la terapia medica e chirurgica della malattia perianale di crohn - gastrolearning®
TRANSCRIPT

La Terapia Medica e Chirurgica della Malattia Perianale di Crohn
Paolo Gionchetti Università di Bologna

Clinical Markers of Disabling Disease
– extensive disease
– disease in multiple sites
– younger patients
– perianal disease at diagnosis
– Severe rectal involvement
– EIMs
Beaugerie L, Gastroenterology 2005
0.5 1 2 3 4 5
2.1 [1.3–3.6]
1.8 [1.2–2.8]
3.1 [2.2–4.4]
perianal disease
age < 40 years
steroid for first flare
OR (95%CI)

Spectrum of Crohn’s anal pathology
Good prognosis
Poor prognosis
Skin tags
Fissures ComplexFistulae
Strictures
Deep cavitating ulcers
SimpleFistulae
ALEXANDER- WILLIAMS, 1980
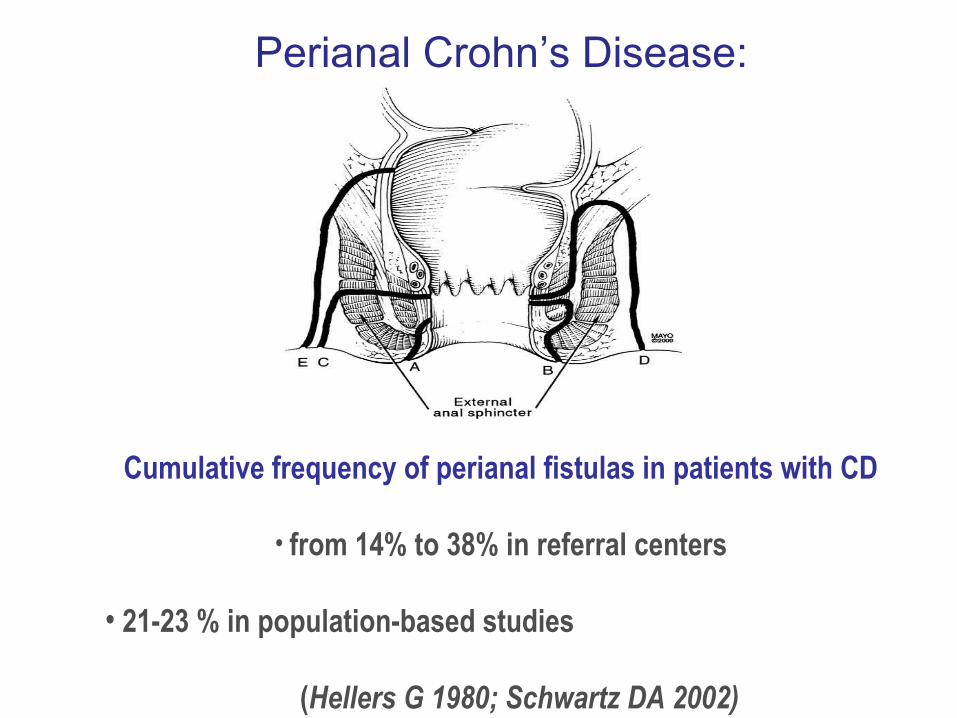
Cumulative frequency of perianal fistulas in patients with CD
• from 14% to 38% in referral centers
• 21-23 % in population-based studies
(Hellers G 1980; Schwartz DA 2002)
Perianal Crohn’s Disease: Epidemiology

Cu
mu
lati
ve in
cid
ence
of
f
istu
la (
%)
00 2015105
100
80
60
40
20
Time from diagnosis (yr)
Any fistula
Perianal fistula
The cumulative risk of at least 1 perianal fistula
after 1 year was 12% (95% CI, 7% to 17%)
after 5 years was 15% (95% CI, 9% to 20%)
after 10 years was 21% (95% CI, 14% to 28%),
after 20 years was 26% (95% CI, 16% to 36%)
The Natural History of Fistulizing Crohn’s Disease in Olmsted County, Minnesota
D.A.Schwartz , Gastroenterology 2002
Population-based study
83% required operations 23% required bowel resection

ileal
ileocolonic
colonic
colonic with rectalinvolvement
Incidence of perianal lesions related to the site of intestinal Crohn’s disease
Hellers G, 1980

