keeping people with a learning disability healthy …...the learning disabilities mortality review...
TRANSCRIPT

P a g e | 1
Keeping People with a Learning Disability Healthy
How Findings from the Learning Disability Review of Mortality (LeDeR) are Influencing the Reduction of
Health Inequalities in Hertfordshire
Annual Report 2018/19
Prepared by: Tracey Brennan, On behalf of: The Hertfordshire LeDeR Steering Group.

P a g e | 2
Contents:
Page number Foreword 3 Chapter 1: Local Context 4 Chapter 2: The LeDeR process in Hertfordshire 7 Chapter 3: Findings from the Hertfordshire LeDeR Programme 11 Chapter 4: Learning into Action (Improving Health Outcomes) 17 Chapter 5: Actions and Recommendations 31 Chapter 6: Conclusion 36 Appendices: Glossary of terms Acknowledgements Links to resources and further reading Case study – End of Life

P a g e | 3
Foreword Dr Kirsten Lamb, Chair of the Hertfordshire LeDeR Programme Steering Group “As a recently retired GP and Clinical Lead for Learning Disability for Herts Valley CCG, I am very privileged to be able to continue to chair the Hertfordshire LeDeR steering group. The driving motivation behind our Steering Group is to develop learning from the reviews of deaths presented to us. Then from this learning, we aim to develop robust and evidence-based changes to service delivery to improve outcomes for our Hertfordshire population of people with a learning disability. Our group has representation from across the health and social care system in Herts but most importantly from a family member and a person with a learning disability. The impact that we are having will be carefully reviewed. Our work will also form part of the action plan for the Hertfordshire Learning Disability Strategy ‘The Big Plan’. As a group we welcome feedback from local people and their representatives and those working in the health and social care sectors in Hertfordshire”. Marie Scales, Parent-Carer representative on Hertfordshire LeDeR Steering Group “I have been a carer representative since the LeDeR project in Hertfordshire commenced. Initially there was another carer representative as well as myself. I was asked if I would join the steering group because unfortunately my son had died earlier than people who did not have a Learning Disability. For me personally the most important parts of the LeDeR project are showing good and not so good practice and how we can reduce the number of premature deaths of those who have a Learning Disability. Having read the reviews, the cause of death is put into a theme e.g. aspiration pneumonia, pneumonia, we feed this back to the Improving Health Outcomes Group. We have found that the majority of our deaths which have been reviewed fall into the same categories as the national findings. The second most important finding is the lessons learnt from the review. We are finding many of the deaths could not be prevented so as carers what can we do? Firstly, you or I are able to make our choices as to how we would like our end of life to be managed. This appears not to be the case for our relative with a Learning Disability, it is so important for those who have the mental capacity to have been involved in the early stages and not leave it to the end when the individual may no longer be able to make their choice known. Therefore, as carers we should be having a discussion with our relative and everyone who is supporting them, perhaps the result of the discussion could then be recorded at the annual review”. Sam Prowse, Expert by Experience Adviser representative on the Steering Group “I have friends and people who I lived with when I was in supported living who died younger than they should have or who have not had the best treatment. It is 2020 and people with a learning disability are still dying younger than people without a learning disability. Through LeDeR we have been looking at why this is and are taking action to improve the health and quality of people’s lives. With my experience I can give my perspective (on behalf of other people with a learning disability) on how things can improve”.

P a g e | 4
CHAPTER 1 – Background 1.1 National Context People with a learning disability continue to die prematurely and of preventable conditions. The 2019 NHS England Long Term Plan recognises that this needs to be addressed.
Action will be taken to tackle the causes of morbidity and preventable deaths in people with a learning disability
The whole NHS will improve its understanding of the needs of people with learning disabilities and autism, and work together to improve their health and wellbeing
www.longtermplan.nhs.uk/wp-content/uploads/2019/08/nhs-long-term-plan-version-1.2.pdf
1.2 Local Context The population of Hertfordshire is 1,154,800 and continues to increase due to higher life expectancy, a rising birth rate, and inward migration. The health of people in Hertfordshire is generally better than the England average and is one of the 20% least deprived counties/unitary authorities in England, however about 11% (24,800) of children live-in low-income families. Life expectancy in Hertfordshire is improving and is higher than the England average, but varies between men and women and between smaller areas of the county according to levels of deprivation. The principal causes of death in Hertfordshire are: heart disease and stroke, dementia and Alzheimer’s disease, cancers, and respiratory diseases. These conditions are also principal causes of disability and ill health. The Hertfordshire all age Learning Disability JSNA (Joint Strategic Needs Assessment) was written in July 2019 and provides a range of comparative data about the health and well-being of people with a learning disability against the general population in Hertfordshire. www.hertfordshire.gov.uk/microsites/jsna/jsna-documents/learning-disabilities-jsna-2019.pdf Hertfordshire has two clinical commissioning groups, Herts Valleys Clinical Commissioning Group (HVCCG) and East and North Herts Clinical Commissioning Group (ENHCCG). A number of areas deliver the LeDeR programme as part of their STP however, the Hertfordshire LeDeR programme covers the Hertfordshire Transforming Care footprint, i.e. co-terminus with Herts County Council and the 2 Hertfordshire CCGs. In wider discussions around improving the health of people with learning disabilities, links with each of the STP work streams are being made.

P a g e | 5
Each CCG holds a register of the number of all people with a learning disability. This is called the QOF (Quality and Outcomes Framework) Register.
The Learning Disability Quality and Outcomes Framework (QOF) register is a list of patients with learning disabilities that GP practices have to maintain. In Hertfordshire, all GP practices should be signed up to maintain a local QOF register. The prevalence of people with a learning disability is 0.466% of the population in Herts Valley CCG and 0.43% in East and North Herts CCG. (This equates to 5,661 people identified as having a learning disability across Hertfordshire). The objective of the QOF is to improve the quality of care patients are given by rewarding practices for the quality of care they provide to their patients. There are challenges to maintain and increase the Learning Disability QOF register to meet local and national targets. Work is ongoing with early identification of learning disabilities and accurate coding for patients. We are working with paediatricians to ensure they include the diagnosis of learning disabilities in children and young people and recommend that these children be included on the GPQOF register. NHSE have produced guidance on how GP practices can increase the number of people on their Learning Disability QOF register. This guidance has been distributed to all the practices via the CCGs. ‘The Big Plan’ (Hertfordshire Learning Disability Strategy) provides oversight as to the priorities for partners to improve the health and well-being of adults with a learning disability in Hertfordshire. www.hertfordshire.gov.uk/media-library/documents/adult-social-services/learning-disability-partnership-board/the-big-plan-easy-read.pdf To monitor whether improvements are seen by people with a learning disability a questionnaire is sent to 1,000 people with a learning disability (18yrs+) annually. The return rate is approximately 35%. This is analysed and used to inform the action plan for the following year.

P a g e | 6
1.2.1 Children and Young People Data from the 2018 school census (spring term) in Hertfordshire showed that there was a total of 6,099 pupils recorded in the school census as having a moderate, severe or profound and multiple learning difficulty, with 2,451 girls (40.2%) and 3,648 boys (59.8%). Of these pupils, 3,061 (50.2%) were in primary school and 3,038 (49.8%) were in secondary school. Not all these individuals are identified on the QoF register. This could be down to how the term learning disabilities is used and whether people identify themselves as having a learning disability. In 2018, the proportion of children with learning disabilities known to schools in Hertfordshire was 23.03 per 1000. Hertfordshire was statistically significantly lower than England (33.9 per 1000). It is important to note that the register does not only capture children with a learning disability but also those with an autistic spectrum disorder. The numbers of adults (25yrs+) on the Social Care Register in Hertfordshire with Learning Disability as the primary need is 3664, with 359 who live outside of Hertfordshire, giving a total of 3,305 compared with 5661 on GP registers (Data as at 30th June 2019). There are approximately 1200 children and young people with a learning disability known to the 0-25 Together Service. The SEND (Special Educational Needs and Disability) offer for people with a learning disability living in Hertfordshire is outlined in the Strategy, ‘Shaping the Future of SEND in Hertfordshire’. www.hertfordshire.gov.uk/microsites/local-offer/media-library/documents/policies-and-procedures/send-strategy-2018-2023.pdf

P a g e | 7
CHAPTER 2 - The LeDeR process in Hertfordshire 2.1. What is LeDeR? The LeDeR programme reports on deaths of people with learning disabilities aged 4 years and over. The definition of ‘learning disabilities’ is that of ‘Valuing People’ (2001 and updated in 2007) and includes the presence of: ‘A significantly reduced ability to understand new or complex information and to learn new skills, with a reduced ability to cope independently, which started before adulthood, with a lasting effect on development.’ LeDeR is the first national programme of its kind and aims to make improvements to the health and well-being of people with a learning disability. Reviews are carried out to learn lessons from which improvements to the standard and quality of care for people with learning disabilities can be made thereby reducing health inequalities and premature mortality. People with learning disabilities, their families and carers have been central to delivering the programme both locally and nationally. The Learning Disabilities Mortality Review (LeDeR) programme is delivered by the University of Bristol. It is commissioned by the Healthcare Quality Improvement Partnership (HQIP) on behalf of NHS England. Currently each ‘Transforming Care Programme’ Partnership is responsible locally for the delivery of the programme. In Hertfordshire this footprint covers Hertfordshire County Council; Herts Valleys CCG and East & North Hertfordshire CCG. This is the second annual report of Hertfordshire Learning Disabilities Mortality Review (LeDeR) programme. LeDeR has been developed as a result of numerous reports over the last 15 years indicating that people with a learning disability die significantly younger than the general population. This report presents information about the deaths of people with learning disabilities living in Hertfordshire aged 4 years and over notified to the LeDeR programme from 1st April 2017 – 30th March 2019. The report reflects on a range of key indicators that offer comparisons with both the national data of the 3rd Annual LeDeR Report (2018) and that of the general Hertfordshire population. It then goes on to describe how Hertfordshire is implementing the actions from learning and outlines plans for the coming year. 2.2 Development of the Hertfordshire programme LeDeR in Hertfordshire commenced in April 2017. Initially the first 6 months involved identifying a ‘Local Area Contact’ (LAC) responsible for the local delivery of the programme; establishing a robust Governance process; an effective Steering Group and training potential reviewers. Whilst this work was taking place deaths were being reported to the LAC by Bristol University. Following the publication of the 2nd National Annual report it was recognised by NHSE that resources to assist local areas were needed. In 2018/19 Hertfordshire were allocated £25,000.

