keep your patients “moving” - home | continuing … · types of constipation: chronic...
TRANSCRIPT

DRUGTOPICS.COM | MAY 2016 | DrugTopics 49
GOAL: To assist pharmacists and pharmacy technicians in their understanding of the role of linaclotide, lubiprostone, methylnaltrexone, and naloxegol in the treatment of constipation after traditional nonpharmacologic interventions and conventional laxatives such as bulking agents, osmotic laxatives, and stimulant laxatives have failed.
After participating in this activity, pharmacists will be able to: > Discuss the different causes of constipation,
including opioid-induced constipation (OIC), chronic constipation, and constipation predominant irritable bowel syndrome (IBS-C)
> De� ne constipation according to Rome III and the American Gastroenterological Association criteria
> Identify the risk factors for constipation
> Review available OTC and prescription drug therapies for constipation, including mechanism of action, indications, side effects, onset of effect, duration of therapy, and clinical usage considerations
> Outline the pharmacist’s role in providing recommendations to treat constipation, referral to a physician for inadequate response to OTC therapies and counseling patients to prevent the development of constipation
After participating in this activity, pharmacy technicians will be able to: > Recall the basic de� nition of constipation
> Recall the risk factors for constipation
> List available OTC and prescription drug therapies for constipation
> Recognize when to refer patients to the pharmacist for recommendations on constipation management.
The University of Connecticut School of Pharmacy is accredited by the Accreditation Council for Pharmacy Education as a provider of
continuing pharmacy education.
Pharmacists and pharmacy technicians are eligible to participate in the knowledge-based activity, and will receive up to 0.2 CEUs (2 contact hours) for completing the activity, passing the quiz with a grade of 70% or better, and completing an online evaluation. Statements of credit are available via the CPE Monitor online system and your participation will be recorded with CPE Monitor within 72 hours of submission.
ACPE# 0009-9999-16-028-H01-PACPE# 0009-9999-16-028-H01-T
Grant support: Supported by an independent educational grant from AstraZeneca
Activity Fee: There is no fee for this activity.
INITIAL RELEASE DATE: MAY 10, 2016EXPIRATION DATE: MAY 10, 2018
To obtain CPE credit, visit www.drugtopics.com/cpe and click on the “Take a Quiz” link. This will direct you to the UConn/Drug Topics website, where you will click on the Online CE Center. Use your NABP E-Pro� le ID and the session code: 16DT28-JVX38 for pharma-cists or the session code: 16DT28-TAK49 for pharmacy technicians to access the online quiz and evaluation. First-time users must pre-register in the On-line CE Center. Test results will be displayed immediately and your participation will be recorded with CPE Monitor within 72 hours of completing the requirements.
For questions concerning the online CPE activities, e-mail: [email protected].
Educational Objectives
IMAG
E: G
ETTY
IMAG
ES /
PH
OTO
ALTO
/LAU
REN
CE M
OU
TON
Faculty: Trinh Pham, PharmD, BCOPDr. Pham is an associate clinical professor at the University of Connecticut, School of Pharmacy, Storrs, Conn.
Faculty Disclosure: Dr. Pham has no actual or potential con� ict of interest associated with this article.
Disclosure of Discussions of Off-Label and Investigational Uses of Drugs: This activity may contain discussion of unlabeled/unapproved use of drugs in the United States and will be noted if it occurs. The content and views presented in this educational program are those of the faculty and do not necessarily represent those of Drug Topics or University of Connecticut School of Pharmacy. Please refer to the of� cial information for each product for discussion of approved indications, contraindications, and warnings.
AbstractConstipation is a common medical problem that can affect patients’ quality of life and ability to function. Patients who are constipated most likely seek treatment � rst by using over-the-counter products and then by visiting their physician if self-treatment was not effective. In recent years, a number of drugs with novel mechanisms of action have been made available for the treatment of constipation, including linaclotide, lubiprostone, methylnaltrexone, and naloxegol. This review will discuss the role of these new agents after treatment failure with conventional laxatives for the treatment of the three most common types of constipation: chronic idiopathic constipation, irritable bowel syndrome with constipation, and opioid-induced constipation.
Trinh Pham, PharmD, BCOPASSOCIATE CLINICAL PROFESSOR, UNIVERSITY OF CONNECTICUT, SCHOOL OF PHARMACY, STORRS, CONN.
AN ONGOING CE PROGRAM OF THE UNIVERSITY OF CONNECTICUT
SCHOOL OF PHARMACY AND DRUG TOPICS
AND
EARN CE CREDIT FOR THIS ACTIVITY AT WWW.DRUGTOPICS.COM /CPE
2CPECREDITS
Keep your patients “moving” An overview of treatment optionsfor constipation

AN OVERVIEW OF TREATMENT OPTIONS FOR CONSTIPATION
50 DrugTopics | MAY 2016 | DRUGTOPICS.COM
CONTINUING EDUCATION
Constipation is a common medical problem that affects patients’ quality of life and inter-feres with daily functioning and well-being.1
Patients with constipation suffer physical and mental discomfort, they are frustrated from lack of effective therapies, and fear their symptoms will relapse. Furthermore, consti-pation affects their well-being and interferes with activities of daily living.1 Chronic idiopath-ic constipation (CIC), irritable bowel syndrome with constipation (IBS-C), and opioid-induced constipation (OIC) are the three most com-mon types of constipation diagnoses. The estimated prevalence rates of CIC and IBS-C in the United States are 14% (~42 million individuals) and 5% (~15 million individuals), respectively.2,3 For OIC, it is estimated that 40% to 90% of patients who use opioids to treat pain experience constipation as a side effect of the opioid. Approximately 4% (~12 million people) of adults in the United States take chronic opioids; thus, 5 to 11 million individuals may have OIC.4,5 Approximately 29% to 34% of patients with constipation seek medical care for self-reported constipa-tion, and 7.2% seek care from pharmacists.1
Constipation-related symptoms account for 2.5 million physician of� ce visits annually, with 85% of these visits resulting in a drug prescription. More than $500 million is spent on laxatives each year. These numbers un-derscore the fact that drugs contribute sig-ni� cantly to the healthcare costs of treating constipation.1
The past 10 years have seen signi� cant developments in the treatment of CIC, IBS-C, and OIC, and several new drugs with novel mechanisms of action have received ap-proval from the Food and Drug Administra-tion (FDA) over the past � ve years. These new agents include linaclotide, lubiprostone, naloxegol, and methylnaltrexone. This article will review the mechanisms of action and side effects of these agents and discuss when these agents should be used to treat patients diagnosed with CIC, IBS-C, or OIC.
De� nition of constipationAppropriate treatment of constipation relies on the accurate diagnosis since the pathophysiol-ogy determines how the constipation may best be treated. For example, the mechanism of OIC is distinctly different from that of CIC and IBS-C,
and so drugs that work for OIC may not be effective for CIC and IBS-C.
Constipation can result from distur-bances in colonic motility and/or problems related to defecating. Constipation can be classi� ed as primary or secondary constipa-tion. Primary constipation may be idiopathic or functional and is divided into three cat-egories: normal-transit constipation, slow-transit constipation, or pelvic � oor disorder.6 Secondary constipation can be caused by an organic disease (i.e., stroke, colorectal cancer, hypothyroidism) or medications (e.g., anticholinergics, antidepressants, anticonvul-sants).6
There is no standardized de� nition for OIC. A multidisciplinary consensus group of experts proposed de� ning OIC as a change from baseline bowel habits upon initiation of opioids. OIC is characterized by reduced bowel movement frequency, development or
worsening of straining to pass stool, a sense of incomplete rectal evacuation, and harder stool consistency.7
Similarly, the Rome III diagnostic criteria are used to de� ne CIC and IBS-C, which are also considered to be functional constipa-tion.8 CIC is de� ned as the presence of ≥ 2 of the following for ≥ 25% of defecations for ≥ 3 months with symptom onset ≥ 6 months before diagnosis: straining, lumpy or hard stools, sensation of incomplete evacuation, sense of anorectal obstruction/blockage, manual maneuvers to facilitate defecation. Additionally, loose stools are rarely present without laxatives and criteria for IBS-C is not ful� lled. IBS-C is de� ned as recurrent abdomi-nal pain or discomfort ≥ 3 days per month in the last 3 months, with symptom onset ≥ 6 months before diagnosis, and with ≥ 2 of the following: improvement with defecation, onset associated with a change in stool frequency, onset associated with a change in stool form.