Perianal Fistulas in CD: classification
Complex fistulas carry a worse prognosis in relation
to the need for and extent of surgery.
Simple fistula Inter-sphincteric / low trans-sphincteric with one primary track and NO extensions or abscesses
Complex fistula Inter-sphincteric / trans-sphincteric with extensions or abscesses; extra-sphincteric; supralevator; recto-vaginal; anal strictures

Clinical Course of Crohn’s FistulaBell et al APT 2003
• 87 patients treated fistula 6 years previously• Median age 35 years
• Median duration Crohn’s disease 8 years
• Median duration fistula 3 years at presentation
• 14% had fistula(s) before diagnosis of Crohn’s• 15% fistulas in same year as Crohn’s diagnosis• 70% fistulas followed Crohn’s diagnosis

Clinical Course of Crohn’s FistulaBell et al APT 2003
Number of fistulas• Single fistula one third• Two or more fistulas two thirds
Disease distribution
•Colonic or ileocolonic disease 85 % •Isolated small bowel disease 14 % •Isolated anal disease 1 %

PERIANAL CROHN’S DISEASEPredictors of Need for Permanent Diversion
Galandiuk S, Ann Surg, 2005
Anal stenosis in colonic Crohn’s
Disease is ultimately the only strong predicting
factor for a permanent stoma

Perianal DiseaseDiagnosis
Statement 5A
Pelvic MRI should be the initial procedure complementing examination under anaesthetic (EUA) because it is accurate and non-invasive, although it is not needed routinely in simple fistulae [EL 2b, RG B]EUA considered the gold standards only in the hands of an experienced surgeon [EL 5, RG D]Ano-rectal ultrasounds require expertise, but can be equivalent to MRI in complementing EUA if rectal stenosis has been excluded [EL 2b, RG B]Fistulography is not recommended [EL 3, RG C]As the presence of concomitant rectosigmoid inflammation has prognostic and therapeutic relevance, proctosigmoidoscopy should be used routinely in the initial evaluation [EL 2b, RG B]
Orlando A et al Dig Liver Dis 2010

Perianal DiseaseDiagnosis
Statement 5A
Pelvic MRI should be the initial procedure complementing examination under anaesthetic (EUA) because it is accurate and non-invasive, although it is not needed routinely in simple fistulae [EL 2b, RG B]EUA considered the gold standards only in the hands of an experienced surgeon [EL 5, RG D]Ano-rectal ultrasounds require expertise, but can be equivalent to MRI in complementing EUA if rectal stenosis has been excluded [EL 2b, RG B]Fistulography is not recommended [EL 3, RG C]As the presence of concomitant rectosigmoid inflammation has prognostic and therapeutic relevance, proctosigmoidoscopy should be used routinely in the initial evaluation [EL 2b, RG B]
Orlando A et al Dig Liver Dis 2010

Therapeutic goals in the management of fistulizing CD
Control overall disease activity
Induce closure of fistulas
Maintain closure of fistulas
Limit scope of surgical
intervention
Improve quality of life
Cooperation between gastroenterologist Cooperation between gastroenterologist and surgeonand surgeon

“A surgeon with a probe can be more dangerous than a monkey with a pistol”
No role for corticosteroidsSparberg 1966; Jones, Lennard-Jones 1966
Use of steroids increased the need for
surgery

Antibiotics
Drugs Evidence Effect
Metronidazole
20 mg/kg
Ciprofloxacin
1−1.5 g
Open-limited
Open-limited
Improvement in 30−50% but early relapse
Improvement in 30−50% but early relapse
Bernstein et al 1980; Brandt et al 1982; Jakobovits et al 1984; Turunen et al 1989; Solomon et al 1993
Useful short-term therapies to decrease or stop drainage but
relapse is immediate upon discontinuation and side effects can be important
AZA / 6-MP
• No RCTs for closure of fistula as primary endpoint.
• Data favoring use: meta-analysis of 5 RCTs with fistula closure as secondary endpoint + uncontrolled case series. Pearson Ann Intern Med 1995;122:132-42.
• Appear effective in closing and maintaining closure of perianal fistulas.
Korelitz Am J Gastroenterol 1993;88:1198-1205.
Effective…
but slow and incomplete

Cyclosporin
Author n Results
Lichtiger 1990Hanauer -Smith 1993
Present - Lichtiger 1994Markowitz 1993O’Neill 1997Hinterleitner 1997Egan et 1998
105
16
879
6/10 response – all relapseClosure of 10/12 fistulas after mean of 7.9 days (range 3-28) – 2 relapses14/16 (88%) response – 5 relapses NS pediatric study7/8 response – all relapsedAll response – 5 relapsed7/9 (relapse in 5 after stop)
Up to 80% response but early relapse!

