kerry general hospital annual report 2013 · this report is an attempt to ensure that every member...
TRANSCRIPT

1
KERRY GENERAL HOSPITAL
Annual Report
2013
2
FOREWORD: .....................................Error! Bookmark not defined. HOSPITAL PROFILE......................................................................4 ORGANISATIONAL STRATEGIC OBJECTIVES ..............................7
EMB PRIORITIES FOR 2014……………………………………….………. ...8 QUALITY AND PATIENT SAFETY .................................................9 RISK MANAGEMENT...................................................................13 HYGIENE SERVICES AND INFECTION CONTROL ......................19 THE RADIOLOGY DEPARTMENT ................................................21 THE SPEECH AND LANGUAGE DEPARTMENT...........................22 THE PHYSIOTHERAPY DEPARTMENT........................................24 THE AUDIOLOGY DEPARTMENT ................................................26 HOUSE KEEPING SERVICES. .....................................................27 THE OCCUPATIONAL THERAPY DEPARTMENT.........................29 THE NURSING DEPARTMENT.....................................................31 THE PASTORAL CARE DEPARTMENT. .......................................33 THE PATHOLOGY DEPARTMENT. ..............................................34 THE MEDICAL RECORDS DEPARTMENT. ...................................36 THE DIETETIC DEPARTMENT.....................................................37

3
Foreword: This report is an attempt to ensure that every member of staff in Kerry General Hospital has an awareness of what is happening across each and every department within the hospital in terms of activities for last year but more importantly targets and goals for this year. This Report isn’t about blinding us with number and statistics. It is an attempt to ensure that all of our staff know and understand what is happening across the hospital. We have attempted to keep the information for each department consistently formatted such that we can all look to each department under the various headings and have a consistent understanding of what is being said. We have also tried to keep the document as brief as possible such that people are getting the message without having to read through reams of narrative. Each department has prepared their submission included in the attached. We are grateful to all for the time and effort put into preparing each and everyone of the attached reports. The single most important resource in any organisation is it’s people. We have fantastic people in KGH who on a daily basis do extraordinary things to support the public that we serve. It is absolutely imperative that each and everyone of our staff members know and understand what our organisational goals are and understands why it is critical that we all play our part in achieving those goals. Hence the importance of making sure that all of our people know and understand what those goals are as we can’t expect people to contribute to the achievement of them if they don’t know what they are in the first instance. We want to acknowledge the work done last year by you all in difficult circumstances. We are extraordinarily lucky in this hospital to have so many committed and skilled people who go the extra mile every day to deliver the highest possible quality of service to our public. We hope that you will take the time to read through the attached document. We also hope that you will take some benefit from the contents such that your understanding of the work that is ongoing across the organisation is broadened. This entire exercise is essentially about attempting to inform you about what is happening in your workplace. We look forward to the year ahead and the many challenges that we will face. Please be assured of our continued support and thanks again for your ongoing commitment to the public that we serve. Regards, Regards,
__________________ ________________________________ Mr TJ O’Connor Dr Helena Moore, General Manager, Clinical Director Kerry General Hospital. Kerry General Hospital
4
HOSPITAL PROFILE Kerry General Hospital is the third largest of the Health Service Executive – Southern Area’s seven acute hospitals. The hospital provides acute general hospital services to the population of Co. Kerry (145,0481) and additionally to a proportion of the populations of West Limerick and North Cork. Equally of essence in the context of delivery of quality & safe services are the demographics unique to Kerry. The population of the catchment area has grown during the intervening decades since the hospital first opened its’ doors in 1984. In 2002, the census population of Kerry was calculated at 132,000 and the 2006 census put the population at 139,000. However more noteworthy than the overall increase in the size of the population is the increase by 20% of our elderly population (over 85 years). The increase in this cohort of the population in Kerry is the highest increase nationally. In addition, the Kerry area has quite a large visiting population – Bord Fáilte/ Shannon Development estimate there are approximately 2 million tourists visiting this region annually, principally during the summer months. The core of our services is the provision of emergency and unplanned specialist care, 24 hours a day, every day of the year. From that core is built a comprehensive medical and surgical investigation, diagnosis and treatment for physical illnesses or conditions, injuries or disease for adults and children. Further specialisation is delivered in a small number of areas e.g. care of those with cancer, renal dialysis care. The breadth and depth of services at Kerry General Hospital supports a holistic “whole patient” approach to care by allowing immediate and easy involvement of different specialists in any patient’s care. There are presently a total of 306 beds in KGH. The breakdown is as follows:
226 inpatient beds 16 day procedure beds 8 AMAU beds 44 mental health beds 9 ICU/CCU beds 12 escalation beds.
Please see below the activity for 2013: Activity Number Inpatient discharges 13,198 Day Cases 10,871 Emergency Presentations 36,517 Outpatient Attendances 54,014 Please see the table below showing what was spent in 2013 and the overrun: Spend for 2013 84 million Including overrun 1.875 Please see table below for WTE numbers at the end of 2013. Date: end 2013 WTE: 902 It is proposed to develop new clinical divisions in 2013 at KGH in line with HSE guidelines, which will provide the framework around which issues of safety, quality and accountability can be developed. This is intended to drive a culture of clinical effectiveness, audit and best practice linked in with the National Clinical Care Programmes and any other evidence, international or otherwise, that provides for safe and effective standard of care.
1 CSO – 2010 census figures
5
The Mission of Kerry General Hospital, which is reflective of the HSE mission, is “To enable people to lead healthier and more fulfilled lives in Kerry, North Cork and West limerick and provide services within a culture of kindness, consideration and respect of each individual” Vision: Our vision is to provide patient centred care at the right time in the right place by the right people. The values of Kerry General Hospital: Respect: Valuing patients / clients and each other. Recognise the fundamental worth of people through trust, courtesy, kindness, consideration, mutual communication and collaboration.
Fairness and Equity: Providing health and personal social services based on need and striving for an equitable health service.
Excellence: Striving for the highest level of achievement in all aspects of our work.
Leadership: Directing the future of the HSE.
Accountability and Responsibility: Honesty, consistency and accountability in decisions, words and actions.
A full range of Specialties, Specialist Out-Patient Services provided by visiting Consultants and Support Services provided at KGH can be found below:
The following Specialties are provided:-
Emergency Medicine Ear, Nose & Throat Services General Medicine including Medicine of the Elderly & Endocrinology General Surgery Gynaecology (Colposcopy & Urodynamics) Obstetrics Orthopaedics Paediatric including Special Baby Care Unit Pathology Psychiatry Radiography including C.T. Scanning Service. Renal Dialysis Satellite Unit Oncology Satellite Unit Palliative Care
The following additional Specialist Out-Patient Services are provided by Visiting Consultants: - Dental Dermatology Nephrology Neurology Oncology Ophthalmology Plastic Surgery Rheumatology S.T.D.
SUPPORT SERVICES ARE PROVIDED AS FOLLOWS: -

6
Audiology Diabetics Endoscopy Suite Medical Assessment Unit Occupational Therapy Out-Patient Department Physiotherapy Speech and Language Therapy
The National clinical care programmes: The programmes support the premise that hospital resources are utilised to ensure that patients receive the best possible clinical outcomes. The programmes will enable the hospital to maximise activity whilst reducing overall cost and head count. In 2013, the following Clinical Care Programmes are being implemented:
Diabetes Stroke OBSGYNAE (Obstetrics & Gynaecology) Acute Coronary Syndrome Elective Surgery Acute Medicine Emergency Medicine programmes
OUR STRATEGIC OBJECTIVES Kerry General Hospital strategic quality objectives have been developed in line with the eight themes of HIQA’s National Standards for Safer Better Healthcare (2012).
1. To achieve person centred care and support that places service users at the centre of all that the service does. It does this by advocating for the needs of service users, protecting their rights, respecting their values, preferences and diversity and actively involving them in the provision of care. Person centred care promotes kindness, consideration and respect for service users dignity, privacy and autonomy.
2. To achieve effective care and support that is delivered consistently and to the best achievable outcomes for the people using our services within the context of the service and the resources available to it. It will be based on National and international best practice and we will evaluate service user outcomes to determine the effectiveness of the design and delivery and will meet the needs of the service users in a timely manner, while balancing the needs of other service users.
3. To ensure the provision of safe care and support and to recognise that safe care is paramount for service users. Steps need to be taken to proactively promote a culture of quality and safety that is embedded in daily practices and processes. We will identify, prevent and minimise risks wherever possible. In the event adverse events do occur and the service user is harmed, we will have formal arrangements in place to respond to this event and support the service user and their family. As providers of high quality safe services we aim to learn from all information relevant to the provision of safe services and from situations where things have gone wrong.
4. To promote better health and wellbeing through our interactions with the population we serve. Through the provision of a high quality, safe and reliable service we will constantly look for ways and opportunities to do this. We will work in partnership with people promoting a culture of better health and wellbeing which will enhance the care we provide enabling people to increase control over their own health and wellbeing and the factors that influence it.
5. To ensure effective leadership, governance and management arrangements are in place thus ensuring a sustainable delivery of safe, effective, person centred care and support. There are clear lines of accountability throughout service provision at individual,

