knee and hip pain –new approaches and options but don’t
TRANSCRIPT

24th Annual Pain Management Symposium 10/23/2020
1
Basic Fluoroscopic and Lumbar Spine Anatomy
Knee and Hip Pain – New Approaches and Options but Don’t Forget the Basics
Zachary L. McCormick, MD FAAPMRAssociate Professor, PM&R; University of Utah School of Medicine
Chief, Spine and Musculoskeletal Rehabilitation Section
Director, Clinical Spine Research
Director, Interventional Spine Fellowship
1

24th Annual Pain Management Symposium 10/23/2020
2
The BasicsDisclosures
• Research Grants: Foundation of PM&R, SIS, RSNA Research & Education Foundation, EpiMed, Avanos, Relievant
• Board of Directors: SIS, PSPS
• Speaker: AAN, AAPM, NASS, PSPS, SIS
• Journal Editorial Boards: Pain Medicine, The Spine Journal, Physical Medicine & Rehabilitation
• Consulting: medicolegal, Soal Therapeutics
2

24th Annual Pain Management Symposium 10/23/2020
3
Spectrum of Care
Continued Pain and Disability Despite Treatment
Weight loss
Bracing
Cane/assistive device
Ice/cryotherapy, Heat
Oral Anti-inflam meds
Targeted Exercise- Quad, hip girdle, core- Bike/swimming
Surgery-Arthroplasty
Formal Physical Therapy- Strength, mobility- Gait- Ergonomics- Pacing- Graded home exercise
program
Joint Injection- Steroid- Hyaluronic Acid- Regenerative agents
Joint Denervation or Neuromodulation
- Radiofrequency- Phenol/alcohol- Peripheral nerve stimulation?
- Dorsal root ganglion stimulation?
3

24th Annual Pain Management Symposium 10/23/2020
4
Weight Loss
Bracing
Cane/assistive device
Ice/cryotherapy, Heat
Oral Anti-inflam meds
Targeted Exercise- Quad, hip girdle, core- Bike/swimming
4

24th Annual Pain Management Symposium 10/23/2020
5
Formal Physical Therapy- Strength, mobility- Gait- Ergonomics- Pacing- Graded home exercise
program
Individualized to unique anatomy and biomechanics
Active > Passive
Quadriceps, hip girdle, core strength - Address imbalances
Gait, movement, lifting mechanics
Techniques for pain exacerbations, pacing
Graded independent exercise program
5

24th Annual Pain Management Symposium 10/23/2020
6
AAOS
2013 2017
6

24th Annual Pain Management Symposium 10/23/2020
7
AAOS
7

24th Annual Pain Management Symposium 10/23/2020
8
AAOS
8

24th Annual Pain Management Symposium 10/23/2020
9
AAOS
9

24th Annual Pain Management Symposium 10/23/2020
10
Injectables?
10

24th Annual Pain Management Symposium 10/23/2020
11
Laudy ABM, et al. Br J Sports Med2015;49:657–672.
11

24th Annual Pain Management Symposium 10/23/2020
12
12

24th Annual Pain Management Symposium 10/23/2020
13
13

24th Annual Pain Management Symposium 10/23/2020
14
Pas HIMFL, et al. Br J Sports Med 2017;0:1–10.
14

24th Annual Pain Management Symposium 10/23/2020
15
15

24th Annual Pain Management Symposium 10/23/2020
16
AAOS Injectables?
16

24th Annual Pain Management Symposium 10/23/2020
17
Injectables?
17
24th Annual Pain Management Symposium 10/23/2020
18
Joint Denervation
Indications• Continued pain and functional disability despite conservative
management • Desire to avoid surgery• Inability to undergo surgery
18

24th Annual Pain Management Symposium 10/23/2020
19
• Thermocoagulation of sensory nerves
• Radiofrequency Energy– Vibration of H2O molecules ‐> heating
– Predictable + Controlled lesion size
Joint Denervation- Radiofrequency
19

24th Annual Pain Management Symposium 10/23/2020
20
Knee Joint Denervation
20

24th Annual Pain Management Symposium 10/23/2020
21
The BasicsGenicular Nerve Radiofrequency Ablation
• Genicular nerves– Sensory– No motor fibers
• Generally Safe
Joint Denervation- Radiofrequency
21