Treatment of fistulas in CDTacrolimus
N= 48 Design: 10 wks, double-blind, placebo controlled trial Treatments: Tacrolimus 0,2 mg/kg/day orally or placebo End points: primary: > 50% reduction of draining fistulas;
secondary: closure of all fistulas Results:
• Primary endpoint: tacrolimus 43% vs placebo 8% (p< 0.004)• Secondary endpoint: tacrolimus 10% vs placebo 8% (p= NS)
Safety• Side effects: 95% tacrolimus vs 76% placebo (p< 0.05)• Nephrotoxicity: tacrolimus 38% vs 0% placebo
Sandborn et al, Gastroenterology 2005
Effective… but no closure?
Side effects!!
Perianal DiseaseDiagnosis
Statement 5A
Pelvic MRI should be the initial procedure complementing examination under anaesthetic (EUA) because it is accurate and non-invasive, although it is not needed routinely in simple fistulae [EL 2b, RG B]EUA considered the gold standards only in the hands of an experienced surgeon [EL 5, RG D]Ano-rectal ultrasounds require expertise, but can be equivalent to MRI in complementing EUA if rectal stenosis has been excluded [EL 2b, RG B]Fistulography is not recommended [EL 3, RG C]As the presence of concomitant rectosigmoid inflammation has prognostic and therapeutic relevance, proctosigmoidoscopy should be used routinely in the initial evaluation [EL 2b, RG B]
Orlando A et al Dig Liver Dis 2010
Treatment of perianal fistulizing CD
ECCO Statement 9GThe presence of a perianal abscess should be ruled-out and if present should be drained. Antibiotics and/or Azathioprine/6-mercaptopurine should be used as first choice for complex perianal Crohn’s disease with surgical therapy despite a lack of clinical trials [EL4, RG D]. Adalimumab or Infliximab should be used as a second line treatment [EL1b, RG B].

InfliximabPresent et al. NEJM 1999;34:1398-1405
Placebo-controlled
tr ial
94 patients
3 infusions of
inf l iximab
68% clinical
response
~50% closed all
f istulas
Median time to achieve response was 2 weeks

Infliximab - Accent IISands et al. NEJM 2004;350:876-885
Maintenance tr ial
282 patients
3 infusions of
inf l iximab
Then IFX or placebo
for 54 wks

Fistula-related abscesses in Infliximab trials
11%Present DH, NEJM 1999;340:1398
13.5%Sands B, NEJM 2004;350:876
“ The primary end-point was based on the Investigators’ physical evaluation …. A fistula was considered closed when it
was no longer draining DESPITE GENTLE FINGER COMPRESSION”


Bouguen et al. Clin Gastroenterol Hepatol 2013

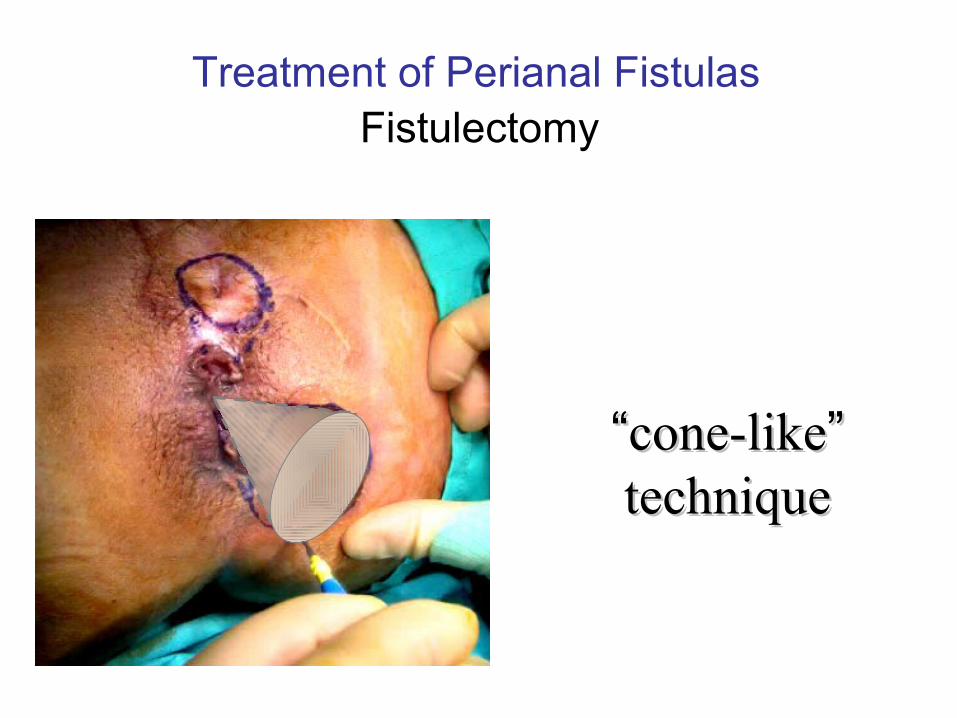
Treatment of Perianal FistulasFistulectomy
““cone-likecone-like”” techniquetechnique