7
team and service levels so that healthcare professionals are aware of their responsibility and accountability to ensure services are planned and managed effectively, efficiently and safely
6. To provide a skilled, knowledgeable competent workforce committed to providing a high quality, person centred and safe service.
7. To use the resources available to us to provide high quality, safe care to support the
services both now and into the future. We aim to plan, manage and deliver service through effective responsible stewardship and decision making on allocation of resources to deliver a high quality, safe and reliable care and support.
8. To use quality information to assist in the planning, managing, delivery and monitoring of healthcare to ensure high quality safe services are provided. Quality information is accurate, valid, reliable, timely, relevant, legible and complete within a information governance framework in line with current best standards and legislative requirements.
Executive Management Board An Executive Management Board for Kerry General Hospital has been established to ensure that Kerry General Hospital is managed in an efficient and effective manner enabling it to provide the highest quality care to the public.
The Objectives of the EMB are as follows:-
Provide direction and leadership to Kerry General Hospital in the attainment of its goals, consistent with the policies of the Health Service Executive.
Manage and develop Kerry General Hospital by – Approving and implementing the Service Plan for Kerry General Hospital. Developing and implementing the appropriate strategies and policies for Kerry General
Hospital. Improve the profile and public perception of Kerry General Hospital at local and national
level. Account for the utilisation of resources and the provision of an efficient and effective
quality service, as agreed in Kerry General Hospital annual service plan. The key priorities for 2014 are: Ensure that both suites in the endoscopy unit are opened and that accreditation is
achieved Implement NEWS/MEWS/PEWS (when available) across the hospital Roll out the new National Consent policy and Open Disclosure policy Ensure that the Major Emergency Plan is updated and communicated appropriately
across the hospital Ensure compliance with good hand hygiene practice Open the “Joint School” and extend anaesthetic involvement on pre operative
assessment leading to an improvement in our AvLos and DOSA rates Introduce and support the maintenance of TARN (Trauma audit and research
network) Introduce and support the maintenance of the hip fracture database Introduce pre operative assessment for all elective admissions Continue to action and monitor the QIPs from the HIQA self assessment commenced
in 2013 Support the theatre review undertaken by the LEAN team and draw up an
implementation plan once the recommendations are received Finalise an agreement with the tertiary referral centre in the SIVUH with regard to a
regional ENT service Implement the recommendations of the catering review finalised in September 2013 Finalise arrangements to move stores off site

8
Develop a UCC funded education centre Progress the agreed move of the laboratory to Loher ward and the associated move
of the oncology department to the vacated laboratory space Address the issue of the storage of medical records Introduce a discharge lounge to assist in bed management Secure the resources to support the introduction of a DEXA scanning service Progress the purchase of a new CT Progress with the introduction of electronic rosters commencing with nursing Ensure that the resources are secured to open the x ray department in ED.
9
QUALITY AND PATIENT SAFETY While 2013 was a challenging year, many improvements in service delivery and quality were evident during the year. Dr Richard Liston has served as Clinical Director for the past five years and his stewardship has seen the integrated nature of service strengthened considerably, providing a more cohesive service delivery model across hospital and community. Dr Liston stepped down from his role as Clinical Director at the end of 2013 but we are sure that this progress will be continued in the future because it is pivotal in ensuring continued close clinical links with local management to optimise patient outcomes. On July 5th Dr Philip Crowley and Dr Mary Browne, HSE National Quality and Patient Safety Directorate visited the health service in Kerry. The visit commenced with a presentation from KGH Clinical Governance Committee followed by a tour of KGH which included the highlighting of improvement initiatives and key risks. This was followed by a visit to Castleisland primary care centre and the day care centre. They were impressed through out their visit by the level of commitment to quality and patient safety in Kerry, whilst also recognising the challenges of he day to day management of quality. The second HSE Kerry Area Quality and Patient Safety awards were held on October 23rd 2013 in the Nurse education Centre, KGH. The theme of the event was “Working together for risk prevention in the Kerry area”. The event attracted 14 presentations and Key note speakers and judges for the event were Dr John Fitzsimons, consultant Paediatrician National Quality and Patient Safety Directorate and Ms Breda Doyle, Best Practice Manager Bons Secours hospital, Tralee. The winning entry was “Advanced Nurse Practitioners-Delivering an autonomous patient care pathway in the Emergency department”. The National Clinical Care Programmes provide an opportunity to foster close multidisciplinary working to ensure the best possible patient outcomes. Under the programmes, Kerry has been fortunate to benefit from the appointment of consultant Dr Haroon, who commenced his rheumatology post in 2013 and will grow this service in the coming year in liaison with his multidisciplinary colleagues. The opening of an additional four beds in AMAU was a welcome development in 2013 which was required under the Acute Medical Programme to ensure the long term viability of KGH as a level 3 hospital. Other initiatives in KGH, such as the Volunteer service, have been instrumental in showing a tangible commitment to improving user service experience. KGH commenced self assessment under the National Standards for Better Healthcare. The standards are grouped under eight themes, four relating to dimensions of quality and four relating to capacity and capability factors. HIQA will monitor compliance of service providers against the standards, which in turn will underpin future licensing of designated healthcare providers. 2014 will bring advancement in the successful completion of the self assessment and the achievement of the numerous quality improvement plans. While many improvements were evident in 2013 thanks to the efforts of all healthcare staff, the planned initiatives for 2014 should enhance services further to ensure the best service delivery possible for all of our clients. HIQA Safer Better Healthcare Standards. The Quality Department led the self assessment of the eight themes of the HIQA standards from July- October 2013. Eight multidisciplinary groups were established and the self assessment completed using the National Quality Assessment and Improvement electronic tool. This self assessment has formed the basis for preparation of evidence and the development of Quality Improvement plans some of which are outlined in this report. A fuller QPS report will be prepared and made available later in 2014. Person Centred Care and Support

10
Comments, Compliments and Complaints management continued to be an excellent source of service user feedback in 2014. Chart 1 and 2 outlines the breakdown of statistics for 2013.
2013 KGH Complaints – Preliminary Summary Statistics only.
17th January 2014. Chart 1.
Complaints received each month
0
2
4
6
8
10
12
Janu
ary
Febru
ary
Mar
chApr
ilM
ayJu
ne July
Augus
t
Septe
mbe
r
Octobe
r
Novem
ber
Decem
ber
Nu
mb
er
79 complaints received in 2013 includes 4 verbal.63 written complaints in 2012 (19% increase)
Chart 2
Categories of complaint
05
10152025303540
1. A
cces
s
2. D
ignity
and
Respect
3. S
afe
and
Effecti
ve C
are
4. C
ommunic
ation an
d Inf
ormatio
n
5. P
artic
ipati
on
6. P
rivac
y
7. I
mpr
oving
Healt
h
8. A
ccou
ntabilit
y
9. O
ther
Nu
mb
ers
Other methods of service user feedback were explored with a Service User Feedback group being established. This group were responsible for leading the Service User Survey 2013 where the NHS survey tool was adapted and administered to 144 adult in-patients by KGH volunteers and some staff. Further surveys are planned in 2014 focussing on maternity services and staff experience. Survey findings will be analysed

