kawasaki disease - link.springer.com · kawasaki disease ho-chang kuoa* and kai-sheng hsiehb...
TRANSCRIPT

Kawasaki Disease
Ho-Chang Kuoa* and Kai-Sheng HsiehbaKawasaki Disease Center and Department of Pediatrics, Division of Allergy, Immunology and Rheumatology, KaohsiungChang Gung Memorial Hospital, Chang Gung University College of Medicine, Kaohsiung city, TaiwanbDepartment of Pediatrics, Kaohsiung Chang Gung Memorial Hospital, Chang Gung University College of Medicine,Kaohsiung city, Taiwan
Synonyms
Kawasaki disease; Kawasaki syndrome; Lymph node syndrome; Mucocutaneous lymph node syndrome
Definition
Prolonged fever (>5 days), with four of the following five phenotypes: conjunctivitis, diffuse oralmucosal inflammation, polymorphous skin rashes, indurative edema of the hands and feet associatedwith the peeling of finger tips, and non-suppurative neck lymphadenopathy.
Epidemiology and Genetics
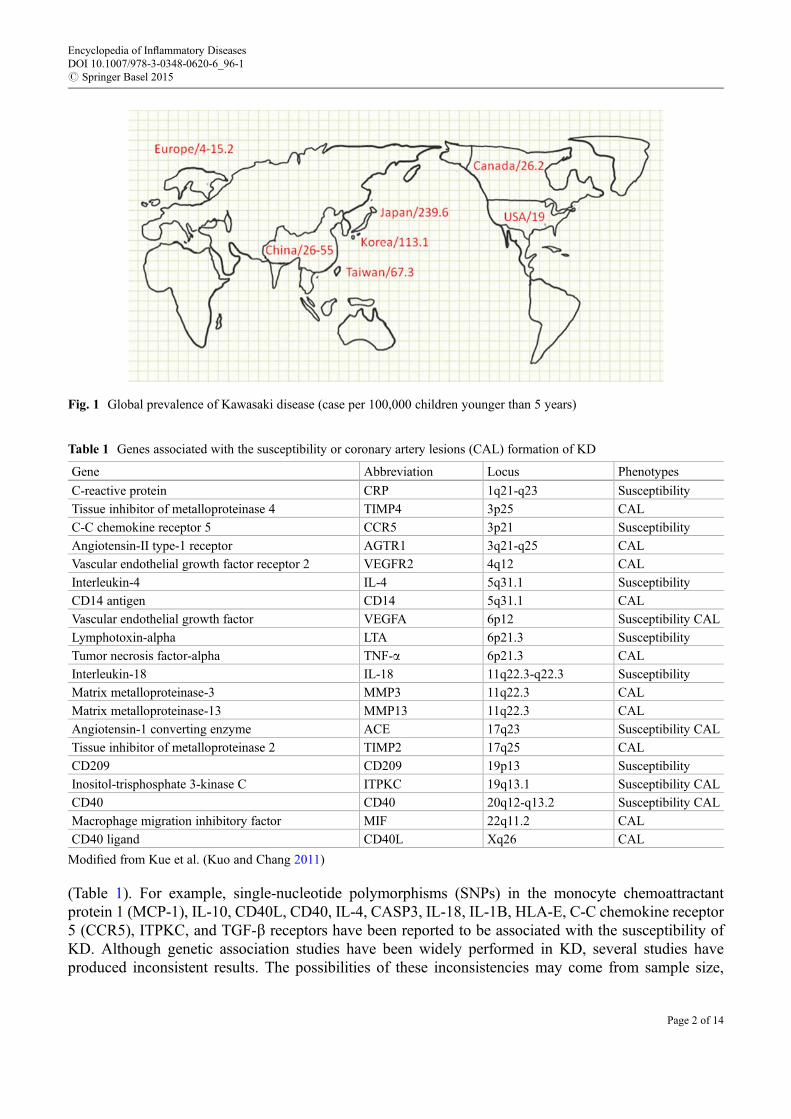
The incidence of KD is increasing globally, especially in Japan (Fig. 1). In Taiwan, Korea, and Japan, theincidence ranges from 67.3, 113, to 239.36 cases per 100,000 children under 5 years of age, respectively(Nakamura et al. 2012). The highest incidence is in Japan, and the lowest is in the United Kingdom (8.39per 100,000 children under 5 years of age, almost 1/30 of the incidence in Japan). The annual incidencerates increase in Japan but not in Taiwan. Epidemiologic surveys of KD found that 1.5 % of all cases wererecurrent (had second episode of KD after first episode) (Huang et al. 2009). In Taiwan, KD occurs mostfrequently in the summer (April to June) and least frequently in winter; for unknown reasons, its seasonaloccurrence varies in other countries. In Japan, monthly number of patients peaked during winter to springmonths; lower peaks were noted during summer months. The environmental factor’s trigger for KD couldbe wind-borne in Japan, Hawaii, and San Diego. The association of KD and vaccination is still unclear.A review of RotaTeq (rotavirus vaccine live) clinical trial data revealed higher but not statisticallysignificant in KD rates among RotaTeq vaccines than placebo recipients. But the Vaccine AdverseEvent Reporting System (VAERS) for all US-licensed vaccines reported that not suggest an elevatedKD risk for RotaTeq or other vaccines. In conclusion, the incidence was increased globally, especially inJapan, and environmental factors may play a role in the epidemiology of KD but not vaccination.
