key clinical lipidology publications: 2015-16 · key clinical lipidology publications: 2015-16...
TRANSCRIPT

Key Clinical Lipidology
Publications: 2015-16
Kevin C. Maki, PhD, CLS, FNLA, FTOS, FACN
MB Clinical Research and DePaul University
Glen Ellyn and Chicago, Illinois

AFFILIATION/FINANCIAL INTERESTS
(past 12 months)
ORGANIZATION
Grants/Research Support: DuPont, AstraZeneca, ACH
Foods, Matinas BioPharma,
Shaklee, Egg Nutrition Center,
National Dairy Council, National
Cattlemen’s Beef Association,
Sancilio & Co.
Scientific Advisory Board/Consultant: AstraZeneca, Pharmavite, Matinas
BioPharma, Sancilio & Co.,
National Dairy Council, Egg
Nutrition Center, National
Cattlemen’s Beef Association
Speakers Bureau: None
Stock Shareholder: None >$10,000
Other Not Applicable
Disclosures

Key Developments in
Clinical Lipidology in 2015-16
• Ezetimibe Outcomes StudyCannon CP, et al.
• PCSK9 Inhibitor StudiesRobinson JG, et al. and Sabatine MS, et al.
• Failure of Another CETP Inhibitor TrialNicholls SJ, et al.
• Statins and Diabetes RiskMansi I, et al.
• Saturated vs. Unsaturated Fats, Carbohydrates and CHDLi Y, et al.
• NLA Recommendations: Part 1 Full Report, Part 2Jacobson TA, et al.
• Drugs for Glycemic Control and Heart Disease RiskKernan WN, et al., Zinman B, et al. and LEADER press release
• Genetic Variants Influencing TG and Coronary RiskDewey FE, et al. and Myocardial Infarction Genetics and CARDIoGRAM
Exome Consortia Investigators

Cannon CP, et al. N Engl J Med. 2015;372:2387-97.
Improved Reduction of Outcomes: Vytorin
Efficacy International Trial (IMPROVE-IT)

Cannon CP, et al. Am Heart J. 2008;156:826-32.
Blazing MA, et al. Am Heart J. 2014;168:205-212.e1.
Cannon CP, et al. N Engl J Med. 2015;372:2387-97.
IMPROVE-IT: Study Design
On treatment LDL-C = 69.5 mg/dL On treatment LDL-C = 53.7 mg/dL
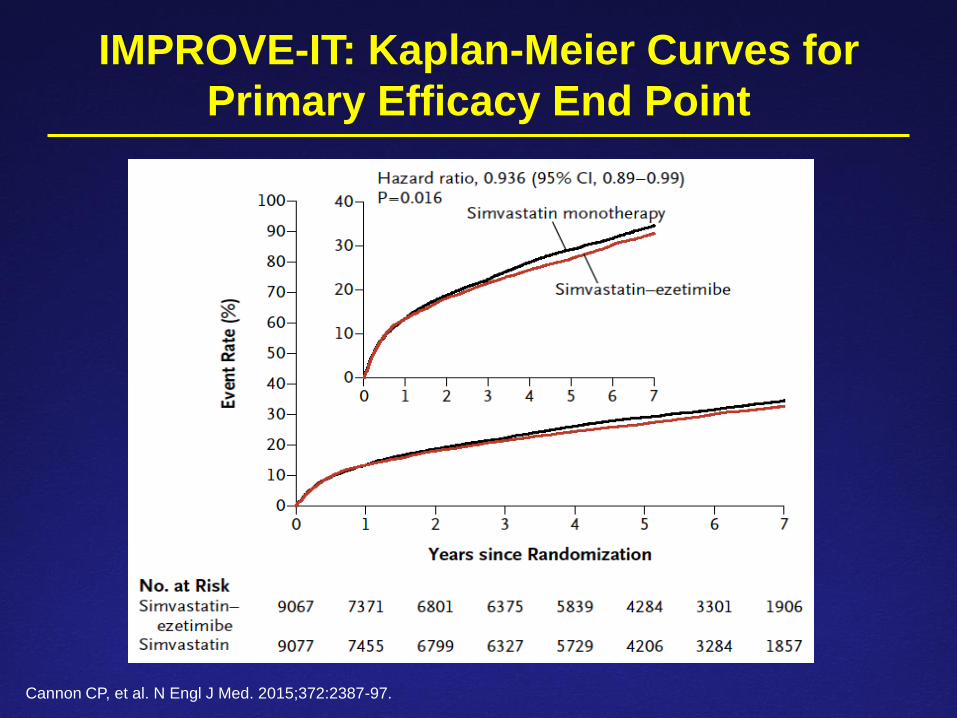
IMPROVE-IT: Kaplan-Meier Curves for
Primary Efficacy End Point
Cannon CP, et al. N Engl J Med. 2015;372:2387-97.