P a g e | 8
This funding was used to employ a LAC 3 days per week to have oversight of the programme. This funding was initially until March 2019, but further monies have been made available for 2019/20 (£54,000). Together with additional investment from Hertfordshire Transforming Care Programme (TCP), this post has been invaluable in ensuring the programme runs smoothly. However, a backlog of the cases waiting to be reviewed has developed due to a lack of reviewers. This has often been due to a lack of capacity alongside their substantive roles to commit to reviewing cases. The 3rd National Annual Report was released in May 2019. At the same time NHSE announced that a £5 million investment had been made available to assist in increasing the completion of reviews. In addition to supporting local areas to ensure cases are reviewed in a timely manner going forward, the funding will be used to support the completion of reviews pre-December 2018 that remain outstanding. This will be done by the commissioning of a 3rd party, North-East Commissioning Support Unit. In Hertfordshire this will involve the completion of reviews for 35 cases. 2.3 Steering Group and Governance LeDeR in Hertfordshire reports to a range of Boards. Ultimately LeDeR sits under the Hertfordshire TCP Board which reports directly to NHSE. Both CCGs have responsibility for the quality and outcomes of the programme, which the Hertfordshire LeDeR Steering Group oversees on their behalf. The Steering Group also reports to Safeguarding Boards and quality boards within the CCGs. (See Appendix 1: Governance Structure & Appendix 2: Terms of Reference). The Steering Group is made up of representation from:
An independent Chair
Family Member – expert by experience
Person with a learning disability
Representative across both CCGs
LAC, Learning Disability Commissioning, Integrated Health & Care Commissioning Team
Adult Disability Services, Hertfordshire County Council
Adult Community Learning Disability Nursing & Heath Liaison Team, Hertfordshire County Council
Hertfordshire Partnership Foundation Trust (HPFT)
Hertfordshire Community Trust (HCT)
Central London Community Health Trust (CLCH) – from October 2019
East and North Herts NHS Trust (ENHNT)
West Herts Hospital Trust (WHHT)
Health Watch
Herts Care Providers Association (HCPA)
NHSE LeDeR Regional Coordinator (East) Information sharing: Records are made available through the application of a Section 251. This is approval given by the Secretary of State for information about an individual who has died being made available to the programme without breaching GDPR.

P a g e | 9
2.4 Children & Young People
Child Death Overview Panels (CDOP) are a statutory NHSE process which involves reviewing the death of anyone under the age of 18 years. The review process of CDOP is different to LeDeR but completing a LeDeR review can complement the outcome of a CDOP. With this in mind, CDOP has requested that LeDeR continues to complete reviews of children with a learning disability and present them at the CDOP panels to provide any additional feedback as to lessons learnt.
2.5 Reviewers.
Reviewers are clinically or social care trained professionals working in Hertfordshire. Reviewers work for CCGs; Hertfordshire Adult Disability Services, ENHNT, WHHT, HCT & HPFT. Independent reviewers are also employed to assist with increasing the output of reviews and to offer objectivity and impartiality where reviews may require it. A key issue around the effectiveness of delivery of the programme is the lack of people who have come forward to be trained reviewers. Once trained, reviewers are asked to complete 2 – 3 reviews a year. Reviewers have raised concerns that a lack of capacity to ring-fence time to complete the reviews within their substantive role has been a problem. With limited reviews being completed, a backlog of cases has developed. Training was initially provided within a structured group, face to face setting. Since October 2018, training is being delivered via e-learning. This is positive in the sense that individuals can do the training in their free time but proves harder to monitor completion of training and thus readiness to perform reviews. Currently Hertfordshire have 20 active reviewers. A further 12 people have not finished their training or have completed it but not yet picked up their password to enable them to carry out a review. In addition, 1 reviewer will now be involved in the quality checking process so is not able to take on any more reviews. However, an additional 14 people have applied to be reviewers from the Mental Health Provider in Hertfordshire, and we are looking at holding a face to face training session for these volunteers. 2.6 Review Process It is the job of the reviewer to conduct an initial review of each death. All information is accessed, edited and completed via the secure web-based portal of the LeDeR Review System. The initial review process involves:
Contacting a family member or another person who knew the deceased person well and discussing with them the circumstances leading up to the person’s death.
Scrutinising at least one set of relevant case notes and extracting core information about the circumstances leading up the persons death, for example from GP, social care or hospital records.
Developing a pen portrait of the person who has died and a timeline of the circumstances leading to their death.

P a g e | 10
Completing the LeDeR programme online documentation and producing recommendations from the review. The recommendations are reviewed by the LAC and Hertfordshire Steering Group, as part of the national LeDeR process. Any specific local recommendations are passed on to any the Improving Health Outcomes Group (IHOG) for implementation.
In some instances, the initial review highlights that specific learning around a death is needed. In this instance a multi-agency review is required. A summary of the Hertfordshire process is in Appendix 1

P a g e | 11
CHAPTER 3 - Findings from the Hertfordshire LeDeR Programme 3.1 Notifications and Data In Hertfordshire, the number of deaths notified to the LeDeR programme in 2017/18 was 45 compared to 60 in 2018/19. This represents a 33% increase for 2018/19. This may be attributed to the fact that through improved communications stakeholders have increased knowledge of the LeDeR process and the requirement to report a death to the University of Bristol. According to the national LeDeR report, which is based on the period from 1st July 2016 to December 2018, it is estimated that the programme received approximately 86% of the estimated number of deaths of people with learning disabilities in England in 2018. Whilst Hertfordshire is unable to measure cases not notified, the national figure suggests continued encouragement to identify and report deaths of people with a learning disability is required. One of the more difficult groups to identify are children and young people. Whilst all deaths are reviewed by CDOP, anecdotally people are not always aware that LeDeR, Bristol also needs to be notified. Furthermore the clarity as to the use of the term ‘learning disability’ can prove problematic as people are generally not diagnosed as having a learning disability; the use of the term ‘learning difficulties’ is often used and ‘global developmental delay’ may also limit whether a case is identified as appropriate for LeDeR. In Hertfordshire, as of the end of May 2019, 62 reviews had not yet been allocated. Of the 62 reviews 18 could not be progressed further due to other investigations being carried out e.g. Safeguarding, Serious Incidents or Police investigations. This equates to almost 30% of the unallocated reviews. The Hertfordshire LeDeR programme carried out a deep dive analysis on the reviews completed between 1st of April 2017 and 31st December 2018. During this period Hertfordshire received 85 notifications of death of which 33 reviews were completed. The deep dive provides an analysis of the 33 completed cases. The analysis of these cases, together with a review of more recent data has provided some valuable information. 3.2 Age In Hertfordshire the median age of death notifications reported in total since April 2017 is 63 years compared to 58 years nationally. This is higher than 17/18 when the median age of death of those notified was 59 years.

P a g e | 12
3.3.1 Level of Disability vs Age
This data comparison is taken from the national LeDeR programme annual report against the Hertfordshire deep dive of 33 completed cases. *It is worth noting that identifying which category of learning disability an individual is in was ascertained from records and based on the person who notified the death’s interpretation. 3.4 Gender
*Actual deaths taken from Hertfordshire LeDeR data 17/18 April – March (Average age).
Actual deaths taken from Hertfordshire LeDeR data 18/19 April to March (Average age).
Male 32 55 yrs. Male 39 62 yrs.
Female 19 58 yrs. Female 19 70 yrs.
Data refers to average age taken from all learning disability deaths reported to the LeDeR programme across Hertfordshire between April 2017 – March 2019 * 46 deaths were ‘reported’ in 17/18, but an additional 5 deaths occurred in 17/18 and were not reported until 18/19
For 17/18 the number of notifications who were male was 64% higher than female and in 8/19 the number of male deaths rose to 105% higher than female deaths.
66
60.5 57
62 63
57
Mild Moderate Severe
Median age at death by level of LD
Hertfordshire NHS
28 39
17 19
17/18 18/19
Gender
Male Female

P a g e | 13
There is a marked difference in the number of deaths reported by gender between Hertfordshire and National data. In Hertfordshire the difference is more pronounced with nearly twice the number of males dying compared to females, whereas nationally, the data is split evenly between males and females. In Hertfordshire there are twice as many males than females with a learning disability on the QOF registers. For example, Herts Valleys CCG has 1858 males compared to 1111 females as at January 2020. 3.5 Ethnicity The majority (90%) of the notifications were of people who were White-British. This is comparable to the National LeDeR Report; however, it is different to the Hertfordshire minority ethnic group data (2011 census) which indicates only 81% of the general population is White-British.
Bangladeshi 1
Gypsy/Irish Traveller 1
Irish 1
White British 29
Not known 1
3.6 Cause of death In the national LeDeR report, the top 3 causes of death are pneumonia, aspiration pneumonia and sepsis. These account for almost 49.5% of the total deaths reported since April 2017 nationally. In Hertfordshire, the cause of deaths has followed the national trend with pneumonia (27%), aspiration pneumonia (14%) and sepsis (16%) as the three main causes of death (57% of all deaths reported locally). Cause of death 1st April 2017 - 31st March 2019 in Hertfordshire in numbers
32
13
12 9
11
6
6
5 4
17 Pneumonia
Aspiration Pneumonia
Sepsis
Cardiovascular
Neoplasms
Digestive Systems
Data taken from Hertfordshire County Council
Deep Dive of 33 completed reviews of LD
deaths across both CCGs April 2017 to
December 2018.

