k - 37 introduction anestesia (anestesia &...
TRANSCRIPT
1
1
INTRODUCTION OF
ANESTHESIA
Departement of Anestesiology and Reanimation , School of Medicine,
Sumatera Utara University2
History of
Anesthesia
3Living Made Easy: Prescription for Scolding Wives [1830]
4
Hinkley, an American portrait painter who studied at the Paris Ecole des Beaux Arts, in 1882 began his
painting of the ether demonstration as a speculative work and took 11 years to complete it.
The Hinkley painting today hangs in the Francis A. Countway Library of Medicine at
Harvard Medical School in Boston. .
2
5 6
7
Ether Monument, Boston Public GardenPhotographs from the Detroit Publishing Company, 1880-1920
American Memory Collection aLibrary of Congress 8
History of Anesthesia History of Anesthesia History of Anesthesia History of Anesthesia
A history of anesthesia or "pain killing" techniques A history of anesthesia or "pain killing" techniques A history of anesthesia or "pain killing" techniques A history of anesthesia or "pain killing" techniques throughout historythroughout historythroughout historythroughout history
Anesthesia, historical background and the word's originPainPainPainPain, however useful as a warning signal designed to keep living organisms from damaging themselves too badly, becomes useless
agony when operations must be performed.Attempts to control pain were many. The use of alcohol or some form of what came to be called hypnotism was old. Acupuncture
was used in the Orient. The new chemistry also contributed nitrous oxide,nitrous oxide,nitrous oxide,nitrous oxide, which, when inhaled, served to suppress the
sensation of pain.
3
9 10The Ether Dome, Boston, Massachussets, USA
Year 1846
11
William TG Morton
Inventor and revealer of anesthetic inhalationBefore whom in all time surgery was agony
By whom pain in surgery was averted and annuled Since whom science has control of pain
H. Bigelow
1846, Boston MassachussettsThe first clinical useof ether as anesthetic
12
Dr. William Morton, a Boston dentist and former partner of Dr. Horace Wells was one of the first to use ether as an
anesthesia. In 1846, just two years after Horace Wells’ anesthetic success with nitrous oxide, Dr. William Morton (1819-68), constructed
the first anesthetic machine. Morton’s simple device was a glass globe housing an ether-
soaked sponge so all the patient had to do was merely to inhale the vapor through one of two outlets.
Morton’s invention was put to the test on October 16, 1846, in the surgical amphitheater of the Massachusetts General Hospital
in Boston when a twenty-year-old man was successfully anesthetized so a tumor could be painlessly removed from what one source said was his neck and another indicated was from his
jaw.

4
13
Anesthesiology is a blessed profession
• When God created Eva from Adam’s rib ………. first, He put Adam into a deep sleep…………….
