lab exercise guide for anatomy and physiology ii biology 2222l
TRANSCRIPT

Updated, 1/15/2009
1
LAB EXERCISE GUIDE FOR
ANATOMY AND PHYSIOLOGY II BIOLOGY 2222L
Author: H. Tresham
This lab guide was written to be used with Human Anatomy and Physiology Laboratory Manual, Cat
Version 9th Edition Update by E. N. Marieb
For use in Fall 08, Spring 09, Summer 09

Updated, 1/15/2009
2
Lab 1:Endocrine Glands & Body Cavities/Regions
(Marieb Exercises 1, 27)
A. Major Endocrine Glands (Exercise 27)
ASSIGNMENT:
1. Identify the endocrine glands listed using lab torsos, brain models, mid- sagittal head models and/or diagrams, Activity 1.
2. Be able to describe the functions of each gland by listing the major hormones produced, Activity 1
3. Study the assigned histology slides of the thyroid and pancreas, Activity 2.
Endocrine glands
pituitary gland-see mid sag head model adrenal gland-see torso
pineal body-see brain or mid-sag head model
pancreas-see torso
thyroid gland-see torso ovaries –see torso insert
thymus gland –diagram only testes-see torso insert
parathyroid glands-diagram only

Updated, 1/15/2009
3
B. Body Cavities (Exercise 1, Activities 4 & 5, pp.6-9)
ASSIGNMENT:
1. Identify on lab torsos/cats, the body cavities and regions listed.
Dorsal body cavity Abdominopelvic regions
cranial right and left hypochondriac region
spinal epigastric region
Ventral body cavity right and left lumbar region
thoracic umbilical region
abdominal right and left iliac region
pelvic hypogastric region
right upper quadrant RUQ
right lower quadrant RLQ
left upper quadrant LUQ
left lower quadrant LLQ