P a g e | 14
3.7 Deep Dive of Reviewed Cases Hertfordshire undertook a deep dive of 33 reviewed cases notified between 1st of April 2017 and 31st December 2018 to further analyse the data from the cases in line with the National LeDeR Report. The pie chart below shows the three main causes of death from the deep dive data Of those 33 individuals who had Pneumonia or Aspiration Pneumonia, 15 had a secondary condition:
Epilepsy
Dementia
Stroke
Congenital heart defect
Cancer
Constipation
Diabetes
Parkinson's disease
3.7.1 Use of psychotropic medication The National LeDeR report mentions that there is a higher rate of prescribing of psychotropic medicines among people with learning disabilities than the general population. Medicines are sometimes prescribed even though there may not be a mental health condition diagnosed in the individual, often to help manage behaviour that challenges. The numbers in the national report who were taking psychotropic medication was small and the report recommended that data is used with caution. In Hertfordshire, 5 of the 33 Deep Dive cases were individuals who were prescribed psychotropic medication. From the information in the reviews none of the 5 had been diagnosed with a mental health issue. 3.8 Place of Death based on number of deaths Nationally, the proportion of people with a learning disability dying in hospital is higher (62%) than in the general population (46%). Hertfordshire: in 2017/18 67% of people reported to LeDeR died in hospital compared to 57% in 2018/19. There was also an increase in the number of people who died at home in the period 2018/19 compared to 2017/18 from 27% to 38%.
16%
27%
14%
43%
Sepsis
Pneumonia
Aspiration
Other

P a g e | 15
3.9 Prevalence data of deaths by month There is no evident trend as to the month people died, however Hertfordshire has experienced a rise in numbers in the winter pressures months. As data continues to be collected in 19/20 and beyond, trends regarding deaths and the month in which they occur can be analysed more accurately.
3.10 Comparison of notification by CCG The number of notifications of deaths to the LeDeR Programme by the two CCGs is also very similar in number. Breakdown of notifications by CCGs: April 2017 – March 2019
27%
4%
67%
2%
38%
2%
57%
3%
Home Hospice/Palliative Hospital Not known
Place of Death in 17/18 and 18/19
17/18 18/19
0
1
2
3
4
5
6
7
8
9
10
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Reported deaths per month 2017/18 and 2018/19
2018/19
2017
ENHCCG - 47
HVCCG - 54

P a g e | 16
3.11 Its not all about the numbers
Whilst it is important to recognise the trends of who has died, when they died, where they died etc. LeDeR is far wider than this. From the reviews qualitative information has provided evidence that identifies where practice has fallen short. It is these themes whereby reviewing practice and developing innovative solutions the programme can influence impact on the quantitative data and ultimately an individual’s health outcome.
Poor understanding/ application of Mental Capacity Act
Do not resuscitate processes not always followed
No advance care planning taking place
End of life plans put in place too late
Limited examples of joined up working, information sharing and involvement of families/ carers
Diagnostic over-shadowing … not recognising the signs and symptoms that may lead to deterioration of health conditions.

P a g e | 17
CHAPTER 4 - Learning into Action (Improving Health Outcomes) 4.1 Introduction Once the reviews have been completed and the LeDeR Steering Group has reflected on the findings and recommendations, actions are identified and added to an action plan. The responsibility for implementation of the actions sits with the ‘Improving Health Outcomes Group’ (IHOG). This group consists of operational staff from health and care sectors. Where actions are identified for their own organisations, individuals are accountable for reporting back to IHOG and ultimately the LeDeR Steering Group. 4.2 Identification of people with a Learning Disability Based on the national prevalence estimations that 1.5% of the population have a learning disability, the number of people recorded on GP Learning Disability Registers in Hertfordshire is lower than the predicted figure. The expectation of CCGs is to ensure practices have an accurate Learning Disability Register. This is being achieved by identifying people who are known to have a learning disability but are not currently on the Learning Disability register and by community learning disability nurses working with GP practices to identify people with a learning disability who are known to Adult Disability Services but are not currently on the Learning Disability register. It is then the requirement of the practice to follow up with patients to ask whether they wish to be added. For individuals without a diagnosed learning disability, a national identification tool has been developed. Whilst this is not a formal diagnosis, GPs are encouraged to use the tool where it is recognised that the individual would benefit from being on the Learning Disability Register in order to receive further support to manage their health. In Hertfordshire the number of children and young people with a learning disability on the GP Learning Disability Registers is disproportionately small compared to the number of children/young people with potential conditions which are linked to the person having a learning disability. Prior to a formal diagnosis being given, paediatricians are often using the term ‘global developmental delay’. This coding is not recognised as being someone with a ‘learning disability’ and so there may be individuals not being included on the Learning Disability register who otherwise could be. The Lead Community Learning Disability Nurse is currently writing guidance to support paediatricians and other professionals in enabling individuals to be added routinely to the Learning Disability register going forward.
4.3 Annual Health Checks Annual Health Checks for people with a learning disability should be offered to people aged 14 and over who are on their GP practice learning disability register. The Annual Health Check includes a physical examination, an assessment of lifestyle, mental health, medication, chronic illness and use of any specialist services. This is an excellent opportunity for health promotion and early intervention and can be effective in detecting previously undiagnosed conditions.

P a g e | 18
Nationally the Annual Health Check (AHC) completion target has been set at 75% of all people on the learning disability register. Figures for 2018-19 illustrated that HVCCG achieved 73% based on QOF Learning Disability register number of 2230 of individuals aged 14+ and ENHCCG achieved 64% based on QOF Learning Disability register number of 2399. However, figures for the completion of Annual Health Checks of the 14 to17 age group are less than 50% for both CCGs. In order to address this and support practices to achieve NHSE targets, the following activity is taking place:
Commissioners are working closely with the Looked After Children Team, the Disability Nursing Team, paediatricians, school nurses who work with children and young people with a learning disability and parents of young people in order to raise awareness as to how a person can be added to the Learning Disability register and the benefits of encouraging people to have an Annual Health Check.
Community Learning Disability Nurses are based within each Locality Team across Adult Disability Services. The Community Learning Disability Nurses act as a link with practices to ensure GPs/ nurses are supporting patients with a learning disability appropriately.
A range of materials have been developed to support individuals to attend an Annual Health Check, for families/ carers to support people at an Annual Health Check and professionals to deliver a high-quality Annual Health Check. This information is widely promoted across a range of services.
A co-produced survey is underway by Health Watch Hertfordshire to determine the quality of the annual health checks. The report will be available by end of May 2020.
4.4 Purple Star Strategy The Purple Star Strategy is an accreditation programme which is delivered by the Hertfordshire Community Learning Disability Nursing Service (part of ADS) in line with the Equality Act 2010 legislation. It includes training for providers followed by ongoing auditing to ensure health services who are awarded a Purple Star are demonstrating that their services are providing high quality, reasonably adjusted services to people with a learning disability. Below is the breakdown of health organisations that have gone through the training and achieved the Purple Star and those in the process of achieving it. So far, 36% of the 110 GP practices/ groups across the two CCGs have been awarded or
are in the process of being awarded the Purple Star, with a target to be at 45% by the end
of the financial year.
GP practices
Specialist Dentistry
Pharmacy Hospices Hospital wards
Others Total
Purple Star Accredited organisations
26 4 1 6 10 6 53

P a g e | 19
Purple Star accredited health services from 2014 to June 2019 (source Health Liaison Team)
To support GP practices on a day to day basis the Community Learning Disability Nurses employed by Hertfordshire County Council can be accessed via a referral form. This form is up and running across both CCGs. It is available on web pages as well as directly on CCG IT systems (Ardens and DXS). The referrals go to a central email address, are triaged and passed to the relevant nurse teams by senior nurses for the two sides of the county. Further analysis is required to check whether the referral form is being used and who is making referrals to ensure this process is working effectively. 4.5 Actions to Address Respiratory Conditions 4.5.1 Flu Jabs Both the National LeDeR report and local reviews that have been carried out to date show that pneumonia or aspiration pneumonia were identified as the most common cause of death. These conditions are potentially preventable and treatable, if caught in time. A focused campaign has been taking place to increase the take up of flu jabs and in turn reduce the potential risk of pneumonia. Public Health England, East of England Regional Team operate a ‘Flu Planning Group’ which covers Herts, Beds, Luton and Milton Keynes. Hertfordshire representation includes members from HCC Public Health department, Integrated Health and Care Commissioning Team, colleagues from the Health Liaison Team and both the CCGs. In partnership, a communication plan has been developed. This is shared with the Hertfordshire and West Essex Sustainability and Transformation Partnership (STP) in order to ensure consistent messages are given. Accessible resources created by Public Health England have been shared widely, for example, ’easy read’ leaflets and posters. Information and guidance about best interest decisions and informed consent have also been put into ‘easy read’ for GPs, nurses and pharmacists to be able to communicate more effectively with patients. The HLT presented at an event for the East of England Regional Team to explain how best to support people with a learning disability to get their flu jabs and make reasonable adjustments. Delegates included clinicians and health professionals’, GPs and pharmacists from across Herts, Beds, Luton and Milton Keynes. As a follow up to the seasonal flu vaccination campaign, the PHE East of England Flu Planning Group have agreed to promote the flu vaccination this year to the following groups with an aim to increase uptake: Social care staff working at care homes & hospices (promoting the message that they are entitled to a free NHS flu jab)
Organisations working towards Purple Star accreditation
11 1 5 17
Organisations on waiting list
6 11 17