Fistulectomy “cone-like”
Treatment of Perianal Fistulas

Perianal Crohn’s Disease High and Complex Fistulas
“ LOOSE“ SETON
• Simple procedure
• Draining seton is used whenever surgeon is concerned about dividing the anal sphincter muscle
• High and complex fistulas
• External tract is left open to promote drainage
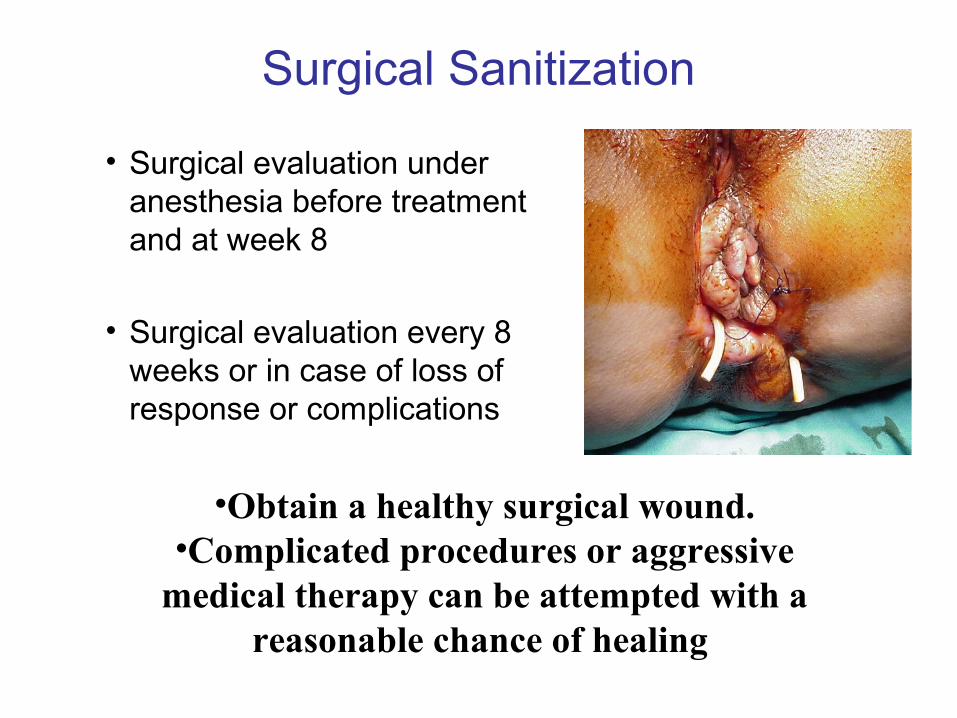
Surgical Sanitization
• Surgical evaluation under anesthesia before treatment and at week 8
• Surgical evaluation every 8 weeks or in case of loss of response or complications
•Obtain a healthy surgical wound.•Complicated procedures or aggressive
medical therapy can be attempted with a reasonable chance of healing