Genetic StudyThe incidence of KD in Asian countries is higher than American and Europe, male predominant, nocertain infectious source found suggests that genetic predisposition might play an important role in thesusceptibility to this disease. There is also evidence that the incidence of KD is higher among siblings thanin the general population (about ten times higher). A number of reports provided evidence that geneticpolymorphisms contribute to the susceptibility to KD and/or coronary artery lesions (CAL) formation
*Email: [email protected]
Encyclopedia of Inflammatory DiseasesDOI 10.1007/978-3-0348-0620-6_96-1# Springer Basel 2015
Page 1 of 14
(Table 1). For example, single-nucleotide polymorphisms (SNPs) in the monocyte chemoattractantprotein 1 (MCP-1), IL-10, CD40L, CD40, IL-4, CASP3, IL-18, IL-1B, HLA-E, C-C chemokine receptor5 (CCR5), ITPKC, and TGF-b receptors have been reported to be associated with the susceptibility ofKD. Although genetic association studies have been widely performed in KD, several studies haveproduced inconsistent results. The possibilities of these inconsistencies may come from sample size,
Fig. 1 Global prevalence of Kawasaki disease (case per 100,000 children younger than 5 years)
Table 1 Genes associated with the susceptibility or coronary artery lesions (CAL) formation of KD
Gene Abbreviation Locus Phenotypes
C-reactive protein CRP 1q21-q23 Susceptibility
Tissue inhibitor of metalloproteinase 4 TIMP4 3p25 CAL
C-C chemokine receptor 5 CCR5 3p21 Susceptibility
Angiotensin-II type-1 receptor AGTR1 3q21-q25 CAL
Vascular endothelial growth factor receptor 2 VEGFR2 4q12 CAL
Interleukin-4 IL-4 5q31.1 Susceptibility
CD14 antigen CD14 5q31.1 CAL
Vascular endothelial growth factor VEGFA 6p12 Susceptibility CAL
Lymphotoxin-alpha LTA 6p21.3 Susceptibility
Tumor necrosis factor-alpha TNF-a 6p21.3 CAL
Interleukin-18 IL-18 11q22.3-q22.3 Susceptibility
Matrix metalloproteinase-3 MMP3 11q22.3 CAL
Matrix metalloproteinase-13 MMP13 11q22.3 CAL
Angiotensin-1 converting enzyme ACE 17q23 Susceptibility CAL
Tissue inhibitor of metalloproteinase 2 TIMP2 17q25 CAL
CD209 CD209 19p13 Susceptibility
Inositol-trisphosphate 3-kinase C ITPKC 19q13.1 Susceptibility CAL
CD40 CD40 20q12-q13.2 Susceptibility CAL
Macrophage migration inhibitory factor MIF 22q11.2 CAL
CD40 ligand CD40L Xq26 CAL
Modified from Kue et al. (Kuo and Chang 2011)
Encyclopedia of Inflammatory DiseasesDOI 10.1007/978-3-0348-0620-6_96-1# Springer Basel 2015
Page 2 of 14

different genetic backgrounds within populations, environmental factors, and/or infectious agentsbetween countries.
Since 2009, first genome-wide association study (GWAS) on 119 Caucasian KD cases and 135matchedcontrols was reported. This insightful work identified SNP within the N-acetylated alpha-linked acidicdipeptidase-like two gene (NAALADL2), which was significantly associated with the susceptibility ofKD. Although the function of NAALADL2 remains unclear, mutations in the gene may be involved in thedevelopment of Cornelia de Lange syndrome. In 2010, GWAS of Korean which reported a locus in the1p31 region was identified as a susceptibility locus for KD, and PELI1 gene locus in the 2p13.3 regionwas confirmed to associate with CAL. Three novel loci was found including COPB2 (coatomer proteincomplex beta-2 subunit), ERAP1 (endoplasmic reticulum amino peptidase 1), and immunoglobulinheavy chain variable region genes in Han Chinese population residing in Taiwan (Tsai et al. 2011). In2011, 5 independent sample collections from the USA, Asia, and Europe reported GWAS from 2,173individuals with KD and 9,383 controls and showed a functional polymorphism in the IgG receptor geneFCGR2A (encoding an H131R substitution) with the A allele (coding for histidine) conferring elevateddisease risk for KD (Khor et al. 2011). In 2012, two independent research groups published GWAS datafrom Taiwanese and Japanese populations (Lee et al. 2012; Onouchi et al. 2012) and suggested that BLK(encoding B-lymphoid tyrosine kinase) and CD40 are novel susceptibility genes for KD. This is the firsttime the same genetic results were found from a different area using GWAS. GWAS is very useful toidentify novel loci for KD, global study cooperation to diminish bias from sample size and environmentfactors, meta-analysis and functional studies are needed to confirm these meaningful findings.
Pathophysiology
Kawasaki disease (KD), an acute systemic vasculitis, occurs mainly in infants and children under 5 yearsof age and was first described by Dr. Tomisaku Kawasaki et al. (Fig. 2) in 1967 in Japanese and later in1974 in English. Currently, it is the leading cause of acquired heart disease in children in orientalcountries; however, its etiology remains unknown (Kuo et al. 2012). The etiology of KD remainsunknown and may be attributed to the combined effects of infection, immune response, and geneticsusceptibility. Standard treatment with high-dose aspirin (80–100 mg/kg/day, acetylsalicylic acid; ASA)and high-dose intravenous immune globulin (2 g/kg, IVIG, or intravenous gammaglobulin, IVGG) has
Fig. 2 Dr. Tomisaku Kawasaki (left) and Dr. Ho-Chang Kuo (right) at 2008 International Kawasaki Disease Symposium,Taipei, Taiwan
Encyclopedia of Inflammatory DiseasesDOI 10.1007/978-3-0348-0620-6_96-1# Springer Basel 2015
Page 3 of 14

been shown to decrease the rate of coronary artery aneurysm development from 25–25 % to 3–5 %. Inchildren with acute KD, a single large dose of IVIG is more effective than the conventional regimen offour smaller daily doses (Burns and Glode 2004).
In the acute stage of KD, activation of numerous immunologic factors including T cell activation,cytokine production (IL-1, IL-4, IL-5, IL-6, IL-8, IL-10, IL-13, IL-17, GM-CSF, TNF-a, IFN-g, TGF-b,MIP-1, MCP-1, CCL17, MMP-9, CD40L, etc.) (Burns and Glode 2004; Hsieh et al. 2011; Kuoet al. 2011, 2012; Lin et al. 2012), nitric oxide (NO) production, autoantibody production, and enhancedadhesion molecule expression is well documented. Pathologic examination of the coronary arteritis in theacute stage of KD indicates that activated T lymphocyte-dependent processes characterized by transmuralinfiltration of activated T lymphocytes occur with accumulation of CD8+ T cells in vascular lesions.Macrophage activation and altered T helper (Th1/Th2) and regulatory cell functions are also implicated indysregulation of the immune response in patients with KD (Wang et al. 2005).