P a g e | 20
The under 65 years of age at risk group – particularly those with liver disease and those with a learning disability The national target for flu jabs has been set at 60% by PHE and to date, HVCCG have achieved 60.09% for flu jabs and so they have exceeded this target. We await figures for ENHCCG on what they have achieved. 4.5.2 Specialist Dentistry The Special Care Dental Service is for people with a learning disability who are unable to access oral health care from their local high street dentist. The service consists of 4 clinics across Hertfordshire. They also provide a Domiciliary Service to patients who are unable to leave their home. The majority of referrals to the Special Care Dental Service come from General Dental Practitioners. Other health and social care providers can also refer to the service. The Special Care Dental Service has promoted its existence and ensures more integration within current patient pathways. All 4 clinics are Purple Star accredited. Competencies are linked to the Commissioning Guidelines for Special Care Dentistry. An accreditation process for Special Care Dentistry is being introduced in the UK and plans are in place to ensure that the service will be running at level 2 accreditation - the process is still in the early stages nationwide, but staff are working to ensure they are ready when it is rolled out. 4.5.3 Swallowing and Eating Difficulties Dysphagia is the medical word for a swallowing problem. Dysphagia can lead to increased risk of aspiration (food or fluid going down the ‘wrong way’ and entering the airway into the lungs). The National LeDeR annual report published in May 2018 highlighted dysphagia as one of the most common long-term conditions experienced by people with a learning disability. 16% of deaths reported to LeDeR are attributable to aspiration pneumonia; some of these deaths may have resulted from dysphagia (swallowing difficulties). Internally, HPFT operate a specialist Dysphagia SLT (speech and language therapy) pathway. Uniquely, this also includes a specialist dietetics service which aims to reduce additional negative health consequences of aspiration such as dehydration and malnutrition. As of May 2019, 152 adults with a Learning Disability were referred to the SLT Dysphagia service for an assessment of their eating and drinking skills. In 2018/19 the number of referrals was 211 The Dysphagia pathway aims to identify the nature and severity of a swallowing difficulty and implement a dysphagia care plan where required. The aims of the care plan are to reduce the risk of choking and aspiration as much as possible, taking into account the best interests and wishes of the service user. Specific assessments are completed by a Speech and Language Therapist with input from the service user, their family, carers and any other key people involved with the individual.

P a g e | 21
In addition to specific, individual work, the SLT and Dietetic service also offer dysphagia training to carers of people with learning disabilities and dysphagia. It is recommended that all people caring for adults with dysphagia and learning disabilities attend this training. This is emphasised in dysphagia care plans and information is enclosed in dysphagia discharge reports as standard. The training has been held quarterly and is free of charge. Following positive feedback on these training sessions and in response to an increase in demand, the length of training has recently been extended from a half day to a full day session and from 2020 onwards, the training will be offered every other month. HPFT is continually looking to improve the dysphagia service, to best ensure that the needs of this vulnerable and complex population group are met. Following liaison with local physiotherapy colleagues, information relating to the risk of sepsis and signs of deterioration is now included in dysphagia guidelines as standard. The current aim of those delivering the dysphagia pathway is to improve the multidisciplinary (MDT) input into the pathway with plans for additional input from both local physiotherapy and Occupational Therapy (OT) services. Shorter, practical workshops delivered by the Assistant Therapy Practitioners (ATPs) take place that focuses on the practical side of things, for example, food preparation, food fortification and thickening drinks. These sessions are in-house and usually based on identified need following a referral or managers may request this when they have got several new staff members. 4.5.4 Sepsis Sepsis is a rare, life-threatening condition that can develop rapidly from a local infection. As, for example, a chest infection, or a urinary tract infection if left untreated. In Hertfordshire we know that 16% of deaths reviewed were attributed to sepsis. Nationally there has been a rise in the number of patients diagnosed with sepsis year on year. This might be because it is being better recognised, but it is also partly due to a rise in cases. We know that changes to the coding guidelines attributed to a sharp rise in recordings for sepsis in 2017/18. In April 2018, the coding guidelines changed again. Sepsis would only be in the primary recorded diagnosis if it was the main condition treated. There has been a lag for these new changes to take effect, but numbers of coded sepsis patients have fallen (nationally) since then. Hertfordshire data is not following the national trend related to coding changes in that our numbers are still high for sepsis. To overcome this, East and North Herts NHS Trust (ENHNT) have established a learning disability working group. ENHNT did a joint presentation to Grand Round with the Sepsis Nurse in September 2018. These are targeted short bite training sessions and provided an opportunity to raise awareness about mortality rates in people with learning disabilities and the deteriorating patient, 60 medical staff attended. A deteriorating patient study day was organised by the Sepsis Nurse for Nursing and
Medical staff in May 2019. ENHNT have updated their Learning Disability policy in 2019
A Task and Finish Group has been created with the Health Liaison Team to identify and produce accessible sepsis resources. As a result, ‘Easy Read Signs of Sepsis Information’

P a g e | 22
leaflet has already been co-produced. A well-established guide (Top to Toe) to support with early recognition of the signs and symptoms of ill health in people with learning disabilities is currently updating the information on sepsis. This guide is used by paid carers. Purple All Stars (creative arts group made up of people with learning disabilities) have produced a song on sepsis and they have promoted this via live performances and social media. This is aimed at more independent people with learning disabilities who may not access other sources of health information. WHHT also have a dedicated Sepsis clinical Nurse Specialist within the Trust who has produced easy read sepsis information and has dedicated sepsis awareness boards in all clinical areas. 4.6 Communication and Access to Services 4.6.1 Purple Folder The Purple Folder was first developed in Hertfordshire in 2010. It is a Health Action Plan and Health Portfolio held by the individual with a learning disability. The Purple Folder holds important health information about the individual that is ideally completed by the health professional and/or their carer/supporter. The health professional should refer to the Purple Folder and contribute to the Health Action Plan within it. The aim is that everyone with a learning disability who wants a Purple Folder will have one and that it will be used as a reasonable adjustment to improving access to equitable health care. The Purple Folder is now in its third version. More recently the information about mental capacity has been updated and three red pages have been added. These help create a speedy summary of what reasonable adjustments someone needs, who else is involved in the person’s health and social care, a summary of the baseline and known ways the person communicates pain or illness. An annual survey was carried out in 2017 with randomly chosen people who are known to social care by the Integrated Health and Care Commissioning Team. In this survey people with learning disabilities were asked questions on the ownership and use of the purple folder. The response was very positive with 73% having a purple folder and 70% said that health staff writes in their purple folder. A maintenance service is offered to provide replacement sheets as/ when requested and there is also an A5 format that has proved increasingly popular. 4.6.2 Purple All Stars The Purple All-Stars are groups of people with a learning disability who use creative arts to deliver health promotion messages to others working alongside the Community Learning Disability Nursing Service. Four groups have been established across Hertfordshire. The health messages are carried out via live performances and social media like ‘YouTube’. Their latest performances included ‘Bridging the Gap’ Learning for Change LeDeR conference (over 120 delegates) and ‘Shout about it’ event where there were over 100 attendees made up of carers and people with learning disabilities.

P a g e | 23
Examples of the work of Purple All Stars: https://www.youtube.com/watch?v=WvgJgBofIXQ https://www.facebook.com/purplestarstrategyproject 4.6.2 Website and links to supporting materials There is a dedicated website ‘My Health’ where professionals and carers can access materials and information to promote and explain health related matters for people with learning disabilities. This website has proved very popular with both paid and unpaid carers as well as professionals. Since its launch in 2016, to end of October 2019 the website has received over 5000 views/hits. ‘My Health’ website has also now been made available to the Hertfordshire Public Health website. A dedicated newsletter for ‘Improving Health Outcomes for people with a Learning Disability’ has been created including an ‘easy read’ version that is shared and promoted widely. Both the Health Liaison Team and Public Health have worked together to make the services delivered by Public Health more accessible for people with a learning disability. An example of this is that both the Customer Services team and the referral forms for services such as drug and alcohol services, weight management and smoking cessation, now ask specific questions about whether the person has a learning disability or any additional needs to access services. Improved joint working is in place across Hertfordshire Public Health and Adult Disability Services. This has assisted colleagues to share information and gather knowledge of services and how to refer to them. Pathways to support dementia and diabetes are developed and embedded. Information about both conditions can be found on the My Health web page. An epilepsy pathway is also in development WHHT has a dedicated web page on the internal intranet page. This is available to all staff to access resources to a range of materials to support the patient. It provides links to easy read materials, national reports, and support services.
4.6.3 Top to Toe
The ‘Top to Toe’ folder is a guide to support early recognition of the signs and symptoms of ill health in people with a learning disability. The Top to Toe folder aims to empower paid carers to be able to undertake their role more effectively, raising awareness about some of the common health conditions more likely to be experienced by people with a learning disability. Providing this information will help carers recognise and respond promptly to symptoms and seeking early medical help, enabling a more knowledgeable exchange of information. Ultimately this will support improved health and well-being of the individual with a learning disability and may prevent premature death. Providers are trained in how to use the handbook however the training programme is currently on hold whilst consideration is given as to how to implement the programme more