Complex fistulasCone-like fistulectomy of each fistula tract should be firstly performed with sparing of sphincteric structures. Seton placement should be recommended [EL 4, RG D], the timing of removal depending on subsequent therapy
Anti-TNFs should be used as the first choice of medical therapy for complex perianal Crohn’s disease [Infliximab EL1b, RG A; Adalimumab EL1b, RG B]. Combination with surgical therapy is recommended despite a lack of clinical trials [EL4, RG D]
Antibiotics and/or azathioprine/6-mercaptopurine should be used as a second line medical treatment, despite a lack of clinical trials [EL4 RG D]
Perianal Disease TherapyStatement 6D (Italian Guidelines)
Orlando A et al Dig Liver Dis 2010
Treatment of perianal Crohn’s disease with combined surgical and biological therapyAim: Evaluate the efficacy of IFX after surgical drainage and loose seton
placementMethods: - 115 patients with complex fistula or simple fistula with rectal
involvement were treated with IFX (0,2,6 and every 8 weeks until fistula closure) after EUA and seton placement.
- 74 on concomitant IMMs, 41 on monotherapy- Median follow-up was 122 wks (range 68-180 wks)- Definitions Healing : complete closure of fistulas tract (confirmed by EUA and
MRI)Improvement : reduction of drainage
Results:Complete closure was observed in in 80 pts (69,5%) and improvement
in 19 pts (16,5%);no response in 16 pts (14%); median time to close was 28 weeks (range 14-54).
Gionchetti et al. submitted

Grade 1: Unmodified / WorsenedGrade 1: Unmodified / Worsened
Grade 2: Sepsis control but persisting pus Grade 2: Sepsis control but persisting pus discharge from fistulasdischarge from fistulas
Grade 3: No pus discharge; no granulation tissueGrade 3: No pus discharge; no granulation tissue
Grade 4: Closure with scar tissue (tested with Grade 4: Closure with scar tissue (tested with probe examination)probe examination)
Perianal Score

Treatment of perianal Crohn’s disease with combined surgical and biological therapy
64%
19% 17%
0
10
20
30
40
50
60
70
80
Healed Improvement Failure
Healed
Improvement
Failure
No difference in the rate of fistula closure was observed between patients on concomitant treatment with immunosuppresants and those without
immunosuppressant (63.7% vs 64.8% respectively)

• 100 pts with complex perianal disease• Inclusion criteria:
– Active luminal CD complicated by a Perianal fistulizing CD– AZA/6MP/MTX intolerant or failure– IFX secondary failure– 64 naive, 36 IFX failure– Concomitant medications (38/100 AZA/6MP, 4/100 MTX, 22/100
steroids)– Disease location (62/100 colic or ileo-colic, 31/100 rectal)
• CDAI and IBDQ• Baseline 320 (49-560) – 120 (58-208)
• Treatment: – Surgical sanitization– Induction= ADA 160/80mg– Maintenance= 40mg eow, weekly in case of loss of response, re-
induction in case of relapse– AZA/6MP/MTX stopped at the beginning of ADA and steroid tapered of
2,5mg/wk after induction
Treatment of perianal Crohn’s disease with combined surgical and biological therapy
Rizzello et al. UEGW 2011

10
21
60
75 77
29
46
69
85 87
0
20
40
60
80
100
week 8 week 24 week 52 week 104 week 156
Remission Response
10/10029/100 21/98 45/98 59/98 69/98
Results – overall population
54/72 61/72 47/61 53/61

Results – follow up of patients with complete response
Eighteen patients relapsed during FU
7 during ADA maintenance treatment
11 during AZA maintenance treatment
0
0,2
0,4
0,6
0,8
1
0 0,5 1 1,5 2 2,5 3Years of follow up
Pat
ient
s th
at m
aint
ain
rem
issi
on
• 24/100 (24%) moved to weekly treatment for loss of response
• 18/100 (18%) were re-induced for relapse, maintained with weekly treatment. All but 2 patients regained the response
• 5 patients refractory (3 naive and 2 relapse)
• All underwent to colectomy plus temporary ileostomy and are currently on treatment

There is a place for treating perianal fistulas with local injection of Infliximab ?
RATIONALE
• Patients not suitable for I.V. Infliximab Patients not suitable for I.V. Infliximab (stenosis!)(stenosis!)
• High dose in the fistula tractHigh dose in the fistula tract
• Lower cost Lower cost →→ 20 mg/pt instead of 5-10 20 mg/pt instead of 5-10 mg /Kgmg /Kg