11
in line with the eight principles of the HSE Healthcare Charter which the QPS continued to support the implementation of in 2014. KGH Also took part in the National 2013 Patient Safety Culture survey, results are due in 2014. Leadership, Governance and Management The QPS Office led the roll out of the HSE National Guidance document such as Terms of Reference for Quality and Patient Safety Committees, the Safety Pause and QPS walk round as well as the QPS prompts for governance groups. These are recommended to form the basis of individual team/departments/specialty agendas. Visit from Dr Phillip Crowley and Dr Mary Browne, HSE National Quality and Patient Safety Directorate On July 5th 2013 Dr Phillip Crowley and Dr Mary Browne visited the Health service in Kerry. The visit commenced with a presentation from KGH Clinical Governance Committee followed by a tour of KGH where improvements initiatives and key risks were highlighted to them. They then visited Castleisland Primary Care Centre and the Castleisland Day Care Centre. They were impressed by the level of commitment to quality and patient safety in Kerry while recognising the challenges the day to day management of quality faces e.g. implementation good practice in hand hygiene, integration of services. They are committed to supporting the service in Kerry in particular with the implementation of the HIQA Safer Better Healthcare Standards.
Workforce Several training events for Quality and safety improvement were co-ordinated in 2014 by the QPS office. KPI’s: QPS Train gin 2013: Open Disclosure OD information sessions held on 18th June 2013 – 70 staff attended OD information sessions held on 2nd October 2013 – 22 staff attended OD Practical training workshop on 2nd October – 17 staff attended OD Practical training workshop on 3rd October – 18 staff attended PPPG Training 26 attended the PPPG training Clinical Audit Training 57 attended Clinical Audit training for 2013.
HSE Kerry Quality and Patient Safety Awards 2013
The second HSE Kerry Area Quality and Patient Safety Awards were held on October 23rd 2013 in the Nursing Education Centre, Kerry General Hospital, Tralee, Co Kerry. The theme of the event was: “Working Together for Risk Prevention in the Kerry Area” The winning entry was ‘Advanced Nurse Practitioners – Delivering an autonomous patient care pathway in the Emergency Department’, presented by Joseph Coolahan, Registered Advanced Nurse Practitioner, KGH on behalf of the Advanced Nurse Practitioner Service, Emergency Department, Kerry General Hospital. We would like to congratulate Mr Coolahan and the team
12
on their achievement. The Keynote speakers and judges for the event were Dr. John Fitzsimons, Consultant Paediatrician, National Quality & Patient Safety Directorate and Ms. Breda Doyle, Best Practice Manager, Bon Secours Hospital, Tralee. Their addresses outlined the importance of quality in the healthcare environment and key challenges in meeting accreditation requirements in healthcare. We would like to congratulate everyone who took part in the event. There were 12 entries in total of very high standard, representing initiatives across hospital and community. The full list of entries are as follows and if you would like to get a copy of the presentation/abstract or follow up with the presenter please contact Majella Daly, Quality Manager in the Office of Quality and Risk [email protected]. Entries: Poster Presentations 1. PHN Best Practice initiatives in supporting breast feeding mothers 2. Time and space for carers in Kerry 3. Mothers care for their babies but who cares for the mothers? 4. An audit of the availability and provision of written head injury advice to patients being
discharged from the emergency department of Kerry General Hospital 5. Treatment of Gastroenteritis in Paediatrics-----Audit 2013 Abstract Title 6. Universal newborn pulse oximetry measurement in newborn infants in a regional hospital 7. UTI in children & emperical choice of Antibiotics 8. Retrospective study looking at the use of hypertonic saline nebulisers vs. normal saline
nebulisers in infants with bronchiolitis in a regional hospital 9. Retrospective study looking at the admission criteria to special care baby unit with infant
of diabetic mother in a regional hospital 10. Multidisciplinary Intradepartmental Audit in Improving Quality of written Inpatient Drug
Kardex in KGH, Tralee 11 Advanced Nurse Practitioners – Delivering an autonomous patient care pathway in the
Emergency Department 12. Every baby in Kerry will experience skin to skin and colostrum, 13. Efforts to Improve Caseload on waitlist for Audiology 14. Incident and non-conformance management in Pathology, KGH The organising committee would like to extend their thanks to all who participated in the event and made it a success, presenting a diverse range of initiatives in the current challenging climate which evidence both quality improvement for service users and overall cost effectiveness.

13
RISK MANAGEMENT The staff of the Quality and Safety Department has an area wide remit which encompasses Kerry General Hospital and all community facilities. Within the Quality and Patient Safety Department, the Risk Manager operates within set of operational guidelines in order to support the work of the Quality Manager but also to ensure a high level of service availability to staff at clinical level. In this context, the Mission Statement of the Quality and Patient Safety Department is itemised below. In addition, the Risk Manager also functions as the Document Controller for policies and procedures for the hospital and authorises them to be placed on the staff noticeboard.
Mission Statement of the Quality and Patient Safety Department
The Quality and Patient Safety Department of the Kerry Area aims to Assist and support the development of the clinical governance framework
and agenda to support quality and patient safety in the Kerry Area. Develop systems for a people centred approach.
Standardise Quality Systems. Support and direct optimum patient safety programmes. Ensure that evidence and strategic objectives underpin all planning and
quality improvement. Focus on integrated Risk Management processes (clinical and non
clinical). Develop and direct proactive Risk Management processes.
Monitor the implementation of recommendations from reviews/incidents to
foster a system wide approach their operationalisation. Establish systems to ensure that learning from complaint, incident reviews,
and audits are disseminated and shared across the Kerry Area, regionally and nationally.
To facilitate the development of a quality/ safety culture through the
dissemination of information, education and training placing the patient at the centre of all endeavours.
Support staff at all levels in preparation for the requirements of external
accreditation processes.
The work of the Risk Manager involves risk management both proactively and reactively. Incident Management will be discussed initially.

14
Person centred care: Explanatory leaflets have been developed and placed on the portal for staff on incident investigations and patient advocacy organistaions. In addition, the QPS newsletter is issued three times per year to provide updates on activities and archived copies are available on the portal. Effective Care: The Quality Manager is co-ordinating the compilation of the Clinical Audit programme for the organisation and has been involved in the co-ordination of the 2013 In Patient Survey and the Patient Safety Culture Survey. The assistance of the volunteers in this initiative is greatly appreciated. Safe care and support:
Incident Management The department co-ordinates the daily management of the incident reporting system, it provides feedback on emerging trends to various fora such as the KGH/CGC Committee, the Area QPS committee and the relevant governance groups for the respective areas throughout the hospital in order to enhance the integration of quality and safety to the organisation and quarterly trends are placed on the staff noticeboard to enable staff feedback. (Such feedback is itemised in the graphs below)
Incident Trend Feedback
Overall Area Rates
Incident reporting rates for the Kerry area have more than doubled since 2012 figures with almost 2500 incident s reported and KGH 2013 figures exceeding those for the whole area in 2012.
15
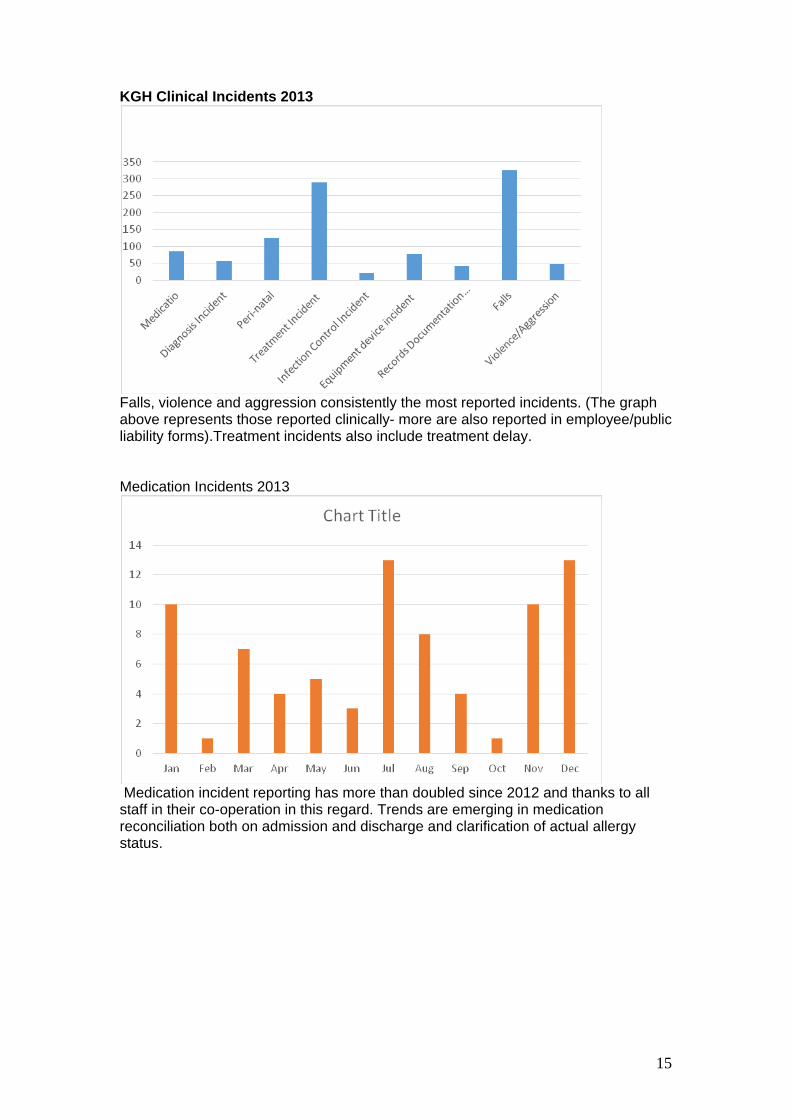
KGH Clinical Incidents 2013
Falls, violence and aggression consistently the most reported incidents. (The graph above represents those reported clinically- more are also reported in employee/public liability forms).Treatment incidents also include treatment delay. Medication Incidents 2013
Medication incident reporting has more than doubled since 2012 and thanks to all staff in their co-operation in this regard. Trends are emerging in medication reconciliation both on admission and discharge and clarification of actual allergy status.
16
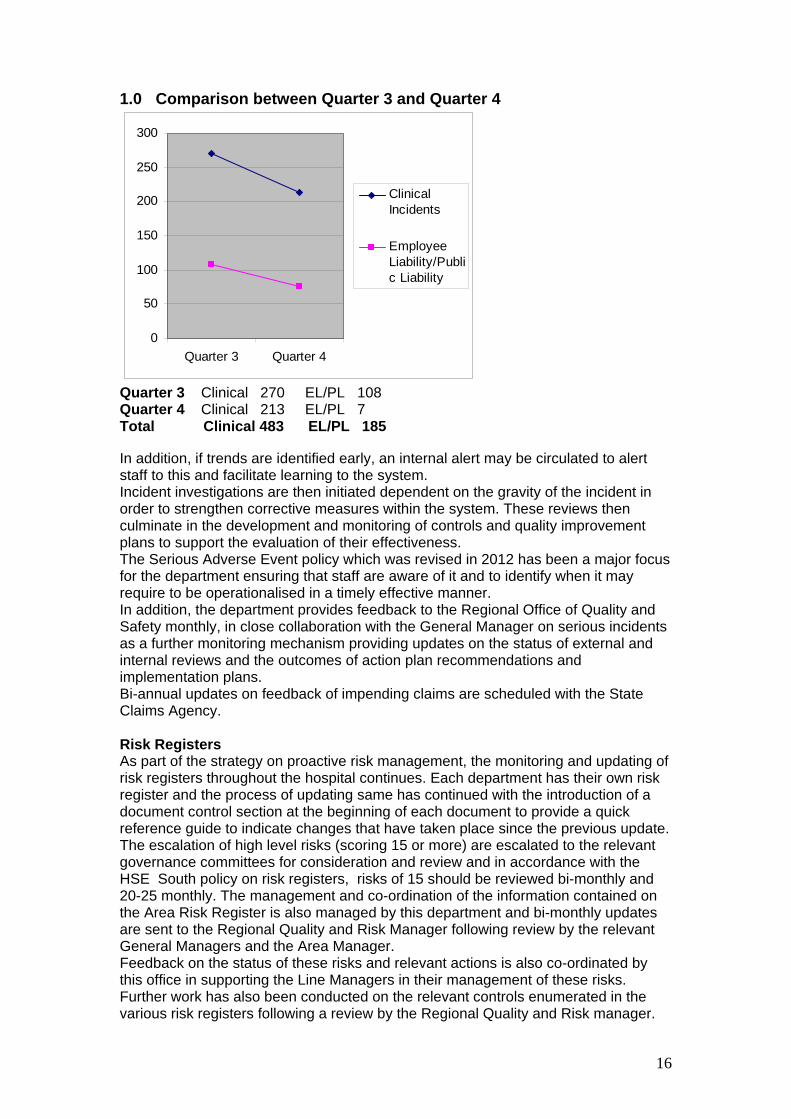
1.0 Comparison between Quarter 3 and Quarter 4
0
50
100
150
200
250
300
Quarter 3 Quarter 4
ClinicalIncidents
EmployeeLiability/Public Liability
Quarter 3 Clinical 270 EL/PL 108 Quarter 4 Clinical 213 EL/PL 7 Total Clinical 483 EL/PL 185 In addition, if trends are identified early, an internal alert may be circulated to alert staff to this and facilitate learning to the system. Incident investigations are then initiated dependent on the gravity of the incident in order to strengthen corrective measures within the system. These reviews then culminate in the development and monitoring of controls and quality improvement plans to support the evaluation of their effectiveness. The Serious Adverse Event policy which was revised in 2012 has been a major focus for the department ensuring that staff are aware of it and to identify when it may require to be operationalised in a timely effective manner. In addition, the department provides feedback to the Regional Office of Quality and Safety monthly, in close collaboration with the General Manager on serious incidents as a further monitoring mechanism providing updates on the status of external and internal reviews and the outcomes of action plan recommendations and implementation plans. Bi-annual updates on feedback of impending claims are scheduled with the State Claims Agency. Risk Registers As part of the strategy on proactive risk management, the monitoring and updating of risk registers throughout the hospital continues. Each department has their own risk register and the process of updating same has continued with the introduction of a document control section at the beginning of each document to provide a quick reference guide to indicate changes that have taken place since the previous update. The escalation of high level risks (scoring 15 or more) are escalated to the relevant governance committees for consideration and review and in accordance with the HSE South policy on risk registers, risks of 15 should be reviewed bi-monthly and 20-25 monthly. The management and co-ordination of the information contained on the Area Risk Register is also managed by this department and bi-monthly updates are sent to the Regional Quality and Risk Manager following review by the relevant General Managers and the Area Manager. Feedback on the status of these risks and relevant actions is also co-ordinated by this office in supporting the Line Managers in their management of these risks. Further work has also been conducted on the relevant controls enumerated in the various risk registers following a review by the Regional Quality and Risk manager.