Clinical Presentation
As shown in Figs. 3, 4, 5, 6, 7, and 8, the clinical characteristics of KD patients include fever lasting>5 days, diffuse mucosal inflammation, bilateral nonpurulent conjunctivitis, dysmorphic skin rashes,indurative angioedema over the hands and feet, and cervical lymphadenopathy. KD should be consideredin the differential diagnosis of any young child with unexplained fever more than 5 days. Changes in theextremities are prominent with redness and edematous change. Erythema of the palms and soles occur
Fig. 3 Face of children with Kawasaki disease showed redness over the perioral area, fissure lip, and strawberry tongue
Fig. 4 Bilateral nonpurulent conjunctivitis
Encyclopedia of Inflammatory DiseasesDOI 10.1007/978-3-0348-0620-6_96-1# Springer Basel 2015
Page 4 of 14

along with firm, sometimes painful induration of the hands or feet in the early phase of KD.A polymorphous exanthema usually appears within 5 days of the onset of fever. The rash may presentvarious forms on the trunk and extremities, including an urticarial exanthema, a maculopapularmorbilliform eruption, a scarlatiniform erythroderma, an erythema multiforme-like rash, and a finemicropustular eruption. Any kind of skin rash should be considered KD-related when suspected.Neck lymph node enlargement, usually >1.5 cm in diameter, also occurs in the early phase. Bilateralconjunctival injection usually begins shortly after the onset of fever. It typically involves the bulbarconjunctivae much more than the palpebral or tarsal conjunctivae and is not associated with an exudate.
Fig. 5 Dysmorphism skin rash
Fig. 6 BCG injection site induration
Fig. 7 Palm erythematic change
Encyclopedia of Inflammatory DiseasesDOI 10.1007/978-3-0348-0620-6_96-1# Springer Basel 2015
Page 5 of 14
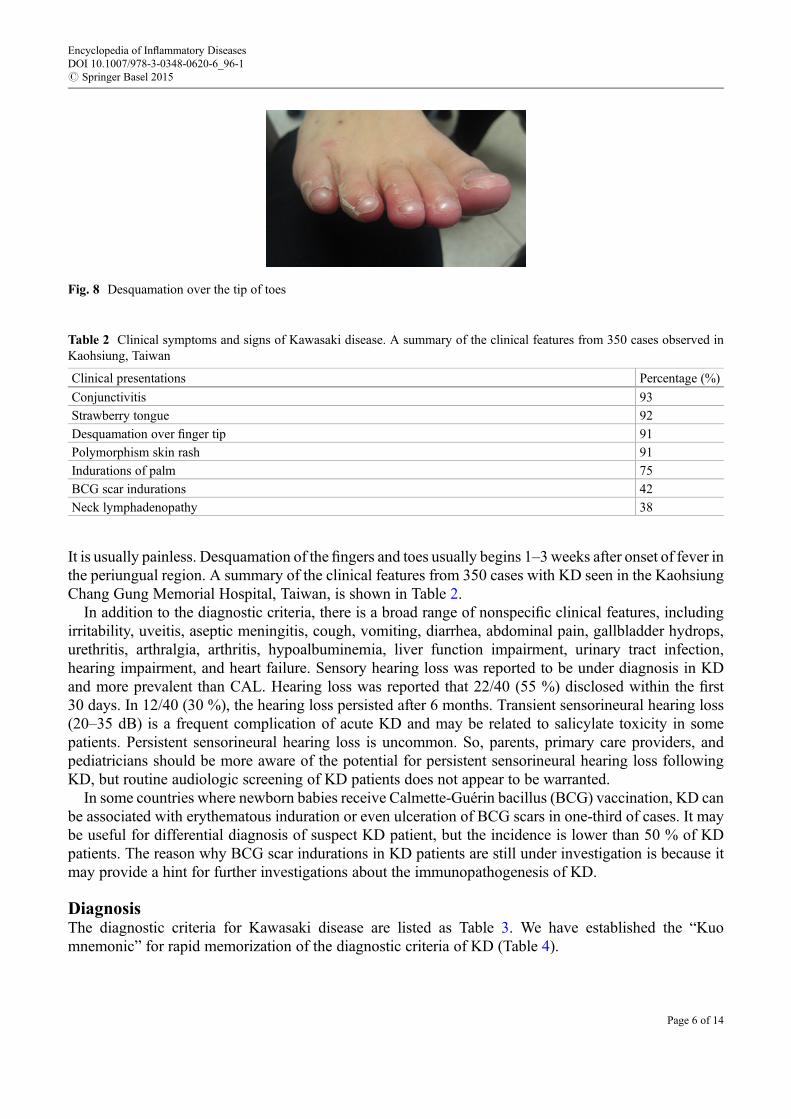
It is usually painless. Desquamation of the fingers and toes usually begins 1–3weeks after onset of fever inthe periungual region. A summary of the clinical features from 350 cases with KD seen in the KaohsiungChang Gung Memorial Hospital, Taiwan, is shown in Table 2.
In addition to the diagnostic criteria, there is a broad range of nonspecific clinical features, includingirritability, uveitis, aseptic meningitis, cough, vomiting, diarrhea, abdominal pain, gallbladder hydrops,urethritis, arthralgia, arthritis, hypoalbuminemia, liver function impairment, urinary tract infection,hearing impairment, and heart failure. Sensory hearing loss was reported to be under diagnosis in KDand more prevalent than CAL. Hearing loss was reported that 22/40 (55 %) disclosed within the first30 days. In 12/40 (30 %), the hearing loss persisted after 6 months. Transient sensorineural hearing loss(20–35 dB) is a frequent complication of acute KD and may be related to salicylate toxicity in somepatients. Persistent sensorineural hearing loss is uncommon. So, parents, primary care providers, andpediatricians should be more aware of the potential for persistent sensorineural hearing loss followingKD, but routine audiologic screening of KD patients does not appear to be warranted.
In some countries where newborn babies receive Calmette-Guérin bacillus (BCG) vaccination, KD canbe associated with erythematous induration or even ulceration of BCG scars in one-third of cases. It maybe useful for differential diagnosis of suspect KD patient, but the incidence is lower than 50 % of KDpatients. The reason why BCG scar indurations in KD patients are still under investigation is because itmay provide a hint for further investigations about the immunopathogenesis of KD.
DiagnosisThe diagnostic criteria for Kawasaki disease are listed as Table 3. We have established the “Kuomnemonic” for rapid memorization of the diagnostic criteria of KD (Table 4).
Fig. 8 Desquamation over the tip of toes
Table 2 Clinical symptoms and signs of Kawasaki disease. A summary of the clinical features from 350 cases observed inKaohsiung, Taiwan
Clinical presentations Percentage (%)
Conjunctivitis 93
Strawberry tongue 92
Desquamation over finger tip 91
Polymorphism skin rash 91
Indurations of palm 75
BCG scar indurations 42
Neck lymphadenopathy 38
Encyclopedia of Inflammatory DiseasesDOI 10.1007/978-3-0348-0620-6_96-1# Springer Basel 2015
Page 6 of 14

To date, there is no specific diagnostic laboratory test for KD available. The diagnosis is based on theclinical phenotype, i.e., the presence of fever lasting longer than 5 days and the fulfillment of four of fivespecific clinical criteria. In Japan, at least five of six criteria (fever and five other clinical criteria) should befulfilled for the diagnosis of KD. However, a diagnosis of KD can be made when coronary aneurysm ordilatation is identified in patients with four of the principal clinical features. According to the JapaneseCirculation Society JointWorking Groups criteria (JCS JointWorking Group 2010), KD can be diagnosedeven when fever lasts less than 5 days. However, according to the American Heart Association (AHA)criteria, fever lasting more than 5 days is essential for the diagnosis of KD.
