kevin creeden, m.a., lmhc whitney academy east freetown, ma kcreeden@whitneyacademy
DESCRIPTION
Re-Attaching the Brain: A Developmental Treatment Approach for Treating Sexual Behavior Problems in Children and Adolescents. Kevin Creeden, M.A., LMHC Whitney Academy East Freetown, MA kcreeden@whitneyacademy .org. A Developmental Framework. - PowerPoint PPT PresentationTRANSCRIPT

Re-Attaching the Brain:A Developmental Treatment Approach
forTreating Sexual Behavior Problems
in Children and Adolescents
Kevin Creeden, M.A., LMHCWhitney AcademyEast Freetown, MAkcreeden@whitneyacademy .org

A Developmental Framework
•Development happens across a variety of areas: neurological, physical, emotional, social, cognitive, academic, moral, etc.
•Development proceeds from the existing competencies

Developmental Framework
•A variety of developmental models can be used in conceptualizing effective treatment
•Maslow (1968), Bowlby (1973) Strayhorn (1988), Erickson (1963)
•Common developmental issues
Common issues•Sense of belonging: trust, safety,
closeness, dependence
•Differentiating self from other
•Self-regulation of physical and emotional responses: delaying gratification
•Developing cognitive skills
Common Developmental Issues
•Cognitive flexibility/adaptive problem solving
•Moral development
•Empathy
•Creativity
Clinical Assumptions
Trauma in early childhood has a neuro-developmental impact
The individual’s own trauma experiences and their current behavior are linked through a variety of trauma associations and cues
Without addressing trauma associated symptoms the integration of new learning and new narratives will not effectively occur
There is a physiological response to trauma cues that effects processing, cognitions, emotional response, and behavioral response
It is impossible to discuss trauma in children without addressing the quality of parental attachment (van derKolk, 2003)

Engaging in abusive behavior is primarily focused on meeting relational needs
Safety is the primary goal
Competency in relationships and developmental tasks are key protective factors
Children do well if they can