IMPROVE-IT: Primary and Secondary
Efficacy End Points
Cannon CP, et al. N Engl J Med. 2015;372:2387-97.

IMPROVE-IT and Statin Trials: Association
Between LDL-C Change and Clinical Benefit
Cannon CP, et al. N Engl J Med. 2015;372:2387-97.
IMPROVE-IT: Conclusions
• These results further support the efficacy of atherogenic cholesterol
lowering per se for reducing the risk for atherosclerotic
cardiovascular disease (ASCVD).
• The degree of ASCVD event reduction was consistent with the
predicted effects based on results from statin trials for the degree of
LDL-C reduction, even in the range of low LDL-C levels.
Cannon CP, et al. N Engl J Med. 2015;372:2387-97.

Proprotein Subtilisin Kexin Type 9 (PCSK9)
Inhibitors: ODYSSEY LONG TERM and OSLER
Robinson JG, et al. N Engl J Med. 2015;372:1489-99.
Sabatine MS, et al. N Engl J Med. 2015;372:1500-9.
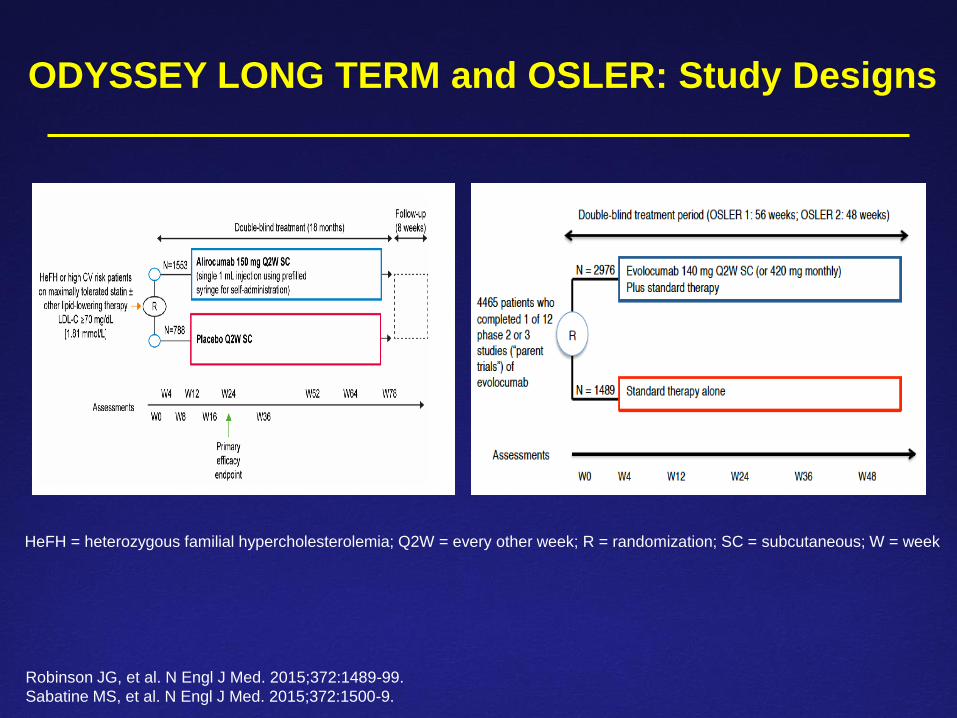
ODYSSEY LONG TERM and OSLER: Study Designs
Robinson JG, et al. N Engl J Med. 2015;372:1489-99.
Sabatine MS, et al. N Engl J Med. 2015;372:1500-9.
HeFH = heterozygous familial hypercholesterolemia; Q2W = every other week; R = randomization; SC = subcutaneous; W = week