Updated, 1/15/2009
4
Lab 2: Blood (Marieb Exercise 29A)
ASSIGNMENT:
1. Identify the formed elements of the blood using prepared microscope slides/micrographs. See pp. 424, 426, 702.
2. Briefly describe the functions of each of the formed elements.
3. Determine hematocrit values using blood sample provided; be able to state human hematocrit normal values and explain their medical significance. Activity 4, pp. 430-431.
4. Determine the blood type using artificial blood samples provided. Activity 7, pp. 434-436. See also the instructions in the Lab Key binder.
5. Explain the theoretical basis of ABO blood typing, see pages 434-435.
Updated, 1/15/2009
5
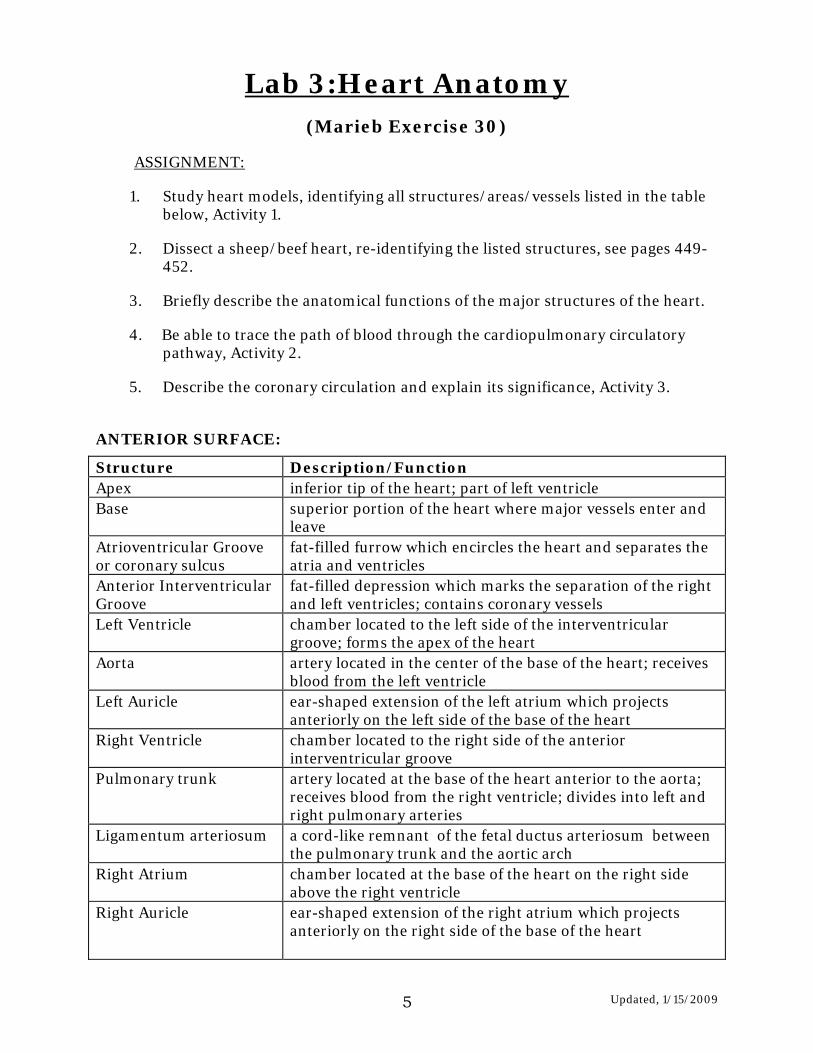
Lab 3:Heart Anatomy (Marieb Exercise 30)
ASSIGNMENT:
1. Study heart models, identifying all structures/areas/vessels listed in the table below, Activity 1.
2. Dissect a sheep/beef heart, re-identifying the listed structures, see pages 449-452.
3. Briefly describe the anatomical functions of the major structures of the heart.
4. Be able to trace the path of blood through the cardiopulmonary circulatory pathway, Activity 2.
5. Describe the coronary circulation and explain its significance, Activity 3.
ANTERIOR SURFACE:
Structure Description/Function Apex inferior tip of the heart; part of left ventricle Base superior portion of the heart where major vessels enter and
leave Atrioventricular Groove or coronary sulcus
fat-filled furrow which encircles the heart and separates the atria and ventricles
Anterior Interventricular Groove
fat-filled depression which marks the separation of the right and left ventricles; contains coronary vessels
Left Ventricle chamber located to the left side of the interventricular groove; forms the apex of the heart
Aorta artery located in the center of the base of the heart; receives blood from the left ventricle
Left Auricle ear-shaped extension of the left atrium which projects anteriorly on the left side of the base of the heart
Right Ventricle chamber located to the right side of the anterior interventricular groove
Pulmonary trunk artery located at the base of the heart anterior to the aorta; receives blood from the right ventricle; divides into left and right pulmonary arteries
Ligamentum arteriosum a cord-like remnant of the fetal ductus arteriosum between the pulmonary trunk and the aortic arch
Right Atrium chamber located at the base of the heart on the right side above the right ventricle
Right Auricle ear-shaped extension of the right atrium which projects anteriorly on the right side of the base of the heart

Updated, 1/15/2009
6
POSTERIOR SURFACE:
Structure Description Left Atrium located at the base of the heart on the left; receives blood
from pulmonary circuit Pulmonary veins four thin walled vessels that drain into the left atrium from
the lung Right Atrium located at the base of the heart on the right; receives blood
from the systemic circulation Superior Vena Cava thin walled vessel draining into the right atrium from above Inferior Vena Cava thin walled vessel draining into the rt. atrium from below Posterior Interventricular Groove
fat-filled depression which marks the separation of right and left ventricles; contains coronary vessels
Left ventricle located inferior to the left atrium and to the left of the posterior interventricular groove; pumps blood to systemic circuit
Right ventricle located inferior to the right atrium and to the right of the posterior interventricular groove; pumps blood into pulmonary circuit
CORONARY BLOOD VESSELS:
Blood Vessel Description
Left Coronary Artery originates from the aorta
circumflex branch supplies left atrium and posterior heart
anterior interventricular supplies interventricular septum & anterior wall of ventricle
Right Coronary Artery originates from the aorta
marginal artery supplies the lateral surface of the right side of the heart
posterior interventricular supplies posterior walls of ventricles
Coronary Sinus
drains venous blood from the heart into the right atrium; located at inferior border of the right atrium, left of the inferior vena cava
Middle Cardiac Vein
ascends from the apex within the posterior interventricular groove; empties into the coronary sinus
Great Cardiac Vein found in anterior interventricular groove; empties into the coronary sinus on the posterior side of the heart