The Rome III diagnostic criteria consider IBS-C and CIC as mutually exclusive distinct entities; however, patients with CIC also ex-
perience the symptoms of abdominal pain, discomfort, and bloating that de� ne IBS-C.9
An accurate diagnosis of CIC or IBS-C can be complicated based on the observation that the symptoms of constipation transition over time from a 12-year population-based survey assessing the natural history of func-tional gastrointestinal tract disorders.10 The investigators discovered that 40% of patients reported different symptoms with a follow-up survey compared to the initial survey, which may result in a different classi� cation and treatment of constipation symptoms.
Assessment of constipationBecause constipation is generally a symptom-based diagnosis, in addition to performing a physical examination, clinicians should obtain a thorough history to diagnose and treat pa-tients appropriately. The ideal history includes the patient’s perception of his or her bowel
pattern and a description of stool frequency, stool form, and ease of stool passages. Edu-cating patients so that they understand how to describe their normal bowel patterns and changes in bowel patterns is an essential � rst step in discussing how to recognize constipa-tion. For patients who take opioids for pain management, this discussion by all healthcare providers, including pharmacists, should occur when opioids are � rst prescribed. This estab-lishes a baseline of current bowel function and can be used as a reference for any changes in bowel pattern after initiation of the opioid.
A discussion of bowel patterns and hab-its may be embarrassing and uncomfortable for some patients. The Bristol Stool Form Scale (BSFS) is a useful visual tool that describes stool consistency and form and can facilitate this discussion with patients (Table 1).11
Similarly, the Bowel Function Index (BFI) is a practical, rapid, validated tool that was developed to facilitate assessment of OIC.12
This tool asks patients three questions re-garding the ease of defecation, feeling of
The BSFS is a useful visual tool that describes stool consistency and form and can facilitate the discussion on bowel function.”

CONTINUING EDUCATION
KEEP YOUR PATIENTS “MOVING”
DRUGTOPICS.COM | MAY 2016 | DrugTopics 51
incomplete bowel evacuation, and personal judgment regarding constipation. Each ques-tion is rated on a visual analog scale from 0 to 100, with 0 representing no dif� culty and 100 representing severe dif� culty. The overall score is an average of the response to the three questions. A change in score of ≥12 points suggests a clinically mean-ingful change in constipation symptoms. A multidisciplinary panel of 10 experts with extensive knowledge of opioid-associated adverse events convened to discuss and evaluate an optimal symptom-based tool for assessing OIC for the American Academy of Pain Medicine.13 This panel recommended the use of the three-item BFI because of its simplicity and its validated threshold of clini-cally signi� cant constipation.13 Based on this consensus, the expert panel recommends that patients on opioids for pain manage-ment should complete the BFI.13 Further, it suggests that prescription treatments for OIC should be considered for patients with BFI scores of ≥30 points and an inadequate response to � rst-line interventions for OIC.13
Ef� cacy and safety data of new agents for the treatment of constipationProsecretory agents that act on chloride channelsLinaclotide and lubiprostone are newer secre-tory laxatives that activate chloride channels. These agents have distinct mechanisms of ac-tion, thus offering two unique new drug classes for the treatment of constipation.
Linaclotide is a � rst-in-class drug that activates the guanylate cyclase-C (GC-C) receptor on the lumen of intestinal epi-thelial cells. This opens the cystic � brosis transmembrane regulator (CFTR) chloride
channel to secrete chloride ions and water into the lumen, which leads to increased colonic transit.14 FDA approval of linaclotide for the treatment of CIC was based on the results of two phase 3 randomized, placebo-controlled trials.15 The primary endpoint in the clinical trials was de� ned as both ≥ 3
complete spontaneous bowel movements (CSBM) per week and an increase from baseline of at least one CSBM per week for ≥ 9 of 12 weeks. Patients received daily doses of 145 mcg versus 290 mcg versus placebo. The results of the two trials showed that the primary endpoints were achieved in 16% and 21% of patients receiving 145 mcg linaclotide daily and 19.4% and 21.3% of patients receiving 290 mcg daily compared to only 3.3% and 6% of patients receiving placebo. Improvements in stool consistency (P < 0.001), straining severity (P < 0.001), abdominal discomfort (P < 0.001 to 0.04), bloating (P < 0.001 to 0.006), and constipa-tion severity (P < 0.001) were signi� cantly greater with both doses of linaclotide than with placebo. Discontinuation of linaclotide did not worsen CIC symptoms.15
FDA approval of linaclotide for the treat-ment of IBS-C was also based on the re-sults of two phase 3 randomized, double-blind, placebo-controlled trials.16,17 One trial
was a 12-week study and the other was 26 weeks. These trials assessed responses to primary endpoints that lasted for nine out of 12 weeks. These primary endpoints included improvements in abdominal pain intensity (reduction of ≥30% from baseline in average daily worst pain score) and stool
frequency (increase of at least one CSBM per week from baseline), as speci� ed by an FDA guidance issued in 2012 for the evalu-ation of drug ef� cacy in treating IBS-C.18 A CSBM is defined as a BM that occurs in the absence of any laxative, enema, or sup-pository and accompanied by a feeling of complete evacuation.18 In these two trials, 33.6% and 33.7% of patients treated with linaclotide achieved the primary endpoints compared with 21% and 13.9% of patients in the placebo group (P < 0.0001).16,17 The attrition rate for all patients was 19.4% and 25.6% at weeks 12 and 26, respectively, for both studies. The percentage of patient attri-tion attributed to side effects was 7.8% and 10.1% for patients receiving linaclotide com-pared to 2.5% in both studies for patients on placebo. Attrition due to perceived lack of ef� cacy was 1.2% and 3.7% for patients on linaclotide compared to 1% and 8% for patients on placebo. In the 12-week treat-ment trial, patients were also randomized to a 4-week withdrawal period at the end of the 12 weeks.17 Discontinuation of linaclotide did not cause worsening of IBS-C symptoms compared to baseline; however, abdominal pain did recur, and CSBM decreased to lev-els similar to the placebo group in the initial 12-week treatment period.
Lubiprostone is an analog of prostaglan-din E1 that binds to and directly activates the chloride channel type 2 (ClC-2), which are cell-membrane bound protein pores involved in chloride secretion, in addition to activating CFTR chloride channels. This increases chlo-ride secretion and leads to passive secretion
Bristol Stool Form Scale
Slow transit
Fast transit
Type 1 Separate hard lumps Hard, impacted stool; constipationType 2 Sausage-like but lumpy
Type 3 Sausage-like but with cracks in the surface Considered normal stool; optimal because stool is easy to passType 4 Smooth and soft
Type 5 Soft blobs with clear-cut edges
May indicate diarrhea and urgency
Type 6 Fluffy pieces with ragged edges, a mushy stool
Type 7 Watery, no solid pieces; entirely liquid
Form available at http://bowelcontrol.nih.gov/Bristol_Stool_Form_Scale_508.pdf. Source: Ref 11
TABLE 1
Prescription treatments for OIC should be considered for patients with BFI scores ≥30 and an inadequate response to � rst-line interventions.”