• The beginning of mankind started with anesthesia
14
Ether :- good narcosis- good analgesia- good muscle relaxation
15
KemajuanIlmu Bedah
Tra
nsfu
si
Ant
ibio
tika
A n
e s
t e
s i
a
N u t r i s i
16
Anesthesia is now much safer and more pleasant for the patient than it was 50 years ago.Factors contributing to the improvements include a fuller understanding of physiology and pharmacology, better preoperative assessment and preparation of patients …… Improvements in anesthesia have allowed surgeons to attempt more complicated operations on increasing number of patients…......
and .…..TODAY
M.Dobson

5
17
Trauma surgery
Endoscopic surgery
18
Many techniques originally developed for use during anesthesiaare now widely recognized as applicable to the care of a variety ofcritically ill patients, for example those with severe head injuries, asthma, tetanus or neonatal asphyxia. Skills such as the rapid assessment and management of unconscious patients, control ofairway, endotrachel intubation,…. cardioplumonary resuscitation have their origins in anesthesia, but are now recognized as essential for all doctors.
19
Working togetherSurgery & Anesthesiology
|extends the boundaries of life and death
Massive Crush Injury - Hb 2 20
6
21
PengembanganIntensive Care / ICU1975 Anestesiologi RSCM1977 Anestesiologi RSDS
22
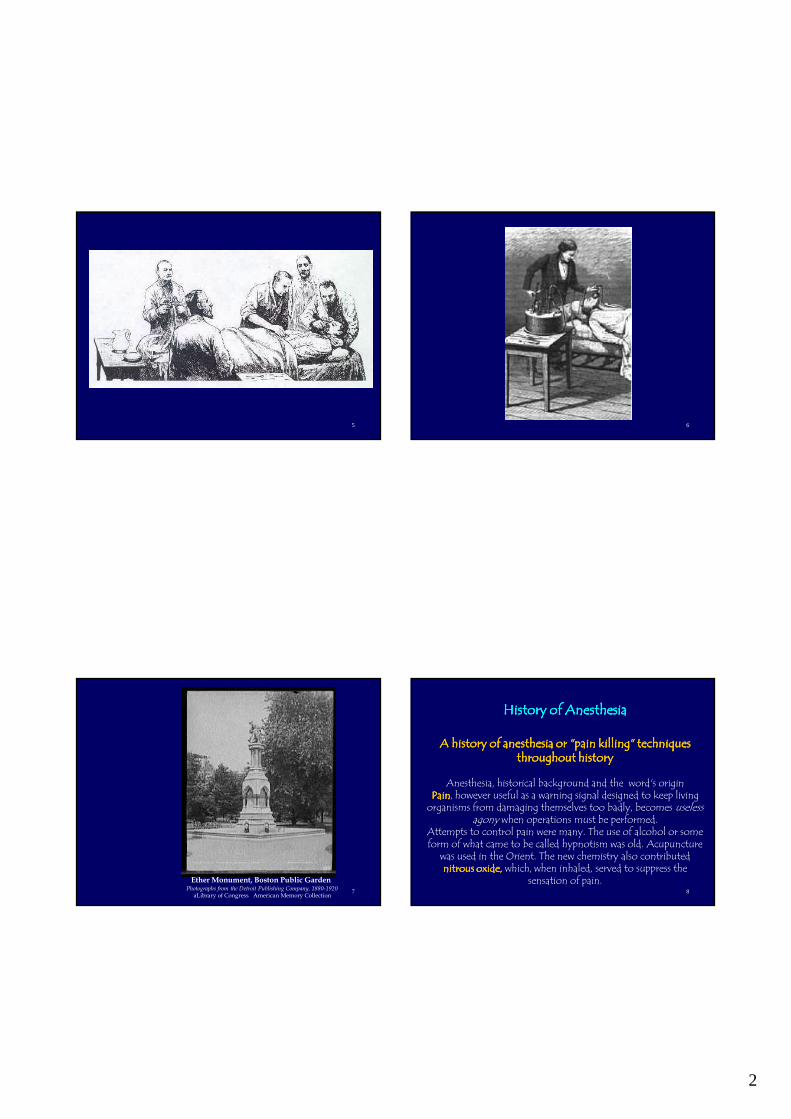
Prolonged Life Supportdi ICU
|adalah bagian dari
Resusitasi
23
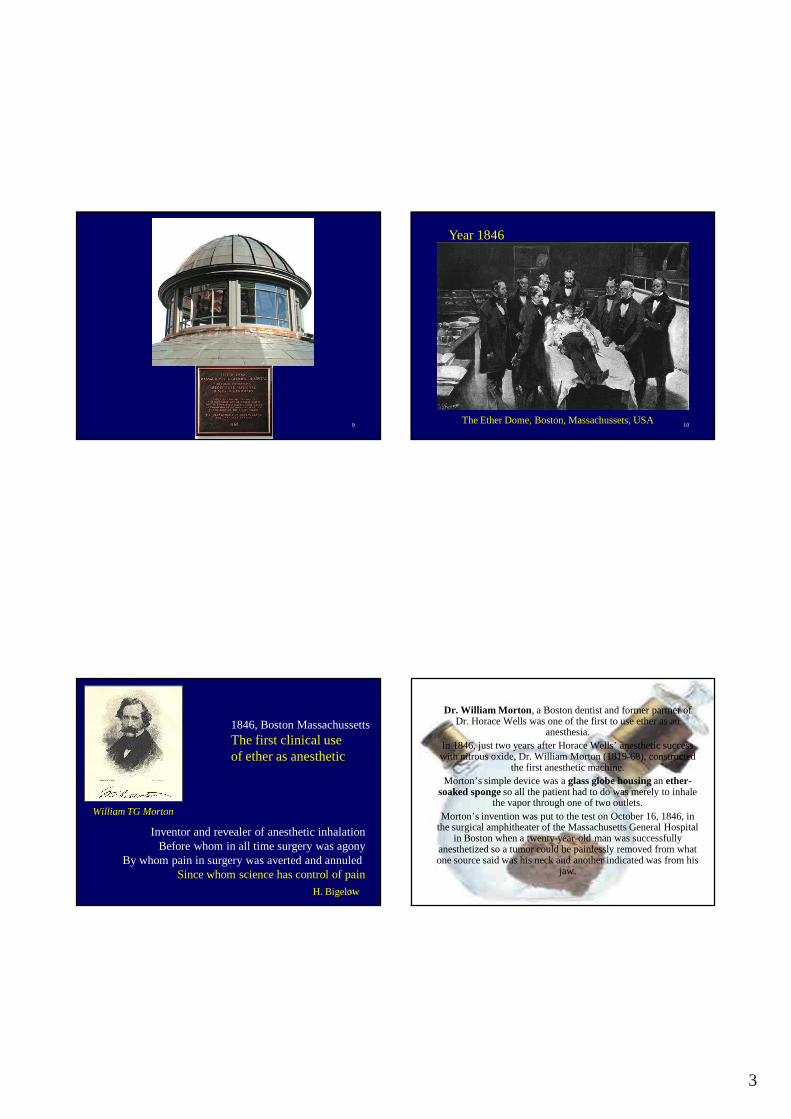
MagillGuedelMacIntoshEpstein
Archie Brain
L M A
24
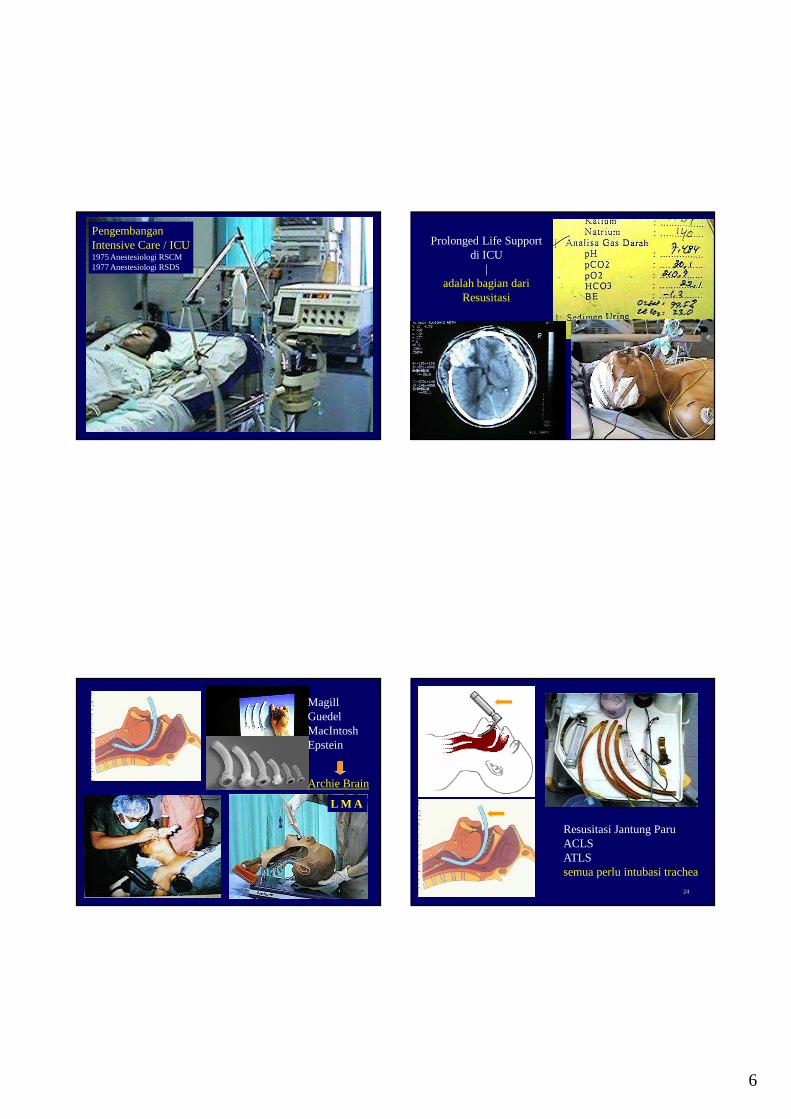
Resusitasi Jantung ParuACLSATLSsemua perlu intubasi trachea

7
25 26
Sekolahnya 4 tahun, 120 SKS + MKDU
27
Anestesia
• Keadaan yang ditandai hilangnya kesadaran dan / atau persepsi nyeri (bersama atau terpisah)
28
Anestesia
• Keadaan yang ditandai hilangnya kesadaran dan / atau persepsi nyeri (bersama atau terpisah)
• Dapat dilakukan secara temporer dengan
– obat anestesia umum
– obat anestesia lokal / regional
– akupunktur
– hipnosis
– stimulasi listrik

8
29
Kapan anestesia diperlukan?
• Menghilangkan nyeri pembedahan & trauma
• Menghilangkan nyeri akut lain:
– proses persalinan
– proses diagnostik medik tertentu
• Menghilangkan nyeri kanker
• Menghilangkan nyeri khronis (ischemia dll)
• Menghilangkan rasa cemas pada anak
30
Apakah anestesia berbahaya?
• Ya– menyebabkan depresi nafas, jantung, sirkulasi,
fungsi otak, hati, usus, ginjal dan sistim imun
• Tidak– jika semua perubahan diawasi dan dikendalikan
maka bahaya dapat di-minimal-kan
• Dengan anestesia yang baik � risiko mati adalah 1: 10,000
31
Throughout America there are thousands of doctors—working in hospitals, clinics and private offices—who hurt and even fatally injure patients through incompetence or carelessness yet remain
in active practice.
In Denver, Richard Corbett Leonard, 8, died during a routine ear operation because the
anesthesiologist allegedly fell asleep.