ODYSSEY LONG TERM (Alirocumab) and OSLER
(Evolocumab): LDL-C Levels
Robinson JG, et al. N Engl J Med. 2015;372:1489-99.
Sabatine MS, et al. N Engl J Med. 2015;372:1500-9.

ODYSSEY LONG-TERM (Alirocumab) and OSLER
(Evolocumab): Incidence of CV Events
Robinson JG, et al. N Engl J Med. 2015;372:1489-99.
Sabatine MS, et al. N Engl J Med. 2015;372:1500-9.

Assessment of Clinical Effects of Cholesteryl Ester
Transfer Protein Inhibition with Evacetrapib in Patients
at High Risk for Vascular Outcomes (ACCELERATE)
• Designed to evaluate the efficacy and safety of evacetrapib, a
cholesteryl ester transfer protein (CETP) inhibitor in participants
with high-risk CVD
• Multi-center, randomized, double-blind, placebo-controlled trial of
12,095 patients conducted at 540 sites in 37 countries
• Primary outcome measure: time to first occurrence of any
component of the composite CV events of CV death, MI, stroke,
coronary revascularization, or hospitalization for unstable angina
• Trial terminated due to insufficient efficacy
• Lilly discontinued development of evacetrapib for the treatment of
high-risk CVD and concluded other studies in the program.
https://clinicaltrials.gov/ct2/show/NCT01687998
https://investor.lilly.com/releasedetail.cfm?releaseid=936130
Nicholls SJ, et al. Am Heart J. 2015;170:1061-9.

Significance of Failure of ACCELERATE
• CETP inhibitors are the most effective high-density lipoprotein
(HDL)-raising agents developed to date; they roughly double HDL-
C concentration. They also reduce LDL-C. However, clinical
outcomes trials conducted to date have failed:
Torcetrapib increased blood pressure; net CV detriment (2006)
Dalcetrapib showed no clinically meaningful CV efficacy (2012)
Evacetrapib showed no clinically meaningful CV efficacy (2015)
• The Randomized Evaluation of the Effects of Anacetrapib Through
Lipid-modification (REVEAL) is an ongoing Phase 3 randomized
controlled trial examining the potential of anacetrapib to reduce
CVD. Data collection planned through 2017.
Page MM, et al. Expert Opin Pharmacother. 2015;Dec 28:1-7 [Epub ahead of print].
Barter PJ, Rye KA. Clin Ther. 2015;37:2716-31.
Hovingh GK, et al. Circulation. 2015;132:433-40.
https://clinicaltrials.gov/ct2/show/NCT01252953

Statins and Diabetes
Mansi I, et al. J Gen Intern Med. 2015;30:1599-610.

Statins and Diabetes:
Retrospective Study Cohort
Mansi I, et al. J Gen Intern Med. 2015;30:1599-610.
CCI = Charlson Comorbidity Index
CVS = Cardiovascular