52 DrugTopics | MAY 2016 | DRUGTOPICS.COM
CONTINUING EDUCATION
AN OVERVIEW OF TREATMENT OPTIONS FOR CONSTIPATION
of sodium, water, and isotonic � uid into the intestinal lumen.18 Lubiprostone is poorly absorbed by the gut, and the serum con-centration of this agent is too low to quantify. The drug has been evaluated in patients with CIC, IBS-C, and OIC.
The ef� cacy and safety of lubiprostone in adults with CIC were evaluated in two 4-week, phase 3, double-blind, randomized, placebo-controlled trials.19,20 The primary endpoint de� ned by the study was the num-ber of SBMs during the � rst week of therapy. The primary endpoint was achieved in 5.69% and 5.89% of patients receiving lubiprostone 24 mcg twice daily compared to 3.46% and 3.99% of patients on placebo. The second-ary endpoints were signi� cantly improved with lubiprostone at all weeks compared to placebo and include: SBMs at weeks 2, 3, 4, stool consistency (P < 0.001), straining (P = 0.0003 to < 0.0001), and constipation severity (P < 0.0003 to 0.0265). Nausea was more common in patients receiving lu-biprostone compared to placebo group (38% and 25% vs 4% and 5%). Headache was the second most common side effect for the lubiprostone group (14% and 6%) compared to placebo (7% and 3%).
The FDA approval of lubiprostone for the treatment of IBS-C in women was based on the combined results of two phase 3 randomized, placebo-controlled clinical tri-als and one 36-week, open-label extension study.21,22 The FDA did not deem that ef-� cacy was demonstrated in men because only 8% of patients in the clinical trials were male. The primary endpoint of the two phase 3 studies was overall responder sta-tus calculated from weekly assessments of symptom relief. A patient was considered a monthly responder if: the symptoms were at least moderately relieved for all 4 weeks within the month, or signi� cantly relieved for at least 2 weeks within the month. Patients receiving lubiprostone 8 mcg twice daily had a signi� cantly higher overall response com-pared to placebo (17.9% vs 10.1%) over 12 weeks of treatment (P=0.001). The primary objective of the open-label extension study was assessment of long-term safety and tol-erability.22 Diarrhea (11%) and nausea (11%) were the most common treatment-related adverse effects.22
The efficacy of lubiprostone 24 mcg twice daily versus placebo in patients with OIC and chronic noncancer pain was estab-lished in two randomized clinical trials.23,24 Lubiprostone was shown to lead to a signi� -cantly greater mean change in the frequency of spontaneous bowel movements (SBM) from baseline (P=0.001 to 0.004) and a shorter median time to � rst SBM compared to placebo (P=0.004). The most common side effects with lubiprostone were diarrhea (9.6% - 11.3%), nausea (9.9% - 16.8%), ab-
dominal pain/distention (7.1% - 8.2%), and vomiting (4.2%).23,24
Peripherally acting mu-opioid receptor antagonistsThe peripherally acting mu-opioid receptor an-tagonists (PAMORAs) methylnaltrexone (MNTX) and naloxegol require a prescription and are not laxatives by de� nition. These agents re-verse constipation caused by the binding of opioid receptor agonists to enteric neuron mu receptors widely expressed throughout the gas-trointestinal tract; this binding between opioid receptor agonists and neuron mu receptors im-pairs peristalsis and intestinal secretions and increases luminal � uid reabsorption, leading to constipation.
In 2008, MNTX subcutaneous injection was the � rst PAMORA to be approved by the FDA for the treatment of OIC in pa-tients with advanced illness in whom laxa-tive therapy failed. In 2014, this agent was also approved for the treatment of OIC in patients with chronic noncancer pain. Two multicenter, randomized, controlled trials of MNTX evaluated the occurrence of laxa-tion within four hours after the � rst dose in patients with advanced illness.25,26 These patients had received opioids for at least two weeks and laxatives for at least three days without relief of OIC. Laxation was achieved within four hours in 48% of pa-tients receiving 0.15 mg/kg of subcutane-ous MNTX versus 15% of patients receiving
placebo and in 62% and 58% of patients receiving MNTX 0.15 mg/kg and 0.3 mg/kg, respectively versus 14% of patients receiving placebo. The ef� cacy of MNTX for OIC in patients with chronic noncancer pain was assessed in a phase 3, placebo-controlled, four-week study. Patients re-ceived either subcutaneous MNTX 12 mg once daily or every other day or placebo. Within the � rst four hours, 34% of patients treated with either dosing regimen of MNTX achieved a rescue medication-free bowel
movement (RFBM) versus 10% of patients treated with placebo.27
Naloxegol is a polymer conjugate of nal-oxone. In 2014, naloxegol became the � rst orally administered PAMORA approved by the FDA for the treatment of OIC in patients with noncancer pain. Two identical phase 3 randomized controlled trials evaluated nal-oxegol 12.5 mg and 25 mg versus placebo in patients with chronic, noncancer pain.4
The primary endpoint was the 12-week response rate of at least three SBM per week, an increase from baseline of at least one SBM for at least nine of 12 weeks and for at least three of the � nal four weeks. The response rate was higher with the 25 mg dose (40% and 44% for the two trials) versus placebo (29.4%). Naloxegol 12.5 mg daily was signi� cantly greater in only one of the studies with a response of 40.8% (P < 0.05); whereas the study with a re-sponse of 34.9% did not show statistical signi� cance compared to placebo.
Alvimopan, another PAMORA agent, is FDA approved to accelerate the time to upper and lower gastrointestinal recovery following partial large or small bowel resec-tion surgery with primary anastomosis. It is not FDA approved for the treatment of OIC because of the high incidence of myo-cardial infarction with this agent in trials of patients receiving opioids for noncancer pain.28
Is there a role for linaclotide, lubiprostone, naloxegol, or methylnaltrexone to prevent the development of
constipation?