From an article, “Why Some Doctors May Be Hazardous to Your Health”, by Bernard Gavzer, in the April 14, 1996, issue of Parade Magazine
32

9
33
Mortality associated w/ anesthesia
• Lund & Mushin (1982)-6 days 1:10,000• Forrest (1990)-7 days 1:10,000• Pedersen (1994)-30 days 1: 2,500• MHA (Maryland Hosp Assoc 1999)-
National Aggregate Data
– Class I 1:10,000– Class II 3:10,000– Clas III 28:10,000– Class IV 230:10,000
34
35
Anestesiamenghambat hantaran impulse nyeri atau
menghilangkan persepsi nyeri
• Suntikan im atau iv
• Inhalasi (dihisap nafas)
• Dengan suntikan syaraf
• Dengan suntikan di tempat operasi
• Anestesia umum
• Anestesia regional / conduction block
• Anestesia (infiltrasi) lokal
36
Anestesia umumblok otak = syaraf pusat

10
37
Anestesi umumMorfin pada reseptor
Ketamin pada jalur thalamus-cortex
38
Anestesia regionalblok serat syaraf
39
OA InhalasiKetamine
Spinal block
Plexus & NerveBlock
40
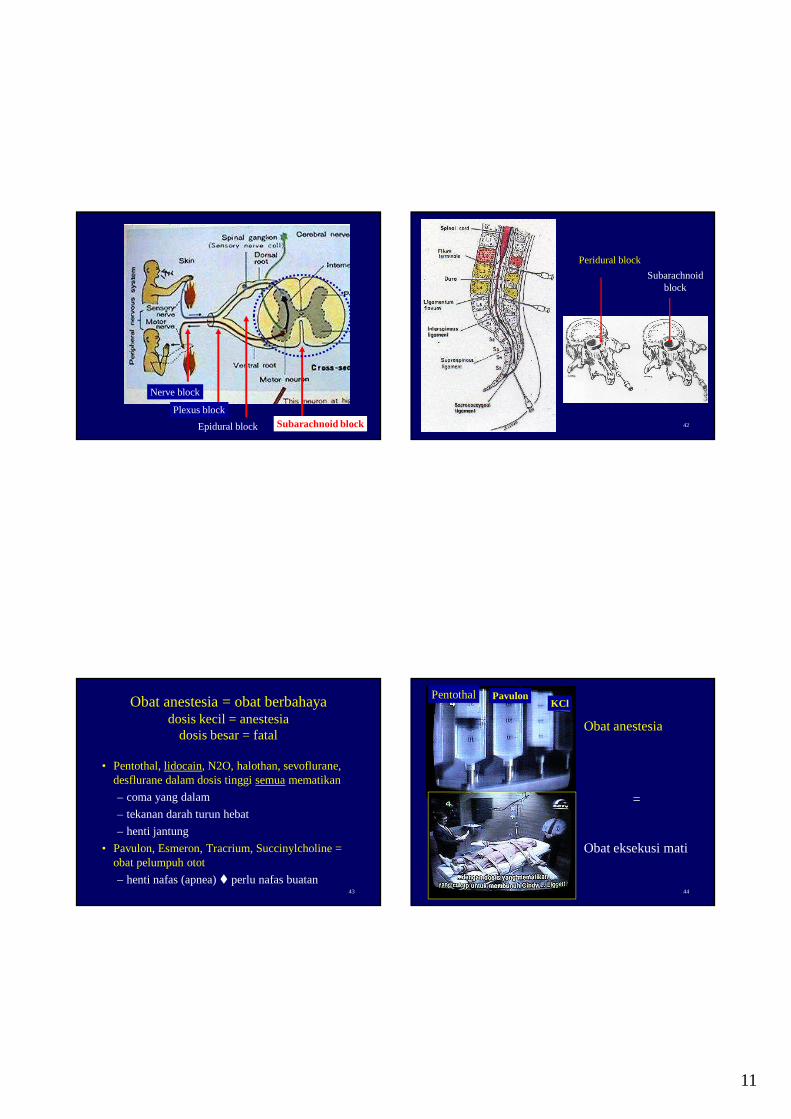
Anestesia regional
• Pada ujung syaraf di lokasi (local infiltration block)
• Pada serabut syaraf (nerve block)
• Pada berkas syaraf dekat medula spinalis (plexus block)
• Pada medula spinalis (peri/epidural block dan subarachnoid block) = spinal anesthesia
11
41
Nerve block
Plexus block
Epidural block Subarachnoid block 42
Peridural block
Subarachnoidblock
43
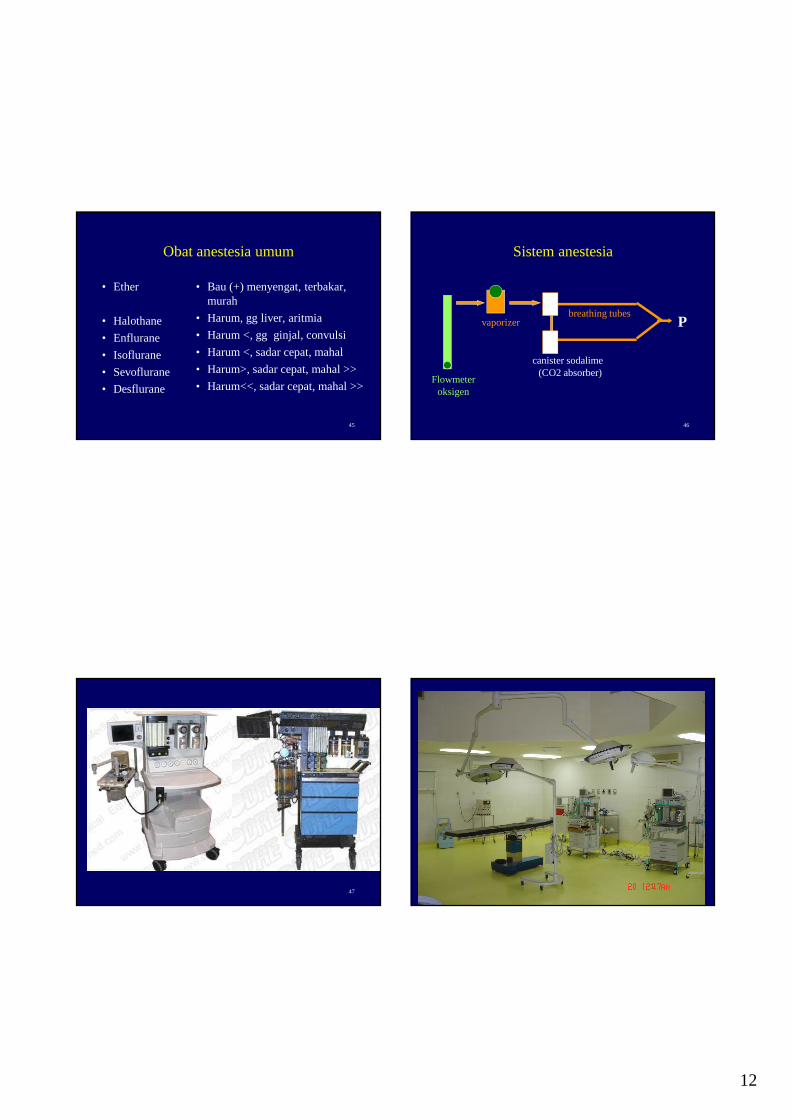
Obat anestesia = obat berbahayadosis kecil = anestesia
dosis besar = fatal
• Pentothal, lidocain, N2O, halothan, sevoflurane, desflurane dalam dosis tinggi semuamematikan
– coma yang dalam
– tekanan darah turun hebat
– henti jantung
• Pavulon, Esmeron, Tracrium, Succinylcholine = obat pelumpuh otot
– henti nafas (apnea) � perlu nafas buatan44
Pentothal PavulonKCl
Obat anestesia
=
Obat eksekusi mati
12
45
Obat anestesia umum
• Ether
• Halothane
• Enflurane
• Isoflurane
• Sevoflurane
• Desflurane
• Bau (+) menyengat, terbakar, murah
• Harum, gg liver, aritmia
• Harum <, gg ginjal, convulsi
• Harum <, sadar cepat, mahal
• Harum>, sadar cepat, mahal >>
• Harum<<, sadar cepat, mahal >>
46
Sistem anestesia
Pvaporizer
Flowmeteroksigen
canister sodalime(CO2 absorber)
breathing tubes
47 48

13
49 50
Sumber gas O2, N2O Vaporizer ether
Vaporizer halothane
Vaporizer enflurane
Flowmeter pengatur gas
51
Uap obat inhalasi
Alveoliparu
Kapiler paru
otak
Art.carotis int..