17
Red Risk review meetings have been scheduled to strengthen the process of review of red risks for departments-these meetings are held quarterly and are attended by the General Manager, Clinical Director, Director of Nursing and Midwifery and the Quality Manager. The dissemination and completion of business continuity plans for each department according to the HSE template is in progress as many departments had such plans in situ in various templates as contingency measures.
Alerts Alerts from both external and internal bodies are co-ordinated through this office and this process has been extended to facilities in the community also to ensure a standardised approach. Alerts are received from the IMB,IMSN(Irish Medication Safety Network) among others. In addition, alerts are also disseminated through this office following emerging incident trends flagged by relevant governance committees. Examples include alerts from the Infection Control Committee and the Drugs and Therapeutics committee. The figures outlined below enumerate the number of alerts circulated from either external bodies or internally by relevant Governance Committees.
KGH Recall Notices issued 102: 2013 External Medical Device Alerts – 2013/79 Irish Medicines Board – 2013/10 Food Safety Authority – 2013/20 Internal Clinical Governance Committee-2 Joint Infection Control Committee- 2 Infrastructural Safety and Risk Committee-1 Drugs and Therapeutics Committee- 1 Policies and Procedures The following policies have been placed on the KGH portal/notice board and have been disseminated to other areas to ensure all staff are aware of these. QPS 007 - Policy and Guidance for the management of Risk Registers in the HSE South. QSRF 008 - Management of Internal and Externally generated safety and device alerts QSRF 016 - Reporting incidents to the Coroner’s office QSRF 022 - Quality and Safety prompts for multidisciplinary teams ISA 005 - Serious Adverse Event Management OPSD-GL-Guidelines for System Analysis Investigation of Incidents and Complaints OQR032 - Business Continuity Management policy OQR033 - Business Continuity Management-Guidance for policy implementation Patient Identification policy Protected Mealtimes Policy Training Training on Incident management and Risk Management processes was delivered in 2013 to 58 staff comprising nursing, nursing students, speech and language therapists. Evaluations conducted on these sessions were positive. Better health and well being:

18
The Quality Manager has now taken on the Chairperson position of the Joint Health Promotion Committee and the Risk Manager has always been member of this committee. Key Initiatives undertaken in 2013 included the introduction of the Protected Mealtimes Policy and the revision of the Health Promotion Policy in addition to the compilation of a work plan for the committee. Leadership, governance and management The Quality and Patient Safety Department advocate the initiation of the Quality and Safety Walk rounds and the introduction of the safety pause as advised by the National Director of Quality and Patient Safety. Workforce: The Quality and Risk Manager work closely together to ensure reviews/responses to complaints are completed in a timely manner. IN addition, in relation to the standards, the Quality Improvement Plan in relation to garda vetting of all employees has been identified.
Key Priorities for 2014 :
Advancing the introduction of the National Policy and Guidance on Open Disclosure.
Strengthen the process of review of risk registers and feedback on progress of escalation of key risks.
Continue to support the preparation of staff for the HIQA Safer Better Healthcare Standards.
Advance the implementation of the National Consent policy and associated documentation.
Support departments in the transition to the National Adverse Event Management System as itemised by the Clinical Indemnity Scheme.
Conduction of internal audits into risk management processes and dissemination of these findings.

19
HYGIENE SERVICES AND INFECTION CONTROL
Hygiene: Kerry General Hospital has continued to strive to achieve improved standards in hygiene services in 2013. The standards for the Prevention and Control of Healthcare Associated Infection (PCHCAI) (including Hygiene Services) and the HIQA Safer Better Healthcare Standards provide the focus for quality improvement in Hygiene Services and this continued throughout 2013 in preparations for hospital licensing. The hospital was also assessed by the Health Information and Quality Authority (HIQA) in August 2013 and this also provide an impetus for ongoing improvements in hygiene services standards at the hospital. It has to be acknowledged that improvements in hygiene services during 2013 would not have occurred without the dedication and commitment of all staff at Kerry General Hospital, the feedback we receive on services by the public and feedback from internal and external assessments. Person centred care: Members of the Hygiene Committee have been involved in devising a service user experience survey for the hospital which was performed during 2013. Many of the elements were reflective of hygiene services including the cleanliness of the ward environmental and also catering related questions. This will provide feedback from service users as to where improvements in hygiene services could be made and a plan will be developed to address concerns by service users once the survey results are published. We also hope to learn from the good practices and feedback and maintain these practices into the future. Effective Care: Hygiene Services were systematically monitored, evaluated and continuously improved through continuous auditing of services. Two monthly management audits and ongoing self audits by wards/ departments throughout the hospital occurred throughout 2013. The results indicate exceptional compliance with self audit (94%) and extensive compliance in management audits (84%). Following the HIQA visits to hospitals regarding PHCHCAI over the past year the Director General of HSE has sought reassurances from each hospital regarding arrangements and improvement plans which are aligned to the 2006 Hygiene standards and National Cleaning Manual. This work is currently in progress and is likely to be completed early in 2014 when improvement plan will be identified to address any areas of concern. All actions from audits are progressed through the CNM/ Departmental Heads responsible for that area. Where there are risks identified through the audit process they are entered onto the appropriate risk register and escalated through the line management structure as appropriate. A log of issues is sent electronically following all management audits and is kept at local level to provide evidence of how the issues have been progressed. Safe care and support: The logging of verbal complaints commenced in 2012 and therefore trending of verbal and written complaints has seen the need to focus more on the learning from the complaint. There has been an increase in the verbal and written complaints. There were no written complaints in 2012 with four hygiene services related complaints in 2013 and there were 32 verbal complaints as compared to 15 in 2012. All complaints are dealt with according to policy and are discussed at as a standing item at hygiene team/ committee meetings.