Kids Have to Think That You Care Before They Care What You Think

Resiliency Factors
1. Positive attachment to emotionally supportive and competent adults
2. Development of self-regulation and cognitive abilities
3. Positive self-concept
4. Motivation to act effectively
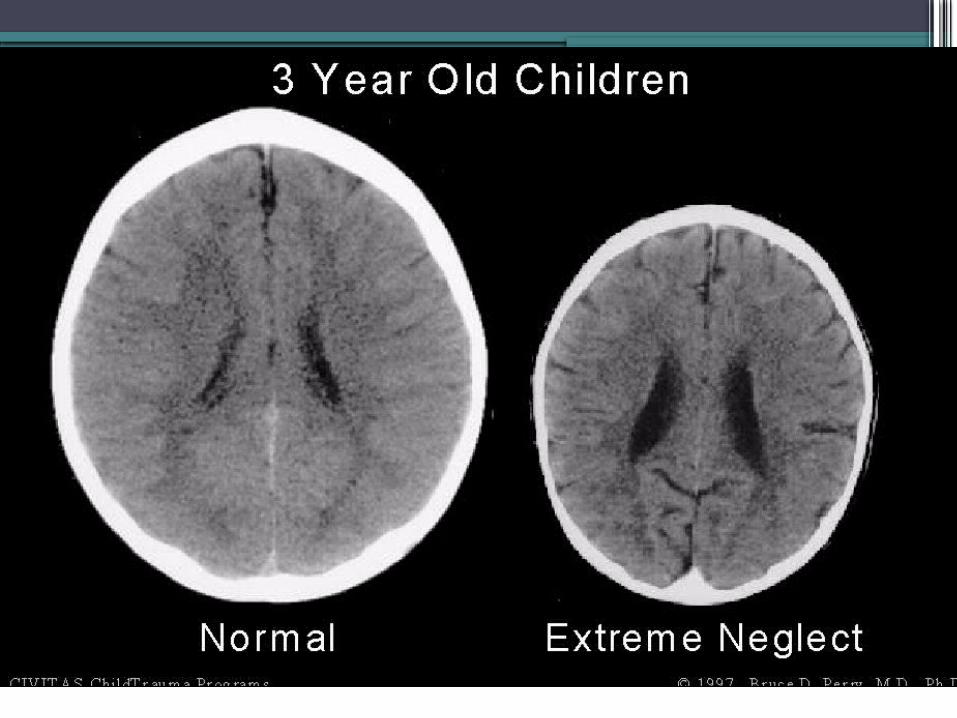
Brain Development and Trauma
Brain abnormalities are associated with childhood abuse and neglect
(Teicher, 2002; DeBellis, 2001)
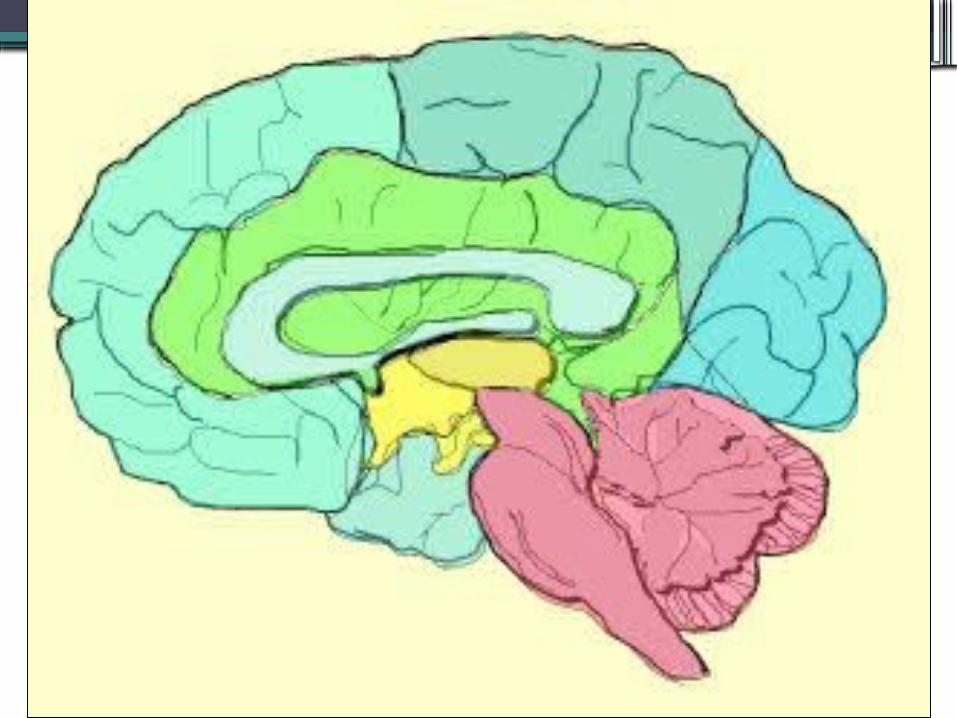

Hypothalamus: controls appetite, hormones, and sexual behavior
Amygdala:responsible for anxiety, fear and emotions
Neocortex: Site of higher cognitive functions and sensory integration
Cerebellum: seat of motor control and coordination
Hippocampus: crucial to memory and learning facts
Brain stem: responsible for sensory input and physiological responses