Obat intravena 52
Mekanisme anestesia umum inhalasi
• TAHAP INDUKSI & MAINTENANCE
• Uap OA kadar tinggi dihisap masuk alveoli paru → kadar OA alveolair tinggi → menembus membran alveoli-kapiler → masuk darah kapiler → kadar OA dalam kapiler tinggi→ sirkulasi oleh jantung kiri ke otak → menembus kapiler di jaringan otak → masuk sel-sel otak → kadar OA dalam sel otak tinggi → pasien menjadi tidak sadar

14
53
Mekanisme anestesia umum inhalasi
• TAHAP RECOVERY
• Bila uap OA dihentikan → kadar alveolair turun → OA dalam darah pindah ke alveolair→ kadar OA dalam darah turun→OA dalam sel otak pindah ke darah→kadar OA dalam otak turun→ pasien sadar kembali
54
Mekanisme anestesia umum parenteral
• TAHAP INDUKSI & MAINTENANCE
• Injeksi obat masuk vena ke jantung kanan lalu ke jantung kiri → sirkulasi oleh jantung kiri ke otak → menembus kapiler di jaringan otak → masuk sel-sel otak →kadar OA dalam sel otak tinggi → pasien menjadi tidak sadar
55
Mekanisme anestesia umum parenteral
• TAHAP RECOVERY
• Bila suntikan OA dihentikan → redistribusi, metabolisme dan ekskresi OA → kadar OA intravena turun → OA dalam sel otak pindah ke darah→ kadar OA dalam otak turun→ pasien sadar kembali
56
Urutan proses anestesia umum
• Puasa: mengosongkan lambung
• Premedikasi: memberi sedatif, analgesia � tenang
• Induksi: memberi loading dose obat anestesia
• Maintenance: memelihara kadar obat anestesia
• Recovery: menunggu siuman kembali
• Post-op care: menunggu normal kembali
15
57
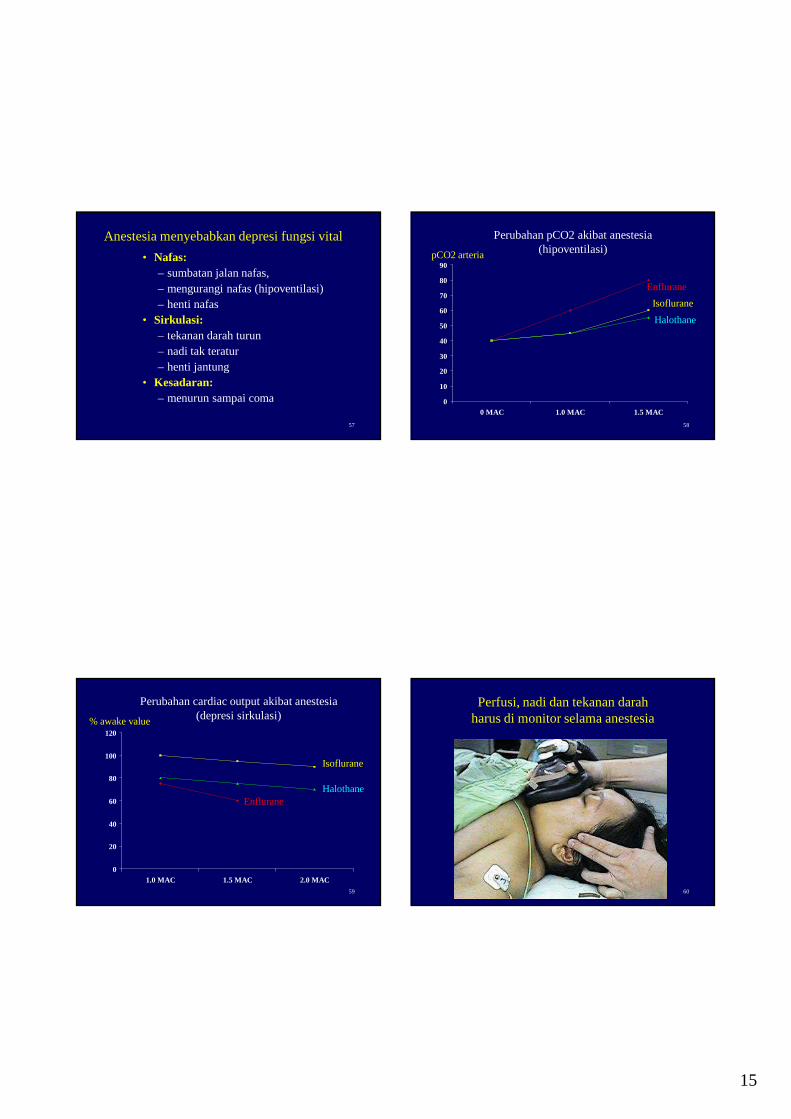
Anestesia menyebabkan depresi fungsi vital
• Nafas:– sumbatan jalan nafas, – mengurangi nafas (hipoventilasi)– henti nafas