Some patients who do not fulfill the criteria have been diagnosed with “incomplete” or “atypical”KD, a diagnosis often based on echocardiographic identification of CAL. The term “incomplete” maybe preferable to “atypical” because these patients have insufficient criteria instead of atypicalpresentation.
In countries with a bacillus Calmette-Guérin (BCG) vaccine policy (i.e., Taiwan, Turkey, and Japan),KD with erythematous induration or even ulceration of the BCG scar has been observed in near 50 % ofKD patients (the incidence of BCG site induration is higher than that of neck lymphadenopathy in thesecountries). Redness or the formation of a crust at the BCG inoculation site is a useful diagnostic sign forKD in children aged 3–20 months. Even if patients exhibit 4 or fewer signs of the clinical criteria for KD,physicians should consider the redness or crust formation at the BCG inoculation site as a possibleindicator of KD.
Incomplete cases of KD are not uncommon (up to 15–20 %). The incidence of CAL in patientsexhibiting four principal symptoms of KD is slightly higher than that in patients with five to six principalsymptoms. Presentation of a small number (<4) of principal symptoms does not indicate a milder form ofthe disease. Patients with at least four principal symptoms require the same treatment as patients withcomplete (typical) presentation of KD, and those with three or fewer principal symptoms should be treatedsimilarly when they meet the supplementary criteria. Herein, common supplementary criteria for thediagnosis of incomplete KD are introduced.
Table 4 “Kuo mnemonic” for the diagnostic criteria regarding the rapid memorization of Kawasaki Disease
Number Mnemonic Clinical signs
1 “One” mouth Diffuse mucosal inflammation with strawberry tongue and fissurelips
2 “Two” eyes Bilateral non-purulent conjunctivitis
3 “Three” fingers palpation neck lymphnodes
Unilateral cervical lymphadenopathy
4 “Four” limbs changes Indurative angioedema over both the hands and feet
5 “Five” = multiple skin rash Dysmorphic skin rashes
Table 3 Diagnostic criteria for Kawasaki disease
Fever more than 5 days
1. Diffuse mucosal inflammation (fissure lip, strawberry tongue)
2. Bilateral nonpurulent conjunctivitis
3. Polymorphous skin rashes (skin rash, wheal formation, urticaria like, any kinds of skin rash should be considered withKD-related when suspect KD)
4. Indurative angioedema of the hands and feet (desquamation in the subacute stage)
5. Cervical lymphadenopathy (unilateral lymphadenopathy, more than 1.5 cm in diameter)
The diagnosis of Kawasaki disease is considered confirmed by the presence of fever, and 4 of the remaining 5 criteria if otherknown diseases can be excluded
Encyclopedia of Inflammatory DiseasesDOI 10.1007/978-3-0348-0620-6_96-1# Springer Basel 2015
Page 7 of 14
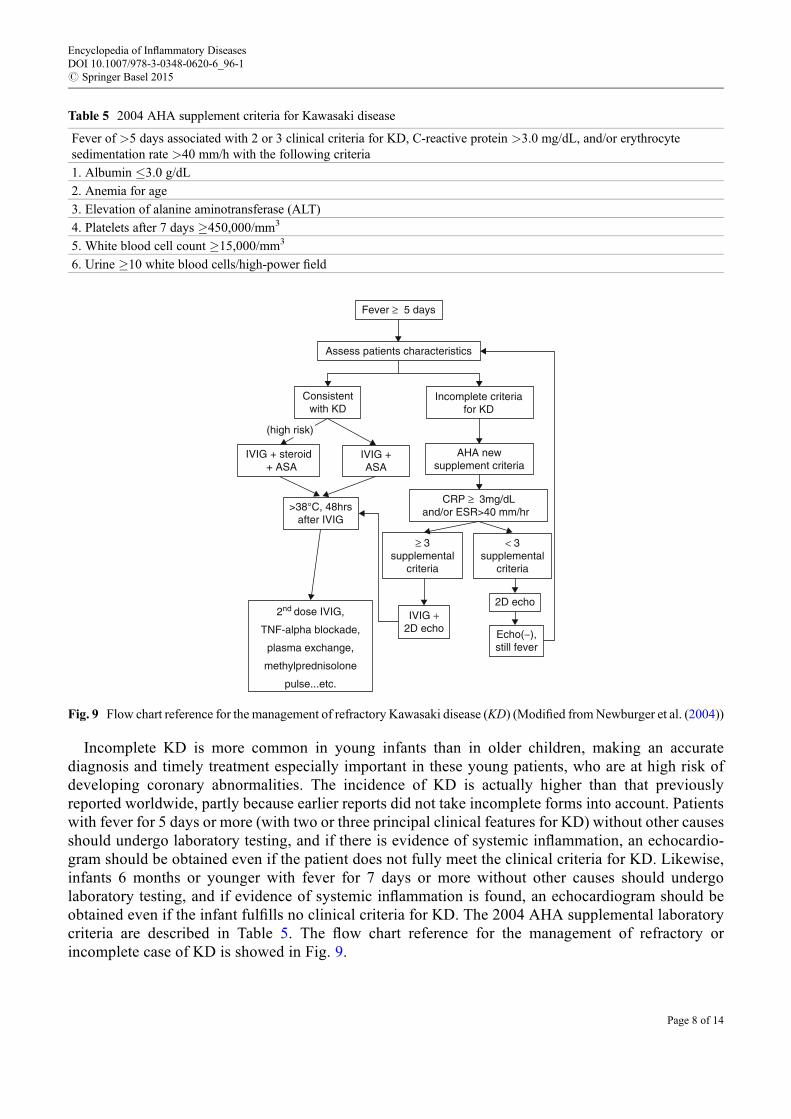
Incomplete KD is more common in young infants than in older children, making an accuratediagnosis and timely treatment especially important in these young patients, who are at high risk ofdeveloping coronary abnormalities. The incidence of KD is actually higher than that previouslyreported worldwide, partly because earlier reports did not take incomplete forms into account. Patientswith fever for 5 days or more (with two or three principal clinical features for KD) without other causesshould undergo laboratory testing, and if there is evidence of systemic inflammation, an echocardio-gram should be obtained even if the patient does not fully meet the clinical criteria for KD. Likewise,infants 6 months or younger with fever for 7 days or more without other causes should undergolaboratory testing, and if evidence of systemic inflammation is found, an echocardiogram should beobtained even if the infant fulfills no clinical criteria for KD. The 2004 AHA supplemental laboratorycriteria are described in Table 5. The flow chart reference for the management of refractory orincomplete case of KD is showed in Fig. 9.