P a g e | 24
effectively. In the meantime, the health information is being updated and being made available on the ‘My Health’ web page. 4.6.4 Communication App
Commissioners from Hertfordshire County Council working in partnership with a software company have developed a communication app called ‘My Health Guide’. This app is aimed at improving communication between individuals, the carers who support them and health professionals. The communication app has been approved by the Assistive Technology team within Hertfordshire County Council and the target is to have 1,000 people recruited to the project in 2020 free of charge. 4.7 Reducing and/ or stopping the overmedication of people with learning disabilities
STOMP stands for stopping over medication of people with a learning disability, autism or both with psychotropic medicines and STAMP stands for Supporting Treatment and Appropriate Medication in Paediatrics. STOMP is an NHSE programme involving a range of key stakeholders to support individuals to ensure they are being medicated appropriately. Other therapies and support (including family support) should be offered before prescribing and while taking psychotropic medication. In Hertfordshire an All Age STOMP/STAMP group has been established. Protocols are in place to identify individuals with a learning disability, being prescribed psychotropic medication and not on the mental health register. Once identified the Community Learning Disability Nurse completes a risk assessment with the individual (and carer) and working closely with the GP and HPFT all parties consider whether the person would be suitable to participate in a reduction programme. Within WHHT a team of pharmacists have been reviewing the medication for all learning disability patients who are admitted as inpatients. The aim is to ensure that there are no patients being inappropriately medicated. Over the last 2 years, HPFT have kept a database to record all medications and related needs for example sensory, on all people with Learning Disability receiving treatment. As part of a reduction research project patients known to HPFT have been profiled and their medication monitored. It has been estimated that approx.100 of these people may benefit from a reduction in line with STOMP. HPFT are working on final audit and results of this piece of work so that it can be clinically validated and published. HVCCG learning disability GP lead continues to raise the STOMP/STAMP profile across the CCG and the implementation of STOMP processes is now part of the accreditation process for GP practices to achieve the Purple Star.

P a g e | 25
4.8 Avoiding and/ or reducing hospital admissions and active planning for people with complex health needs 3 Health Improvement and Prevention Nurses for people with learning disabilities (HIP-Learning disabilities) have been employed by the Health Liaison Team. The role of the Health Improvement and Prevention nurses (HIP LD) is to provide an individual health assessment and identify clinical markers that put the service user at risk of clinical deterioration, which due to communication difficulties may make these difficult for the carers to detect. They develop a health contingency plan with the carers using tools developed to help carers identify whether the baseline measurements such as temperature, blood pressure, pulse and respiration deteriorate and how to respond. It is anticipated that this will ensure that clinical deterioration is identified early, and medical help sought with information that allows the clinicians to assess and diagnose in a timely way. 4.9 Acute Liaison Nursing Service The Acute Liaison nurses have a specific focus on supporting adults and transition age patients (16 – 18 years) with a learning disability to access the Acute Hospital Trusts across the county of Hertfordshire. The team work specifically with both West Hertfordshire Hospitals Trust and East and North Hertfordshire Hospital Trust. Furthermore, they also provide support within Hertfordshire Community Trust settings. Support is provided during normal working hours of Monday to Friday 09:00 -17:00. Referrals to the Acute Liaison Nurses are made via the team contact number or email and can be made by anyone. Between January and August 2019 there have been 483 referrals made to the Acute Liaison Nursing Service. The Acute Liaison Nursing service has supported both Acute Trusts in developing local plans for embedding the NHS Hospital improvement standards. Trust specific actions plans are in place; they were jointly developed by the Trust and the Health Liaison Team. 4.10. Improvement Standards The standards have been developed with several outcomes created by people and families — which clearly state what they expect from the NHS. By taking this approach to quality improvement, it places patient and carer experience as the primary objective, as well as recognising the importance of how the NHS listens, learns and responds in order to improve care. The four standards concern:
respecting and protecting rights
inclusion and engagement
workforce
learning disability services standard (aimed solely at specialist mental health trusts providing care to people with learning disabilities, autism or both)
The standards are intended to help organisations measure quality of service and ensure consistency across the NHS in how we approach and treat people with learning disabilities, autism or both. ENHHT, WHHT, HCT, CLCH and HPFT all have action plans in place to measure improvements. Feedback to NHSE is provided annually and Trusts are being benchmarked against other trusts. Whilst this framework is now being applied across NHS

P a g e | 26
Trusts as a matter of course, locally the Trusts have been working on specific projects to improve practice in mainstream provision. East & North Herts NHS Trust (ENHHT) In ENHNT there is a more proactive and responsive clinical management of Sepsis for patients enabling clearer pathways for managing complex issues that delay treatment. For example, consideration of alternative routes of administering emergency/essential medication when IV access is difficult or not possible. The Learning Disabilities working group is well established with representation from various specialisms, professionals and commissioning. The group meets regularly to look at ways of ensuring that the Learning Disabilities action plan and standards are implemented within the Acute Trust and to enable a more proactive approach for patient care overall within the Trust. Learning Disabilities Awareness Workshops were delivered to midwife champions to improve their understanding of support available and to ensure more positive outcomes for patients There is regular training to Preceptorship nurses and Clinical Support Workers. Purple Star strategy is well embedded in four awarded areas – Day surgery, Ophthalmology, Diabetic eye screening, ambulatory care QEII. 2 areas are currently in progress – Emergency department and Endoscopy. All awarded clinical areas have been able to demonstrate improved practices in the care of people with a learning disability A pilot is currently in progress for an earlier start for the acute liaison nurses. This is allowing concerns and issues to be highlighted in a timely way enabling nurses to be more proactive in ensuring appropriate actions are taken. There is evidence that this has had a positive effect by improving identification of patients with a learning disability and swift intervention for patients. West Herts Hospital Trust (WHHT) In the West Acute Trust, the Acute liaison nursing service continues to provide Learning Disability Awareness training face to face at corporate induction days two - three times per month. There has also been training provided to junior doctors, student nurses and adults’ at-risk champions within the Trust. An e- learning package was developed by the Acute Health Liaison team to assist in increasing training compliance, to give staff more flexibility and access as to when they can do the training. The Purple Star Strategy is well embedded in St. Albans City hospital Day Surgery Unit, Watford General hospital, St. Albans Pre-op, Watford General hospital pre-op and vascular lab and AAA screening lab. A palliative pathway has been developed to enable a clearer process for enabling support and a more proactive management of learning disability patients who are palliative. This ensures that all Learning Disability patients who are deemed to be palliative are reviewed by the palliative care team regardless of whether they are symptomatic or not.

P a g e | 27
A pathway has been developed for Learning Disability patients who may require sedation or anaesthetic to enable outpatient investigations to be undertaken which may otherwise be distressing for the patient. A specific pathway has been developed for patients with complex care needs who attend hospitals repeatedly for the same issues. This has been devised using a collaborative approach between, the hospital team, carers and the health liaison team with an aim to reduce unnecessary repeat admissions and waiting times. It also identifies the individuals’ specific needs and a reasonable adjustment that may be required to enable a less distressing visit. This has led to improved patient experiences and outcomes. There was successful engagement with staff and public during learning disability awareness week and a pledge for enabling good care was recorded and shared using Makaton signs and shared on social media. In addition, an event was held to engage with people with learning disabilities and their carers to get direct feedback on their experiences. An escalation pathway for carers has been developed to provide a clearer process in highlighting concerns and to enable earlier resolution. Hertfordshire Community Trust (HCT) Hertfordshire Community NHS Trust have produced a Learning Disability Plan. The plan is based on the Learning Disability Improvement Standards for NHS Trusts that came out in 2018. HCT is using three of the NHS standards to inform their action plan for people with learning disabilities. It is hoped that the learning disability action plan will demonstrate the Trust’s commitment to provide people with learning disabilities, autism or both and their families and carers high quality care across all services provided by the Trust. For governance purposes, the action plan will be presented as part of the safeguarding work-stream to the Healthcare Governance Committee and to the Trust Board. The Executive Lead for the Learning Disability Action Plan is the Director of Nursing and Quality and the delegated responsibility is with the Deputy Director of Nursing and Quality. 4.11 End of Life Feedback from LeDeR reviews has identified the assessment and quality of care provided at the end of life fell short of good practice. In Hertfordshire, reviews carried out inform us that there is a lack of planning in end of life care. It has been identified during some of the reviews that recognition of end of life and timely referrals to Palliative care services has been an issue that needs improvement, and a project is underway at WHHT to improve this recognition and referrals. Where these referrals have been made there has been a marked improvement in co-ordination of care and improved quality of the death. The Hertfordshire 4 Hospice Education Consortium, in collaboration with Hertfordshire County Council Adult Services have to date trained over 110 staff in over 12 care homes across the county on learning disability and end of life care. Isabel Hospice, Garden House Hospice, Rennie Grove Hospice have all completed the Purple Star Strategy Accreditation programme. Hospice of St Francis have completed their training and prepare to be considered for accreditation and Peace Hospice have yet to start the Accreditation process.
P a g e | 28
Funding has been secured to continue with this delivery of training to staff in care homes and day services over the next 6-12 months and study days for the Learning Disability nurses as well. (For case studies please see Appendix 5) 4.12 Work-force development and Training 4.12.1 Acute Care It is recognised that from reviews carried out as part of the LeDeR Programme some social care providers and health professionals have a poor understanding/ application of Mental Capacity Act and ‘Do Not Attempt Cardiopulmonary Resuscitation’ orders. (DNACPR) processes not always followed as highlighted in the national LeDeR report 2019. In WHHT, 91% of all staff have received MCA/Deprivation of Liberty safeguards training and 94% of staff have received learning disability awareness training up until October 2019. During the last reporting period WHHT reviewed and updated the ‘Care of Adult Patients with Learning disabilities and Autism’ Acute Trust policy. This is in partnership with the Health Liaison Team and is available on the Trust intranet which is accessible to all staff. The Named Safeguarding Nurse attends advanced training within protected time to enhance and continue to develop current knowledge regarding the Mental Capacity Act, case law and changes to policy and process. This training is supported by the Hertfordshire Safeguarding Adults Board as well as the Associate Director for adult safeguarding in the CCG. A named Consultant for safeguarding provides MCA training for medical staff as well as teaching medics on a 1:1 basis. A cohort of registered nurses have become ‘at risk’ champions in WHHT. Training sessions are arranged every quarter and the HLT have held training sessions. Topics covered have included LeDeR, reasonable adjustments, and communication with patients with learning disabilities. WHHT safeguarding team undertake monthly deep dive audits on learning disabilities and reasonable adjustments, MCA/DoLS and DNACPR. These audits are presented to the safeguarding panel for discussion. In addition, a bi-annual Trust wide audit is undertaken to review practice and this forms part of the safeguarding adult strategy. East and North Herts NHS Trust (ENHHT) East and North Hertfordshire NHS Trust has introduced an initiative whereby patients with
learning disabilities wear purple bands, this means that patients are easily recognisable and
given appropriate support. This is in a pilot phase and has been received well by patients
and staff who find this visual reminder to make reasonable adjustments helpful.
Also, Individuals who access ENHNT services have an electronic flag in place on the medical records system. This is to highlight to clinical staff that the individual who is being treated has a learning disability and may require reasonable adjustments in the delivery of care. In ENHNT, all preceptorship nurses and preparation to practice clinical support workers receive Learning Disability Awareness training provided by the Health Liaison Team as part of a structured training programme. Staff in clinical areas participating in the purple star accreditation scheme also receive learning disability awareness training.