• Sirkulasi:– tekanan darah turun– nadi tak teratur– henti jantung
• Kesadaran:– menurun sampai coma
58
0
10
20
30
40
50
60
70
80
90
0 MAC 1.0 MAC 1.5 MAC
Perubahan pCO2 akibat anestesia(hipoventilasi)pCO2 arteria
Enflurane
Isoflurane
Halothane
59
0
20
40
60
80
100
120
1.0 MAC 1.5 MAC 2.0 MAC
Perubahan cardiac output akibat anestesia(depresi sirkulasi)
Isoflurane
EnfluraneHalothane
% awake value
60
Perfusi, nadi dan tekanan darah harus di monitor selama anestesia
16
61
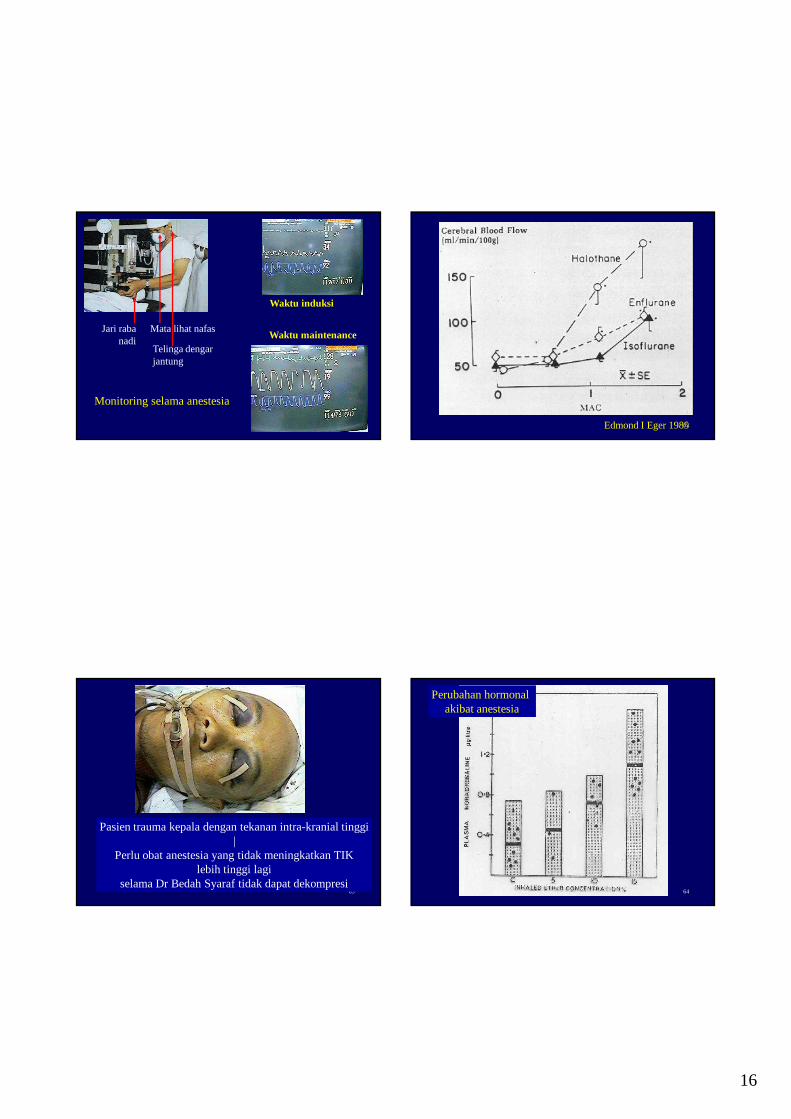
Monitoring selama anestesia
Jari rabanadi
Mata lihat nafas
Telinga dengar jantung
Waktu induksi
Waktu maintenance
62Edmond I Eger 1985
63
Pasien trauma kepala dengan tekanan intra-kranial tinggi|
Perlu obat anestesia yang tidak meningkatkan TIKlebih tinggi lagi
selama Dr Bedah Syaraf tidak dapat dekompresi64
Perubahan hormonal akibat anestesia
17
65
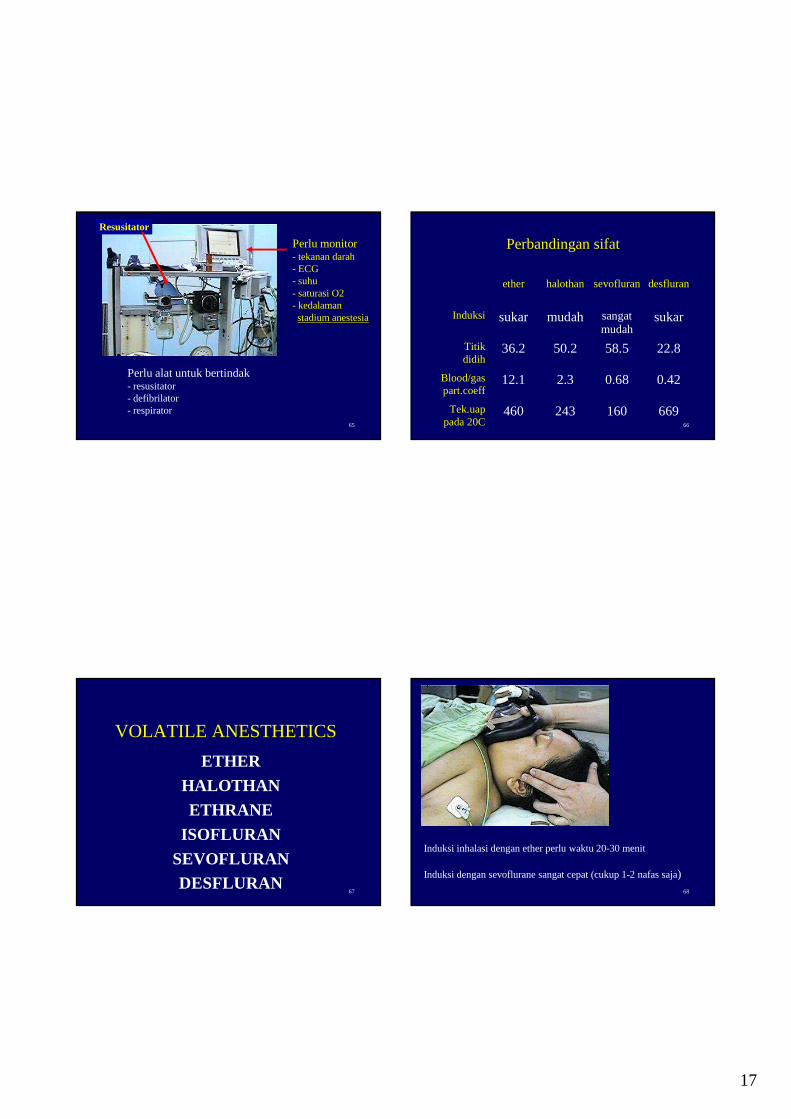
Perlu monitor- tekanan darah- ECG- suhu- saturasi O2- kedalamanstadium anestesia
Resusitator
Perlu alat untuk bertindak- resusitator- defibrilator- respirator
66
Perbandingan sifat
ether halothan sevofluran desfluran
Induksi sukar mudah sangatmudah
sukar
Titikdidih
36.2 50.2 58.5 22.8
Blood/gaspart.coeff
12.1 2.3 0.68 0.42
Tek.uappada 20C
460 243 160 669
67
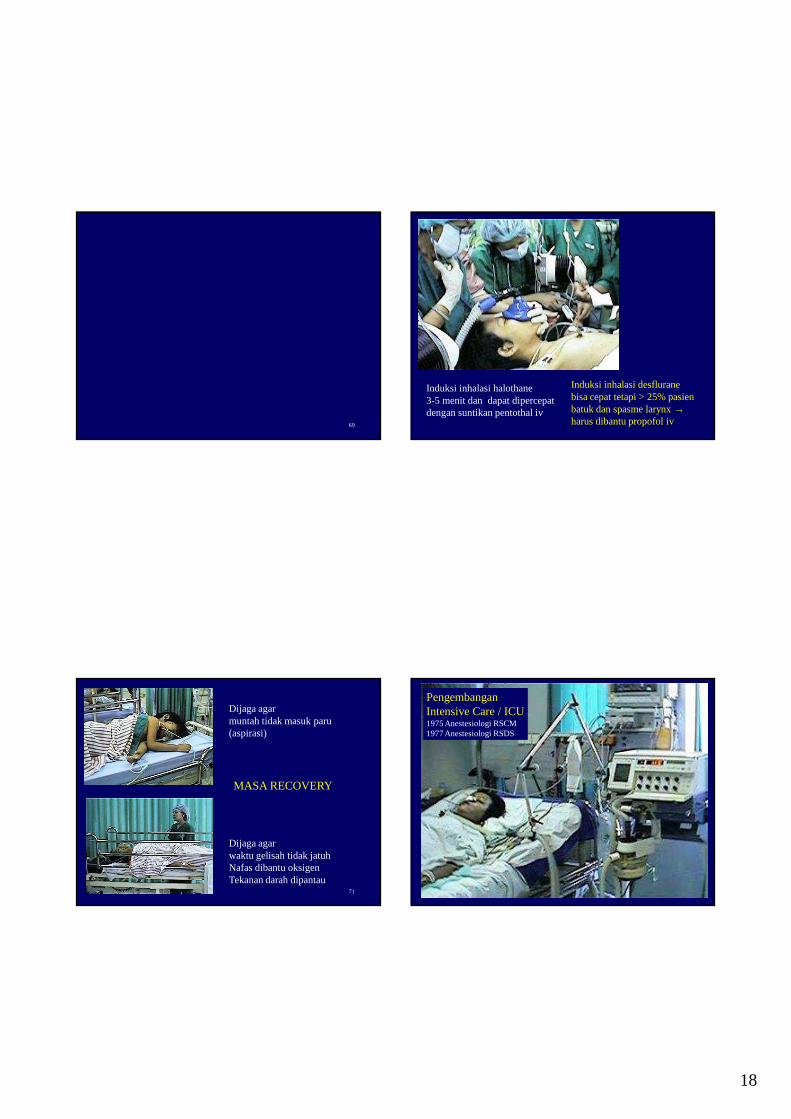
VOLATILE ANESTHETICS
ETHER
HALOTHAN
ETHRANE
ISOFLURAN
SEVOFLURANDESFLURAN
68
Induksi inhalasi dengan ether perlu waktu 20-30 menit
Induksi dengan sevoflurane sangat cepat (cukup 1-2 nafas saja)
18
69 70
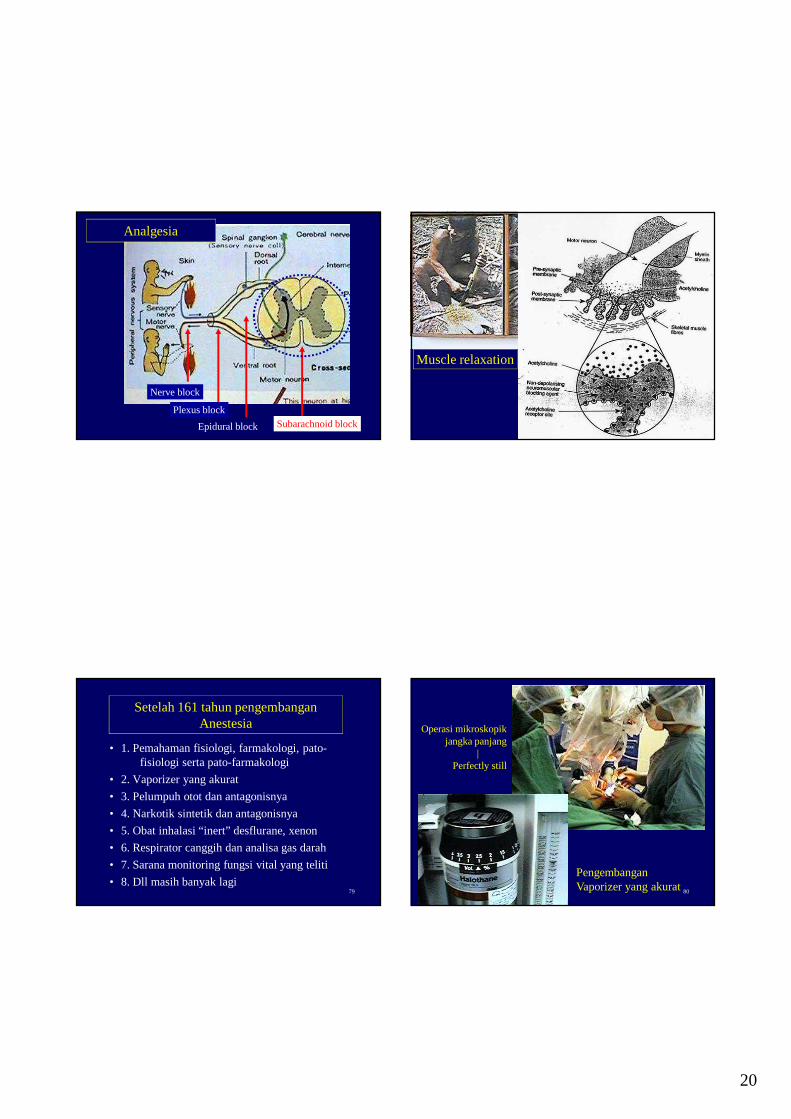
Induksi inhalasi halothane3-5 menit dan dapat dipercepatdengan suntikan pentothal iv