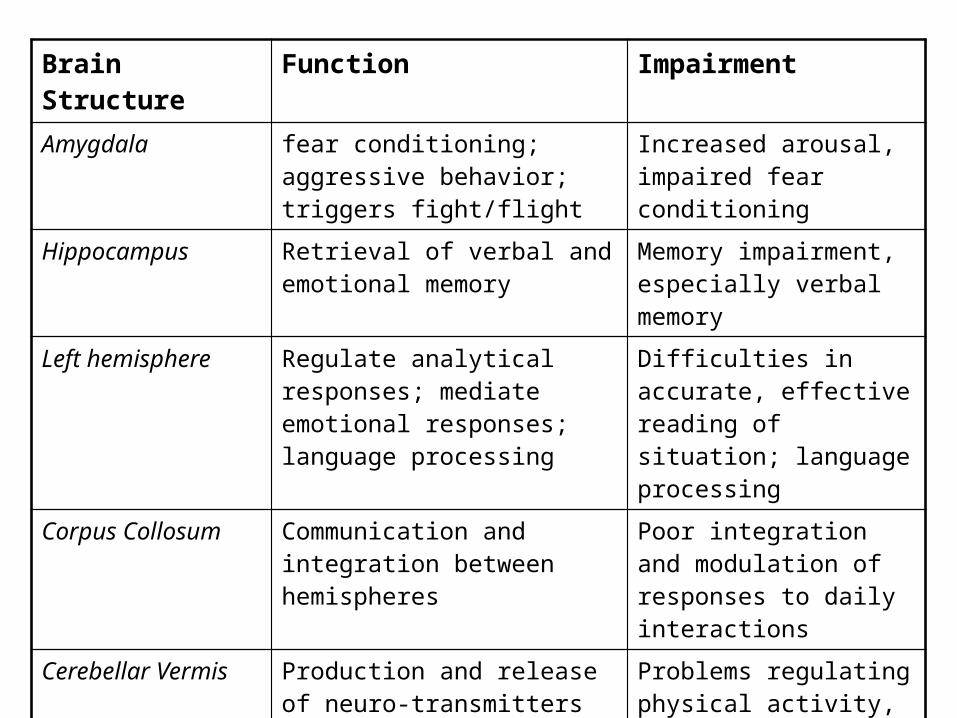
Brain Structure Function ImpairmentAmygdala fear conditioning; aggressive
behavior; triggers fight/flightIncreased arousal, impaired fear conditioning
Hippocampus Retrieval of verbal and emotional memory
Memory impairment, especially verbal memory
Left hemisphere Regulate analytical responses; mediate emotional responses; language processing
Difficulties in accurate, effective reading of situation; language processing
Corpus Collosum Communication and integration between hemispheres
Poor integration and modulation of responses to daily interactions
Cerebellar Vermis Production and release of neuro-transmitters
Problems regulating physical activity, attention, emotions
Prefrontal cortex Center for executive functions Poor organization, rigid problem solving; increased impulsivity
Assessment Issues•Trauma symptom assessment • TSCC; TSI
•Screening for processing difficulties• SCAN:A; Bender; RCFT; WCST

•Family of origin issues and expectations of the parents, foster parents, or other caregivers• FAM:III; Stress Index for Parents of
Adolescents (SIPA); Clinical interview; TSI
•Discriminate attachment styles for the parents and child• Relationship Questionnaire
(Bartholomew and Horowitz, 1991)

•Behavior specific assessment: sexual knowledge, attitudes, cognitive distortions, focus of fantasies.
•Personality assessment to examine issues of depression, aggression, anti-social attitudes
Phase Oriented Treatment
Stabilization, including education and identification of feelings/somatic states
De-conditioning traumatic memories and responses
Restructuring traumatic personal schemes
van der Kolk, et al , 1996
Maslow’s Hierarchy of Needs
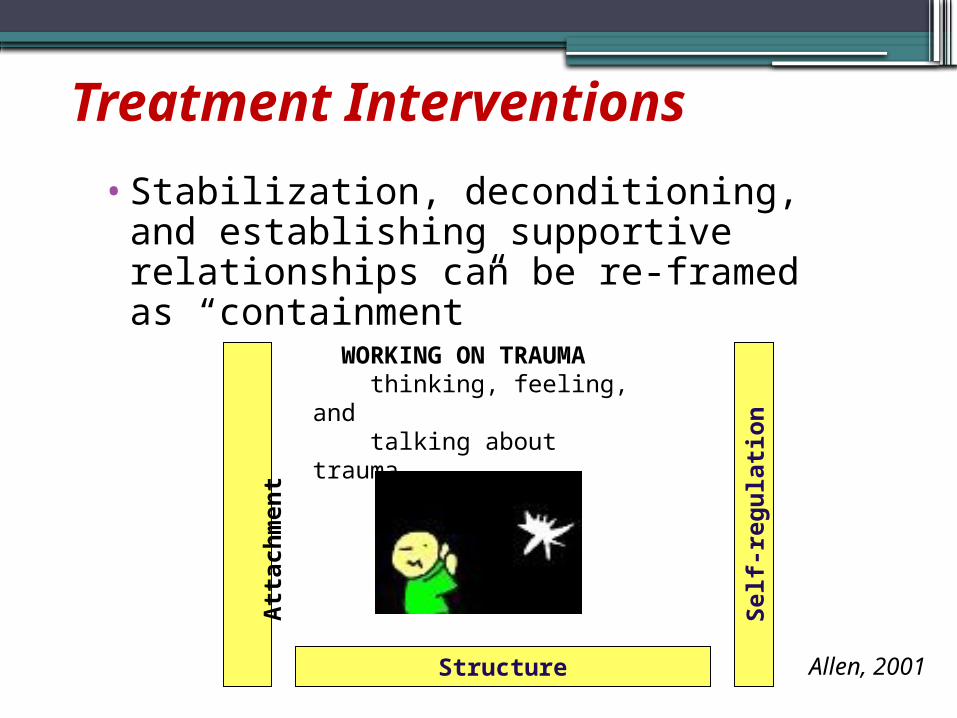
Treatment Interventions•Stabilization, deconditioning, and establishing
supportive relationships can be re-framed as “containment”
Structure
Self-
regu
latio
n
WORKING ON TRAUMA thinking, feeling, and talking about trauma
Allen, 2001
Atta
chm
ent