Table 5 2004 AHA supplement criteria for Kawasaki disease
Fever of >5 days associated with 2 or 3 clinical criteria for KD, C-reactive protein >3.0 mg/dL, and/or erythrocytesedimentation rate >40 mm/h with the following criteria
1. Albumin �3.0 g/dL
2. Anemia for age
3. Elevation of alanine aminotransferase (ALT)
4. Platelets after 7 days �450,000/mm3
5. White blood cell count �15,000/mm3
6. Urine �10 white blood cells/high-power field
Fever ≥ 5 days
Assess patients characteristics
Consistentwith KD
IVIG + steroid + ASA
IVIG +ASA
>38°C, 48hrsafter IVIG
AHA newsupplement criteria
CRP ≥ 3mg/dLand/or ESR>40 mm/hr
≥ 3supplemental
criteria
IVIG +2D echo
2nd dose IVIG,
TNF-alpha blockade,
plasma exchange,
methylprednisolone
pulse...etc.
2D echo
Echo(−),still fever
< 3supplemental
criteria
Incomplete criteriafor KD
(high risk)
Fig. 9 Flow chart reference for the management of refractory Kawasaki disease (KD) (Modified fromNewburger et al. (2004))
Encyclopedia of Inflammatory DiseasesDOI 10.1007/978-3-0348-0620-6_96-1# Springer Basel 2015
Page 8 of 14

If a patient has more than three supplementary criteria, incomplete KD is diagnosed and IVIG should beprescribed before performing echocardiography (Newburger et al. 2004).
Therapy
Intravenous Immunoglobulin (IVIG or IVGG)IVIG was used for treatment of KD since 1983 reported by Furusho et al. (1983), more than 10 years afterfirst report of KD by Dr. Kawasaki. A randomized control trail revealed that high-dose IVIG (400 mg/kg/day for 4 days) is safe and effective in reducing the prevalence of CAL from 20 % to 3–5 % whenadministered in those at the acute stage of KD. A study by Newburger et al. contributed greatly in thisregard, and a single high dose of IVIG (2 g/kg) is considered to be the gold standard therapy in the acutestage of KD in 1991 (Newburger et al. 1991). The mechanism of IVIG in reducing inflammation in KD isnot clearly understood. Possible mechanisms include Fc receptor blockade, neutralization of the causativeagents or a toxin produced by an infectious agent, an immunomodulating effect, induction of suppressoractivity, and modulation of the production of cytokines and cytokine antagonists. IVIG treatment reducedthe activity of oxidative stress, which provokes vasculitis in KD. The mechanism of IVIG action is stillunder investigation. IVIG appears to have a generalized anti-inflammatory effect. Possible mechanisms ofaction include modulation of cytokine production, neutralization of bacterial superantigens or otheretiologic agents, augmentation of regulatory T cell activity (TGF-b), suppression of antibody synthesisand inflammatory markers (CD40-CD40L, nitric oxide, and iNOS expression), provision of anti-idiotypicantibodies, Fc-gamma receptor, and balancing Th1/Th2 immune responses (Kuo et al. 2009, 2011; Wanget al. 2002, 2003).
KD patients should be treated with a single 12-h infusion of IVIG, 2 g/kg in a single infusion, togetherwith aspirin in acute phase with fever. This therapy should be performed within 10 days of illness onset,and, if this is not possible, within 7 days of illness onset. Treatment of KD before day 5 of illness appearsnomore likely to prevent cardiac sequelae than treatment on days 5–9. It may, however, be associated withan increased need for IVIG re-treatment. In the presence of four of five classic criteria for KD, US andJapanese experts agree that only 4 days of fever are necessary before initiating treatment with IVIG.
The efficacy of treating patients using IVIG after 10 days of illness is unknown; therefore, earlydiagnosis and treatment is desired. IVIG should be administered to children presenting after day 10 ofillness (i.e., children with delayed diagnosis or incomplete KD) if they have either persistent fever withoutexplanation or aneurysms and ongoing systemic inflammation, as manifested by elevated ESR or CR-P. Any child with KDwho has evidence of persisting inflammation, including fever or high concentrationsof inflammatory markers with or without coronary artery abnormalities, should be treated even if thediagnosis is made after 10 days of illness. For IVIG-resistant patients, earlier and more effective anti-inflammatory therapy might not be emphasized enough to reduce the risk of CAL.
AspirinNow, aspirin is forbidden to be used in children for antipyretics regiment except in cases of KD. Aspirinhas been prescribed in the treatment of KD for many years, even before the usage of IVIG. Althoughaspirin has important anti-inflammatory (high dose) and antiplatelet (low dose, 3–5 mg/kg/day) effects, itdoes not appear to reduce the frequency of CAL formation and IVIG resistance rate. Anti-inflammatorydoses of aspirin are recommended in conjunction with IVIG, but controversy remains regarding anti-inflammatory doses of aspirin. In North America, high-dose (80–100 mg/kg per day) aspirin is mostwidely used during the acute phase. In Japan, concern about hepatic toxicity has led to the use ofmoderate-dose (30–50 mg/kg per day) aspirin as a recommended standard therapy in the acute phase.
Encyclopedia of Inflammatory DiseasesDOI 10.1007/978-3-0348-0620-6_96-1# Springer Basel 2015
Page 9 of 14

The results of our previous study indicate that treatment without aspirin in acute-stage KD had no effecton the response rate of IVIG therapy, duration of fever, or CAL incidence (Hsieh et al. 2004). High- ormedium-dose aspirin therapy may be unnecessary in acute KD when the available data show noappreciable benefits in preventing the failure of IVIG therapy or CAL formation or in shorteningfever duration. Aspirin has been reported to have hemolytic potential in individuals with glucose-6-phosphate dehydrogenase (G6PD) deficiency. Whether or not high-dose aspirin should be utilized in theacute stage of KD needs further multiple center randomized control trials before making a definitiverecommendation.