Induksi inhalasi desfluranebisa cepat tetapi > 25% pasienbatuk dan spasme larynx →harus dibantu propofol iv
71
Dijaga agarmuntah tidak masuk paru(aspirasi)
Dijaga agarwaktu gelisah tidak jatuhNafas dibantu oksigenTekanan darah dipantau
MASA RECOVERY
72
PengembanganIntensive Care / ICU1975 Anestesiologi RSCM1977 Anestesiologi RSDS

19
73
Anestesiologi & Reanimasisangat kompleks
|dimana multiple variables bekerja cepat dalam
hitungan menit dan detik
dan dalam range mati-hidupnya seorang pasien
74
Penyulit buruk adalahCARDIAC ARREST- karena penyakitnya sendiri- karena pembedahannya- karena anestesianya
Penyulit terburukadalahMALIGNANT HYPERTHERMIA
obat cuma satu (dantrolene)efeknya belum tentu
Dipicu succinyl - halothan
75
Goodgeneral anesthesia
Nar
cosi
s
Ana
lges
ia
Mus
cle
rela
xatio
n
Stress Free
76
Narcosis dan analgesia
Anestesi umum
Morfin pada reseptor
Ketamin pada jalur thalamus-cortex
20
77
Nerve block
Plexus block
Epidural block Subarachnoid block
Analgesia
78
Muscle relaxation
79
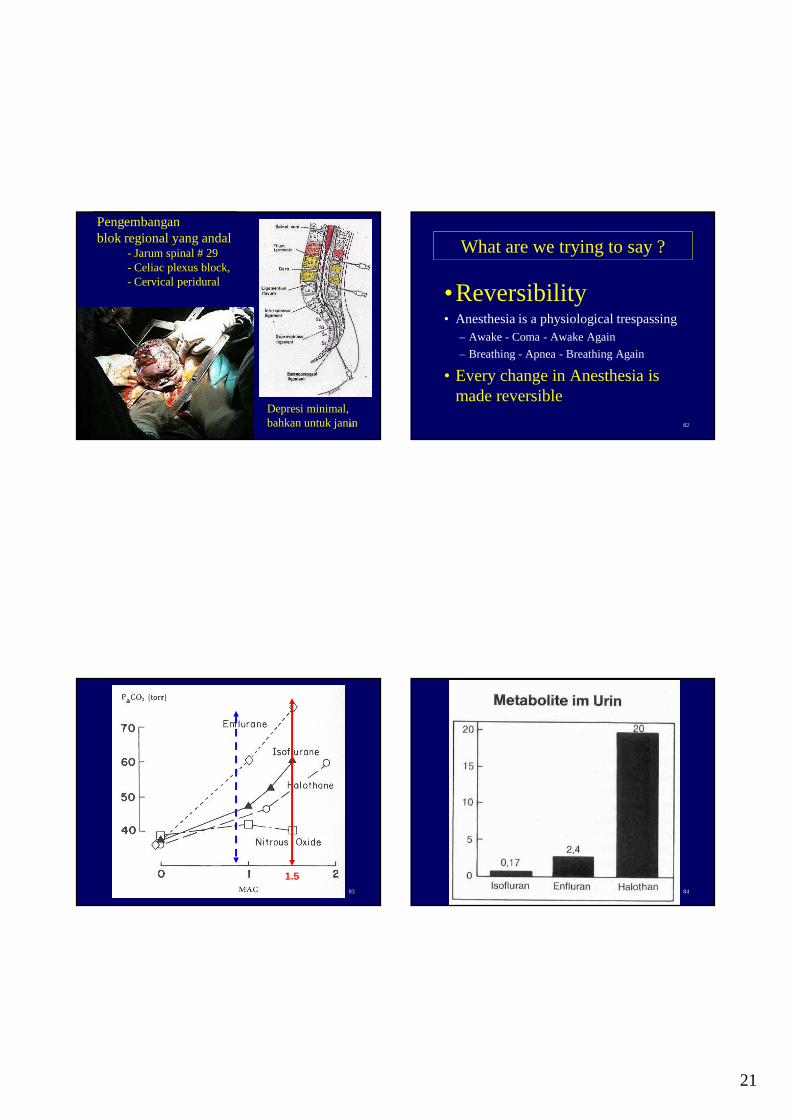
Setelah 161 tahun pengembangan Anestesia
• 1. Pemahaman fisiologi, farmakologi, pato-fisiologi serta pato-farmakologi
• 2. Vaporizer yang akurat
• 3. Pelumpuh otot dan antagonisnya
• 4. Narkotik sintetik dan antagonisnya
• 5. Obat inhalasi “inert” desflurane, xenon
• 6. Respirator canggih dan analisa gas darah
• 7. Sarana monitoring fungsi vital yang teliti
• 8. Dll masih banyak lagi80
PengembanganVaporizer yang akurat
Operasi mikroskopikjangka panjang
| Perfectly still
21
81
Pengembanganblok regional yang andal
- Jarum spinal # 29 - Celiac plexus block, - Cervical peridural
Depresi minimal,bahkan untuk janin 82
What are we trying to say ?