PAUSE AND PONDER

DRUGTOPICS.COM | MAY 2016 | DrugTopics 53
CONTINUING EDUCATION
KEEP YOUR PATIENTS “MOVING”
Side effects and administration considerations for new agents for the treatment of constipationLinaclotide. Linaclotide has minimal sys-temic exposure after oral administration. It is rapidly converted in the small intestine to a metabolite that has a half-life of 10 minutes, and 3% to 5% of the oral dose is excreted in the feces. This agent has dem-onstrated an antinociceptive or analgesic ef-fect in various animal models of pain, which may translate to improvements in abdomi-nal pain symptoms in patients with IBS-C. Among side effects occurring within the � rst four weeks of treatment initiation, diarrhea was the most frequently reported in phase 3 clinical trials (14.2% to 19.7% compared to 2.5% to 5% with placebo). Other side effects included abdominal pain and distention, � atulence, and headache. Linaclotide has a boxed warning regarding its use in pediatric patients aged six to 17 years because of observed cases of dehydration and death in young juvenile mice. This agent is also contraindicated in children aged less than six years and in patients with mechanical gastrointestinal obstruction. Lina-clotide has a category C rating for pregnancy. It is not expected to enter breast milk, and renal and hepatic impairment does not affect dosing because of minimal systemic absorption. Lina-clotide should be taken 30 minutes before the � rst meal of the day, as the presence of food may result in looser stools. There are no drug interactions with linaclotide.18
Lubiprostone. Nausea was the most common adverse event seen in patients treated with lubiprostone in phase 3 trials (32%). Other gastrointestinal symptoms in-cluded diarrhea (11%), abdominal distention (6%), abdominal pain (5%), and � atulence (4%). Administration of lubiprostone with a meal may reduce the risk of nausea. Me-chanical gastrointestinal obstruction is the only contraindication to lubiprostone treat-ment. Even though this agent is similar to a prostaglandin analog that is considered to be an abortifacient, lubiprostone has a category C pregnancy rating because it has limited systemic exposure. Breastfeeding women should use lubiprostone with caution, and infants of breastfeeding mothers should be monitored for the occurrence of diarrhea. Lu-biprostone is metabolized by the cytochrome P450 system, but drug interaction is unlikely
because of its minimal systemic absorption. Methadone decreases ClC-2 activation and may reduce the efficacy of lubiprostone; therefore, lubiprostone should not be used in patients with OIC from methadone. Dose adjustment is recommended for patients with moderate or severe hepatic impairment (Child-Pugh class B or C) but not for patients with renal impairment.18,29
MNTX. This agent is a weak CYP2D6 inhibitor with no significant drug interac-tions. Abdominal pain (17%), flatulence (13%), vomiting (13%), nausea (11%), dizzi-ness (8%), and diarrhea (6%) are the most common side effects with MNTX in phase 3 clinical trials.25,26 MNTX is contraindicated in patients with bowel obstruction, diarrhea, or acute abdominal conditions. This agent does not cross the blood-brain barrier and has not been observed to reverse analgesia or cause symptoms of opioid withdrawal. The recom-mended dose is 8 mg in patients weighing 38 to 61 kg and 12 mg in patients weighing 62 to 114 kg; a dose of 0.15 mg/kg should be used for patients outside of these weight ranges. After one dose of MNTX, a bowel movement occurs within four hours in 50% to 60% of patients. The dose may be given every other day if no therapeutic effect is observed with the � rst dose. No dose ad-justment is required in patients with mild to moderate hepatic impairment, but the dose should be reduced by 50% in patients with creatinine clearance <30 mL/min. MNTX is not recommended for patients with end-stage renal impairment requiring dialysis or for those with severe hepatic impairment.29
Naloxegol. Abdominal pain (8.5% - 10%) and diarrhea (3.3% - 9.3%) were common in phase 3 trials of naloxegol.4 Opioid with-drawal occurred in less than 5% of patients in all studied groups and was comparable to the rates of withdrawal seen with placebo or usual care. For OIC caused by methadone, this agent is preferred over lubiprostone. Naloxegol 25 mg should be taken one hour before or two hours after the � rst meal of the day. The dose may be reduced to 12.5 mg if the 25-mg dose is not tolerated. Patients with creatinine clearance <60 mL/min and those who require treatment with moderate CYP3A4 inhibitors should begin naloxegol treatment at 12.5 mg and increase to 25 mg
as tolerated. This agent is contraindicated in patients being treated with a strong CYP3A4 inhibitor.30
Stepwise approach to treating CIC, IBS-C, and OIC Pharmacists must understand the possible causes and underlying mechanisms of consti-pation symptoms to determine the appropriate treatment approach and recommendation. Or-ganic causes of secondary constipation such as colorectal cancer are managed by treating the underlying disease. The pharmacist should assess the patient for “red � ags” that raise suspicion of an underlying organic disease. The patients should be asked the following ques-tions: have you had a sudden change in bowel habits, do you have a family history of colon cancer, do you see blood in your stool or blood from your rectum after a bowel movement, do you have recent unexplained weight loss, do you have a fever, vomiting, rectal or abdomi-nal pain? If the patient answers yes to any of these questions, he or she should be referred to a physician for further work-up and evalua-tion.6 The patient should also be asked how long he or she had the constipation symptoms, if the patient experiences straining, sensation of incomplete evacuation, or the need for digi-tal removal of the stool. If the patient had the symptoms for more than 7 days or answers yes to these questions, he or she should also be referred to a physician. The pharmacist can introduce the patient to the BSFS at this point to help the patient describe the stool form and ease of stool passage. Drug-induced constipa-tion is another major cause of constipation; therefore, the pharmacist should review the patient’s medication history. If the pharmacist identi� es that the patient is on a drug or drugs that can cause constipation, the pharmacist can provide this list of constipating drugs to the patient to provide to his/her physician. The pharmacist should inform the patient that the physician may consider discontinuation of the offending agent if it is safe for the patient or another agent with fewer or no constipating ef-fects may be substituted. The pharmacist can also request the patient to complete the BFI at the time of opioid initiation and/or at the time of assessment of constipation to estab-lish the patient’s baseline bowel function and, in cases of opioid treatment, ensure that the

54 DrugTopics | MAY 2016 | DRUGTOPICS.COM
CONTINUING EDUCATION
AN OVERVIEW OF TREATMENT OPTIONS FOR CONSTIPATION
patient does not have underlying constipation. For patients with OIC, before resorting to ag-gressive pharmacologic therapy, clinicians and pharmacists specializing in pain treatment should evaluate whether it is possible to:• reduce the dose of the opioid without com-promising pain control,• consider adding adjuvant analgesics to allow for reduction of the opioid dose,• explore the possibility of opioid rotation (switching to another opioid) to treat constipa-tion.
When a defecation disorder, organic or drug-induced causes of constipation have been ruled out, the next step is to consider options for treating the constipation. The pri-mary goal in treating constipation is symptom improvement, and the secondary goal is for the patient to be able to pass soft, formed stool without straining at least three times per week. For patients with CIC, increasing the frequency of SBM and CSBM is desir-able. For IBS-C, reducing symptoms of ab-dominal pain is a major goal in addition to improving constipation symptoms.18 Preven-tion of constipation is the key in managing OIC. Pharmacists can counsel patients to promptly respond to the urge to defecate to minimize the amount of time that the stool is retained in the bowel; this will prevent water resorption, which can make the stool hard and difficult to pass.31 Advise the patient to provide a consistent time for defecation based on his or her everyday living demands. The urge for defecation is strongest for about 15 minutes in the � rst hour after a meal; therefore, the best time to toilet is 30 to 40 minutes after a meal.6
The initial, conservative treatment of con-stipation is a nonpharmacologic approach that includes a high-� ber diet, increased � uid intake, and physical activity. This approach is safe and well tolerated in most patients, making this a reasonable � rst-line approach for therapy. It should be noted that in the ab-sence of dehydration, increased � uid intake is unlikely to relieve constipation.32
Fiber supplementation bene� ts both CIC and IBS-C.8 The soluble � ber psyllium pro-vides symptom relief, whereas bran does not, in patients with IBS-C.8 Psyllium has also been associated with improvements in straining, pain on defecation, and number
of stools per week compared with placebo in patients with CIC.33 The ef� cacy of � ber has not been demonstrated in patients with OIC. However, � ber is inexpensive, nontoxic, and readily available, making it worthwhile to attempt a brief trial period with � ber de-spite the lack of data for its ef� cacy in these patients, with the caveat that it may not be as effective and can worsen the problem for patients with slow-transit constipation.32
Educating patients to distinguish between soluble and insoluble � bers is useful, as sol-uble � ber causes less cramping and bloating and is more effective than insoluble � ber for constipation. Soluble � ber is found in barley, � ax, oats, certain fruits and vegetables, and supplements such as psyllium, methylcellu-lose, and calcium polycarbophil. Examples of foods containing insoluble � ber include wheat bran, whole grains, corn � ber, skin on fruits and vegetables, seeds, and nuts.33
Fiber requires adequate water intake to be effective; otherwise, constipation symptoms can be exacerbated. A gradual increase of � ber supplement intake every seven to 10 days up to three times daily is recommended to minimize bloating. Patients should also be counseled that response will not be im-mediate and so they should remain on the regimen for several weeks before declaring therapy failure.