Statins and New-Onset Diabetes Mellitus and
Diabetes Complications
Mansi I, et al. J Gen Intern Med. 2015;30:1599-610.
Outcome Statin
non-users
(N = 3351)
Statin
users
(N = 3351)
Odds ratio
(95% CI)
P-value
Diabetes Mellitus 19.4% 30.9% 1.87
(1.67, 2.01)
<0.0001
Diabetes Mellitus with
Complications
2.1% 5.0% 2.50
(1.88, 3.32)
<0.0001
Outcome High-
intensity
statins
(N = 1155)
Lower-
intensity
statins
(N = 2827)
Adjusted*
odds ratio
(95% CI)
P-value
Diabetes Mellitus 39.3% 29.7% 1.50
(1.30, 1.73)
<0.0001
Diabetes Mellitus with
Complications
8.2% 4.2% 1.97
(1.49, 2.61)
<0.0001
*Adjusted for propensity score

Statins and Diabetes: Conclusions
• Most prior studies of statin use and increased incidence of new-
onset diabetes have been conducted in higher risk populations.
This study demonstrated an increased risk for diabetes among
statin users vs. non-users among healthy U.S. adults, and also
reported an increased risk for diabetes complications.
• Generally, the increased risk for diabetes mellitus is more than
offset by the reduced risk for CVD associated with statin use,
however, this study was not designed to investigate the trade-offs
between risks and benefits.
Mansi I, et al. J Gen Intern Med. 2015;30:1599-610.
A Prospective Cohort Study of Saturated Fats Compared with
Unsaturated Fats and Sources of Carbohydrates in Relation
to Risk of Coronary Heart Disease
• 84,628 women (Nurses’ Health Study, 1980-2010) and 42,908
men (Health Professionals Follow-up Study, 1986-2010)
• Subjects were free of diabetes, CVD, and cancer
• Diet assessed by semi-quantitative food frequency
questionnaire every 4 years
• Follow-up of 24-30 years
• 7,667 documented incident cases of CHD
Li Y, et al. J Am Coll Cardiol. 2015;66:1538-48.

Estimated Percent Changes in CHD Risk
Associated with Isocaloric Substitutions
of Dietary Components for SFAs
Li Y, et al. J Am Coll Cardiol. 2015; 66:1538-48.
5%
-15%
-25%
2%
-9%

Implications of Findings from Dietary
Component Substitution Analyses
• Results from these two large, prospective cohorts of U.S. men
and women suggest that consumption of unsaturated fats and/or
high-quality carbohydrates may be used to replace saturated fats
(and refined starches/added sugars) to reduce CHD risk.
• These findings support the recommendations of the Dietary
Guidelines for Americans to reduce intakes of saturated fats and
refined starches/added sugars and to replace these dietary
components with unsaturated fats and carbohydrates from whole
grains.
Li Y, et al. J Am Coll Cardiol. 2015;66:1538-48.
National Lipid Association (NLA)
Recommendations Part 1 – Full Report
Jacobson TA, et al. J Clin Lipidol. 2015;9:129-69.
NLA Part 2 Recommendations
Jacobson TA, et al. J Clin Lipidol. 2015;9:S1-S122.

Key Differences Between the ACC/AHA Guidelines
and the NLA Recommendations
• Methods of CVD risk assessment• Four statin benefit groups, primary prevention risk assessment based
largely on age and quantitative risk scoring (ACC/AHA)
• Risk categories + risk factor counting + supplemental methods
including quantitative risk scoring (NLA)
• Use of treatment goals for atherogenic cholesterol (NLA)
• Inclusion of non-high-density lipoprotein cholesterol (non-HDL-C) as
a treatment target
• Approach to dietary cholesterol• No recommendation from the ACC/AHA
• Limitation of dietary cholesterol recommended by the NLA Expert Panel
Stone NJ, et al. J Am Coll Cardiol. 2014;63(25 Pt B):2889-934.
Goff DC Jr., et al. J Am Coll Cardiol. 2014;63(25 Pt B):2935-59.
Eckel RH, et al. J Am Coll Cardiol. 2014;63(25 Pt B):2960-84.
Jacobson TA, et al. J Clin Lipidol. 2015;9:129-69.