24th Annual Pain Management Symposium 10/23/2020
22
The Basics
• Genicular RFA > sham RFA (Choi)• Genicular RFA > IA steroid injection (Davis)• Genicular RFA > IA hyaluronic acid + prp (Shen)• Genicular RFA > PT and NSAIDs
50% pain reduction responder rate at 6 month f/u: 55‐75% *practice audit data demonstrates responder rate as as low as 35%
Current Outcome Literature
22

24th Annual Pain Management Symposium 10/23/2020
23
The BasicsOptimizing Outcomes: Predictive Factors
23

24th Annual Pain Management Symposium 10/23/2020
24
The Basics
24

24th Annual Pain Management Symposium 10/23/2020
25
The BasicsOptimizing Outcomes: Prognostic Block Paradigm
25

24th Annual Pain Management Symposium 10/23/2020
26
Prognostic Genicular Blocks
Choi et al: 2mL of 2%; >50% relief
Typical: 1mL of 2% lidocaine; >50% relief
26

24th Annual Pain Management Symposium 10/23/2020
27
Prognostic Block: 1mL of 2% lidocaine; >50% relief
27

24th Annual Pain Management Symposium 10/23/2020
28
Prognostic Block: 1mL of 2% lidocaine; >50% relief
‐ Choi et al: 2mL of 2%; >50% relief
28

24th Annual Pain Management Symposium 10/23/2020
29
29

24th Annual Pain Management Symposium 10/23/2020
30
The BasicsOptimizing Outcomes: Correct Targets?
30

24th Annual Pain Management Symposium 10/23/2020
31
Horner & Dellon 1994
Horner G, Dellon AL: Innervation of the human knee joint and implications for surgery. Clin Orthop 301:221‐226, 1994.
31

