upper GI bleeds,and liver ds, or known portal HTN, until source can beand liver ds, or known portal HTN, until source can be
ID¶d by endoscopy.ID¶d by endoscopy.PPI¶s reduce risk of rebleed in PUDPPI¶s reduce risk of rebleed in PUD
EndoscopyEndoscopy ± ± To ID sourceTo ID source
± ± Determine risk of rebleedDetermine risk of rebleed ± ± HemostasisHemostasis
Other Tx modalities (used only if endoscopy fails)Other Tx modalities (used only if endoscopy fails) ± ± Angiographic embolization Angiographic embolization
± ± Transvenous shunts (for portal HTN, and variceal bleeds)Transvenous shunts (for portal HTN, and variceal bleeds)

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 76/79
2/5/20112/5/2011 7676
ReviewReviewAcute Erosive GastritisAcute Erosive Gastritis ± ± D/C NSAIDS or add misoprostolD/C NSAIDS or add misoprostol
± ± If bleeding caused by ASA; consider plateletIf bleeding caused by ASA; consider plateletadministrationadministration
± ± Sucralfate/ H2 antagonistsSucralfate/ H2 antagonists
Chronic Gastritis (Nonerosive)Chronic Gastritis (Nonerosive) ± ± Type AType A
Eradicate H. pylori: amox + tetracycline + PPIEradicate H. pylori: amox + tetracycline + PPI
± ± Type BType BTreat pernicious anemia: monthly lifelong IM B12Treat pernicious anemia: monthly lifelong IM B12
Specific Types of GastritisSpecific Types of Gastritis

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 77/79
2/5/20112/5/2011 7777
ReviewReviewPeptic Ulcer DiseasePeptic Ulcer Disease
± ± Almost all need Pepsin, Acid, & Almost all need Pepsin, Acid, & H. pylori H. pylori to form ulcer to form ulcer
± ± Eradicate H. pyloriEradicate H. pylori
± ± Endoscopic bx to exclude adenocarcinomaEndoscopic bx to exclude adenocarcinomarecommended for all patientsrecommended for all patients
± ± If refractory: obtain fasting serum gastrin levels toIf refractory: obtain fasting serum gastrin levels to
exclude Zollinger exclude Zollinger--EllisonEllison
± ± Consider parietal cell vagotomy.Consider parietal cell vagotomy.Partial gastrectomy c/ gastroPartial gastrectomy c/ gastro--duodenostomy (Billroth I) or duodenostomy (Billroth I) or
gastrojejunostomy (Billroth II) are rarely used now.gastrojejunostomy (Billroth II) are rarely used now.

8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 78/79
2/5/20112/5/2011 7878
ReviewReviewUpper GI BleedUpper GI Bleed ± ± Evaluate hemodynamic status, stabilizeEvaluate hemodynamic status, stabilize
± ± Nasogastric tubeNasogastric tube
± ± OctreotideOctreotide
± ± Endoscopy if bleeding is severe enough toEndoscopy if bleeding is severe enough torequire blood transfusionsrequire blood transfusions
± ± Bleeding from esophageal varices: endoscopicBleeding from esophageal varices: endoscopicsclerotherapy preferredsclerotherapy preferred
8/7/2019 jr pud presentation
http://slidepdf.com/reader/full/jr-pud-presentation 79/79
ReviewReviewLower GI BleedLower GI Bleed
± ± T he most common cause of significant bleeding isT he most common cause of significant bleeding is
diverticular bleeding; that of intermittent minor diverticular bleeding; that of intermittent minor
hematochezia is hemorrhoidal bleeding hematochezia is hemorrhoidal bleeding
± ± Evaluate hemodynamic status, stabilizeEvaluate hemodynamic status, stabilize
± ± Colonoscopy if bleeding is severe or patient >50 yrsColonoscopy if bleeding is severe or patient >50 yrs
(neoplasms)(neoplasms)
± ± If bleeding continues consider nuclear bleeding scan or If bleeding continues consider nuclear bleeding scan or
mesenteric angiography (often of limited use if mesenteric angiography (often of limited use if
bleeding is slow or intermittent), or Intrableeding is slow or intermittent), or Intra--arterialarterial
vasopressin or embolization.vasopressin or embolization.
±± Surgery as last resortSurgery as last resort