P a g e | 29
All staff in ENHNT has received training about the Mental Capacity Act and Deprivation of Liberty Safeguards for the period till end of March 2019, with 90% of staff in date for the bi-annual training. The Trust has also introduced a daily ward and site safety huddle system to ensure that the needs of all inpatients with a learning disability is discussed on a daily basis and to ensure that concerns are identified and actioned promptly. All individuals with a learning disability are also subject to a review by a senior nurse daily at matron level and are automatically referred to the HLT for support. 4.12.2 Social Care Providers There are 162 care providers, supporting people with learning disabilities, registered with HCPA (Herts Care Providers Association). HCPA is currently reviewing the ‘Learning Disabilities Champion Pathway’ that is delivered to care providers. In response to the requirement for mandatory training in 2021, HCPA is also developing a mandatory training grid to ensure care staff are appropriately equipped with skills to support people with a learning disability. 4.12.3 Training of staff working for In-house (HCC) services There is a rolling programme for learning disabilities awareness, MCA and DoLS training, in 2017/2018, 538 staff received training and in 2018/2019 600 people were trained. 4.12.4 ‘Bridging the Gap’ Conference In October 2019 a conference was held for health professionals focusing on the key themes impacting on the health of people with a learning disability and how these health inequalities can be addressed in Hertfordshire. Delegates had a choice of several workshops including The Mental Capacity Act in Practice, Supporting End of Life, This is Me! (the family), Applying the Equalities Act and Reasonable Adjustments, Recognising Overshadowing, Health Improvement and Advanced Care Planning – Hospital Avoidance, Understanding Eating/Drinking Difficulties faced by People with Complex Learning Disabilities and What I expect!! Several stands relevant to the conference were also present. Over 120 delegates attended from a wide range of backgrounds including GPs, practice nurses, matrons, physiotherapists, specialist screening practitioners, nurses, etc. Two mini follow up conferences/workshops are planned to take place in May and June to cover both sides of the county. 4.13 Children and Young People The number of notifications who are children or young people received in 18/19 was small and so no specific learning has been identified that differs from findings of adults. Materials that have already been developed by community learning disability nurses have been shared with parent forums, Children’s Services and Paediatricians. Several Learning Disability Nurses work within the 0 – 25 years Team. Whilst they only generally support people aged 18 and over, they are pro-actively involved in the transition process, attending reviews and ensuring that any involvement with children’s health services is transferred to adults in a planned way.

P a g e | 30
Children’s Services Commissioners are working with providers to raise awareness of the Learning Disability Annual Health Check and increase the number of people with a learning disability aged 14 – 17 years who have one. For anyone aged 0-17 years, further support to encourage the uptake of flu immunisation and ensure that individuals are identifiable on the GP learning disability continues to also take place. Representation from Children’s Services are on the STOMP - STAMP working group. STAMP (Supporting Treatment and Appropriate Medication in Paediatrics) is still a relatively new element of the programme. Currently work is taking place around understanding the prevalence of prescribing psychotropic medication to children and young people.
P a g e | 31
CHAPTER 5 – Actions and Recommendations 2019/20 and beyond
5.1 Stakeholder Engagement
Improve engagement with people with a learning disability and families to ensure they are more involved in the LeDeR programme, understand the findings from reviews and are involved in measuring the impact of change.
Develop better ways to provide feedback to those involved in LeDeR reviews and be able to offer more information about how recommendations are being implemented.
Ensure Adult Disability Services are engaged in LeDeR and are aware of their relationship in the bid to reduce health inequalities
Increase engagement with Children’s Services and understand the issues around access to health services faced by children and young people particularly as young people move into adulthood.
5.2 Improving GP Learning Disability Register
Practices should be familiar with the identification tool and the benefits of its application in order to recognise where someone who may have an undiagnosed learning disability would benefit from being on the GP Learning Disability Register.
Commissioned health services for children and young people should be aware of the local guidance outlining the benefits of the person being flagged and on the GP Learning Disability register.
Further analysis is required to check whether the referral form created for practices is being used and that referrals are appropriate.
5.3 Annual Health Checks
GP Practices in both Herts Valleys CCG and East and North Herts CCG should aspire to exceeding the 75% target of completion of annual health checks.
Annual Health Checks should be completed on the most up to date template (devised in 2018) and the individual should leave the Annual Health Check with a Health Action Plan.
Providers, in line with the East of England contracts, should support people with a learning disability at their Annual Health Check where appropriate.
Providers/ family carers should be encouraged to use the Carers Preparation Tool to collate the Annual Health Check information required prior to the meeting.
Continue to work with CCGs and NHS Digital to improve accuracy of data recording.
Work with Healthwatch to implement findings from their current Annual Health Check Quality Audit

P a g e | 32
5.4 Purple Star Strategy
CCGs are encouraged to provide sustainable funding to the Purple Star Strategy with an aspiration for 75% of practices to have achieved/ be working towards achieving a Purple Star by March 2022.
Extending funding to ensure capacity is available to support acute and secondary provision should be considered.
5.5 Respiratory Conditions
The flu campaign initiated by the Health Liaison Team should be continued annually to encourage an increase in uptake of the flu jab amongst people with a learning disability. A target of 60% of people with a learning disability in receipt of a flu jab should be aspired to.
Providers/ families should also be encouraged to have a flu jab for infection control purposes.
Providers would benefit from receiving postural support training which would reduce the likelihood of infection leading to pneumonia and aspiration pneumonia. Working with HCPA to pilot postural support training programme for staff across a range of settings.
Working with HPFT, to develop a physio service for individuals who have complex physical health conditions to directly support individuals with good positioning and dysphagia.
Providers should be made aware of the importance of good oral hygiene and links with aspiration pneumonia and know where to access support.
5.6 STOMP/ STAMP
Review outcomes of the Learning Disability STOMP project. Request further funding to extend the project in order for the Learning Disability Community Nurse working with primary care practices to continue to risk assess potential individuals suitable for a reduction in medication.
Work in partnership with Community Learning Disability Nurses, GPs and HPFT when following any ‘reduction pathway’.
Community Learning Disability Nurses and Specialist Learning Disability Nurses to also consider the benefits of implementing PBS (Positive Behavioural Support) Strategies with families/ paid carers as an alternative to prescribing.
Ensure STAMP is considered where children and young people are being prescribed medication.
Monitor that STOMP is considered when prescribing medication to autistic people who don’t have a learning disability.

P a g e | 33
Continue to monitor HPFT’s management of STOMP through contract and quality monitoring processes.
5.7 Avoiding Hospital Admissions
Funding should continue to be made available to support the HIP LD nurses.
Ensure all providers are aware of NEWS2 scoring being used by Acute Care, GPs and Ambulance Services in Hertfordshire and consider a version to complement this with local settings.
Providers need to be aware of early warning signs and symptoms leading to deterioration of conditions such as Sepsis.
Working in partnership with health and care providers to increase the number of people with a learning disability who have an advance care plan.
Review the ‘Top to Toe’ paperwork and consider how the programme can be implemented going forward.
Providers need to be familiar with pathways to support conditions including, diabetes and constipation and promote healthy lifestyles in line with standards included in the East of England Contract.
5.8 Acute and Community Services
Review initiative around changes to working hours of Acute Liaison Nurses.
Consider the implementation of 7 day working of Acute Liaison Nursing generally.
Seek further funding to expand the Purple Star Strategy across Acute and Community Care Services.
Monitor Acute, Community and Mental Health Trusts Action Plans in response to Learning from Deaths and NHSi requirements.
5.9 End of Life
Continue to identify funding to continue the training and support more providers to
understand how to care for a person with a learning disability on an end of life
pathway.
5.10 Workforce Development
Prepare health and social care provision for the implementation of mandatory learning disability and autism training for all staff.
Review and improve the understanding of MCA; DNACPR; Assessing ‘Best Interest’ and legislation around reasonable adjustments.