24th Annual Pain Management Symposium 10/23/2020
32
Choi et al 2011
Choi W‐JJ, Hwang S‐JJ, Song J‐GG, Leem J‐GG, Kang Y‐UU, Park P‐HH, et al. Radiofrequency treatment relieves chronic knee osteoarthritis pain: A double‐blind randomized controlled trial. Pain. 2010/11/09. 2011 Mar;152(3):481–7.
32
24th Annual Pain Management Symposium 10/23/2020
33
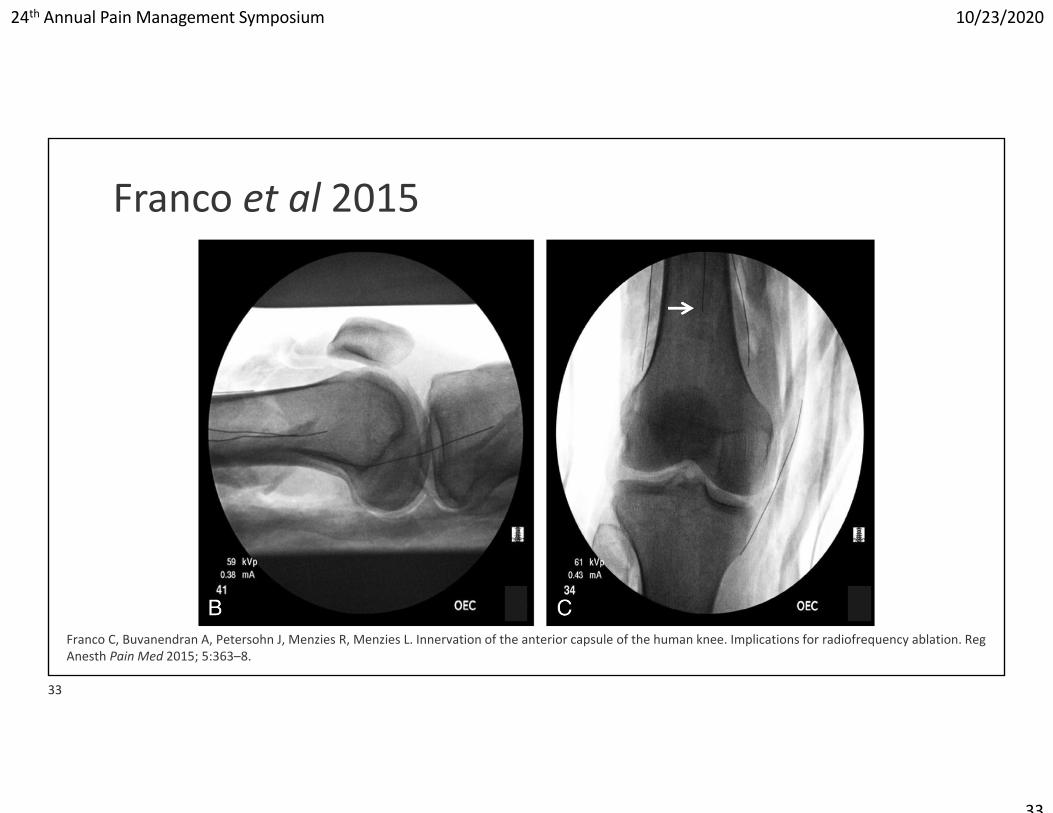
Franco et al 2015
Franco C, Buvanendran A, Petersohn J, Menzies R, Menzies L. Innervation of the anterior capsule of the human knee. Implications for radiofrequency ablation. RegAnesth Pain Med 2015; 5:363–8.
33
24th Annual Pain Management Symposium 10/23/2020
34
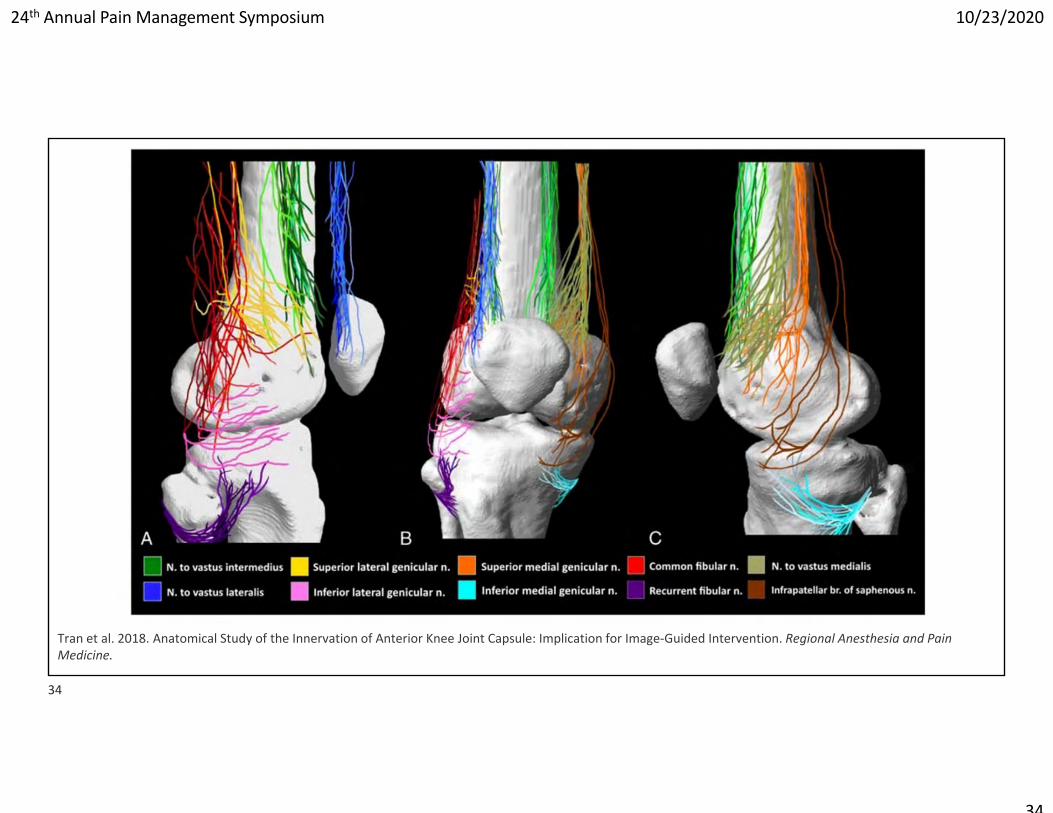
Tran et al. 2018. Anatomical Study of the Innervation of Anterior Knee Joint Capsule: Implication for Image‐Guided Intervention. Regional Anesthesia and Pain Medicine.
34

24th Annual Pain Management Symposium 10/23/2020
35
Tran et al. 2018. Anatomical Study of the Innervation of Anterior Knee Joint Capsule: Implication for Image‐Guided Intervention. Regional Anesthesia and Pain Medicine.
35