Updated, 1/15/2009
7
INTERNAL ANATOMY OF THE HEART:
Structure Function
Right Atrium receives venous drainage from systemic circulation
opening of coronary sinus returns venous coronary circulation to r. atrium
pectinate muscles muscle ridges more prominent in right atria wall
fossa ovalis remnant of fetal foramen ovale… connection of right to left atria to bypass fetal lungs
Right Ventricle pumps blood to lungs
tricuspid valve prevents backflow from rt. ventricle into rt. atrium
chordae tendineae attach valve cusps to papillary muscles
papillary muscles contraction prevents valve eversion
pulmonary valve prevents backflow from pulmonary trunk into rt. ventricle
interventricular septum divides left and right ventricles
Left Ventricle pumps blood to systemic circulation
aortic semilunar valve prevents backflow from aorta into left ventricle
bicuspid valve prevents backflow from left ventricle into left atrium
chordae tendineae attach valve cusps to papillary muscles
papillary muscles contraction prevents valve eversion
Left Atrium receives venous drainage from pulmonary circulation
Pericardium fibroserous sac enclosing the heart
Epicardium epithelial membrane covering the heart surface
Myocardium muscular layer of the heart wall
Endocardium epithelial membrane lining the heart chambers

Updated, 1/15/2009
8
Lab 4: Blood Vessels (Marieb Exercise 32 and Cat Dissection # 4)
ASSIGNMENT:
1. Identify the arteries listed using: torsos, “circulatory man” plaques, arm/ leg models and diagrams; indicate the region supplied by each vessel, Activity 2, 4, 6.
2. Identify the veins listed using: torsos, “circulatory man” plaques, arm/ leg
models and diagrams; indicate the region drained by each vessel, Activity 3, 4, 5, 6.
3. Complete the “Trace a Drop of Blood Exercise” on page 11 of this lab guide. 4. Open the body cavities on the cat. 5. Dissect and identify the listed blood vessels on the cat. 6. Compare and contrast the cat and human vasculature. 7. Study assigned histology slide of artery/vein; identify the three tunics, Activity
1. See slide photos on page 470 and page 696, plate 21
Artery Region Supplied
Ascending Aorta
Right Coronary Artery Heart
Left Coronary Artery Heart
Arch of Aorta
Brachiocephalic Trunk
Rt. side of head, neck, and upper arm; thyroid and thymus
Right Common Carotid right side of the head and neck ; brain
Internal Common Carotid Ant. and middle arteries of cerebrum
Right Subclavian neck, thorax, arm and shoulder; spinal cord; brain
Vertebral (Paired arteries which form) Basilar Artery
Pons, cerebellum, inner ear posterior cerebral arteries and Circle of Willis
Circle of Willis Arterial anastomosis at base of brain for alternate brain supply
Axillary
Brachial shoulder, arm, forearm, and hand

Updated, 1/15/2009
9
Radial forearm and hand, radius, parts of hand
Ulnar supplies: hand, wrist, and forearm
Aortic Arch
Left Subclavian neck, thorax, arm and shoulder; spinal cord; brain
Left Common Carotid left side of the head and neck ; brain
Thoracic Aorta
Intercostals intercostal muscles; chest; part of lungs
Abdominal Aorta
Inferior Phrenics diaphragm and adrenal glands
Artery Region Supplied
Celiac trunk
Common Hepatic liver; stomach; pancreas; duodenum;
Left Gastric stomach; part of esophagus
Splenic spleen; pancreas
Superior Mesenteric small intestine; cecum; parts of the colon; pancreas
Suprarenals adrenal glands
Renals kidneys; adrenal glands; ureters
Gonadals Ureters, gonads and associated structures
Lumbars spinal cord; skin and lumbar region of the back
Inferior Mesenteric parts of colon and rectum
Common Iliac pelvis; genitals, and gluteal regions
Internal Iliac pelvis, external genitals, medial thigh
External Iliac abdominal wall, external genitals, psoas major
Femoral thigh, external genitals, abdominal wall, and groin
Deep Femoral hip joint, thigh muscles, and gluteal muscles
Lateral Circumflex hip joint and thigh muscles
Popliteal
muscles in the region of the knee, femur, patella, and tibia
Anterior Tibial muscles of the knee, leg, ankle, and foot
Posterior Tibial muscles and bones of the leg, ankle, and foot
Fibular(Peroneal ) structures on the medial side of the fibula and calcaneus
Vein Region Drained
Superior Vena Cava right and left brachiocephalic veins; azygos vein
Azygos right side of thorax
Right Intercostals right intercostal spaces; skin and muscles of the back
Hemiazygos lumbar veins; intercostal veins
Left Intercostals left intercostal spaces; skin and muscles of the back
Ascending Lumbar common iliacs; lumbar veins