20
INFECTION CONTROL: Infection Control is dedicated to promoting a safe and quality service to all service users in Kerry General Hospital. Throughout 2013 Infection Control continued to implement and participate in programmes to embrace national initiatives and reduce healthcare associated infection rates. Initiatives include
Audit of hand hygiene compliance Hospital wide hand hygiene awareness campaigns Participation in National Enhanced surveillance of Clostridium difficile Reduction in MRSA Blood Culture rates Ongoing implementation of PVC care bundles
Kerry General Hospital participates in the National Hand Hygiene Audits which are submitted to the HPSC biannually. Hand hygiene audits were performed by the Infection Control Team quarterly during 2013 utilising the HSE Observational Hand Hygiene Audit tool based on the WHO ‘5 Moments for Hand Hygiene’. Analysis of the results identified an improvement in the overall score for each quarter however not all staff disciplines are meeting the required national standard of 90%. Infection Control offered these identified groups follow up Hand Hygiene education sessions / re -audit as per hand hygiene action plan. Kerry General Hospital had an unannounced HIQA inspection of the Prevention and Control of Infection Standards (PCHCAI) on 22 August 2013 overall HIQA found the areas assessed were generally clean but highlighted some areas for improvement. Hand hygiene compliance on the day was not in line with best practice guidelines or Standard 6 of the National Standards Prevention & Control of Healthcare Associated Infections. HIQA concluded from the inspection that the culture of hand hygiene practice was not embedded throughout the hospital and poor hand hygiene practices posed a risk to patients of contracting a HCAI A quality improvement plan has been developed to address the areas highlighted by the HIQA inspection. A major challenge for 2014 will be to achieve the HSE set national target that 100% of staff must receive hand hygiene education by June 2014 Since the introduction of specific key interventions over the past number of years to reduce MRSA bacteraemia rates at Kerry General Hospital, this has resulted in a significant reduction in MRSA bacteraemia rates being achieved, from a high of 21 cases in 2006 and just 3 cases in 2013. Clostridium difficile is a major cause of antibiotic-related diarrhoea, particularly in the elderly and in May 2008, it became a notifiable disease.In June 2010 Yakult probiotic drinks were introduced for all patients over the age of 65 years and in that time there has been a reduction in the number of cases from 17 in 2010 to 9 cases in 2013. The Infection Control plan for 2014 is to continue our commitment to ongoing education and training for all healthcare staff and reduce HCAI rates Key Performance indicators for Infection Control for 2014
Increase Hand Hygiene compliance to meet the HSE target set at 90% hand hygiene compliance for 2014
Continue to monitor and reduce rates of MRSA positive bacteraemia cases
Monitor Clostridium difficile rates Monitor rates of Staphloccocus aureus blood stream infections Monitor and control outbreaks of infection if they occur Ongoing surveillance of alert organisms

21
RADIOLOGY DEPARTMENT Person centred care: In 2013, additional information was added to the CT appointment letters issued to patients informing patients of possible use of contrast medium, the side effects and the need for contrast medium to improve the quality of necessary CT examinations. Leadership, governance and management: Radiology Clinical Governance Meetings are held once a month on the last Thursday of each month. Radiation Safety Council meeting is held every 6 months in KGH. Workforce: The complement of consultant radiologist posts has been increased from 3 to 4 and the recruitment process has commenced for a further post. There are 14 full time radiographers 3 part time radiographers 1 agency radiographer 1 PACS manager 1 RSM 1 Darkroom technician Within this complement of staff there are: 5 Ultrasonographer’s (1part time) and 9 CT radiographers (1 part time). Use of resources: The x-ray department of KGH joined the newly established national Radiology Steering Group. The Radiology Clinical Lead is Dr. Simelane. The inaugural meeting will tale place in CUH January 2014. The main objectives of this group include the standardisation on PPPG, the devolvement of a robust educational and academic programme at regular intervals rotating to sites throughout the region to bring radiologist and radiographers together on the common ground of teaching, training and research. Use of information: The HSE NIMIS (National Integrated Medical Imaging System) project is investing in providing state of the art electronic radiology systems for 35 Irish hospitals. This new imaging system allows doctors to electronically view their patients’ diagnostic images, such as X-Rays and CT Scans, quickly and easily. The rapid access and availability of patient records to health professionals is a significant step forward for patient safety. Plans for 2014. A voice recognition system has been approved which will save on radiologist and clerical time and will be installed in February 2014. It will prove effective in reducing reporting time, as reports are generated automatically - using voice recognition technology - as opposed to transcribing and typing.

22
SPEECH AND LANGUAGE DEPARTMENT Overall Activity for 2013: 911 patients were seen and 3324 OPD appointments facilitated. Effective Care & Person centred care: In 2013, SLTS assessed, diagnosed and treated patients under the following National Clinical Programmes: COPD, Critical Care, Emergency Medicine, Mental Health, Older People,
Pediatrics and neonatology, Palliative, Primary Care, Radiology, Rehabilitation Medicine, Stroke & Surgery.
Supported the Health Care Associated Infection programme working to reduce unnecessary use of antibiotics through the identification and treatment of aspiration pneumonias.
Supported the Medicine Management programme to reduce or eliminate
aspiration or choking risk.
Both of these initiatives help to reduce the number of GP visits and hospital admissions required by this cohort of patients.
Audits carried out in 2013: Excluding participation in Hospital wide hygiene audits, Interdepartmental audits included Health Record Audit which demonstrated a need for electronic referral system and a Patient Satisfaction audit. Safe Care and support Activity: The SLT department facilitated 3324 appointments in 2013 and saw 911 patients. Education attended by staff: please see specific SLT training attended:
Tracheosotomy Care, NIMIS, MDT In Services, Cleft Palate, Communication in Dementia, Pediatric EDS, Intra-Department Laryngectomy, Intra-Department Videofluoroscopy, Laryngeal Manipulation.
Training provided for other health care professionals, patients and their families: Safe Management of People with EDS, Intra Department Videofluoroscopy, Intra Department Laryngectomy, Intra Department Pediatric EDS, Dysphasia and Communication for final year nursing students
SLTS use X- ray facilities for videofluoroscopic swallow assessments for both in patient and outpatients. In 2013, 58 patients were seen for this procedure. In-patients are seen as soon as time in the X-ray suite is available while the current waiting list for out patients is 2 months.
Better health & well being “The Safe Management of People with eating, drinking and swallowing
disorders” is a half or full day training developed by KGH SLT Dept. Held on a monthly basis for community hospital, nursing home, day care and
KGH staff. It aims to train front line staff in the early identification of Feeding, eating and
drinking difficulties and in the appropriate management of these difficulties. The programme is reviewed and amended to ensure relevance and quality.
Leadership, governance and management Clinical Governance is facilitated in three ways: Monthly departmental meetings attended by the 3 therapists who deliver the
face to face care and the head of the department. Each therapist attends professional supervision session every two months.

23
Bimonthly team meetings including discussion of complex cases and journal club.
All statutory regulations, including the National Consent Policy, Data Protection Acts and Health Act are complied with.
Workforce Three speech & language therapists (SLTs) (2.8 wtes) based in Kerry
General Hospital providing an inpatient and outpatient service. Two basic grade therapists work full time in KGH 0.8 Clinical Specialist rotates every 6 months with Senior SLT working in
primary care. The clinical specialist is an active member of a national working group
Secretarial support is received from one clerical staff member. Plans for 2014 To establish use of electronic referral systems. Audit PPPG on photography, audio and video recording Audit PPPG on Management of patients with communication disorders Audit waiting times for initial appointment/visit Audit impact of “The Safe Management of People with eating, drinking and
swallowing disorders”. Patient experience survey.
24
PHYSIOTHERAPY DEPARTMENT Summary of activity data in 2013: 7,589 outpatients were seen and 10,580 appointments were facilitated. Person centred care: Audit of ED/Physiotherapy linkages commenced in October 2013. Physiotherapy protocols were updated in relation to orthopaedics: e.g. facet
joint injection leaflet. Referral forms were updated for paediatrics physiotherapy for talipes to
ensure standard assessment and treatment. Standardised stroke assessment forms were completed which have been
printed and are currently being used to ensure detailed assessment. Effective Care: Service integration across acute and community increases effective
management of waiting lists on a county wide basis allowing for early identification of increased areas of activity and waiting times. This enables the service to act responsively to target resources effectively in both the acute and community settings. It also facilitates patient discharge, so improving patient outcomes. The Physiotherapy Service in Kerry has been integrated since 1998.
The department supports the Fracture clinic through attendance at morning fracture clinics on Tuesday, Wednesday and Friday, promoting more effective patient care.
Safe care and support: In service training/journal club takes place on a weekly basis. A Staff grade competency system is in operation. Complex cases are discussed at education sessions to provide learning
opportunities for less experienced staff.
Better health and well being: Membership of the Health Promoting Hospitals committee Membership of primary care groups in PCCC - allows for information sharing
e.g. suicide information leaflets placed in OPD/ED/Radiology waiting areas in KGH to inform the public regarding local services.
Leadership, governance and management: Staff meetings are held weekly to communicate key organisational
information. There are a number of standing items relating to quality and patient safety which are discussed at each meeting. Incidents are discussed as they arise to share the learning from these incidents.
Seniors meetings are held as required with line management. Annual service plans are completed within each area, e.g. neurology,
respiratory care etc. PPPG's were updated in 2013 and are currently available on the KGH
noticeboard. Physiotherapy management is involved in a membership capacity on
numerous committees within the hospital: HIQA Standards, Hygiene Committee, Hygiene Team, AMAU, Major Emergency Planning, Palliative Care Steering Group and the EMB/CGC.