24th Annual Pain Management Symposium 10/23/2020
36
36

24th Annual Pain Management Symposium 10/23/2020
37
37

24th Annual Pain Management Symposium 10/23/2020
38
Hip Joint Denervation
38
24th Annual Pain Management Symposium 10/23/2020
39
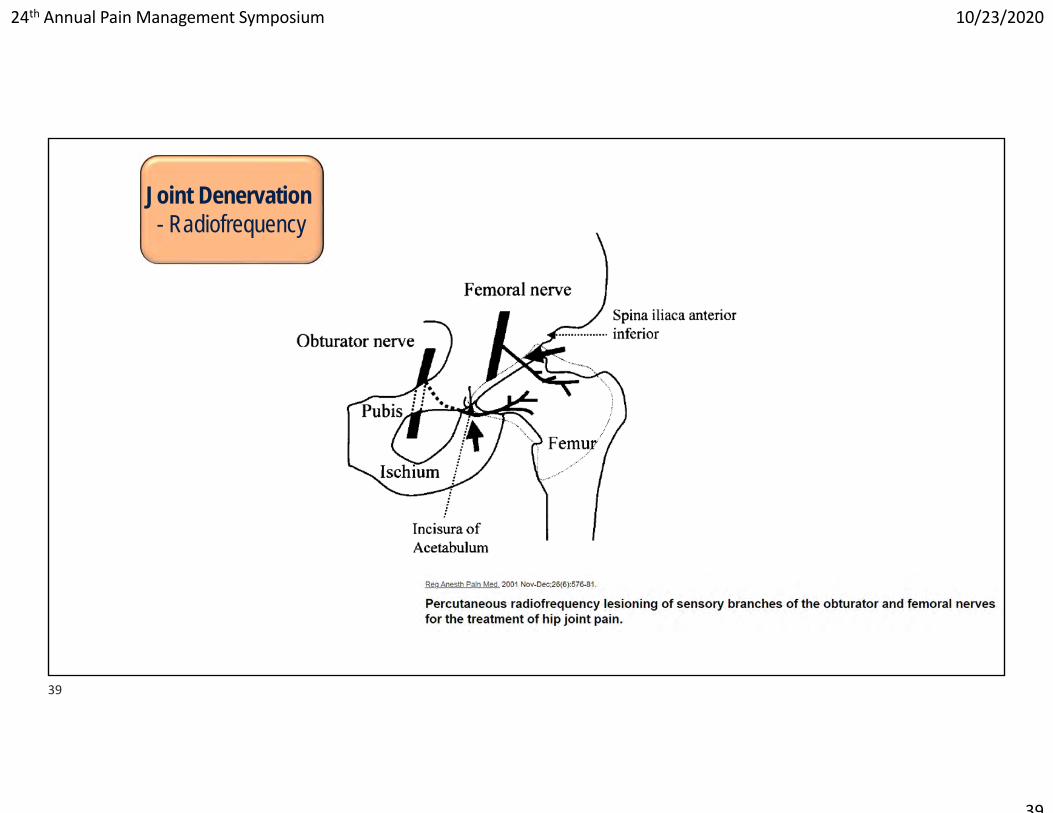
Joint Denervation- Radiofrequency
39