P a g e | 34
5.11 Communication
Continue to provide updates on LeDeR through already established communication networks e.g. Co-production Board (& specifically the Learning Disability Co-production work stream); a range of newsletters including the Improving Health Update produced in an accessible format.
Continue to update and develop the ‘My Health’ web pages for people with a learning disability, carers and professionals and the LeDeR web page, both on the Hertfordshire County Council Website.
Continue to share messages with key stakeholders developed by ‘The Purple All Stars’.
Continue to develop materials to expand on the Purple Folder.
Facilitate the introduction of ‘My Plan’ App and develop the ‘my good day’ campaign. 5.12 Strategic Commissioning
Deliver 3 workshops to continue to develop on the work following the 2019 Conference ‘Bridging the Gap’. 2 for professionals on either side of the county and one for families/ paid carers and people with a learning disability.
Work closely with CCGs to continue to collect and monitor data around Annual Health Checks; Flu Jabs: STOMP; Screening; hospital admissions.
Carry out a targeted piece of work to review whether low notifications of people from ethnic minority groups and females is reflective of care management data.
Work more closely with STP work streams to improve pathways for people with Learning Disabilities and with Primary Care Networks to support knowledge of local initiatives and provide training.
Work more closely with Public Health commissioners to ensure people with a learning disability are included in the development of health improvement initiatives.
Develop closer links with Community Navigators and Social Prescribing programmes to ensure people with a learning disability have full access to these services.
Ensure good practise examples are shared and embedded across all services.
Consider measures/ tools to evidence progress and improvement to services and reduction in health inequalities.

P a g e | 35
5.13 LeDeR
Continue to facilitate an effective LeDeR Steering Group and Improving Health Outcome Group.
Operate an action plan to manage and monitor outcomes of LeDeR reviews.
Continue to improve the completion rate of reviews so that all reviews in scope are completed within 6 months.
Produce an Annual Report based on 2019/20 outputs and findings.

P a g e | 36
CHAPTER 6 – Conclusion: The Future of LeDeR It is unclear whether there will be ongoing funding from NHS England to support the sustainability of the programme, however The NHSE Long Term Plan does refer to the ongoing delivery of the programme. Hertfordshire will continue to support the LeDeR programme with the recruitment of a Local Area Contact to manage the programme and work closely with the Learning Disability Commissioning Managers responsible for Improving Health Outcomes going forward. Whilst the Improving Health Outcomes Action Plan continues to develop, further evidence needs to start being collected to ensure that activity being worked on is actually making a difference. In addition to questionnaires, case studies and anecdotal feedback, how progress is measured needs further consideration. Going forward actions will be categorised by immediate, medium and long-term impact. As this Hertfordshire Annual Report illustrates, findings from the Hertfordshire data is comparable to the data included in the National LeDeR report. Given the findings of Hertfordshire LeDeR, the programme has been instrumental in identifying gaps in provision, practise issues and limited monitoring of service delivery. This information is already seen to be supporting commissioners and key stakeholders in directing change which hopefully will demonstrate both short-term and long-term benefits to people with learning disabilities living in Hertfordshire. Hertfordshire remains committed to the LeDeR programme and recognises the benefits it brings to identifying why people with a learning disability are dying prematurely. Whilst the term LeDeR is over-arching and has become a process, through the evidence gained from reviews it has created a springboard to influence change locally.

P a g e | 37
Appendix 1 Glossary of terms ADS Adult Disability Service
AHLT Acute Health Liaison Team
ATP Assistant Therapy Practitioner
CCG Clinical Commissioning Group
CHIT Care Improvement Team
CLCH Central London Community Health Trust
CLDT Community Learning Disability Team
DOLs Deprivation of Liberty Safeguards
ENHCCG East and North Hertfordshire’s Clinical Commissioning Group
ENHNT East and North Hertfordshire’s NHS Trust
HAAARC Hospital Admissions Avoidance Ambulance Response Car
HCC Hertfordshire County Council
HCPA Hertfordshire Care Providers Association
HCT Hertfordshire Community Trust
HLT Health Liaison Team
HPFT Hertfordshire Partnership Foundation Trust
HQIP Healthcare Quality Improvement Partnership
HVCCG Herts Valleys Clinical Commissioning Group
LD Learning Disabilities
LeDeR Learning Disability Review of Mortality
NHSE Nation Health Service (England)
QOF Quality Outcomes Framework
STAMP Supporting Treatment and Appropriate Medication in Paediatrics
STOMP Stop the over medication of people with a learning disability, autism or both with psychotropic medicines
STP Sustainability and Transformation Partnerships
TCP Transforming Care Programme
WHHT West Herts Hospital Trust

P a g e | 38
Appendix 2: Acknowledgements Report contributors: Adefunke Eriolu Strategic Liaison Nurse for Secondary and Tertiary Care Anne Hunt Lead Sepsis Nurse, Lister Hospital Bernadette Herbert Adult Safeguarding Nurse for E&N Herts NHS Trust Bonita Sparkes Clinical Nurse Specialist, Safeguarding Team, WHHT Clare Thompson Lead for Speech & Language Therapist, HPFT Dawn Bailey Named Nurse for Safeguarding Adults, WHHT Dr Vicky McCulloch Clinical Lead LD, HVCCG Elaine Scott Commissioning Officer LD, HCC Hansa Nariapara Commissioning Officer LD, HCC Hilary Gardener Strategic Liaison Nurse for Primary Care, HCC Karenann Spicer Director of Education Research, Hospice of St Francis Kathryn Dempsey Local Area Contact for LeDeR, HCC Katie Wallace Programme Manager, Public Health, HCC Liz Kenyar Support Officer Louise Jenkins Strategic Lead Nurse Manager, HCC Monika Kalyan Equality & Diversity Lead, HCT Una Monaghan Clinical Director, Herts Special Care Dental Service, HCT

P a g e | 39
Appendix 3: Links to resources and further reading https://www.england.nhs.uk/learning-disabilities/improving-health/annual-health-checks/ (Guidance, advice and support materials for annual health checks for people with learning disabilities) https://www.gov.uk/government/publications/learning-disability-applying-all-our-health (Evidence and guidance to help healthcare professionals to improve the health and wellbeing of people with learning disabilities.) https://www.nice.org.uk/guidance/qs187 (Guidance on looking after people with learning disabilities as they grow older) https://www.england.nhs.uk/publication/improving-identification-of-people-with-a-learning-disability-guidance-for-general-practice/ (NHS England has published some guidance on how to improve the identification of people with a learning disability in order to improve the health and wellbeing outcomes.) https://www.hertfordshire.gov.uk/services/adult-social-services/disability/learning-disabilities/learning-disability-partnership-board/learning-disability-mortality-review-leder-programme-information-for-professionals-and-carers.aspx
(LeDeR HCC Page)
https://www.youtube.com/watch?v=Sw0nfCJ7Ftc (Sepsis video starring Purple all Stars) https://youtu.be/6XM6wLe8u6Q (Sepsis information for family and carers of people with a learning disability) https://www.hertfordshire.gov.uk/services/adult-social-services/disability/learning-disabilities/my-health/my-health.aspx (Hertfordshire website for people with learning disabilities and their families/ carers with guidance and information on looking after their health) https://www.hertfordshire.gov.uk/services/adult-social-services/disability/learning-disabilities/my-health/information-for-professionals.aspx (Hertfordshire website for professionals to support people with learning disabilities)
www.bristol.ac.uk/sps/leder/ (LeDeR Programme website) www.gov.uk/government/collections/reasonable-adjustments-for-people-with-a-learning-disability (Guides on how reasonable adjustments should be made to health services and adjustments to help people with learning disabilities to access services.) https://www.btm.org.uk/wp-content/uploads/2018/05/Understanding-Constipation-high-res.pdf (Easy read guide to understanding constipation) https://www.bristol.ac.uk/medialibrary/sites/cipolearningdisabilities/migrated/documents/fullfinalreport.pdf (CIPOLD Report (2013) )

P a g e | 40
Appendix 4: For more information about IHOG or LeDeR Hertfordshire LeDeR Programme Tracey Brennan Commissioning Manager/ LeDeR Lead, Integrated Health and Care Commissioning Team SFAR224 2nd Floor, Farnham House Stevenage, SG1 2FQ Hertfordshire County Council The LeDeR e-learning course link to become a trained reviewer: www.lederlearning.co.uk :

P a g e | 41
Appendix 5
Steering Group Terms of Reference
Hertfordshire
AMENDMENT HISTORY
VERSION DATE AMENDMENT
1 16/1/17 18/5/17
2 18/5/17 2/2/19 3 2/2/19 15/3/19
4 15/3/19
Terms of reference
This document sets out the standard terms and background that will apply to all meetings.
Background
The Learning Disability Mortality Review (LeDeR) Programme, delivered by the University of Bristol,
is commissioned by the Healthcare Quality Improvement Partnership (HQIP) on behalf of NHS
England.
The aim of the programme is to drive improvement in the quality of health and social care service
delivery for people with learning disabilities and to help reduce premature mortality and health
inequalities in this population, through mortality case review. These reviews are intended to
support health and social care professionals, and policy makers to clarify the contribution of various
causes of death to the overall burden of excess premature mortality for people with learning
disabilities; identify variation and best practice; and identify key recommendations for
improvement.
The programme will complement and contribute to the work of other agencies such as the Learning
Disability Public Health Observatory, academic research studies, NICE, the CQC inspection
programme, Local Government Associations, The Transforming Care (Winterbourne View)
Improvement Programme, and Third sector and voluntary agencies.
The scope of the local reviews of deaths
The LeDeR Programme will support reviews of deaths of people with learning disabilities aged 4 and
over who are registered with a GP in Hertfordshire, England at the time of their death.
The Programme will support reviews of all deaths, irrespective of the cause of death or place of
death.