25
Workforce: WTE consists of 6.6 seniors and 8 staff grades Cross cover is facilitated in all areas through shared expertise and skill mix.
This allows for rotation of staff to the hospital and community, and continuous up skilling of staff to cover in case of absenteeism etc.
Professional development plans (PDP's) are developed annually with line management to provide a formal opportunity for staff development.
PDP's are developed at each change of rotation with the relevant senior in each area. Staff grades complete projects on each rotation.
Plans for 2014: Audit of current physiotherapy assessment and treatment in relation to
osteoarthritis of the knee. Audit of physiotherapy referral information to be analysed in relation to an
audit undertaken with the ED in late 2013, audit of physiotherapy referral to orthopaedics to be undertaken in 2014.
Patient experience survey is to be completed in outpatient areas. Relevant patient information leaflets to be updated within the department. Physiotherapy assessment of rheumatology patients to run in conjunction with
the Consultant Rheumatologist which links into the National Rheumatology Programme.
A physiotherapy led Oxygen Clinic initiative which encompasses review of clients with home oxygen requirements to ensure appropriate oxygen prescription for clients. This was presented to the Medical Board in 2013 and is due to commence in early 2014.
Pulmonary Rehabilitation is to re-commence in community which would include the health needs of medical clients who would be reviewed in KGH.
Paediatrics, Women’s Health and Palliative Care upskilling is to take place to ensure appropriate levels of cross cover are available in these specialist areas.
Provision of educational updates as appropriate, e.g. updates given to the ED on an annual basis regarding the role of the physiotherapy service.

26
AUDIOLOGY DEPARTMENT Person centred care: The Department primarily deals with diagnostic testing and rehabilitation of
children (0-18years) with hearing problems. Patients may be referred by the New Born Hearing Screening (UNHS)
program, the community care setting or from within the hospital. Diagnostic hearing tests are also provided for adult patients referred by GPs
or as an in patient. Patients may be referred on to outside services. Effective Care: One of the main KPI’s for the department are for UNHS referrals. New borns
must be seen by 4 weeks of age for diagnostics, and where appropriate, fitted with hearing aids by 6 weeks of age.
There is a waiting list for routine testing of older children. Urgent referrals are given the next available appointment.
Hearing aid fitting for late diagnosed children is carried out within 3 weeks of diagnosis.
Training attended by clinic staff in 2013 excluding mandatory training; PPPG training, Hearing Aid training at Cork for new hearing aids introduced in HSE tender, Hearing Aid training in clinic at KGH and attendance at the Irish Academy of Audiology Conference in Dublin for Diagnosing & rehabilitation of babies with Auditory Processing Disorder
Safe care and support: A high DNA rate was noted in adult clinics that were run Monday to Friday,
therefore the department held 10 Saturday clinics in 2013 to facilitate adult patients. There was a very low DNA rate for these clinics.
The initiative resulted in more paediatric clinic slots becoming available during the week, resulting in a reduced waitlist from 18-24 months to 12 months
A DNA x 1 policy for discharge from clinic for all patients was initiated. These initiatives were presented at the KGH QPS awards.
Better health and well being: The department provided the following training in 2013; Guest lecture on Audiology to PHN students at UCC Guest lecture on Audiology testing to GP trainees at IT Tralee Second tier training in testing for school going children to AMO at KGH
Audiology Dept Clinical training for MSc Audiology student one day a week at KGH Audiology
Department Assistance for complex case clinics at SRBP cork.
Leadership, governance and management: Clinical governance group for Audiology in Cork-Kerry is provided by UCHG. Day to day operational matters are directly accountable to the General
Manager in KGH. Workforce: 1 full time Audiologist, 1 part time Audiology Assistant, 1 part time secretary.
Plans for 2014 – To develop PPPG’s for department at hospital level (National PPPG’s being
developed by National Lead in Dublin) To attend Audit training To facilitate extra clinics

27
HOUSE KEEPING SERVICES Person centred care: A patient experience survey was completed in all wards with regard to the
cleanliness of the ward areas. The results will be available early 2014.
Effective Care: The housekeeping supervisor reviews the results of the internal self audits
from a housekeeping perspective to ascertain improvements required in housekeeping services.
The mean score of the internal self audits for the hospital in 2013 was 94%. The environment section of the audit reflects the cleanliness of the audited
area and this achieved compliance of 87% The cleaning equipment section scored 95% overall for 2013. Audits are performed on the response rates by the housekeeping and
contracting cleaning services to non routine cleaning requirements. The majority of these requests are dealt with within 10 minutes.
An audit performed by HIQA identified areas for improvement. A quality improvement plan was implemented which has allowed the housekeeping department to address the deficiencies. An additional 50 hours of contract cleaning have been approved to implement the plan.
An updated curtain recording system has been introduced in 2013. The aim is to make it easier for staff to recognise when curtains are changed and therefore eliminate unnecessary changing of curtains.
Following the HIQA visits to a number of acute hospitals regarding PHCHCAI, during 2013 the housekeeping department has been involved in the review of the cleaning manual. Quality improvements are being implemented to ensure all elements of the cleaning manual requirements are met from a housekeeping perspective.
Safe care and support:
A verbal complaints register for all housekeeping / contract cleaning issues reported during 2013 was commenced and has seen a marked increase in the reporting of these complaints. The complaints generated are reviewed at all hygiene services team meeting; recurring issues are identified and progressed appropriately. Three written complaints were received in 2013- two of these were for the same issue but were from a staff member and service user perspectives. Two incidents were reported by housekeeping staff to the Health and Safety Authority and the staff were off work for more than four days.
Excluding attendance at mandatory training, staff attended training on the “KGH “notice board” to facilitate access to policies and procedure on there.
Leadership, governance and management: The housekeeping supervisor has a reporting relationship with and is accountable to the operations manager and is a member of the hygiene services committee, which reports to the EMB. Workforce: There are currently 37WTE in the housekeeping department. Plans for 2014:
The focus for the housekeeping department during 2014 will be to improve compliance with hand hygiene and education for the department
Implement a safety package for staff. Cleaning schedules and policies due for review will be updated. Devise a quality improvement plan to address any deficiencies identified in
the patient experience survey.

28
Catering Department Person centred care:
The catering department, in conjunction with the health Promotion Committee introduced the “Protected meal time “initiative in 2013 because the nutritional status of the patients impacts strongly on their recovery.
The initiative was introduced to eliminate, and at the very least minimise the amount of clinical contact that takes place at meal time, allowing the patient to eat, digest and enjoy their meal.
Safe care and support: The Department legal requirements and industry standards are as follows Food Hygiene Regulations 1950/1998, Official Control of Foodstuffs S.I 85
OF 1998, Hygiene of Foodstuffs Regulations S.I 86 OF 1998, Hygiene in the Catering Sector I.S 340 2007 and Guidelines on the Cook Chill System in the Food Service Sector
In the Department there is a HACCP System in place which a systematic approach to the identification assessment and control of hazards. There are three HACCP Teams in the Department which meet on a regular basis.
Fire Audits and Maintenance Audits and reports are carried out weekly. There are four HACCP audit checklists carried out on the last week of every
month: Time –Temperature Audit, Food Safety Audit, Personnel hygiene Audit and other hazards.
An Annual HACCP audit on facilities and other hazards is carried out annually The Mandatory Compliance Assessment in association is carried out every
three months.
Staff attended training as follows: Fire training-29 Occupational health training-32 Hand Hygiene-30 Ecolab chemical training-39 Standards for better healthcare presentation-33.
Leadership, governance and management: The Catering Department comprises of a team which includes a Department
Head, Supervisors, Chefs and Catering Attendants. All team members meet on a daily basis with morning meetings for day to day
operational organisation. Use of Resources: The Catering Department operates a Cook Chill system. All food which is served to patients, staff and visitors is prepared and
processed in the Main Production Kitchen. The department provides, on average 1300 meals per day. This figure includes patient meals, staff meals, public meals and meals provided to two Satellite Units.
Workforce There are 57 Catering Attendants (49.1 WTE), 9 Chefs (8.8 WTE) and 6
members of staff on the Management team (5.5 WTE). The Department is open from 6.30am to 2am daily
Plans for 2014: To introduce new “Food Distribution Trolleys” in the department. We will roll out a programme for improved service delivery for our Catering
Attendants in February 2014.