If patients do not respond to the con-servative, nonpharmacologic approach after several months of therapy, it is reasonable to initiate treatment with an osmotic laxative and/or a stimulant as the next step.6 The American College of Gastroenterology con-ducted a series of systematic reviews of ther-apy in IBS and CIC and found no evidence for the ef� cacy of osmotic or stimulant laxatives for the treatment of IBS-C.8 The group did strongly recommend using polyethylene gly-col (PEG), lactulose, and bisacodyl in patients with CIC, as these agents have been shown to be effective in improving symptoms from CIC even though the quality of evidence was low for lactulose and moderate for bisacodyl
(but high for PEG).8 The American Gastroen-terological Association Technical Review in Constipation recommended the use of PEG over lactulose because a Cochrane Data-base review of 10 randomized trials compar-ing PEG and lactulose found that PEG was superior for improving stool frequency, stool consistency, and abdominal pain.34 Further-more, lactulose requires a prescription and may cause more bloating and cramping than PEG. The American Gastroenterological Asso-ciation also prefers PEG over stimulant laxa-tives because of more evidence of short- and long-term ef� cacy for osmotic agents. Thus, the � nal recommendation is that an osmotic agent may be used regularly for CIC, with PEG being the preferred product, and a stimulant laxative may be used as a rescue or add-on agent if PEG is not effective.34
Consensus statements for OIC and clini-cal guidelines for the use of opioids in chron-ic cancer or noncancer pain all recommend the use of nonpharmacologic conservative therapy and conventional laxatives for the prophylaxis and management of OIC, even though there is little evidence to support the ef� cacy of these treatment approaches. The National Comprehensive Cancer Network recommends the use of sennoside (laxative) with or without a stool softener or PEG while the patient maintains adequate intake of � uids and dietary � ber. The administration of docusate (stool softener) is optional be-cause one study showed that the addition of docusate to the sennoside laxative was less effective than sennoside administered alone.35,36 Laxatives should be titrated to achieve one nonforced bowel movement ev-ery one to two days.35
When conventional laxatives are not ef-fective for treating constipation, after several months of trial period,6 the use of prescrip-tion agents such as lubiprostone and lina-clotide is indicated for IBS-C and CIC. There is a strong recommendation from the Ameri-can College of Gastroenterology for the use of linaclotide and lubiprostone for IBS and
Is there a role for over-the-counter laxatives for the treatment of IBS-C or CIC?
PAUSE AND PONDER
DRUGTOPICS.COM | MAY 2016 | DrugTopics 55
CONTINUING EDUCATION
KEEP YOUR PATIENTS “MOVING”
CIC based on high and moderate quality of evidence.8 However, linaclotide and lubipros-tone were evaluated versus placebo; no com-parative studies between the two agents or between these agents and the standard, con-ventional treatment have been performed, making it dif� cult to determine the place of each agent in the treatment algorithm for CIC and IBS-C. The American Gastroenterologi-
cal Association states that for patients with IBS-C who place a high value on avoiding diarrhea or the high out-of-pocket expenses associated with linaclotide, an alternative agent to linaclotide should be considered. For patients who wish to avoid nausea or the high out-of-pocket expenses associated with lubiprostone, an alternative agent to lubipro-stone should be considered.37
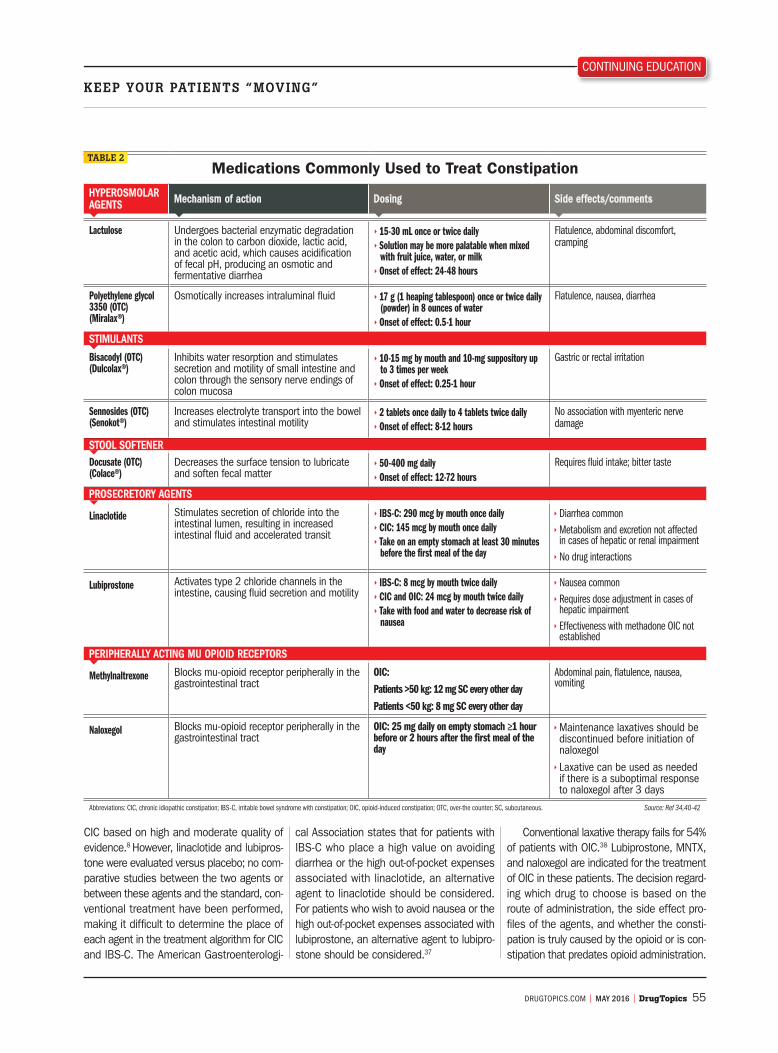
Conventional laxative therapy fails for 54% of patients with OIC.38 Lubiprostone, MNTX, and naloxegol are indicated for the treatment of OIC in these patients. The decision regard-ing which drug to choose is based on the route of administration, the side effect pro-� les of the agents, and whether the consti-pation is truly caused by the opioid or is con-stipation that predates opioid administration.