Updated, 1/15/2009
10
Brachiocephalics subclavian and internal jugular veins
Internal Jugular brain, face, and neck
Subclavian axillary vein and external jugular vein
External Jugular deep parts of the face; exterior of the cranium;
Axillary cephalic, brachial, and basilic veins
Brachial upper arm; radial and ulnar veins
Radial parts of hand
Ulnar Basilic Median Cubital
parts of hand
Vein Region Drained
Inferior Vena Cava
Inferior phrenics Diaphragm
Hepatic Liver
Suprarenals adrenal glands
Right renal Right kidney
Right gonadal Right ovary or testis
Left renal Left kidney; left gonadal
Left gonadal Left ovary or testis
Lumbars skin and muscles of the loin; abdominal wall; vertebrae
Common Iliacs internal and external iliac veins
Internal Iliac pelvic region; gluteal muscles; medial thigh
External Iliac lower extremities; lower abdominal wall
Femoral deep structures of the thigh
Popliteal anterior and posterior tibial veins; small saphenous vein
Anterior Tibial foot; muscles and bones of the anterior leg
Posterior Tibial muscles and bones of the posterior leg
Fibular(Peroneal) leg muscles; calcaneus (heel)
Great Saphenous (sp.) foot; superficial tissues of the lower extremities
Small Saphenous (sp.) foot and posterior portion of the leg
Hepatic Portal superior mesenteric, splenic and gastric veins
Superior, and Inferior Mesenteric s
small intestine; colon, appendix, stomach; pancreas
Splenic spleen; parts of colon; parts of stomach
Gastric stomach

Updated, 1/15/2009
11
Assigned Vessels On The Dissected Cat: see Cat Dissection # 4, pages 731-739: Arteries: Veins: 1. Pulmonary trunk 2. Aortic Arch 1. Superior vena cava 3. Descending aorta: Thor., Abd., Pelvic 2. Inferior vena cava 4. Common Carotid 3. External jugular 5. Subclavians 4. Subclavian 6. Brachiocephalic 5. Brachiocephalic 7. Axillary 6. Renal
8. Brachial 7. Iliacs: common, ext., int. 9. Celiac trunk 8. Femoral 10. Mesenterics: sup., inf. 9. Greater saphenous 11. Renal 12. Iliacs: ext., int. 13. Femoral Trace a Drop of Blood Exercise: Trace a drop of blood from: a. the left internal iliac vein to the right internal iliac artery b. the right renal vein to the left renal artery c. the superior mesenteric artery to the right atrium d. the right brachial vein to the left internal carotid artery

Updated, 1/15/2009
12
Lab 5: Cardiovascular Physiology: Study of Pulse, Heart Sounds, Blood Pressure
(Marieb Exercise 33 A) ASSIGNMENT:
1. Auscultate the heart sounds using a stethoscope. Explain the heart activities which produce the “lub-dub” sounds, Ex. 33A, Activity 1.
2. Locate the nine human pulse points on the body, Ex. 33A, Activity 2.
3. Determine and record the pulse by palpating the carotid, brachial and radial arteries, Ex. 33a, Activity 2.
4. Determine the apical pulse with a stethoscope. Calculate, record and define pulse deficit and explain its significance, Ex. 33A, Activity 4.
5. Define systolic and diastolic blood pressures. Determine and record blood pressure using a sphygmomanometer, Ex. 33A, Activity 5.
6. Calculate pulse pressure and mean arterial pressure (MAP) and explain their significance, Ex. 33A, Activity 5.
7. Demonstrate and explain the effects of posture and exercise on blood pressure, Ex. 33A, Activity 7.
8. Optional: Utilize the Doppler ultrasound equipment to hear the radial pulse.
See instructions in Lab Model Key Binder