Structure
•Consistency and predictability in the schedule
•Consistency in expectations
•Consistency in responses
•Consistency in environment
•Use of rituals
Self-Regulation•Active learning and practice of a
variety of activities and techniques
Deep breathing and “counting to 10”Visualization and “safe place”Yoga or tai chiMusic, journaling, artDaily exerciseBrain gymBiofeedback
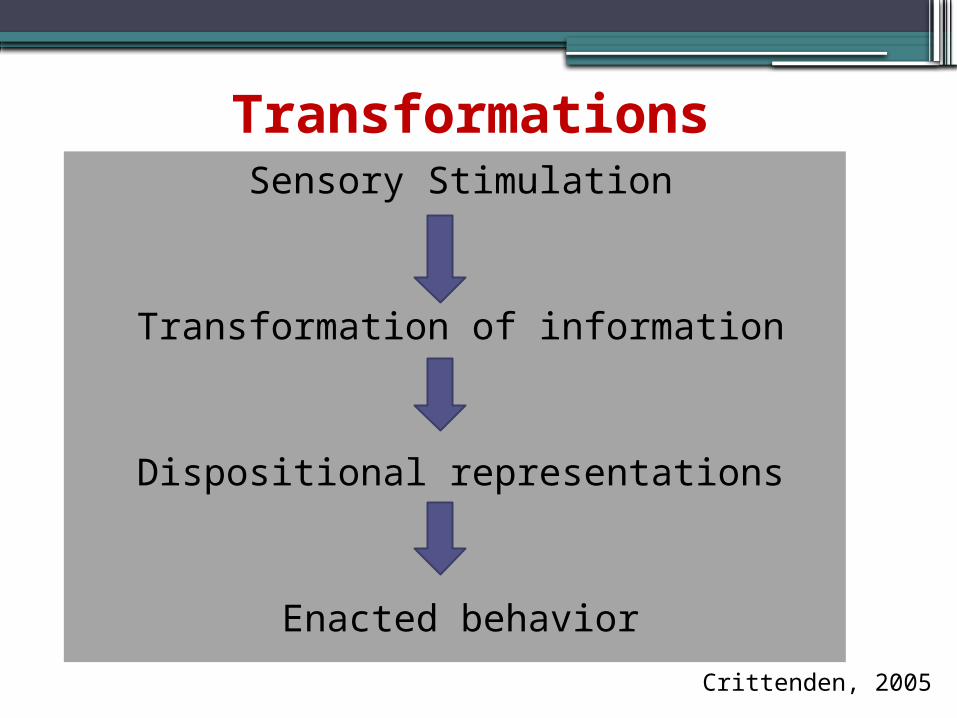
TransformationsSensory Stimulation
Transformation of information
Dispositional representations
Enacted behaviorCrittenden, 2005

Sensory Areas
•Proprioception•Vestibular•Auditory•Visual•Tactile•Olfactory•Gustatory

Proprioception•Sensations derived primarily from large muscles and joints; especially during movement against resistanceCan help person feel grounded
• DEEP Pressure: often over-rides over arousal
Proprioception examples
•Weighted blankets or vests•Wall push ups•Walking•Isometric exercise•Brain gym•Exercise balls•Clay work
Vestibular•Sensation derived from stimulation of vestibular mechanism in the inner ear
•Provides a sense of equilibrium and balance
•Contributes to a sense of one self in space“boundary issues”