SteroidsAlthough corticosteroids are the treatment of choice in other forms of vasculitis, the usefulness of steroidsin treatment of KD is not well established. Corticosteroids were used as the initial therapy for KD longbefore the first report of IVIG efficacy. An early study suggested that steroids exerted a negative effectwhen used as the initial therapy for KD, but some studies have shown possible benefit. Corticosteroidtherapy combined with IVIG as the initial treatment was showed rapidly ameliorated symptoms byreducing cytokine levels in children with KD. Methylprednisolone and IVIG were also effective andsafe as a primary treatment for high-risk KD patients. However, Newburger et al. (2007) demonstratedthat their data do not provide support for the addition of a single-pulsed dose of intravenous methylpred-nisolone to IVIG for routine primary treatment of children with KD. Meta-analysis of comparison of theincidence of CAL between IVIG plus corticosteroid therapy and IVIG therapy alone for the initialtreatment of KD showed that IVIG plus corticosteroid therapy significantly reduced the risk of coronaryabnormality (Kobayashi et al. 2012). In conclusion, steroids are beneficial for acute stage of KDespecially in cases involving the high-risk group but not necessarily for methylprednisolone pulse as anadditional treatment to initial IVIG.
OthersA new class of therapies directed against specific cytokines has expanded treatment for KD. Infliximab isa monoclonal antibody to TNF-a and has been effective in the treatment of patients with refractoryKD. Treatment with infliximab might also be an initial therapy for high-risk KD patients. Acute KD canlead to the development of large coronary artery aneurysms that may persist for years. Abciximab, aplatelet glycoprotein IIb/IIIa receptor inhibitor, is associated with resolution of thrombi and vascularremodeling in adults with acute coronary syndromes. KD patients who were treated with abciximab anddemonstrated greater regression in aneurysm diameter at early follow-up were reported. Abciximab seemsto benefit KD patients, especially those who developed aneurysms.
There are still no well-defined treatments for refractory KD (all see Fig. 9). Cyclosporine A (CyA)treatment is considered safe and well tolerated and may serve as a promising option for patients withrefractory KD. Hyperkalemia developed in 9/28 (32 %) patients 3–7 days after commencing CyAtreatment. Adverse effects such as arrhythmias should be monitored with CyA.
Specific changes in inflammatory markers (such as white blood cell count, neutrophil count, C-reactiveprotein, IL-6, soluble IL-2 receptor, T helper-type 17/regulatory Tcell imbalance, and IL-1 pathway) havebeen reported to disturb immunological functions and result in KD with IVIG resistance and CALformation. This indicates the possible treatment role of plasma exchange (PE) for KD with IVIGresistance. PE is considered safe and effective in the prevention of CAL in KD that is refractory toIVIG therapy. PE could be performed at an early stage, as soon as fractional increases in inflammatorymarkers are found after first or second dosage of IVIG therapy.
Encyclopedia of Inflammatory DiseasesDOI 10.1007/978-3-0348-0620-6_96-1# Springer Basel 2015
Page 10 of 14

Outcome
Coronary Artery Lesions (CAL) and AneurysmEven after the use of high-dose IVIG treatment, there are still 3–5 % of KD patients that developedCAL. This may indicate that anti-inflammatory regiments other than IVIG are needed for high-risk KDpatients. The most serious complication of KD is the development of CAL, including myocardialinfarction, coronary artery fistula formation (Liang et al. 2009), coronary artery dilatation, and coronaryartery aneurysm. Definition of CAL (also known as coronary artery abnormality) is based on the JapaneseMinistry of Health criteria:>3 mmmaximum absolute internal diameter of the coronary artery in childrenyounger than 5 years of age or >4 mm in children 5 years and older, or a segmental diameter 1.5 timesgreater than that of an adjacent segment, or the presence of luminal irregularity.
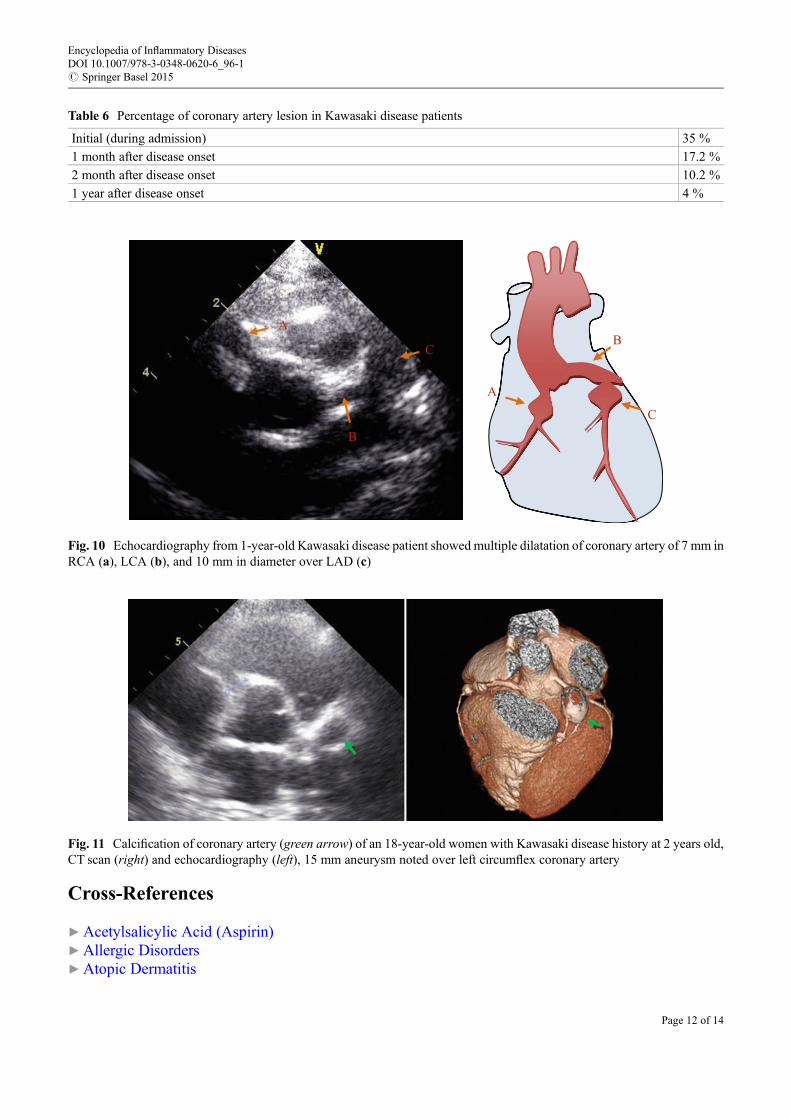
Coronary arteries should be corrected relative to body surface area (BSA) (if body weight and bodyheight were available) and expressed as standard deviation units from the mean (Z scores). Several studieshave analyzed CAL, including aortic root dimension, and transient CAL (the definition of “transient”varies among studies, from 30 days to 6–8 weeks after diagnosis of disease). As such, KD patients withcoronary artery ectasia or dilatation, which disappears within the first 8 weeks after disease onset, aredefined as transient ectasia or dilatation (transient CAL). According to our previous report on CALanalysis including 341 KD patients, 35 % of KD patients had dilatation during the acute phase ofadmission, 17.2 % had dilatation 1 month after disease onset, 10.2 % had dilatation at 2 months, and4 % had persistent CAL for more than 1 year (Table 6). Echocardiography is most common tool forfollow-up cardiovascular complication of KD patients, the time schedule varying according to severity ofCAL. Computed tomography (CT) scan also provides good image of coronary artery. Figures 10 and 11show coronary artery dilation or aneurysm formation with calcification in KD patient fromcardioechography and CT scan.