Updated, 1/15/2009
13
Lab 6: Respiratory Anatomy (Marieb Exercise 36 and Cat Dissection # 6)
ASSIGNMENT:
1. Identify the structures listed using torso models, larynx models, and mid-sagittal head models, Activity 1.
2. State the function of the major structures listed, Activity 1.
3. Study the prepared slide of lung tissue, Activity 3.
4. Identify the listed respiratory structures/organs in a dissected cat. See Cat Dissection 6, pp. 743-745.
Respiratory Anatomy Structures
Structure Function
Nose/Nostrils external nares internal nares superior, middle inferior meatus superior, middle inferior conchae
Air intake and passage; warms, moistens, and filters inhaled air
Paranasal sinuses ethmoid sphenoid frontal maxillary
Produce mucus; provide sound resonance; lighten the skull
Pharynx nasopharynx oropharynx laryngopharynx pharyngeal tonsils palantine tonsils
Serves as passageway for air into the larynx and for food into the esophagus. Actually belong to lymphatic-immune system; aid in defending against infections Actually belong to lymphatic-immune system; aid in defending against infections
hard palate soft palate Used in mastication and vocalization

Updated, 1/15/2009
14
Structure Function
Larynx thyroid cartilage cricoid cartilage
passageway for air from laryngopharynx to trachea; produces sound;
epiglottis covers the glottis (opening of the larynx) during swallowing
glottis opening at top of larynx where air enters respiratory passage; speech sounds
true vocal cords speech
false vocal cords
Trachea air passageway from larynx to primary bronchus; ciliated columnar epithelium lining and vessels in underlying connective tissue, cleanses, warms and moistens the air
Lungs contain secondary and tertiary bronchi, bronchioles, alveolar ducts, alveoli and pulmonary vessels, passageways for air and site of gas exchange
left superior lobe
left inferior lobe
right superior lobe
right middle lobe
right inferior lobe
Bronchi
Primary/main
Secondary/lobar
Tertiary/segmental
Passageway for air; cleansing, warming, moistening of air, lined with ciliated columnar epithelium; smooth muscle in wall allows them to constrict and dilate
Bronchioles
Terminal
Respiratory
Microscopic air passageways: Same as above
Alveolar ducts Branches off respiratory bronchioles, transport air
Alveoli Functional units of respiration; site of gaseous exchange; walls contain capillaries
parietal pleura visceral pleura
Compartmentalize, protect, and lubricate the lungs
mediastinal cavity Area of thoracic cavity containing heart and lungs
Diaphragm /External Intercostal muscles
contraction aids in inspiration by increasing volume of thoracic cavity/lungs

Updated, 1/15/2009
15
Assigned Structures On Dissected Cat: see Cat Dissection # 6, pages 743-745.
1. Epiglottis 2. Thyroid cartilage of larynx 3. Trachea with cartilage rings 4. Primary Bronchus, right /left 5. Secondary bronchus 6. Lobes of lung 7. Diaphragm 8. Intercostal muscles

Updated, 1/15/2009
16
Lab 7:ECG and Respiratory Physiology
(Marieb Exercise 31, 37A, and Appendix A, B of the Lab Guide)
A. CV Physiology: ECG (Exercise 31)
Note: The exercise in #1 will be completed via the iWORX program on the lab laptop computers
ASSIGNMENT:
1. Complete iWORX, Exp. 18, Ex. 1: ECG in Resting Volunteer; see Appendix A. Identify the characteristic waves on an ECG and relate them to the electrical events in the heart; be able to determine heart rate from ECG tracing.
2. Completion of Ex.3: ECG and Heart Sounds is optional; see Appendix A.
B. Respiratory Physiology (Exercise 37A)
ASSIGNMENT:
1. Measure and record expired lung volumes using the iWORX Spirometry Flowhead. This exercise will be performed utilizing the lab’s laptops computers. See Appendix B: Exp 29, Ex.1 and 3 for instructions.
2. Define and list normal values of all lung volumes and capacities. See Activity 3.
3. Define, calculate and record MRV. See Activity 3.
4. Ascultate the respiratory sounds with a stethoscope, Activity 2.
5. Demonstrate Boyle’s law with model lung via completion of Activity 1 and review sheet page 569, # 1.