24th Annual Pain Management Symposium 10/23/2020
40
Obturator branchesJoint Denervation
- Radiofrequency
40
24th Annual Pain Management Symposium 10/23/2020
41
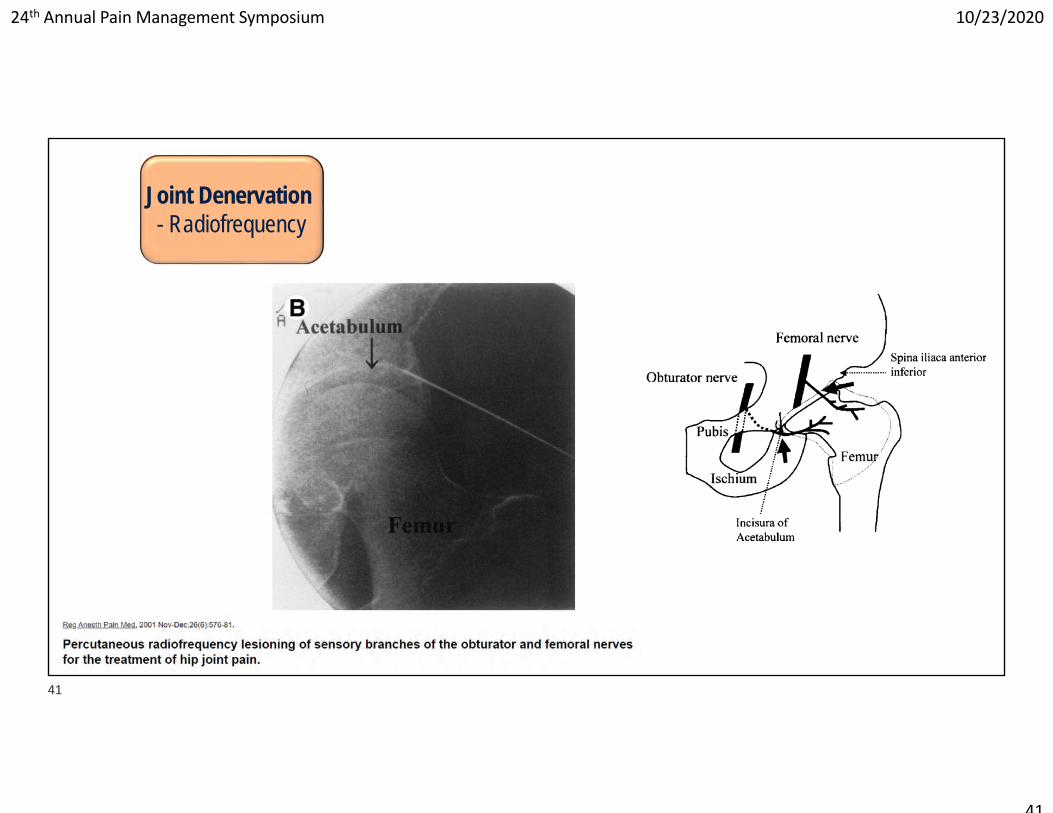
Femoral branchesJoint Denervation
- Radiofrequency
41

24th Annual Pain Management Symposium 10/23/2020
42
Joint Denervation- Radiofrequency
42

24th Annual Pain Management Symposium 10/23/2020
43
Limitations
• Multiple nerves supply sensation to the hip joint• Obturator nerve branches• Femoral nerve branches• Accessory femoral and accessory obturator nerves• Nerve to the quadratus femoris• Superior gluteal nerve• Direct branches from the sciatic nerve
• Parallel placement of electrode?• Femoral Artery and Vein
43