29
OCCUPATIONAL THERAPY DEPARTMENT. Person centred care: OT Service users audit completed. OT patient information leaflets have been specifically designed for our clients.
These include a list of equipment suppliers, directions to community stores, memory, thinking & understanding leaflets and pendant alarms.
An OT in patient prioritisation system has been reviewed and updated The department completed a 2013 annual report for the CNU.
Effective Care: OT care pathways have been updated and linked to National Clinical Care
Programmes, in particular the care of the elderly, orthopaedics, palliative care, stroke, rheumatology & acute medicine programme.
OT manager is a member of AHP advisory committee for the acute medicine programme
Links with PCCC have been maintained through referral pathways, shared patient care as required and staff grade journal clubs
Safe care and support: Journal club/education sessions are held every 2 weeks. Education attended by OT staff includes supervision for occupational
therapists, dementia care for occupational therapists, stroke assessment for occupational therapists, seating- an introduction, memory impairment, OT Driving skills assessment ,OT in the palliative care setting, hand hygiene, moving and handling, fire and infection control
OT Department Safety statement completed OT Dept. risk assessments completed OT manager is a member of the hygiene team in KGH OT manager is a member of the SDU team in KGH Management of safety alerts are managed appropriately and discussed in OT
team meetings. Education provided by OT department in 2013 included: a presentation to
the Kerry PD support group OT treatment in Parkinson’s disease. This was a joint initiative between the OT and the physiotherapy departments. Undergraduate nurses, health care assistants, multi task attendants and the community nursing unit received education. Transition year & leaving certificate students were facilitated within the department. OT student placements and education were provided to UCC students OT Cardiac rehabilitation, both individual sessions and group sessions were facilitated in conjunction with the cardiac rehabilitation team.
Better health and well being: We liaise with the OTs in the community regarding pre-discharge home
assessments and post discharge follow up, facilitating a successful patient discharge and the necessary follow up in the community setting.
Pre-operative orthopaedic assessment planning was examined in 2013. Research with regard to best practice was completed and OT documentation is awaiting implementation.
Out patient splinting service; plastic surgery, orthopaedics, neurology, rheumatology.
Leadership, governance and management: Weekly team meetings in OT dept. where all staff including rehabilitation
assistant attend – all adverse incidents are reviewed & discussed. Risks are identified and entered into the Risk Log.

30
Department professional supervision policy revised 2013. Supervision structure in place for all OT staff Support structure in place for all OT staff Accountability is being assured through regular staff supervision, each
therapist engaged with a supervisor and a supervision contract completed, as per department policy. Competency reviews being completed in planning for staff rotation.
Workforce: WTE: there are 5.86 WTE OTs comprising 0.86WTE OT Manager,2 Senior
OT and 3 Staff Grade OT providing OT inpatient services to the rehabilitation ward, general surgery and general medical wards.
Staff competency reviews, completed at the end of 2013 Annual Personal Development Plans are completed Plans for 2014: OT discharge planning audit to be completed Orthopaedic audit to be completed Cognitive screening for in patients audit to be completed A working group is to be convened in 2014 to address write a policy for
standardised assessment of patients’ medical fitness to drive. Staff rotation is planned for January 2014. All staff to change areas or to
change work practices as required. The OT team will participate in the pre operative orthopaedic joint school
initiative.

31
NURSING DEPARTMENT Person centred care: Commencement of CNS Jan 2013 in Symptomatic Breast Disease and
Oncology Liaison Recruitment of Clinical Nurse Specialist (CNS) Diabetes community outreach
September 2013, with 0.2 WTE commitment to the hospital. Commencement of Pre-conceptual Diabetes advice clinic Renal CNS has compiled 3 patient booklets-“Renal Patients Guide to testing
for blood borne Viruses in blood”, “A-V fistula patient education” leaflet and a Patient record booklet.
A patient/carer satisfaction survey (AMAU) conducted and published internally in KGH and externally to the HSE.
The National Cancer Screening Bowel and Cervical Programme has seen the progression of a colorectal Advance Nurse Practitioner on an educational and training pathway.
2013 saw the appointment of a 3rd ANP in ED. Effective Care: Revision and sign off of collaborative practice agreements for nurse
prescribers Practice Development are the lead on Self assessment and quality
improvement planning for Standard 2, Safe and Effective Care, of the HIQA Standards
Implemented internal rotation of staff between CCU and Sceilig to facilitate up skilling of Sceilig staff in CCU.
Chest pain pathway and Sepsis Pathway implemented in ED. Safe care and support: The following specialist training has been facilitated: the revised National
Management of Spinal injury guidelines, Identification of Sepsis (Sepsis 6), and P.R.O.M.P.T (pregnancy related), Category 1 Nursing Board approved ECG Interpretation study day by KGH cardiology nurses, Tracheotomy Care, Palliative Care, Gerontology, nurse prescribing (medication and ionising radiation) and Cardiac care, perineal suturing, neonatal and paediatric care, cannulation and phlebotomy, paediatric life support, Dementia care, HIQA standards for Quality and Patient Safety, NIMIS (X-ray & ECG) ordering and results, clinical audit, policy and procedure development, open disclosure,training in Epidural Care and the new Epidural Policy
Staff undertook Higher Diploma specialist education programmes in emergency, critical care and peri-operative nursing and Masters Degrees.
Implementation of the National Early Warning Score and iMEWS (maternity early warning score)
Staff of Muckross ward undertook on-line HseLAnd Stroke programme Nurse colposcopist completed supervisor training and Second Nurse
Colposcopist commenced training under the Cervical Screening programme. Better health and well being: Waiting list for all investigations in cardiology diagnostics reduced by half Patient experience times ED and AMAU- 96% patients are seen within 9hrs in
department and 85% within six hours. KGH is consistently in the top 5 performers nationally for wait times in ED.
Scheduled Hygiene Management and ward based hygiene audits Out patients – additional sessions, including out of hours clinics were held to
clear end of year waiting times and so achieve waiting list targets

32
Extra endoscopy sessions were scheduled to facilitate routine and emergency patients.
Leadership, governance and management: The Nursing Department at Kerry General Hospital is Lead by the Director of
Nursing and Midwifery and Nurse Executive Team of four Divisional Nurse Managers and two Night Assistant Directors.
Governance is further strengthened by Divisional Nurse Management Team membership of the medical, surgical, ED, OT, Orthopaedic, Maternity and paediatric clinical governance and operational groups. These groups report directly through their chairperson to the EMB.
Under and post graduate education governance is provided through the Directors of Nursing and Heads of Department committee (HSE, Bon Secours and I.T.Tralee) and the Director membership of the Board of Management of Kerry/Bantry Centre for Nurse Education.
Workforce: Nursing whole time equivalents in December 2013 was 411 (excludes staff on
unpaid leave) Plans for 2014: Develop and implement nurse sensitive patient outcome indicators and pilot Implement nurse led elective in-patient preoperative assessment Open a stroke unit and reorganise the rehabilitation ward. LEAN method review of Theatres and implementation of the national ‘The
Productive Operating Theatre’ Commence data collection for orthopaedic ‘hip fracture’ and trauma
databases and participate in national database. Provide additional training at Higher Diploma level in critical and specialist
area nursing Improve nurse compliance rates with hand hygiene training to the national
required standard of 100%. Participation in audit of ITU Acquired Blood Stream Infections Surveillance
Protocol Establish a nurse led clinic for Irritable Bowel Disease (IBD) patients. Roll out in service ward based cardiology programme RGN’s (AMAU) to commence the certificate in Nurse Authority -Prescribe
Ionising Radiation. Extend use of red aprons’ Do not Disturb’ for staff nurses doing medication
rounds in 2014. Set up clinics for the Colorectal CNS using electronic resources (PIMS).