Updated, 1/15/2009
17
Lab 8: Anatomy of the Digestive System (Marieb Exercise 38, Cat Dissection # 7)
ASSIGNMENT:
1. Identify the structures listed using models and diagrams; state the functions for each structure, Activity 1.
2. Locate and identify on a dissected cat the assigned organs/structures. State the function of each organ/structure. Dissection #7, pp.747-752.
3. Study the assigned histology slides of digestive organs: stomach, duodenum, colon, liver, pancreas, Activities 2, 3, 4, 8. Study also the histology models of the duodenum and liver.
4. Study the purple plastic plaque of the teeth and a skull; identify the major types and numbers of teeth in the adult. Be able to state and explain the adult dental formula. State the functions of each tooth type Activity 5, see pages 586-587.
5. On purple plastic tooth model identify the parts of a tooth listed in chart on page 18.

Updated, 1/15/2009
18
Anatomy of Digestive System
mouth large intestine
labia haustra
vestibule caecum/ileocaecal junction
oral cavity appendix
tongue ascending colon
hard palate transverse colon
soft palate descending colon
teeth (types and number, parts) sigmoid colon
See table on page 19
uvula rectum
sublingual salivary gland anus
submandibular salivary gland pancreas
parotid salivary gland liver
oropharynx/laryngopharynx right liver lobe
esophagus left liver lobe
stomach quadrate lobe
lesser curvature of stomach caudate lobe
greater curvature of stomach hepatic bile duct
rugae gall bladder
cardiac region of stomach cystic bile duct
fundus of stomach common bile duct
body of stomach parietal peritoneum
pyloris of stomach visceral peritoneum
pyloric sphincter mesentery
cardiac/esophageal sphincter
small intestine greater omentum
duodenum lesser omentum
jejunum mesocolon: transverse and sigmoid
ileum

Updated, 1/15/2009
19
Tooth Anatomy and Classifications
crown Incisors ; lateral , central neck Canine root Premolars/bicuspids
enamel Molars dentin
pulp cavity/pulp Adult formula: 2I, 1C, 2PM, 3M/2I, 1C, 2PM, 3M x2 (32 teeth)
gingivae cementum root canal
periodontal ligament apical foramen
Assigned Structures On Dissected Cat: see Cat Dissection #7, pp. 747-752:
1. Esophagus 2. Stomach-cardiac, fundus, body, pyloric areas 3. Small intestine: duodenum, jejunum, ileum 4. Caecum/ileocaecal junction 5. Large intestine: ascending., transverse, descending. 6. Rectum 7. Liver lobes 8. Pancreas 9. Gallbladder 10. Greater omentum 11. Lesser omentum 12. Mesocolon 13. Mesentery 14. Parietal peritoneum 15. Visceral peritoneum

Updated, 1/15/2009
20
Lab 9: Digestive Physiology (Marieb Exercise 39A, required/assigned and 39B, optional)
ASSIGNMENT:
1. Complete the experiment “Assessing Starch Digestion by Salivary Amylase”, Activity 1. Collect your own saliva as your source of salivary amylase!
2. Complete the experiment “Demonstrating the Emulsification Action of Bile and Assessing Fat Digestion by Lipase”, Activity 3.
3. Be able to describe/discuss and explain: the procedures used in these experiments (methods and materials), the theory for each experiment, and the results.
4. Complete and explain Activity 5, “Observing Movements and Sounds of Digestion”.

Updated, 1/15/2009
21
Lab 10:Urinary Anatomy and Urinalysis (Marieb Exercise 40 and 41A)
A. Urinalysis (Exercise 41A)
ASSIGNMENT:
1. Complete Activity 1, “Analyzing Urine Samples” on three artificial urine samples provided. In the section on Determination of Inorganic Constituents, omit sulfates, phosphates, chlorides; nitrites are included on the lab dipstick. In the section on Determination of Organic Constituents omit urea and icotest; they are not on our lab dipstick. Note also that albumin equals protein on our dipstick! PH is on our dipstick; you do not have to use separate PH paper.
2. Know the theory on urinalysis on pp. 621-623; use this info to interpret/explain your results from urine samples tested.
B. Anatomy of the Urinary System (Exercise 40, Cat Dissection # 8) ASSIGNMENT:
1. Identify the structures below using kidney, nephron and torso models. Use diagram for bladder anatomy. Activity 1 & 2.
2. State the function of the major structures listed. Activity 1 & 2.
3. Dissect and examine a preserved sheep/beef kidney, re-identifying assigned structures/functions. See dissection pp. 612-613.
4. Identify on a dissected cat the urinary system organs and describe the general function(s) of each. See Dissection # 8, pp.753-756.
5. Study assigned kidney histology slide, Activity 2, page 615.
6. Study assigned transitional epithelium slide of ureter/bladder, see plate 43, page 700 and page 73 of Ex. 6A, tissues lab.