Perianal CrohnPerianal Crohn’s Disease’s DiseaseINFLIXIMAB FOR PERIANAL FISTULASINFLIXIMAB FOR PERIANAL FISTULAS
LOCAL INFUSION LOCAL INFUSION
METHODSMETHODS
Local Injection of Infliximab for the treatment of perianal Crohn’s Disease
G. Poggioli, M.D., S. Laureti, M.D., F. Pierangeli, M.D., F. Rizzello *, MD, F. Ugolini, M.D, P. Gionchetti *, MD, M. Campieri *, MD April, 2005
•Appropriate screening•EUA (Spinal or General anesthesia)•15-21mg / patient•6 initial infusions at 0, 4 and 8 , 12, 16, 20 weeks and eventually subsequent infusions every 4 weeks
RATIONALE•Patients not suitable for I.V. Infliximab Patients not suitable for I.V. Infliximab (stenosis!)(stenosis!)•High dose in the fistula tractHigh dose in the fistula tract•Lower cost Lower cost →→ 20 mg/pt instead of 5-10 mg /Kg 20 mg/pt instead of 5-10 mg /Kg

LOCAL INJECTION OF INFLIXIMAB
Identification of internal orifice
( mainly with injection of H2O2 from external orifice)
TECHNIQUE
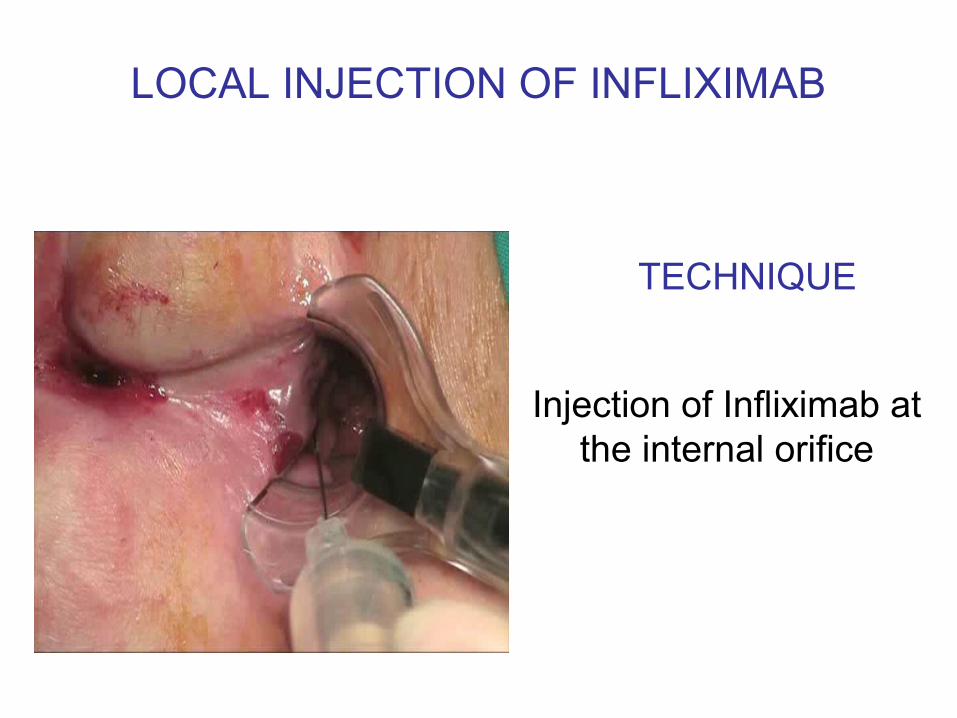
LOCAL INJECTION OF INFLIXIMAB
Injection of Infliximab at the internal orifice
TECHNIQUE

77
55
22
116565
Contraindications to I.V. infusion
Associated colo - proctitis
Not responders to I.V. infusionNot responders to I.V. infusion
Pouch-vaginal fistula
Cuffitis
Perianal Crohn’s Disease
Surgical complications of IPAA
11
Pouch-anal fistula
Local Infusion of Infliximab(81 pts)