ACC Expert Consensus Clinical
Pathway on Lipid Management
• Writing committee of clinical experts was assembled following the
LDL: Address the Risk Think Tank meeting in September 2015.
• Participants identified the need for expert consensus document on
incorporation of non-statin therapies into treatment strategies for
higher risk patients if the response to statins is deemed inadequate.
• A 9-person writing committee was selected, chaired by Donald
Lloyd-Jones, MD and included a majority of members without
relevant relationships with industry (RWI); authors with relevant RWI
were not permitted to draft or vote on content or recommendations
pertaining to their RWI.
• Peer reviewers were established and the respective executive
boards of the professional societies provided final review and
endorsement of the document.

Questions Addressed by the ACC
Expert Consensus Writing Committee
1) In whom should non-statin therapies be considered?
1) In what situations should non-statin therapies be considered, i.e.
when is the amount of LDL-C lowering (percent LDL-C reduction or
LDL-C range achieved on therapy) less than anticipated, less than
desired, or inadequate, and what should be done with patients who
are truly statin intolerant?
1) If non-statin therapies are to be added, which agents or therapies
should be considered and in what order?

Insulin Resistance Intervention
after Stroke (IRIS) Trial
Kernan WN, et al. N Engl J Med. 2016;Published online.

Pioglitazone Effects on CVD and Diabetes
Incidence in the IRIS Trial
0
1
2
3
4
5
6
7
8
9
Pioglitazone (N = 1939) Placebo (N = 1937)
Incid
ence o
f D
iabe
tes M
elli
tus (
%)
Hazard Ratio, 0.48 (95% CI 0.33-0.69)
P < 0.001 7.7%
CVD Events Type 2 Diabetes Mellitus
Kernan WN, et al. New Engl J Med. 2016;Published online.
3.8%
Cardiovascular Outcome Event Trial in Type 2
Diabetes Mellitus Patients (EMPA-REG OUTCOME)
Zinman B, et al. New Engl J Med. 2015;373:2117-28.

Empagliflozin Effects on Cardiovascular
Outcomes in the EMPA-REG OUTCOME Trial
Primary composite outcome was death from CV causes,
nonfatal myocardial infarction, or nonfatal stroke
Zinman B, et al. New Engl J Med. 2015;373:2117-28.

Marso SP, et al. Am Heart J. 2013;166:823-30.
http://globenewswire.com/news-release/2016/03/04/816952/0/en/Victoza-significantly-reduces-the-risk-of-major-adverse-
cardiovascular-events-in-the-LEADER-trial.html
Liraglutide Effect and Action in Diabetes: Evaluation
of Cardiovascular Outcome Results (LEADER) Trial
• Multicenter, international (32 countries), randomized,
double-blind placebo-controlled trial• 9,340 adults with type 2 diabetes at high risk of major adverse
CV events
• Liraglutide (1.2 and 1.8 mg) compared to placebo, both in
addition to standard of care; patients followed for 3.5-5 y
• Primary endpoint: composite outcome of the first occurrence
of CV death, non-fatal myocardial infarction or non-fatal stroke
• The study met its primary endpoint and demonstrated
a statistically significant reduction in CV risk• Detailed results to be presented at the American Diabetes
Association Scientific Sessions, June 2016