33
PASTORAL CARE DEPARTMENT Person centred care: We visit each patient at least once during their stay (Over 14000 patients in
2013). We also meet relatives and offer support. We are an integral part of the holistic and total patient care offered at the
hospital. The chaplains are available to all patients, relatives and staff regardless of
religious belief. Amongst many of the supports we provide, we assist with naming services for
deceased babies, arrange emergency baptism for ill babies as requested and support the parents with their loss and bereavement.
We provide support and counselling for bereaved families. There were 348 families bereaved last year.
Better health and well being: We help provide for individual spiritual and emotional needs. We offer special help to those who are critically ill and their relatives. We are available to staff in either in their work where they are experiencing
personal challenges and difficulties.
Leadership, governance and management: The department meets at least twice a week. Mary Quinlan is responsible for Palliative Care, Oncology, and Maternity ward
areas. In 2013 she organised a prayer service to take place three times a year for palliative care relatives and friends of those who have died.
Fr Martin Spillane is responsible for Mental Health. There is a Pastoral Group meeting each Wednesday evening with Mental Health patients and reflection groups take place two days a week.
Fr Teddy Linehan Dept Head is responsible for Tralee Community Nursing Unit, Ardagh and Rathass wards. He is responsible for the administration of the department.
Workforce: Fr Linehan is the department head. Our Department consists of three fulltime Chaplains. There are two Catholic
Priests and a lay Catholic lady Chaplain. We also have two Catholic Priests who provide holiday cover.
The Chaplains within the Pastoral Care Department are certified members of the National Association Healthcare Chaplains.
Since September 2013 we have a lay Health Care Chaplain three days a week.
There is an unrostered Church of Ireland part time Chaplain. There is a night on call service available.

34
PATHOLOGY DEPARTMENT
Overall Activity for 2013. Biochemistry test number total -2622359, up 9.5% on 2012 levels. Haematology test number total-358493-up 3% on 2012 levels. Blood bank requests- 26237 and 4885 products issued. Microbiology test number 90701—down 1.3% on 2012 levels. Histopathology activity is down 2% on 2012 levels. Molecular diagnostics activity is down 6% on 2012 levels. Effective Care: 104 audits were scheduled in total and corrective action taken for non
compliances. Safe care and support: The Pathology Blood Transfusion service is required to be inspected annually
by The Irish National Accreditation Body (INAB) for compliance to ISO 15189. The accreditation status of Pathology departments is as follows:
Blood Transfusion and Haemovigilance-accreditation was retained-April 2013
Haematology- accreditation was retained- April 2013
Molecular Diagnostics- accreditation was retained- April 2013
Histopathology-following close out of NCR raised in April 2013, accreditation status was re-instated in June 2013.
The accreditation certificate for all tests included on scope was re-issued for a 2nd 5 year accreditation cycle.
Biochemistry-due to a lack of clinical governance the department was denied accreditation in April 2012 and is unable to proceed until there is a resolution to this issue. Biochemistry continues to participate actively in the pathology quality management system.
Microbiology- Microbiology will continue to strive for INAB accreditation but the process will take some time.
Leadership, governance and management: Authority, interrelation and responsibilities of all Pathology personnel are
defined in the form of job descriptions, which are available in the document “Roles and Responsibilities in Pathology” [P-PATH-ROLRESP] on Q-pulse.
Staff meetings, including heads of Pathology sections, quality and Health and safety are held regularly.
Professional development plans (PDP's) are developed annually with line management to provide a formal opportunity for staff development.
Annual Quality Management review meeting is held to review the Pathology service and develop key objectives for the coming year.
Workforce: The staff numbers consists of: 32.25 WTEs, which consists of: 1 Chief Medical Scientist, 1 IT Manager, 1 Quality Manager; 1 Senior Biochemist, 6 senior Medical Scientists, 22.5 Basic Grade Medical scientists.

35
There is one resident Consultant Histopathologist (1WTE) and one visiting Consultant Haematologist (0.2 WTE). There are 4.4 Lab Aids and 2 Haemovigilance nurses working on a part-time basis. Plans For 2014: QMS-QOP-14-01: Pathology move and installation of new Pathology equipment: A master plan for validation processes will be drawn up, in order to carefully plan and implement all validations required prior to use. QMS-QOP-14-02: Referral laboratories: A list of all referral laboratories for Pathology will be compiled; each department list will be amalgamated into one complete consolidated review list which will assist audit of this area. This master list will be maintained and reviewed by QM. QMS-QOP-14-03: Suppliers: A list of all suppliers for Pathology will be compiled; each department list will be amalgamated into one complete consolidated review list which will assist audit of this area. This master list will be maintained and reviewed by QM. QMS-QOP-14-04: A plan for transition to ISO15189:12 standards will be drawn up. In conjunction with each department’s quality officer, the necessary changes will be made to processes, practices and procedures to ensure that the requirements for these standards are met. The most important long term goal however is to continue to provide a safe, high quality service to users of our service.
36
MEDICAL RECORDS DEPARTMENT
Person centred care: There were a total of 13,223 admissions in 2013 and 13,198 discharges. There were a total of 54,681 OPD attendances and 34,288 ED attendances. Safe care and support: The medical record departments’ achievements in 2013 are as follows: Centralised the Outpatient waiting lists in central referral office. AMAU patients are capture on PiMs system since April 2013. Implemented the Medical Records Policy Implemented the HIQA Standards Theme 8 in relation to Safety and Security
of Records. Audit compliance with Theme 8 of HIQA standards for safety and security of
medical records. An audit carried out in 2013 demonstrated issues regarding medical record storage which have been placed on the risk register. A business case has been submitted to the EMB for consideration to address the issues.
An Audit was carried out by NTPF in relation to the validation process for OPD and they found KGH to be compliant with the process.
Leadership, governance and management:
The committee, chaired by the Medical Records Officer works under the Governance of the Operations Manager and holds quarterly meetings. Medical Records contribute to the following committees. AMAU Maintenance Group Outpatient Services Management Group Information Governance Committee SDU Bed Management Committee Inpatient Services Management Group NIMIS Implementation Group Major Emergency Committee.
Workforce: There are 95 WTEs in the medical records department.
Plans for 2014: PiMs Amalgamation Project April 2014. Implementation of Standard 8 with relocation of Medical Records Library to
the vacant stores department. E-Referrals Project – enable KGH to accept GP referrals electronically
through central location. Patient Document Tracking. Implementation of 4 week HIPE coding deadline in line with MFTP targets. Implementation of DNA Policy for OPD in conjunction with OSMG. Implementation of OPD Policy in line with SDU Guidelines. Implementation of the Inpatient Waiting List National Policy.

37
DIETETIC DEPARTMENT
Person centred care: The Department of Nutrition and Dietetics, Kerry General Hospital provides nutrition support and dietary intervention/education to inpatients and outpatients. Dieticians assess the nutritional status of patients, determine individual nutritional requirements and formulate a plan of care to meet these nutritional requirements. Education is provided for patients and carers on nutrition support and/or special dietary interventions appropriate to their plan of care.
Department Activity/Statistics- 2013
Total number of patients seen: 5401 Total new patients: 1375 Total reviews: 4026 Gestational Diabetes Referrals 2010 39 2013 97 During 2013 we revised and updated some of our patient education material and dietary advice literature. These included: Gestational Diabetes diet sheet, in line with the HSE document “Guidelines
for the Management of Pre Gestational and Gestational Diabetes from pre - conception to the postnatal period” and the Diabetes Interest Group of the INDI (Irish Nutrition and Dietetic Institute) guidelines.
New Modified Texture diet sheets, (including diabetic versions) were produced for patients with dysphagia. These diet sheets were developed in line with National descriptors for modified texture diets.
Diet sheets for surgical patients with diverticular disease, post oesophagectomy and Nissens funduplication.
Safe care and support: During 2013 state registration for Dietitians was introduced under the
regulation of CORU (Health and Social Care Professionals Council and Registration Board). Continuous Professional Development (CPD) is a requirement for registration with CORU.
All Dietitians in the department are members of the INDI, which now also has an obligatory CPD requirement to practise as a professional Dietitian, since January 2014.This year, we will endeavour to facilitate this compulsory CPD for department members, in association with hospital management.
In 2011 Kerry General Hospital adopted the new Diagnostic criteria for Gestational Diabetes (as per ‘Guidelines for The Management of Pre - Gestational and Gestational Diabetes from Pre- Conception to the Post- Natal period’, July 2010), which has had and is continuing to have a direct effect on the number of patients diagnosed with GDM referred for dietary advice.
In 2010, 39 patients with Gestational Diabetes were seen, increasing to 97 in 2013 (148% increase).
Education provided by the department- Our Cardiac Dietitian delivers a dietary education talk to patients attending
the six week cardiac rehabilitation programmes. One of our Dieticians also participates in and presents in turn at the Ardagh
monthly in service education session.

38
Leadership, governance and management: All departmental staff are responsible to the Dietitian Manager. At present bimonthly department meetings are held, however for 2014 we aim to increase this to monthly to facilitate staff education and CPD obligations. Workforce: There are 4.8 WTEs dieticians in the department. The department has secretarial support for two half days per week.
Plans for 2014: We will continue to record patient statistics and monitor trends in 2014. We
plan to implement our updated outpatient DNA policy and evaluate its effects on attendance and outpatient waiting lists.
Good compliance with an appropriate diet is of fundamental importance in the management of all types of diabetes. During 2014, we will continue to highlight the need for a dedicated Dietetic post for Diabetes, particularly with the planned developments for KGH under the Diabetes National Clinical Care Programme.
We plan to carry out an outpatient satisfaction survey and further develop department policies and guidelines.
We will develop a Parenteral Nutrition Policy (Drugs & therapeutics Committee) for inpatients of KGH. Nutritional care of patients on parenteral nutrition is a new development for the department and one with significant time implications.
To update the therapeutic diet guidelines for catering staff.