Updated, 1/15/2009
22
URINARY SYSTEM
Parietal peritoneum Ureters hilum Urinary bladder cortex trigone medulla internal urethral sphincter renal pyramids external urethral sphincter papilla Urethra renal columns Urethral orifice renal pelvis/sinus Kidney Vessels Segemental artery major/minor calyces Lobar artery nephron Interlobar artery/vein afferent arteriole Arcuate artery/vein efferent arteriole CorticalRadiate/Interlobular artery/vein glomeruli/Bowman’s capsule podocytes portions of nephron tubules distal convolutions loop of Henle, ascending and descending
proximal convolutions collecting ducts
Assigned Structures On The Dissected Cat: see Cat Dissection # 8, pp.753-756 1. Kidneys, observe retro-peritoneal position, and location of right vs. left. 2. Ureters 3. Urinary bladder 4. Urethra: male/female

Updated, 1/15/2009
23
Lab 11: Reproductive Anatomy& Physiology
(Marieb Exercise 42 and 43; Optional Cat Dissection # 9)
ASSIGNMENT:
A. REPRODUCTIVE ANATOMY: Marieb exercise 42
1. Identify the structures below using reproductive models and torso reproductive male/female inserts. Ex. 42, Activities 1 and 5.
2. State the function of the major structures listed below. Ex. 42, Activities 1 and 5.
3. Study assigned histology slides: wall of uterus, Ex. 42, Activity 6.
4. Study female mammary gland models, identifying assigned structures; describe functions of these structures in lactation. See diagram in binder of lab model keys and see also page 1089 of textbook.
5. Optional: Identify and state the function of the major male and female reproductive structures on a dissected cat. Note: female cat has bicornate uterus.
MALE REPRODUCTIVE ANATOMY
Testes Seminal Vesicle Scrotum Prostate gland Epididymis Ejaculatory duct Vas deferens Prostatic urethra Spermatic cord Membranous urethra Vas deferens Bulbourethral gland/Cowper’s glands Testicular artery Penis Testicular vein Penile Urethra Cremaster muscle Corpora cavernosa Inguinal Ring Corpus spongiosum Inguinal Canal Glans Ampulla of Vas deferens Prepuce

Updated, 1/15/2009
24
FEMALE REPRODUCTIVE ANATOMY
Ovaries Vulva
Suspensory ligament Labia majora
Uterine tubes (Fallopian) Labia minora
Infundibulum Vestibule
Fimbriae Vestibular.glands (Bartholin's)
Uterus Clitoris
Endometrium Urethral orifice
Myometrium Mons pubis
Ovarian ligament Mammary Gland
Broad ligament Areola
Round ligament Nipple
Cervix Alveoli
Vagina Lactiferous ducts
Vaginal orifice Lactiferous sinuses Optional Assigned Structures On The Dissected Cat: see Cat Dissection #9, pp.757-761.
Male: Female: 1. Scrotal sac 1. Ovaries 2. Testes 2. Uterine tube 3. Spermatic cord 3. Bicornate uterus: Uterine horns 4. Prostate gland 4. Body of uterus 5. Urethra 5. Vagina 6. Bulbourethral glands 7. Penis

Updated, 1/15/2009
25
B. REPRODUCTIVE PHYSIOLOGY: Marieb exercise 43
1. Learn and describe the stages and events of meiosis using meiosis model/plaque and diagrams. Ex. 43, Activity 1.
2 Compare and contrast meiosis in male testes and female ovaries via study of assigned histology testes and ovary slides and the meiosis model. Activities 2, 3, 4, and 5.
3. Identify and describe the main ovarian and uterine phases of the human menstrual cycle on purple menstrual plaque. See pages 647-648.
Meiosis
oogonium (diploid) spermatogonium (diploid)
primordial follicle (diploid) primary spermatocyte (diploid)
primary oocyte (diploid) secondary spermatocyte (haploid)
primary follicle (diploid) spermtid (haploid)
spermatozoa (haploid)
growing follicle (diploid)
vesicular Graafian follicle (haploid) Meiosis I
first polar body (haploid) Meiosis II
secondary oocyte (haploid) spermiogenesis
second polar body (haploid)
ovum (haploid)
Menstrual Cycle Phases
Ovary Uterine Endometrium
Follicular/Preovulatory phase Proliferative phase
Ovulation Secretory phase
Luteal/postovulatory phase Menstrual phase