Local Infusion of InfliximabHealed patients (“Grade 4”)
BEFORE AFTER
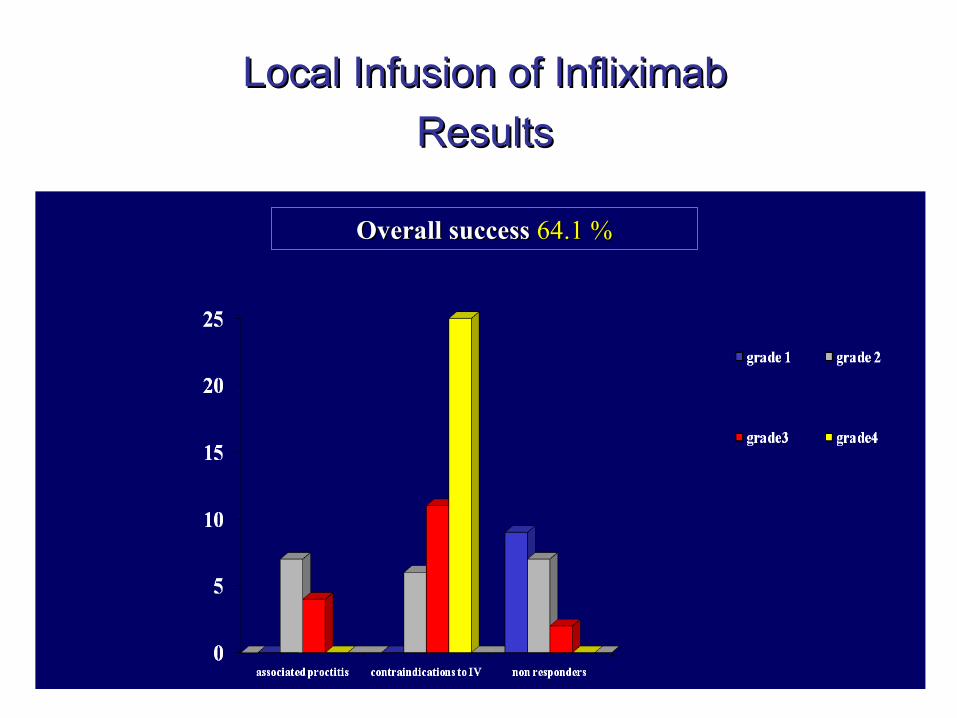
Local Infusion of InfliximabLocal Infusion of Infliximab
ResultsResults
Overall success Overall success 64.1 %64.1 %

Overall success Overall success 64.1 %64.1 %
53,2 %53,2 %
11,1 %11,1 %13,6 %13,6 %
6,1 %6,1 % 9,9 %9,9 %6,1 %6,1 %
Mean f.u. 48 monthsMean f.u. 48 months
8484%%
4%4% 6%6% 4%4% 2%2%
Local Infusion of InfliximabResults

Local Injection of adalimumab for perianal Crohn’s Disease: Better than infliximab?
Poggioli G, Laureti S, Pierangeli F, Bazzi P, Coscia M, Gentilini L, Rizzello F, Gionchetti PPoggioli G, Laureti S, Pierangeli F, Bazzi P, Coscia M, Gentilini L, Rizzello F, Gionchetti P
Inflamm Bowel Dis, 2010
34 pts treated 10 rescue therapy after local injection of Infliximab
24 naïve therapy
• Injection of 40 mg every 15 days
• Outpatient treatment
• Consistence more convenient for local injection
• Same technique as Infliximab local injection

• 15 pts healed ( score 4)15 pts healed ( score 4)
• 5 pts still in therapy pts5 pts still in therapy pts
• 8 pts failure 8 pts failure ( 80% waiting for ( 80% waiting for rescue surgical procedure )rescue surgical procedure )
• 6 pts* ruled out6 pts* ruled out
Local Injection of adalimumab for perianal Crohn’s Disease: Better than infliximab?
Local Injection of adalimumab for perianal Crohn’s Disease: Better than infliximab?
34 pts treated
42%
18% 18%22%
RESULTS

• Endorectal Advancement Flap
• Biological Glues (Bio Foam)
• Biological Prosthesis (Surgisis)
• Split Ileostomy
• Subtotal Colectomy with Ileostomy followed by Anti-TNF treatment
Treatment of Complex Perianal FistulasStrategies for Patients Unhealed after
Combined Surgical and Biological Therapy

Take Home Messages
• Complete drainage of sepsis allow better results of medical therapy
• Biologicals are the first-line therapy in complex fistulas
• Timing of seton removal is important• Repeat scanning:
may provide information on deep healing
may help decide on duration of therapy
proven