Medications Commonly Used to Treat ConstipationHYPEROSMOLAR AGENTS Mechanism of action Dosing Side effects/comments
Lactulose Undergoes bacterial enzymatic degradation in the colon to carbon dioxide, lactic acid, and acetic acid, which causes acidi� cation of fecal pH, producing an osmotic and fermentative diarrhea
15-30 mL once or twice daily Solution may be more palatable when mixed
with fruit juice, water, or milk Onset of effect: 24-48 hours
Flatulence, abdominal discomfort, cramping
Polyethylene glycol 3350 (OTC)(Miralax®)
Osmotically increases intraluminal � uid 17 g (1 heaping tablespoon) once or twice daily (powder) in 8 ounces of water Onset of effect: 0.5-1 hour
Flatulence, nausea, diarrhea
STIMULANTS
Bisacodyl (OTC)(Dulcolax®)
Inhibits water resorption and stimulates secretion and motility of small intestine and colon through the sensory nerve endings of colon mucosa
10-15 mg by mouth and 10-mg suppository up to 3 times per week Onset of effect: 0.25-1 hour
Gastric or rectal irritation
Sennosides (OTC)(Senokot®)
Increases electrolyte transport into the bowel and stimulates intestinal motility
2 tablets once daily to 4 tablets twice daily Onset of effect: 8-12 hours
No association with myenteric nerve damage
STOOL SOFTENERDocusate (OTC)(Colace®)
Decreases the surface tension to lubricate and soften fecal matter
50-400 mg daily Onset of effect: 12-72 hours
Requires � uid intake; bitter taste
PROSECRETORY AGENTS
Linaclotide Stimulates secretion of chloride into the intestinal lumen, resulting in increased intestinal � uid and accelerated transit
IBS-C: 290 mcg by mouth once daily CIC: 145 mcg by mouth once daily Take on an empty stomach at least 30 minutes
before the � rst meal of the day
Diarrhea common Metabolism and excretion not affected in cases of hepatic or renal impairment No drug interactions
Lubiprostone Activates type 2 chloride channels in the intestine, causing � uid secretion and motility
IBS-C: 8 mcg by mouth twice daily CIC and OIC: 24 mcg by mouth twice daily Take with food and water to decrease risk of
nausea
Nausea common Requires dose adjustment in cases of hepatic impairment Effectiveness with methadone OIC not established
PERIPHERALLY ACTING MU OPIOID RECEPTORS
Methylnaltrexone Blocks mu-opioid receptor peripherally in the gastrointestinal tract
OIC:
Patients >50 kg: 12 mg SC every other day
Patients <50 kg: 8 mg SC every other day
Abdominal pain, � atulence, nausea, vomiting
Naloxegol Blocks mu-opioid receptor peripherally in the gastrointestinal tract
OIC: 25 mg daily on empty stomach ≥1 hour before or 2 hours after the � rst meal of the day
Maintenance laxatives should be discontinued before initiation of naloxegol Laxative can be used as needed if there is a suboptimal response to naloxegol after 3 days
Abbreviations: CIC, chronic idiopathic constipation; IBS-C, irritable bowel syndrome with constipation; OIC, opioid-induced constipation; OTC, over-the counter; SC, subcutaneous. Source: Ref 34,40-42
TABLE 2

56 DrugTopics | MAY 2016 | DRUGTOPICS.COM
CONTINUING EDUCATION
AN OVERVIEW OF TREATMENT OPTIONS FOR CONSTIPATION
Lubiprostone is safer in patients with renal impairment or receiving therapy with a moderate or strong CYP3A4 inhibitor. Naloxegol is safer in patients with hepatic impairment. If opioid use is the most likely cause of constipation, MNTX or naloxegol is indicated as � rst-line therapy when contrain-dications are ruled out.39 Naloxegol may be preferred over MNTX because it is available for oral administration, and most patients may not want to self-inject with subcutane-ous MNTX. If the PAMORA does not relieve constipation after a signi� cant amount of time (1 to 2 months of therapy), lubipros-tone may be tried next. On the other hand, if opioid use is ruled out as the cause for constipation in a patient who is taking opi-oids for pain management, then lubiprostone may be preferred as � rst-line therapy after failure of conventional laxatives. If a patient already had signs and symptoms of consti-pation prior to initiation of the opioid, it is reasonable to assume that the opioid may not necessarily be the cause of the consti-pation. Lubiprostone may not be effective in a patient with OIC caused by methadone; therefore, naloxegol or MNTX should be used in these patients. According to the multidisciplinary panel of 10 experts with extensive knowledge of opioid-associated adverse events who developed consensus recommendations on OIC assessment for
the American Academy of Pain Medicine, the use of a PAMORA or lubiprostone is recom-mended in patients with BFI scores of ≥30 points and an inadequate response to � rst-line interventions.13 When lubiprostone or a PAMORA is initiated, preexisting scheduled and as-needed laxatives should be discontin-
ued and then resumed in a stepwise fashion if OIC persists after three days of treatment with lubiprostone or the PAMORA.30
Table 2 provides detailed information on the mechanisms of action, indications, dos-ing, and clinical considerations for the agents most commonly used to treat constipa-tion.34,40-42 Table 3 summarizes the strengths of recommendation for the treatment of CIC and IBS-C and the quality of evidence for recommendations by the American College of Gastroenterology.8
Take-home messageConstipation is a common complaint that prompts individuals to seek medical care from primary care providers, gastroenterolo-
gists, and other healthcare providers such as pharmacists. The treatment of constipation is multifaceted and requires the implementation of multiple strategies both concurrently and in a stepwise algorithmic approach. Pharma-cists can play an integral role in helping pa-tients with constipation by promoting lifestyle
changes; counseling on the use of convention-al and novel laxative products; and providing information on side effects, drug interactions, and when to expect a response to therapy. Pharmacists may also educate patients on how to recognize the signs and symptoms of constipation through the use of the BSFS and should remind patients to allow enough time for the laxative to work before declaring it ineffective. Most signi� cantly, pharmacists can perform a comprehensive medication review with patients and provide documenta-tion for drugs that may cause constipation; patients can share this information with their primary care provider to instigate con-sideration of changing to an alternative drug that does not cause constipation. Pharmacy technicians may facilitate the management of constipation by ensuring that the appropriate prescription drug with the appropriate dose is prescribed for patients with CIC, IBS-C, or OIC when reviewing the prescription pre-sented by a patient. If the technician notices a signi� cant discrepancy with the dose or the speci� c agent for type of constipation, the pharmacist should be alerted so that he or she can contact the prescriber to clarify the prescription. The pharmacy technicians may also refer patients to the pharmacist for con-stipation counseling if they notice patients are purchasing over-the-counter laxatives such as polyethylene glycol (Miralax®), sennosides (Senokot®), bisacodyl (Dulcolax®), docusate so-dium (Colace®), or sennosides plus docusate (Senkot-S®, Peri-Colace®).
REFERENCES are available online at www.drugtopics.com/cpe. •
American College of Gastroenterology Recommendationsand Quality of Evidence for IBS-C and CIC Therapy
Statement for IBS-C/CIC Recommendation/quality of evidence for IBS-C
Recommendation/quality of evidence for CIC
Fiber provides overall symptom relief in IBS-C/Fiber increases stool frequency in CIC Weak/Moderate Strong/Low
No evidence that polyethylene glycol improves overall symptoms and pain in patients with IBS/Polyethylene glycol increases stool frequency and consistency in CIC
Weak/Low Strong/High
NA/Lactulose increases stool frequency and consistency in CIC NA/NA Strong/Low
NA/Bisacodyl is effective in CIC NA/NA Strong/Moderate
Linaclotide is superior to placebo for IBS-C/Linaclotide is effective in CIC Strong/High Strong/High
Lubiprostone is superior to placebo for IBS-C/Lubiprostone is effective in CIC Strong/Moderate Strong/High
Abbreviations: CIC, chronic idiopathic constipation; IBS-C, irritable bowel syndrome with constipation; NA, not applicable. Source: Ref 8
TABLE 3
When should the discussion of bowel function be initiated for a patient who is prescribed an opioid for
pain management?
PAUSE AND PONDER
DRUGTOPICS.COM | MAY 2016 | DrugTopics 57
CONTINUING EDUCATION
TEST QUESTIONS
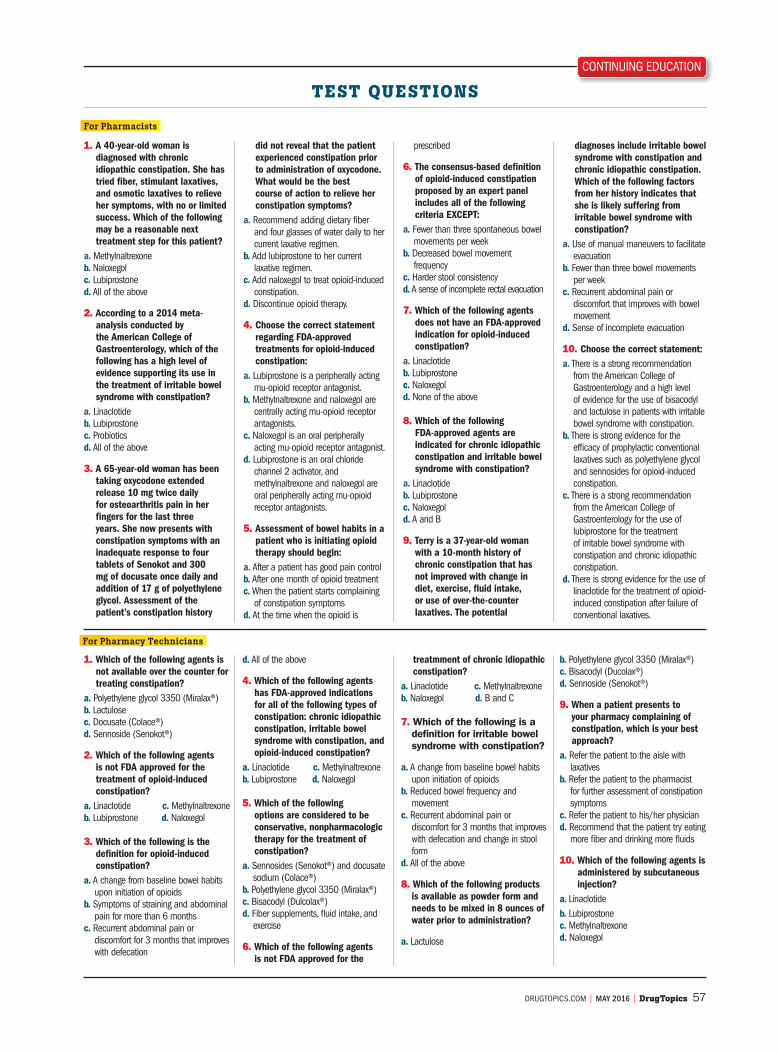
1. A 40-year-old woman is diagnosed with chronic idiopathic constipation. She has tried � ber, stimulant laxatives, and osmotic laxatives to relieve her symptoms, with no or limited success. Which of the following may be a reasonable next treatment step for this patient?