Auditory•Directly connected to vestibular•Sound, music, rhythm serves as a “pacemaker”
•Different sounds connected to mood, pace
•Consider different sounds in transition in environments like residential centers and schools

Gustatory•Includes oral motor as well as taste
•Stimulation can help with attention, comfort, and overall organization
Tactile•Touch, pressure, vibration, temperature, pain
•Provides sense of body image, boundaries, self
•Fundamentally connected to safety, comfort, self-soothing, attachment
General CharacteristicsCalming•Mild•Rhythmic•Simple•Familiar•Consistent•Soothing•Low demand
Alerting•Strong•Fast paced•Non-rhythmic•Complex •Novel•Unpredictable•High demand
Anxiety and Agitation•Deep breathing•Isometric exercise
•Rocking•Using weighted blanket
•Stress balls•Calming music•Chewing gum
•Rocking chairs or gliders
•Yoga•Mindfulness•Biofeedback•Rowing
Grounding Approaches
•Strong tastes•Sour candy or hot candy•Chewing gum•Ice tapping•Hot/cold shower•Pacing•Tapping•Movement: yoga, tai chi
Depression•Weighted vest•Movement and exercise•Beanbag tapping•Warm pad•Scented lotion•Stroking/brushing
Calming techniques are often not helpful

Developmental Model1) Self-Regulation
2) Attachment
3) Cognitive skills
4) Social Skills
5) Adaptive Living Skills
6) Healthy Sexuality

Self-regulation (2)
•Identifying triggers
•Connecting sensations w/ thoughts, feelings, behaviors
•Identifying choices
aspects of BrainWise

Attachment styles: BartholomewStyle
Secure
Preoccupied
Avoidant
Dismissive
Self Others pos (+) pos (+)
neg (-) pos (+)
neg (-) neg (-)
pos (+) neg (-)
Domains of Impairment: Complex TraumaI. Attachment
Distrust
Social isolation
Attunement difficulties
Boundary problems
Problems with perspective taking
Cook, Spinnazzola, et al (2005)
Addressing Attunement•Eye contact
•Thoughtful use of touch
•Mirroring
•Being “in sync”
•Listen, reflect, check

Brain Wise: The 10 Wise Ways1. Wizard Brain over Lizard Brain
2. Constellation of Support
3. Recognize Red Flag Warnings
4. Exit the Emotions Elevator
5. Separate Fact from Opinion
Wise Ways6. Ask Questions
7. Identify Your Choices
8. Consequences: Now and Later; Affecting Others
9. Set Goals and Form a Plan
10.Communicate Effectively
6. Domain:Healthy Sexuality
Elements: Understanding Rules and Limitations of Sexual Behavior at Whitney
Interventions: Present and discuss Whitney Sexual Behavior Rules
Elements: Self-Regulation (see above)
Elements: Maintaining appropriate personal space (see above)Interventions: Kornblum: Chapter 2
Recreational therapy
Elements: Accurate Sexual InformationInterventions: Sex ed curriculum (medical)
Elements: Sexual Behavior in context of relationshipsInterventions: Sex ed curriculum (clinical)
Elements: Cognitive distortionsInterventions: BrainWise curriculum: Separate Fact from
Opinion
Elements: Role models and masculine identityInterventions: Circles curriculum
Family therapy Group therapy

•Domain: Self-Regulation
Elements: Behavior ManagementInterventions: Level System
Individual behavior management plan
Elements: Sensory IntegrationInterventions: Complete Sensory Profile
Introduce to Sensory Room Develop individualized sensory/self-regulation
tools Elements: Self-regulation skill training
Interventions: Daily stress buster exercises Use of biofeedback tools: Wild Divine; pulse
meters, etc. Dialectical Behavior therapy exercises:
(Linnehan)
Elements: Safe PlaceInterventions: Describe, write about, build, develop safe places
both real and imagined (visualization) EMDR: safe place installation (individual)
Elements: Adaptive Problem Solving SkillsInterventions: BrainWise curriculum