24th Annual Pain Management Symposium 10/23/2020
44
2. Currently limited evidenceAuthor, Year N
Time of Follow‐up Assessment Outcome
Akatov, 1997 13 36 months 92% (12) patients with “pain relief”*
Kawaguchi, 2001 141 month‐11 months
86% (12) patients with >50% pain reduction*‐60% pain reduction†
Malik, 2003 43 months‐1‐3 months
75% (3) patients with >50% pain reduction*‐30‐70% pain reduction†
Rivera, 2012 18 6 months44% (8) patients with > 50% pain reduction‐33% pain reduction at 6 months†
Cortiñas‐Sáenz, 2014 3
1 month‐6 months
100% (3) of patients with >50% pain reduction* **50‐80% pain reduction‐100% (3) of patients with >50% pain reduction**50‐80% pain reduction†
Kapural, 2018 23 6 months >80% pain reduction*
*Categorical †Con nuous**Calculated from primary data
44
24th Annual Pain Management Symposium 10/23/2020
45
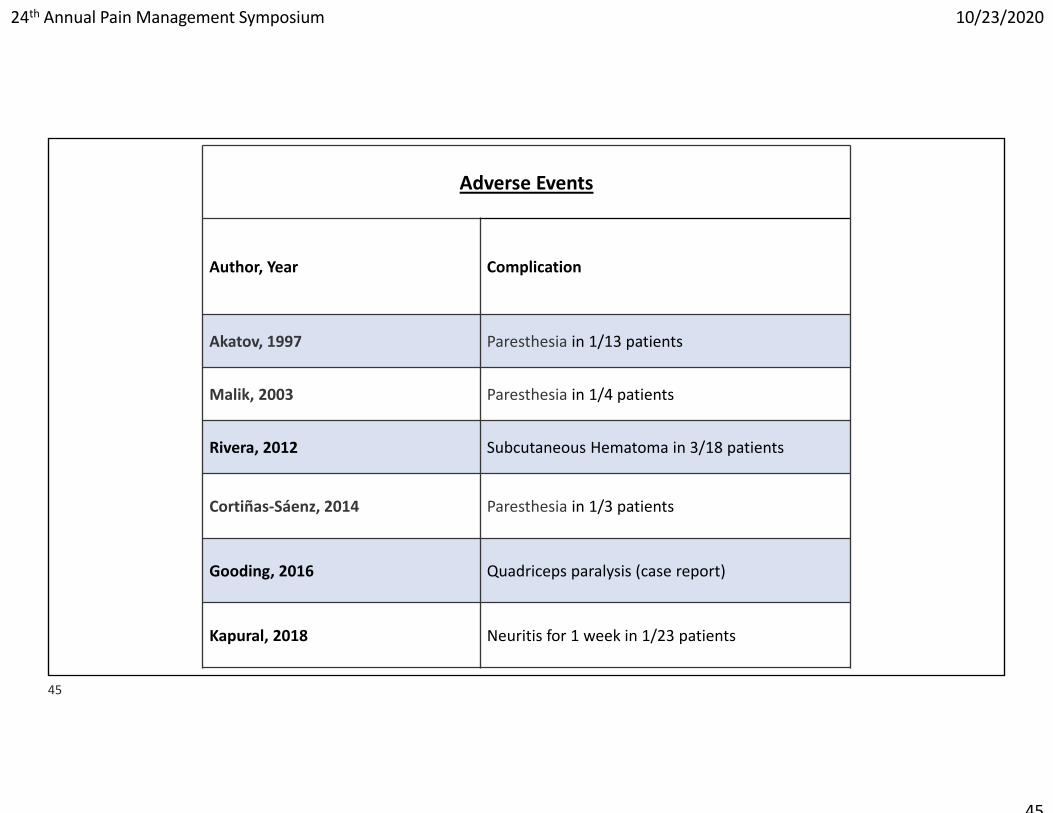
2. Currently limited evidenceAdverse Events
Author, Year Complication
Akatov, 1997 Paresthesia in 1/13 patients
Malik, 2003 Paresthesia in 1/4 patients
Rivera, 2012 Subcutaneous Hematoma in 3/18 patients
Cortiñas‐Sáenz, 2014 Paresthesia in 1/3 patients
Gooding, 2016 Quadriceps paralysis (case report)
Kapural, 2018 Neuritis for 1 week in 1/23 patients
45

24th Annual Pain Management Symposium 10/23/2020
46
Spectrum of Care
Continued Pain and Disability Despite Treatment
Weight loss
Bracing
Cane/assistive device
Ice/cryotherapy, Heat
Oral Anti-inflam meds
Targeted Exercise- Quad, hip girdle, core- Bike/swimming
Surgery-Arthroplasty
Formal Physical Therapy- Strength, mobility- Gait- Ergonomics- Pacing- Graded home exercise
program
Joint Injection- Steroid- Hyaluronic Acid- Regenerative agents
Joint Denervation or Neuromodulation
- Radiofrequency- Phenol/alcohol- Peripheral nerve stimulation?
- Dorsal root ganglion stimulation?
46

24th Annual Pain Management Symposium 10/23/2020
47
Summary• Treatments range from conservative to surgical
‐ Guideline Concordant: weight loss, PT, NSAIDs, Tramadol, steroid injection (mild/mod OA), HMW hyaluronic acid.
‐ Lack of positive or negative rec: passive PT modalities, TENS, acupuncture, medial compartment unloading (foot orthotic, knee brace), steroid injection (all grades of OA), PRP injection.
‐ Guideline Discordant: LMW hyaluronic acid, stem cell injection.…A guidelines is just that… may not apply to each unique patient
• Regenerative treatments ‐ Theoretical benefits vs. repeated steroid injections; Literature is fairly young.
• Radiofrequency neurotomy‐ Encouraging outcomes; not yet optimized
47

24th Annual Pain Management Symposium 10/23/2020
48
Thank You!
Zachary McCormick, MDAssociate Professor, PM&R; University of Utah School of Medicine
Chief, Spine and Musculoskeletal Rehabilitation SectionDirector, Clinical Spine Research
Director, Interventional Spine [email protected]
48