•Reversibility• Anesthesia is a physiological trespassing
– Awake - Coma - Awake Again
– Breathing - Apnea - Breathing Again
• Every change in Anesthesia is made reversible
83
1.584
22
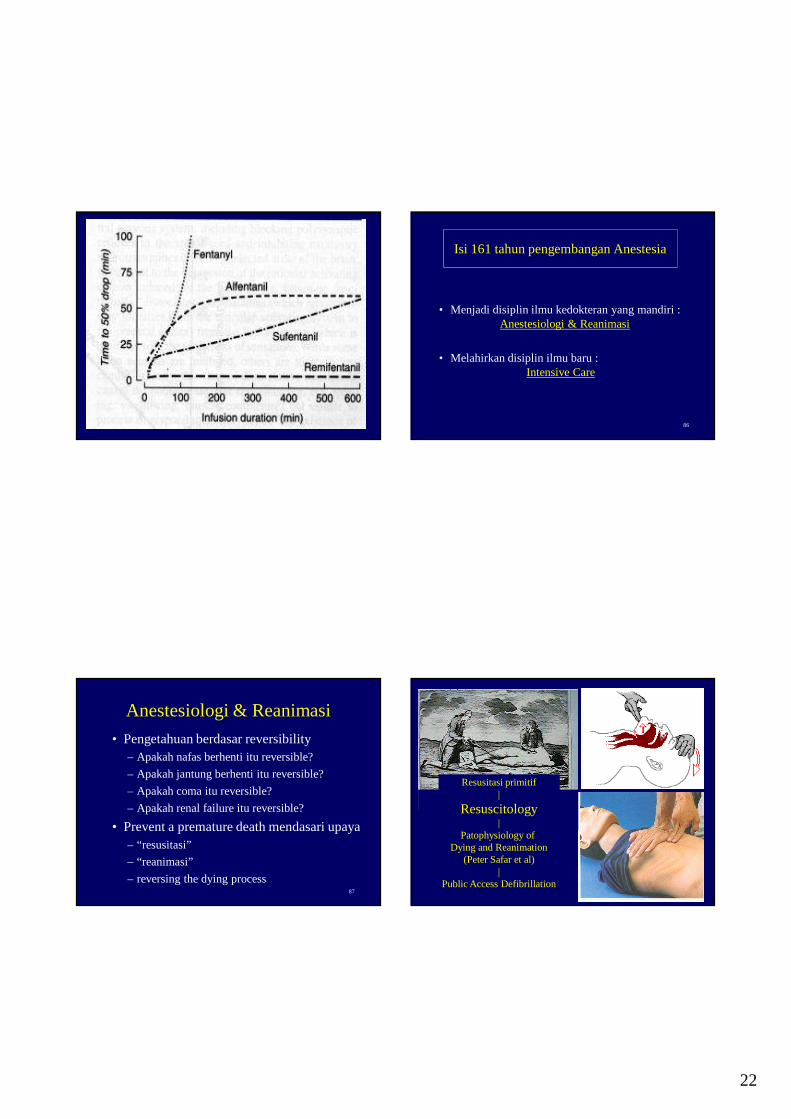
85 86
Isi 161 tahun pengembangan Anestesia
• Menjadi disiplin ilmu kedokteran yang mandiri : Anestesiologi & Reanimasi
• Melahirkan disiplin ilmu baru : Intensive Care
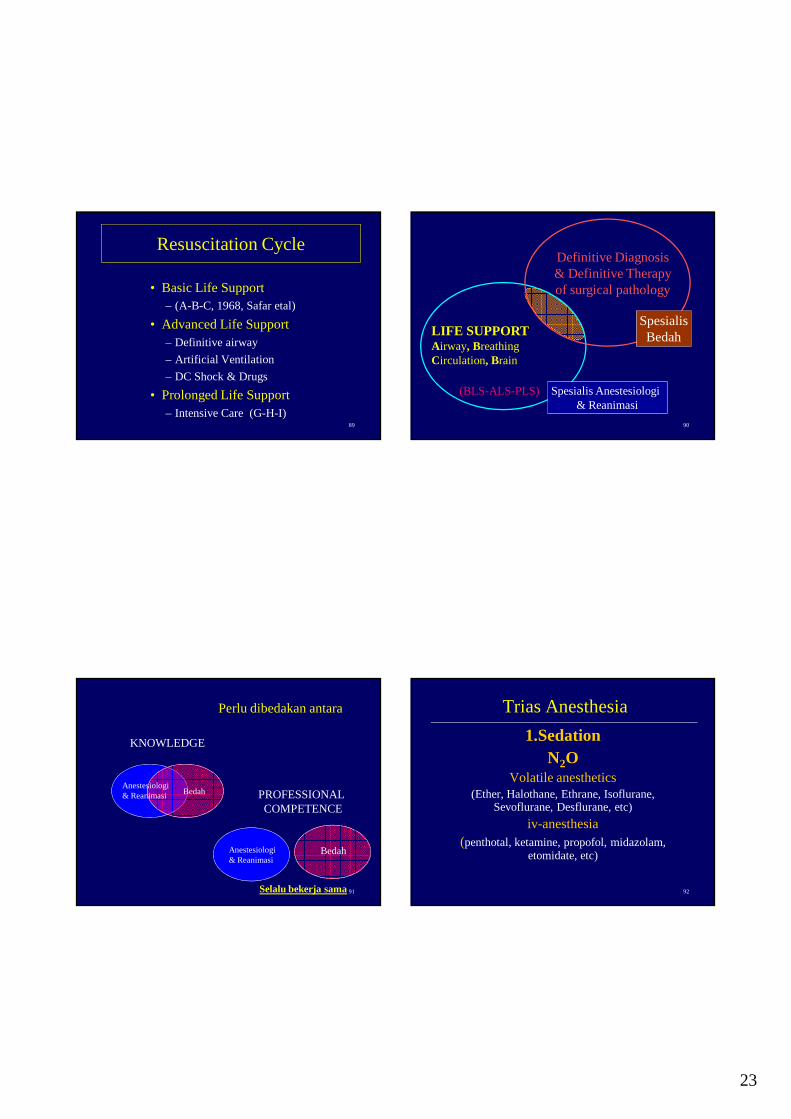
87
Anestesiologi & Reanimasi
• Pengetahuan berdasar reversibility– Apakah nafas berhenti itu reversible?
– Apakah jantung berhenti itu reversible?
– Apakah coma itu reversible?
– Apakah renal failure itu reversible?
• Prevent a premature death mendasari upaya – “resusitasi”
– “reanimasi”
– reversing the dying process88
Resusitasi primitif|
Resuscitology|
Patophysiology of Dying and Reanimation
(Peter Safar et al)|
Public Access Defibrillation
23
89
Resuscitation Cycle
• Basic Life Support– (A-B-C, 1968, Safar etal)
• Advanced Life Support– Definitive airway
– Artificial Ventilation
– DC Shock & Drugs
• Prolonged Life Support– Intensive Care (G-H-I)
90
LIFE SUPPORTAirway, BreathingCirculation, Brain
(BLS-ALS-PLS)
Definitive Diagnosis& Definitive Therapyof surgical pathology
SpesialisBedah
Spesialis Anestesiologi & Reanimasi
91
Perlu dibedakan antara
Anestesiologi& Reanimasi Bedah
BedahAnestesiologi& Reanimasi
KNOWLEDGE
PROFESSIONAL COMPETENCE
Selalu bekerja sama 92
Trias Anesthesia
1.SedationN2O
Volatile anesthetics(Ether, Halothane, Ethrane, Isoflurane,
Sevoflurane, Desflurane, etc)
iv-anesthesia(penthotal, ketamine, propofol, midazolam,
etomidate, etc)
24
93
Trias Anesthesia
2. Analgesia,Narcotic-analgetic
(morphin, petidin, fentanyl, sufentanyl, alfentanyl, etc),
N2O
94
Trias Anesthesia
3. Relaxation,Muscle relaxan
( succinylcholine, pancuronium bromide, atracurium, vecuronium
rocuronium, etc)
95
ROUTINE PREOPERATIVE LABORATORY EVALUATION OFROUTINE PREOPERATIVE LABORATORY EVALUATION OFASYMPTOMATIC, APPARENTLY HEALTHY PATIENTSASYMPTOMATIC, APPARENTLY HEALTHY PATIENTS
Hematocrit of hemoglobin concentrationAll menstruating womenAll patients over 60 years of ageAll patients who are likely to experience
significant blood loss and may require transfusion
�Serum glucose and creatinine ( or blood urea nitrogen )concentration : All patients over 60 years of age
�Electrocardiogram : all patients over 40 years of age�Chest radiograph : all patients over 60 years of age
96
THE ANESTHETIC PLANTHE ANESTHETIC PLAN
PremedicationType of anesthesia
GeneralAirway managementInductionMaintenanceMuscle relaxation
Local or regional anesthesiaTechniqueAgents
Monitored anesthesia careSupplement oxygenSedation
Intraoperative managementMonitoringPositioningFluid managementSpecial techniques
Postoperative managementPain controlIntensive care
Postoperative ventilationHemodynamic monitoring
25
97
PREOPERATIVE PHYSICAL STATUS CLASSIFICATION ofPATIENTS ACCORDING TO THE AMERICAN SOCIETY OF ANESTHESIOLOGIST
98
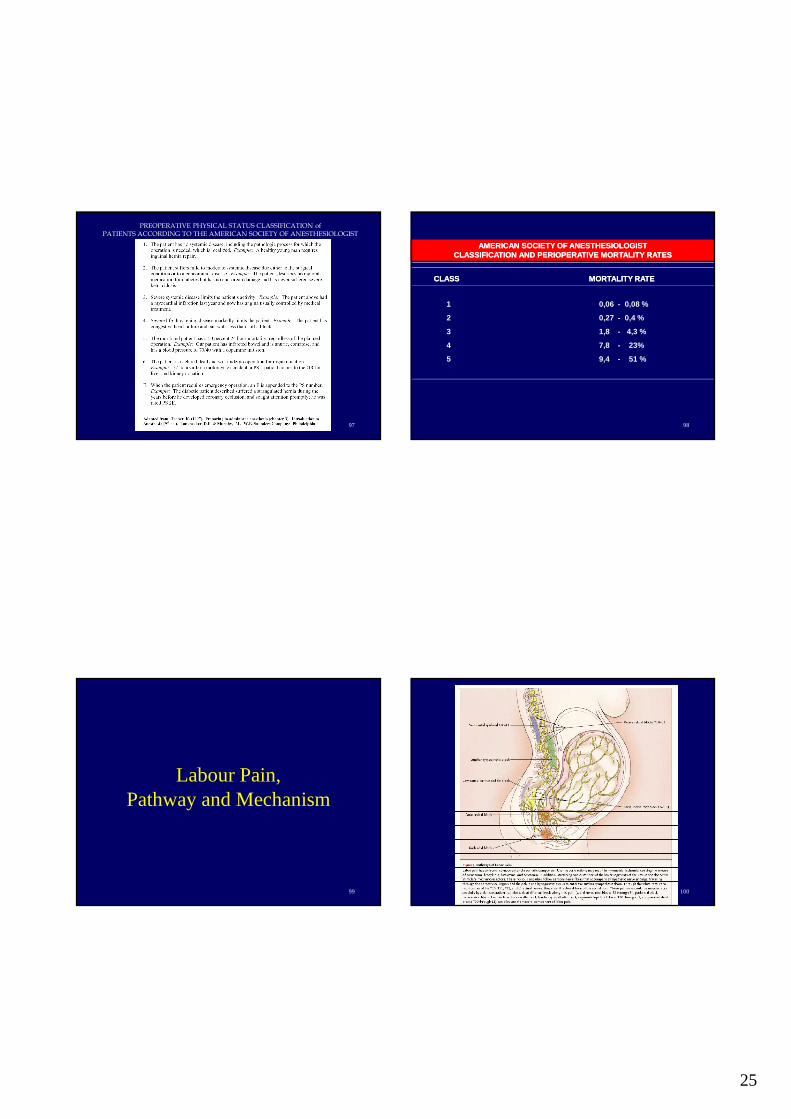
AMERICAN SOCIETY OF ANESTHESIOLOGISTAMERICAN SOCIETY OF ANESTHESIOLOGISTCLASSIFICATION AND PERIOPERATIVE MORTALITY RATESCLASSIFICATION AND PERIOPERATIVE MORTALITY RATES