a. Methylnaltrexoneb. Naloxegolc. Lubiprostoned. All of the above
2. According to a 2014 meta-analysis conducted by the American College of Gastroenterology, which of the following has a high level of evidence supporting its use in the treatment of irritable bowel syndrome with constipation?
a. Linaclotideb. Lubiprostonec. Probioticsd. All of the above
3. A 65-year-old woman has been taking oxycodone extended release 10 mg twice daily for osteoarthritis pain in her � ngers for the last three years. She now presents with constipation symptoms with an inadequate response to four tablets of Senokot and 300 mg of docusate once daily and addition of 17 g of polyethylene glycol. Assessment of the patient’s constipation history
did not reveal that the patient experienced constipation prior to administration of oxycodone. What would be the best course of action to relieve her constipation symptoms?
a. Recommend adding dietary � ber and four glasses of water daily to her current laxative regimen.
b. Add lubiprostone to her current laxative regimen.
c. Add naloxegol to treat opioid-induced constipation.
d. Discontinue opioid therapy.
4. Choose the correct statement regarding FDA-approved treatments for opioid-induced constipation:
a. Lubiprostone is a peripherally acting mu-opioid receptor antagonist.
b. Methylnaltrexone and naloxegol are centrally acting mu-opioid receptor antagonists.
c. Naloxegol is an oral peripherally acting mu-opioid receptor antagonist.
d. Lubiprostone is an oral chloride channel 2 activator, and methylnaltrexone and naloxegol are oral peripherally acting mu-opioid receptor antagonists.
5. Assessment of bowel habits in a patient who is initiating opioid therapy should begin:
a. After a patient has good pain controlb. After one month of opioid treatmentc. When the patient starts complaining
of constipation symptomsd. At the time when the opioid is
prescribed
6. The consensus-based de� nition of opioid-induced constipation proposed by an expert panel includes all of the following criteria EXCEPT:
a. Fewer than three spontaneous bowel movements per week
b. Decreased bowel movement frequency
c. Harder stool consistencyd. A sense of incomplete rectal evacuation
7. Which of the following agents does not have an FDA-approved indication for opioid-induced constipation?
a. Linaclotideb. Lubiprostonec. Naloxegold. None of the above
8. Which of the following FDA-approved agents are indicated for chronic idiopathic constipation and irritable bowel syndrome with constipation?
a. Linaclotideb. Lubiprostonec. Naloxegold. A and B
9. Terry is a 37-year-old woman with a 10-month history of chronic constipation that has not improved with change in diet, exercise, � uid intake, or use of over-the-counter laxatives. The potential
diagnoses include irritable bowel syndrome with constipation and chronic idiopathic constipation. Which of the following factors from her history indicates that she is likely suffering from irritable bowel syndrome with constipation?
a. Use of manual maneuvers to facilitate evacuation
b. Fewer than three bowel movements per week
c. Recurrent abdominal pain or discomfort that improves with bowel movement
d. Sense of incomplete evacuation
10. Choose the correct statement:a. There is a strong recommendation
from the American College of Gastroenterology and a high level of evidence for the use of bisacodyl and lactulose in patients with irritable bowel syndrome with constipation.
b. There is strong evidence for the ef� cacy of prophylactic conventional laxatives such as polyethylene glycol and sennosides for opioid-induced constipation.
c. There is a strong recommendation from the American College of Gastroenterology for the use of lubiprostone for the treatment of irritable bowel syndrome with constipation and chronic idiopathic constipation.
d. There is strong evidence for the use of linaclotide for the treatment of opioid-induced constipation after failure of conventional laxatives.
1. Which of the following agents is not available over the counter for treating constipation?
a. Polyethylene glycol 3350 (Miralax®)b. Lactulosec. Docusate (Colace®)d. Sennoside (Senokot®)
2. Which of the following agents is not FDA approved for the treatment of opioid-induced constipation?
a. Linaclotide c. Methylnaltrexoneb. Lubiprostone d. Naloxegol
3. Which of the following is the de� nition for opioid-induced constipation?
a. A change from baseline bowel habits upon initiation of opioids
b. Symptoms of straining and abdominal pain for more than 6 months
c. Recurrent abdominal pain or discomfort for 3 months that improves with defecation
d. All of the above
4. Which of the following agents has FDA-approved indications for all of the following types of constipation: chronic idiopathic constipation, irritable bowel syndrome with constipation, and opioid-induced constipation?
a. Linaclotide c. Methylnaltrexone b. Lubiprostone d. Naloxegol
5. Which of the following options are considered to be conservative, nonpharmacologic therapy for the treatment of constipation?
a. Sennosides (Senokot®) and docusate sodium (Colace®)
b. Polyethylene glycol 3350 (Miralax®)c. Bisacodyl (Dulcolax®)d. Fiber supplements, � uid intake, and
exercise
6. Which of the following agents is not FDA approved for the
treatmment of chronic idiopathic constipation?
a. Linaclotide c. Methylnaltrexoneb. Naloxegol d. B and C
7. Which of the following is a de� nition for irritable bowel syndrome with constipation?
a. A change from baseline bowel habits upon initiation of opioids
b. Reduced bowel frequency and movement
c. Recurrent abdominal pain or discomfort for 3 months that improves with defecation and change in stool form
d. All of the above
8. Which of the following products is available as powder form and needs to be mixed in 8 ounces of water prior to administration?
a. Lactulose
b. Polyethylene glycol 3350 (Miralax®)c. Bisacodyl (Ducolax®)d. Sennoside (Senokot®)
9. When a patient presents to your pharmacy complaining of constipation, which is your best approach?
a. Refer the patient to the aisle with laxatives
b. Refer the patient to the pharmacist for further assessment of constipation symptoms
c. Refer the patient to his/her physiciand. Recommend that the patient try eating
more � ber and drinking more � uids
10. Which of the following agents is administered by subcutaneous injection?
a. Linaclotideb. Lubiprostonec. Methylnaltrexoned. Naloxegol
For Pharmacy Technicians
For Pharmacists

CONTINUING EDUCATION
A REVIEW OF NEW TREATMENT OPTIONS FOR CONSTIPATION
1. Sanchez MI, Bercik P. Epidemiology and burden of chronic constipation. Can J Gastroenterol. 2011;25 Suppl B:11B-15B.
2. Higgins PD, Johanson JF. Epidemiology of constipation in North America: a systematic review. Am J Gastro-enterol. 2004;99:750-759.
3. Saito YA, Schoenfeld P, Locke GR 3rd. The epidemiology of irritable bowel syndrome in North America: a sys-tematic review. Am J Gastroenterol. 2002;97:1910-1915.
4. Chey WD, Webster L, Sostek M, Lappalainen J, Barker PN, Tack J. Naloxegol for opioid-induced constipa-tion in patients with noncancer pain. N Engl J Med. 2014;370:2387-2396.