IVIG Resistance or NonresponsivenessHowever, there are still 7.8–38.3 % of children that are unresponsive to initial IVIG treatment. Recentstudies have identified demographic and laboratory characteristics as predictors of IVIG resistance,including age, illness day, platelet count, erythrocyte sedimentation rate, hemoglobin concentration,C-reactive protein, eosinophil, lactate dehydrogenase, albumin, alanine aminotransferase (ALT),G-CSF, and sonographic gallbladder abnormalities (Abe et al. 2008; Kuo et al. 2010). Because IVIG-resistant patients are at a higher risk for CAL formation, it is important to identify those who may benefitfrom a more aggressive therapy.
Allergic Diseases Followed Kawasaki DiseaseAtopic dermatitis (AD) was shown to increase the incidence among children with KD than that ofcontrols. KD was reported to be associated with AD, allergy, elevated total serum IgE levels, andeosinophilia and that may be related to the effects of IL-4 (Burns et al. 2005; Kuo et al. 2007). KD maybe a risk factor for subsequent allergic disease and occurs more frequently in children at risk of immunedisequilibrium, with an initial abnormal inflammatory response, and, subsequently, more allergic mani-festations as well as admitted with asthma/allergy. T-helper (Th) type 2 immune response was elevated inthe acute stage of KD, including eosinophils, IL-4, IL-5, and eotaxin than in age-matched control. There isa fair amount of evidence to support abnormal Th1/Th2 balance in KD patients. Comparison ofeosinophils in KD and enterovirus (EV) patients with IVIG treatment demonstrated a more significanteosinophil increase in KD patients than patient with EVafter IVIG treatment (Lin et al. 2012). This mayindicate an imbalance of the Th1/Th2 immune response, with a skewed Th2 response in KD. The skewedTh2 immune response in patient with KD may lead to allergic diseases late after disease onset.
Encyclopedia of Inflammatory DiseasesDOI 10.1007/978-3-0348-0620-6_96-1# Springer Basel 2015
Page 11 of 14
Cross-References
▶Acetylsalicylic Acid (Aspirin)▶Allergic Disorders▶Atopic Dermatitis
Table 6 Percentage of coronary artery lesion in Kawasaki disease patients
Initial (during admission) 35 %
1 month after disease onset 17.2 %
2 month after disease onset 10.2 %
1 year after disease onset 4 %
C
B
A
A
B
C
Fig. 10 Echocardiography from 1-year-old Kawasaki disease patient showed multiple dilatation of coronary artery of 7 mm inRCA (a), LCA (b), and 10 mm in diameter over LAD (c)
Fig. 11 Calcification of coronary artery (green arrow) of an 18-year-old women with Kawasaki disease history at 2 years old,CT scan (right) and echocardiography (left), 15 mm aneurysm noted over left circumflex coronary artery
Encyclopedia of Inflammatory DiseasesDOI 10.1007/978-3-0348-0620-6_96-1# Springer Basel 2015
Page 12 of 14

▶Autoinflammatory Syndromes▶Henoch-Schonlein Purpura▶ Idiopathic Thrombocytopenic Purpura▶ Inflammation and Autoimmunity▶ Juvenile Idiopathic Arthritis▶Rheumatic fever
References
Abe, J., Ebata, R., Jibiki, T., Yasukawa, K., Saito, H., & Terai, M. (2008). Elevated granulocyte colony-stimulating factor levels predict treatment failure in patients with Kawasaki disease. The Journal ofAllergy and Clinical Immunology, 122(5), 1008–1013 e1008.
Burns, J. C., & Glode, M. P. (2004). Kawasaki syndrome. Lancet, 364(9433), 533–544.Burns, J. C., Shimizu, C., Shike, H., Newburger, J. W., Sundel, R. P., Baker, A. L., et al. (2005). Family-
based association analysis implicates IL-4 in susceptibility to Kawasaki disease. Genes and Immunity,6(5), 438–444.
Furusho, K., Sato, K., Soeda, T., Matsumoto, H., Okabe, T., Hirota, T., et al. (1983). High-doseintravenous gammaglobulin for Kawasaki disease. Lancet, 2(8363), 1359.
Hsieh, K. S., Weng, K. P., Lin, C. C., Huang, T. C., Lee, C. L., & Huang, S. M. (2004). Treatment of acuteKawasaki disease: Aspirin’s role in the febrile stage revisited. Pediatrics, 114(6), e689–e693.
Hsieh, K. S., Lai, T. J., Hwang, Y. T., Lin, M. W., Weng, K. P., Chiu, Y. T., et al. (2011). IL-10 promotergenetic polymorphisms and risk of Kawasaki disease in Taiwan. Disease Markers, 30(1), 51–59.
Huang, W. C., Huang, L. M., Chang, I. S., Chang, L. Y., Chiang, B. L., Chen, P. J., et al. (2009).Epidemiologic features of Kawasaki disease in Taiwan, 2003–2006. Pediatrics, 123(3), e401–e405.
JCS JointWorking Group (2010). Guidelines for diagnosis andmanagement of cardiovascular sequelae inKawasaki disease (JCS 2008)–digest version. Circ J, 74(9), 1989–2020.
Khor, C. C., Davila, S., Breunis, W. B., Lee, Y. C., Shimizu, C., Wright, V. J., et al. (2011). Genome-wideassociation study identifies FCGR2A as a susceptibility locus for Kawasaki disease. Nature Genetics,43(12), 1241–1246.
Kobayashi, T., Saji, T., Otani, T., Takeuchi, K., Nakamura, T., Arakawa, H., et al. (2012). Efficacy ofimmunoglobulin plus prednisolone for prevention of coronary artery abnormalities in severe Kawasakidisease (RAISE study): A randomised, open-label, blinded-endpoints trial.Lancet, 379(9826), 1613–1620.