Dewey FE, et al. N Engl J Med. 2016;Published online.
Myocardial Infarction Genetics and CARDIoGRAM Exome Consortia Investigators. New Engl J Med. 2016;Published online.
Genetic Variants Influencing TG Levels and
Risk of Coronary Artery Disease (CAD)
Loss-of-function Mutations in ANGPTL4 and CAD
• DNA sequencing in 72,868 patients with CAD and
120,770 controls without CAD (Consortia Investigators) Carriers of loss-of function mutations in ANGPTL4 had 35%
lower TG levels than non-carriers (p = 0.003)
Odds ratio for myocardial infarction in carriers vs. non-carriers
was 0.47 (p = 0.04)
• DNA sequencing in 10,552 patients with CAD and
29,223 controls without CAD (Dewey et al.) Carriers of the E40K loss-of-function mutation in ANGPTL4
had 13% lower TG and 7% higher HDL-C than non-carriers
Odds ratio for CAD in carriers vs. non-carriers of the E40K
variant was 0.81 (p = 0.002)
Dewey FE, et al. N Engl J Med. 2016;Published online.
Myocardial Infarction Genetics and CARDIoGRAM Exome Consortia Investigators. New Engl J Med. 2016;Published online.
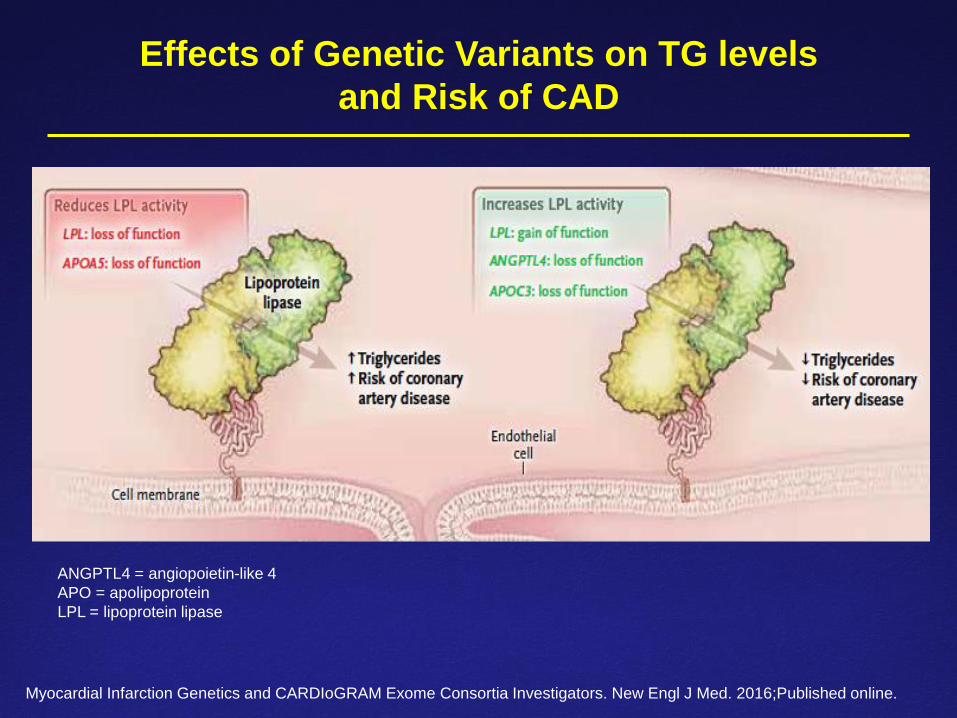
Effects of Genetic Variants on TG levels
and Risk of CAD
ANGPTL4 = angiopoietin-like 4
APO = apolipoprotein
LPL = lipoprotein lipase
Myocardial Infarction Genetics and CARDIoGRAM Exome Consortia Investigators. New Engl J Med. 2016;Published online.

Summary/Take Home Messages
• 2015-16 saw some exciting advancements in the understanding of CVD and
lipid-altering therapies, and drugs for glycemic control, for reducing risk for CVD
Clinical trials with PCSK9 inhibitors and ezetimibe showed evidence that
further supports the view that lower is better for LDL-C.
There is increasing evidence to suggest that statins increase the risk for
developing new-onset diabetes mellitus.
CV outcomes benefits from raising HDL-C via CETP inhibition continues to
lack clinical trial support.
Unsaturated fats and high quality carbohydrates are recommended to
replace saturated fats to reduce risk for CHD in the 2015 Dietary Guidelines
for Americans. Data from large prospective cohort studies in men and
women support these recommendations.
Hypoglycemic drugs (pioglitazone, empagliflozin, liraglutide) were shown to
decrease CV events in outcomes trials.
Carriers of genetic variants resulting in reduced TG levels were shown to
have lower risk of CAD than non-carriers.

Thank You
QUESTIONS?