5. Nelson AD, Camilleri M. Opioid-induced constipation: advances and clinical guidance. Ther Adv Chronic Dis. 2016;7:121-134.
6. Bassotti G, Villanacci V. A practical approach to diag-nosis and management of functional constipation in adults. Intern Emerg Med. 2013;8:275-282.
7. Gaertner J, Siemens W, Camilleri M, et al. De� nitions and outcome measures of clinical trials regarding opi-oid-induced constipation: a systematic review. J Clin Gastroenterol. 2015;49:9-16.
8. Ford C, Moayyedi P, Lacy BE, et al; Task Force on the Management of Functional Bowel Disorders. American College of Gastroenterology monograph on the man-agement of irritable bowel syndrome and chronic idio-pathic constipation. Am J Gastroenterol. 2014;109 Suppl 1:S2-S26.
9. Heidelbaugh JJ, Stelwagon M, Miller SA, Shea EP, Chey WD. The spectrum of constipation-predominant irritable bowel syndrome and chronic idiopathic constipation: US survey assessing symptoms, care seeking, and dis-ease burden. Am J Gastroenterol. 2015;110:580-587.
10. Halder SLS, Locke III GR, Schleck CD, et al. Natural his-tory of functional gastrointestinal disorders: A 12-year longitudinal population-based study. Gastroenterol. 2007;133:799-807.
11. Lewis SJ, Heaton JW. Stool form scale as a useful guide to intestinal transit time. Scand J Gastroenterol. 1997;32:920-924.
12. Rentz AM, Yu R, Muller-Lissner S, Leyendecker P. Vali-dation of the Bowel Function Index to detect clinically meaningful changes in opioid-induced constipation. J Med Econ. 2009;12:371-383.
13. Argoff CE, Brennan MJ, Camilleri M, et al. Consensus Recommendations on Initiating Prescription Thera-pies for Opioid-Induced Constipation. Pain Med. 2015;16:2324-2337.
14. Vazquez-Roque MI, Bouras EP. Linaclotide, novel therapy for the treatment of chronic idiopathic consti-pation and constipation-predominant irritable bowel syndrome. Adv Ther. 2013;30:203-211.
15. Lembo A, Schneier HA, Shiff SJ, et al. Two randomized trials of linaclotide for chronic constipation. N Engl J Med. 2011;365:527-536.
16. Chey WD, Lembo AJ, Lavins BJ, et al. Linaclotide for irritable bowel syndrome with constipation: a 26-week, randomized, double-blind, placebo-controlled trial to evaluate ef� cacy and safety. Am J Gastroenterol. 2012;107:1702-1712.
17. Rao S, Lembo AJ, Shiff SJ, et al. A 12-week, random-ized, controlled trial with a 4-week randomized with-drawal period to evaluate the ef� cacy and safety of linaclotide in irritable bowel syndrome with constipa-tion. Am J Gastroenterol. 2012;107:1714-1724.
18. Thomas RH, Luthin DR. Current and emerging treat-ments for irritable bowel syndrome with constipation and chronic idiopathic constipation: focus on prosecre-tory agents. Pharmacotherapy. 2015;35:613-630.
19. Johanson JF, Morton D, Geenen J, Ueno, R. Multicenter, 4-week, double-blind, randomized, placebo-controlled trial of lubiprostone, a locally-acting type-2 chloride channel activator, in patients with chronic constipation. Am J Gastroenterol. 2008;103:170-177.
20. Barish CF, Drossman D, Johanson JF, Ueno R. Ef� cacy and safety of lubiprostone in patients with chronic con-stipation. Dig Dis Sci. 2010;55:1090-1097.
21. Drossman DA, Chey WD, Johanson JF, et al. Clinical trial: lubiprostone in patients with constipation-associ-ated irritable bowel syndrome - results of two random-ized, placebo-controlled studies. Aliment Pharmacol Ther. 2009;29:329-341.
22. Chey WD, Drossman DA, Johanson JF, et al. Safety and patient outcomes with lubiprostone for up to 52 weeks in patients with irritable bowel syndrome with constipa-tion. Aliment Pharmacol Ther. 2012;35:587-599.
23. Cryer B, Katz S, Vallejo R, Popescu A, Ueno R. A ran-domized study of lubiprostone for opioid-induced con-stipation in patients with chronic noncancer pain. Pain Med. 2014;15:1825-1834.
24. Jamal MM, Adams AB, Jansen JP, Webster LR. A ran-domized, placebo-controlled trial of lubiprostone for opioid-induced constipation in chronic noncancer pain. Am J Gastroenterol. 2015;110:725-732.
25. Thomas J, Karver S, Cooney GA, et al. Methylnaltrexone for opioid-induced constipation in advanced illness. N Engl J Med. 2008;358:2332-2343.
26. Slatkin N, Thomas J, Lipman AG, et al. Methylnaltrex-one for treatment of opioid-induced constipation in ad-vanced illness patients. J Supp Oncol. 2009;1:39-46.
27. Michna E, Blonsky ER, Schulman S, et al. Subcutane-ous methylnaltrexone for treatment of opioid-induced constipation in patients with chronic, nonmalignant pain: a randomized controlled study. J Pain. 2011; 12:554–562.
28. Weber HC. Opioid-induced constipation in chronic non-cancer pain. Curr Opin Endocrinol Diabetes Obes.
2016;23:11-17.
29. Leppert W. Emerging therapies for patients with symp-toms of opioid-induced bowel dysfunction. Drug Des Devel Ther. 2015;9:2215-2231.
30. Holder RM, Rhee D. Novel oral therapies for opioid-induced bowel dysfunction in patients with chronic non-cancer pain. Pharmacotherapy. 2016;36:287-299.
31. McCarberg BH. Overview and treatment of opioid-induced constipation. Postgrad Med. 2013;125:7-17.
32. Dorn S, Lembo A, Cremonini F. Opioid-induced bowel dysfunction: epidemiology, pathophysiology, diagnosis, and initial therapeutic approach. Am J Gastroenterol. 2014;2:31-37.
33. Shah BJ, Rughwani N, Rose S. In the clinic: constipa-tion. Ann Intern Med. 2015;162:ITC1. doi:10.7326/AITC201504070
34. Bharucha AE, Pemberton JH, Locke GR 3rd. American Gastroenterological Association technical review on constipation. Gastroenterology. 2013;144:218-238.
35. NCCN clinical practice guidelines in oncology: adult cancer pain. National Comprehensive Cancer Net-work Website. http://www.nccn.org/professionals/physician_gls/pdf/pain.pdf. Updated 2016. Accessed March 20, 2016.
36. Hawley PH, Byeon JJ. A comparison of sennosides-based bowel protocols with and without docusate in hospitalized patients with cancer. J Palliat Med. 2008;11:575-581.
37. Weinberg DS, Smalley W, Heidelbaugh JJ, Sultan S; American Gastroenterological Association. American Gastroenterological Association Institute Guideline on the pharmacological management of irritable bowel syndrome. Gastoenterology. 2014;147:1146-1148.
38. Pappagallo M. Incidence, prevalence, and man-agement of opioid bowel dysfunction. Am J Surg. 2001;182:11S-18S.
39. Wald A. Constipation: advances in diagnosis and treat-ment. JAMA. 2016;315:185-191.
40. Andromanakos NP, Pinis SI, Kostakis AI. Chronic severe constipation: current pathophysiological aspects, new diagnostic approaches, and therapeutic options. Eur J Gastroenterol Hepatol. 2015;27:204-214.
41. Gyawali B, Hayashi N, Tsukuura H, Honda K, Shimokata T, Ando Y. Opioid-induced constipation. Scand J Gas-troenterol. 2015;50:1331-1338.
42. Eoff JC. Optimal treatment of chronic constipation in managed care: review and roundtable discussion. J Manag Care Pharm. 2008;14:1-15.
References