CLASSCLASS MORTALITY RATEMORTALITY RATE
1 0,06 - 0,08 %
2 0,27 - 0,4 %
3 1,8 - 4,3 %
4 7,8 - 23%
5 9,4 - 51 %
99
Labour Pain,Pathway and Mechanism
100
26
101 102
103
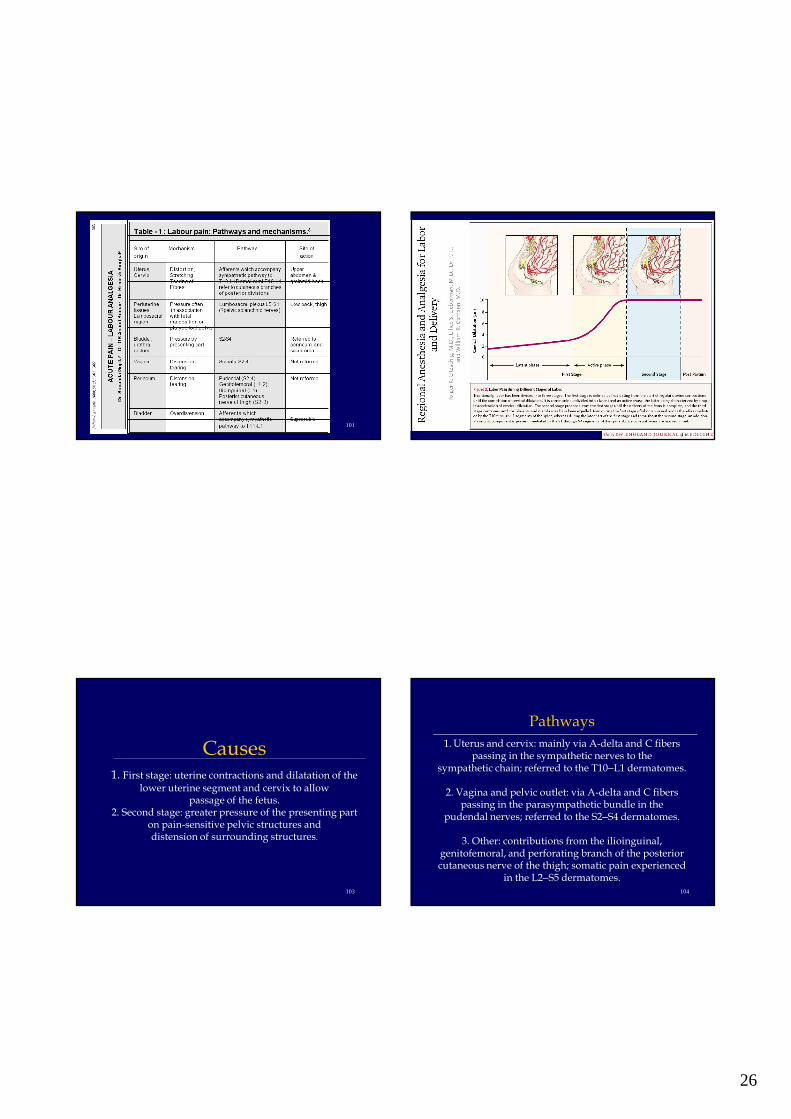
Causes1. First stage: uterine contractions and dilatation of the
lower uterine segment and cervix to allowpassage of the fetus.
2. Second stage: greater pressure of the presenting part on pain-sensitive pelvic structures anddistension of surrounding structures.
104
Pathways
1. Uterus and cervix: mainly via A-delta and C fibers passing in the sympathetic nerves to the
sympathetic chain; referred to the T10–L1 dermatomes.
2. Vagina and pelvic outlet: via A-delta and C fibers passing in the parasympathetic bundle in the
pudendal nerves; referred to the S2–S4 dermatomes.
3. Other: contributions from the ilioinguinal, genitofemoral, and perforating branch of the posteriorcutaneous nerve of the thigh; somatic pain experienced
in the L2–S5 dermatomes.

27
105
Features.1Over 90% of women experience severe/unbearable labor
pain, although recollection fades with time
2. Typically, pain is similar to other types of visceral pain, i.e., intermittent, severe, and colicky; it starts in the lower
abdomen and back, spreading to the perineum and thighs (Lowe 2000).
3. Pain may be influenced by the factors already listed above, in particular by social, societal, and cultural aspects.
Certain cultures are more emotive and expressive than other, more stoic ones, leading possibly to differences in pain behavior rather than in the extent of pain felt. Fatigue and
general debility, common in late pregnancy, may also contribute to the experience of labor pain. 106
Consequences of labor pain
A. Understand that labor pain may have adverse physiological and psychological consequences:
1. Respiratory: causes hyperventilation, leading to hypocapnia and respiratory aLKALOSIS.
2. Cardiovascular: increases cardiac output and blood pressure via sympathetic activity; this may be
problematic in cardiac disease and pre-eclampsia. Increased venous return associated with uterinecontractions may also contribute.
3. Neuroendocrine: increases maternal catecholamine secretion with risk of uteroplacental
constriction.
107
4. Gastrointestinal: effect of labor on gastric emptying and acidity is unclear, although delayed emptying and
increased acid secretion have been suggested. Opioids are well known to induce gastric stasis
5. Psychological: severe labor pain has been implicated in contributing to long-term emotional stress, with
potential adverse consequenceson maternal mental health and family relationships.
108
B. Understand also that pain during labor may have benefits:
1. Indicates to the mother and those assisting labor/delivery that contractions are occurring.2. May have positive connotations regarding
childbirth, related to societal/cultural influences.3. May indicate problems (e.g. uterine rupture,
placental abruption).

28
109 110
111 112

29
113 114
115 116

30
117 118
119 120

31
121 122
123 124
Thank you for listening