P a g e | 42
Name of group
Hertfordshire LeDeR Steering Group
Purpose / role of the group
In partnership with stakeholders to identify and work with, the Regional Area contact who
will have strategic oversight of the programme activities in the local area.
To act as the responsible representatives for the programme on behalf of their organisation.
Representatives from health and social care will commit to supporting the participation of
local reviews of deaths of people with learning disabilities.
To help interpret and analyse the data submitted from local reviews, including areas of good
practice in preventing premature mortality, and areas where improvements in practice
could
be made.
To monitor the action plans that are developed as a result of the reviews of deaths, and take
or guide appropriate action as a result of such information within steering group members
own organisations.
To ensure agreed protocols are in place for information sharing, accessing case records and
keeping content confidential and secure
Membership
In Hertfordshire representation of the LeDeR programme includes:
Commissioners both Local Authority and Clinical Commissioning Groups
Primary and secondary healthcare
Family carer
Expert by experience
Community Learning Disability Team, Social care
Community Learning Disability Team, Health
Provider organisations – Hertfordshire Care Providers Association
HealthWatch
Regional LeDeR lead
Local Area Contact
Additional Attendees Observers will be allowed to attend meetings with agreement of chair
Additional, co-opted attendees will be identified prior to meeting and requested to attend
for specific purposes

P a g e | 43
Role of Members
Members review programme direction and make decisions to make sure that:
Partners work together to support the success of the project and make sure that no single
interest will undermine the programme.
All risks are assessed and managed well, putting in place actions and contingency plans for
all high impact risks.
Recording of programme information is accurate and coherent.
Support is available for the Local Area Contact.
The progress of the overall programme is monitored, and any remediable action is
undertaken.
Governance
Confirmation around the use of the S251 has been given.
Information is kept securely
Reviews are redacted by the time they are presented to the Steering Group
The group provide reports to Regional LeDeR Programme Lead; Transforming Care Board; All age Safeguarding Board
Focus on specific issues, which may be delegated to resolve / approve specific actions will be given to the ‘Improving Health and Lives’ group.
The Quorum shall be ‘representation’ from ENHCCG or HVCCG (or a member who covers both);
all Trusts commissioned in Hertfordshire; Social Care, and an expert by experience (person with a LD
or family carer). If named members are unavailable, a deputy should be attendance.
Meeting frequency
Meetings to be held every 2 months
Notification and recording of meetings are the responsibility of the Integrated Health and
Care Commissioning Team
Papers to be circulated one week prior to the meeting wherever possible
Meeting chaired by Dr. Kirsten Lamb.
Deputy Chair is TBC
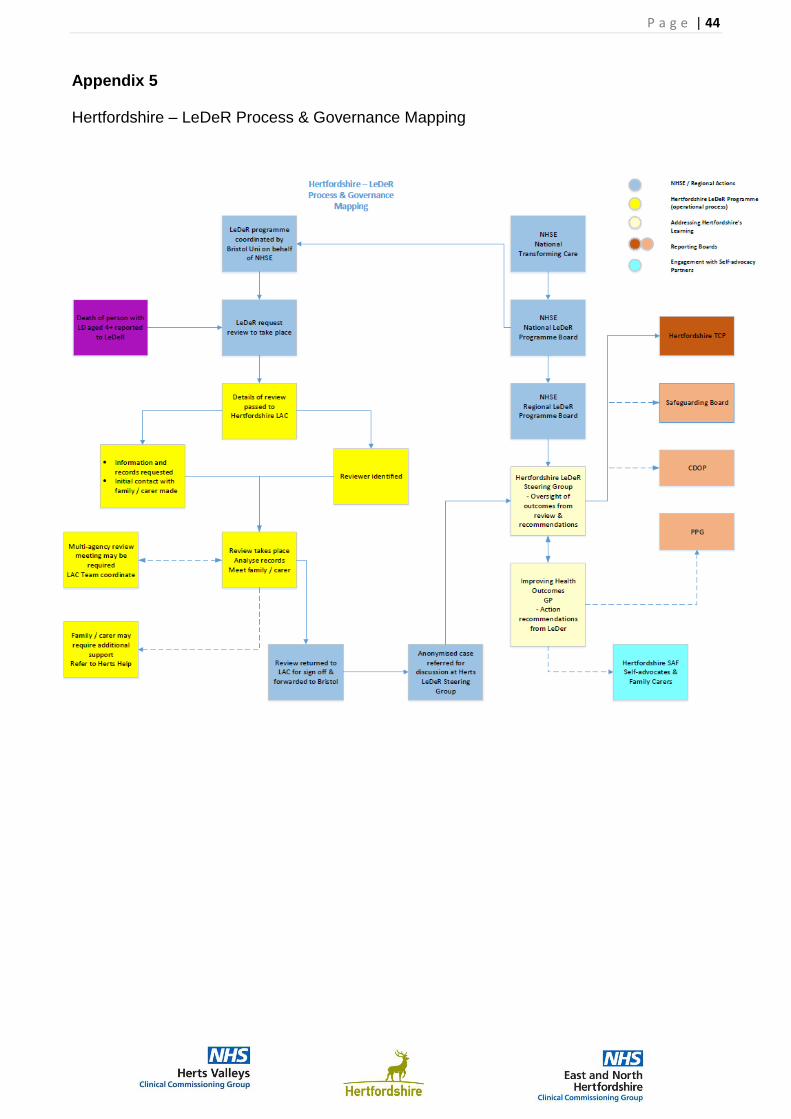
P a g e | 44
Appendix 5 Hertfordshire – LeDeR Process & Governance Mapping

P a g e | 45
Appendix 6 Total population of Hertfordshire with the following parameters taken from HCC data: List of service users open to the Adult Disability Service living in Hertfordshire where the primary need is a Learning Disability:

P a g e | 46
Appendix 7
Case Studies and Reflection from the ABC4LD education Project.
Helen Miller, Educational Specialist, Isabel hospice 25/07/2019
Before the ABC4LD training commenced there was an unexpected death in the care home of a longstanding elderly resident. Even though a DNACPR was in place staff panicked and called emergency services. This event was traumatic for staff. On reflection with the management, there were signs in the last weeks of life that the very elderly resident was deteriorating and could be in the last months of life. In contrast just before the second cohort of teaching another long-term elderly resident was admitted to hospital and then discharge back to the care home for end of life care with the support of the district nursing team. Care home management noted increased confidence and communication skills when co-ordinating and planning care for this resident. The death of this resident in contrast was peaceful, with two member of staff each holding one of the resident’s hands while they died; their favourite classical music playing in the background. The window was then opened for the resident’s soul to leave the room after they died. One of the staff present was also present at the death of the first resident, she reflected on the positive effect of being able to support this ‘Good death’ and how the training had helped her.
The care home has another palliative care resident. Care home management fed back how the education project has opened up the topic of palliative care generally amongst staff. Staff discussing and alert to increased bereavement support that the other residents may need, especially to nonverbal bereavement distress. Staff have produced remembrance material for the care home of the residents who have died.
Reflecting on education given around pain control in nonverbal residents. Staff noted a resident was often agitated on rising each morning and reluctant to get washed and dressed. They were on regular paracetamol four times a day for generalised stiffness and possible joint pain. The first dose of paracetamol was given at breakfast after washing and dressing. Reflecting on the possible stiffness first thing in the morning, the paracetamol was given half an hour before the patient was asked to get up to be washed and dressed. There was a marked drop in the resident’s agitation once this regime was adopted, improving resident care and staff time management.
A palliative care resident with dementia. Only family live in Australia. Family visited resident yearly (during education programme). Care home demonstrated excellent advance care planning implementation. Arranging MDT meeting while family present and discussing resident’s preference and wishes for the future. Family complied a very large photo album with attached dialog around each photo. This has proved most therapeutic for the resident and has improved communication skills between staff and the resident. This album will be able to be used for reminiscence therapy as the dementia progresses. DNACPR, Advance care planning and funeral plans now in place.
One of the Attached GP practices is working towards its purple star award. The care home is sharing the knowledge from this education programme with them and some of the easy read documents they have been given.

P a g e | 47
One link GP practice employees a pharmacist. Care home management will ensure at resident’s annual review that GP’s are made aware of any advance care planning and that medication is reviewed with pharmacist.
Care home management had reviewed the need to be more alert to absorption of PEG feeds and medication in palliative care patients. They are now aware of the potential need to have a plan for palliative care residents who are being PEG fed on, nutrition, hydration and medication delivery; especially those who are suffer from epilepsy. Following education, the care home sent a SALT team request to review a resident.
Care home staff advised education had improved assessment skills. Reviewing agitation in a non-verbal resident first thing in the morning, noted agitation linked with constipation. Laxatives prescribed and agitation reduced.
Care home staff report following education, a nonverbal resident was admitted to hospital, they reflected on the importance of handing over his detailed body language to hospital staff thus aiding communication and care.
Care home staff on reflection commented on the importance of supporting other residents when another resident dies in the care home. They were not aware of bereavement services available. They identified one resident with behavioural issue post bereavement and the possible need for further support.
On the topic of pain control, in many of the homes staff reported district nurses attending residents to perform wound care. None of these visits were timed, so staff could not give analgesic in anticipation of the wounds being dressed. Hence staff gave analgesic once the dressing was completed and the patient was noted to be in pain. All staff were educated on the possibility to request a timed visit within a 2-hour window from the district nursing service to allow analgesic to be given before the visit if this would have the potential to reduce pain and distress caused by wound care.