Kuo, H. C., & Chang, W. C. (2011). Genetic polymorphisms in Kawasaki disease. Acta PharmacologicaSinica, 32(10), 1193–1198.
Kuo, H. C., Yang, K. D., Liang, C. D., Bong, C. N., Yu, H. R., Wang, L., et al. (2007). The relationship ofeosinophilia to intravenous immunoglobulin treatment failure in Kawasaki disease. Pediatric Allergyand Immunology, 18(4), 354–359.
Kuo, H. C., Wang, C. L., Liang, C. D., Yu, H. R., Huang, C. F., Wang, L., et al. (2009). Association oflower eosinophil-related T helper 2 (Th2) cytokines with coronary artery lesions in Kawasaki disease.Pediatric Allergy and Immunology, 20(3), 266–272.
Kuo, H. C., Liang, C. D., Wang, C. L., Yu, H. R., Hwang, K. P., & Yang, K. D. (2010). Serum albuminlevel predicts initial intravenous immunoglobulin treatment failure in Kawasaki disease. ActaPaediatrica, 99(10), 1578–1583.
Kuo, H. C., Onouchi, Y., Hsu, Y. W., Chen, W. C., Huang, J. D., Huang, Y. H., et al. (2011a). Poly-morphisms of transforming growth factor-beta signaling pathway and Kawasaki disease in the Tai-wanese population. Journal of Human Genetics, 56(12), 840–845.
Encyclopedia of Inflammatory DiseasesDOI 10.1007/978-3-0348-0620-6_96-1# Springer Basel 2015
Page 13 of 14

Kuo, H. C., Yang, K. D., Juo, S. H., Liang, C. D., Chen, W. C., Wang, Y. S., et al. (2011b). ITPKC singlenucleotide polymorphism associated with the Kawasaki disease in a Taiwanese population. PloS One,6(4), e17370.
Kuo, H. C., Yang, K. D., Chang, W. C., Ger, L. P., & Hsieh, K. S. (2012a). Kawasaki disease: An updateon diagnosis and treatment. Pediatrics and Neonatology, 53(1), 4–11.
Kuo, H. C., Yang, Y. L., Chuang, J. H., Tiao, M.M., Yu, H. R., Huang, L. T., et al. (2012b). Inflammation-induced hepcidin is associated with the development of anemia and coronary artery lesions inKawasaki disease. Journal of Clinical Immunology, 32(4), 746–752.
Lee, Y. C., Kuo, H. C., Chang, J. S., Chang, L. Y., Huang, L. M., Chen, M. R., et al. (2012). Two newsusceptibility loci for Kawasaki disease identified through genome-wide association analysis. NatureGenetics, 44(5), 522–525.
Liang, C. D., Kuo, H. C., Yang, K. D., Wang, C. L., & Ko, S. F. (2009). Coronary artery fistula associatedwith Kawasaki disease. American Heart Journal, 157(3), 584–588.
Lin, I. C., Kuo, H. C., Lin, Y. J., Wang, F. S., Wang, L., Huang, S. C., et al. (2012a). Augmented TLR2expression on monocytes in both human Kawasaki disease and a mouse model of coronary arteritis.PloS One, 7(6), e38635.
Lin, L. Y., Yang, T. H., Lin, Y. J., Yu, H. R., Yang, K. D., Huang, Y. C., et al. (2012b). Comparison of thelaboratory data between Kawasaki disease and enterovirus after intravenous immunoglobulin treat-ment. Pediatric Cardiology, 33(8), 1269–1274.
Nakamura, Y., Yashiro, M., Uehara, R., Sadakane, A., Tsuboi, S., Aoyama, Y., et al. (2012). Epidemio-logic features of Kawasaki disease in Japan: Results of the 2009–2010 nationwide survey. Journal ofEpidemiology, 22(3), 216–221.
Newburger, J. W., Takahashi, M., Beiser, A. S., Burns, J. C., Bastian, J., Chung, K. J., et al. (1991).A single intravenous infusion of gamma globulin as compared with four infusions in the treatment ofacute Kawasaki syndrome. The New England Journal of Medicine, 324(23), 1633–1639.
Newburger, J. W., Takahashi, M., Gerber, M. A., Gewitz, M. H., Tani, L. Y., Burns, J. C., et al. (2004).Diagnosis, treatment, and long-term management of Kawasaki disease: A statement for health pro-fessionals from the Committee on Rheumatic Fever, Endocarditis and Kawasaki Disease, Council onCardiovascular Disease in the Young, American Heart Association. Circulation, 110(17), 2747–2771.
Newburger, J.W., Sleeper, L. A.,McCrindle, B.W.,Minich, L. L., Gersony,W., Vetter, V. L., et al. (2007).Randomized trial of pulsed corticosteroid therapy for primary treatment of Kawasaki disease. The NewEngland Journal of Medicine, 356(7), 663–675.
Onouchi, Y., Ozaki, K., Burns, J. C., Shimizu, C., Terai, M., Hamada, H., et al. (2012). A genome-wideassociation study identifies three new risk loci for Kawasaki disease. Nature Genetics, 44(5), 517–521.
Tsai, F. J., Lee, Y. C., Chang, J. S., Huang, L. M., Huang, F. Y., Chiu, N. C., et al. (2011). Identification ofnovel susceptibility Loci for kawasaki disease in a Han chinese population by a genome-wideassociation study. PloS One, 6(2), e16853.
Wang, C. L., Wu, Y. T., Lee, C. J., Liu, H. C., Huang, L. T., & Yang, K. D. (2002). Decreased nitric oxideproduction after intravenous immunoglobulin treatment in patients with Kawasaki disease. TheJournal of Pediatrics, 141(4), 560–565.
Wang, C. L., Wu, Y. T., Liu, C. A., Lin, M. W., Lee, C. J., Huang, L. T., et al. (2003). Expression of CD40ligand on CD4+ T-cells and platelets correlated to the coronary artery lesion and disease progress inKawasaki disease. Pediatrics, 111(2), E140–E147.
Wang, C. L., Wu, Y. T., Liu, C. A., Kuo, H. C., & Yang, K. D. (2005). Kawasaki disease: Infection,immunity and genetics. The Pediatric Infectious Disease Journal, 24(11), 998–1004.
Encyclopedia of Inflammatory DiseasesDOI 10.1007/978-3-0348-0620-6_96-1# Springer Basel 2015
Page 14 of 14