Updated, 1/15/2009
26
Lab 12:Embryonic Development (Marieb Exercise 44)
ASSIGNMENT:
1. Describe the processes of fertilization, cleavage (morula), blastulation and gastrulation. Study pages 653-656.
2. Name the three germ layers and describe their significance by listing organs which develop from each layer. Read page 655.
3. Identify (on development boards and purple plaques and stand models) the structures listed below. Consult diagrams on pages 655-656. Describe the function/significance of each structure.
EMBRYONIC DEVELOPMENT
Fertilization producing
Diploid zygote
Cleavage stages
Morula
Blastula/Blastocyst
Inner cell mass: ectoderm and endoderm
Trophoblast: ectoderm
Gastrula: ectoderm, mesoderm, endoderm
Chorion
Yolk Sac
Allantois
Amnion

Updated, 1/15/2009
27
Appendix A
iWORX CV PHYSIOLOGY LAB Exp. 18: The ECG Background: page 27
ECG in a Resting Volunteer, pp. 28-31. Data table : page 38
The Electrocardiogram and Heart Sounds (Experiment 18-iWorx)
Background: The cardiac cycle involves a sequential contraction of the atria and the ventricles. The combined electrical activity of the different myocardial cells produces electrical currents that spread through the body fluids. These currents are large and can be detected by recording electrodes placed on the skin. In this lab you will attach three electrodes to a student volunteer. These electrodes will be connected to the iWorx unit and the signal will be displayed on the computer screen in a strip chart format. The regular pattern of “peaks” produced by each heart beat cycle is called the electrocardiogram or ECG.
The action potentials recorded from atrial and ventricular fibers are different from those of nerves and skeletal muscle. The cardiac action potential is composed of three phases: a rapid depolarization, a plateau depolarization (which is pronounced in ventricular fibers), and a repolarization back to resting membrane potential. The components of the ECG can be correlated with the electrical activity of the atrial and ventricular fibers such that:

Updated, 1/15/2009
28
1. Atrial depolarization produces the P wave; atrial contraction or systole will follow.
2. Atrial repolarization (producing atrial diastole/relaxation) and ventricular depolarization produce the QRS complex; ventricular systole or contraction will follow.
3. Ventricular repolarization produces the T wave; this results in ventricular diastole/relaxation.
In this lab you will record the ECG from a volunteer. During the cardiac cycle the
heart makes its’ characteristic “lub-dup” heart sounds. The “lub” sound occurs during the early phase of ventricular contraction and is produced by closing of the atrioventricular valves, which prevents blood flow into the atria. When the ventricles relax, the blood pressure drops below that in the artery and the semilunar valves close, producing the “dub” sound. Setup & Experiment-Resting ECG:
1. Turn on the computer if it is not already on, all of the iWorx connections are already made from the unit to the electrodes and from the unit to the computer.
2. Have the first volunteer in the group (don’t worry you will all get a chance)
remove all jewelry from their wrists and ankles and then use an alcohol pad to scrub both wrists and the left ankle.
3. Remove a disposable electrode from the plastic strip and apply the electrode to
the scrubbed area on one wrist (try to avoid hair if possible). Repeat for the other wrist and the left ankle.
4. Attach the three color-coded lead ends onto the disposable electrodes, so that
(Lead II):
a. The red ‘+1’ lead is attached to the left leg. b. The black ‘-1’ lead is connected to the right wrist c. The green ‘C’ lead is connected to the left wrist
5. The volunteer needs to sit quietly for the duration of this experiment; even small movements of muscle will produce electrical ‘noise’ in the system obscuring the ECG in a dramatic fashion. So, make sure the volunteer is comfortable.

Updated, 1/15/2009
29
6. Double-click the ‘Labscribe’ icon on the desktop.
7. When the program opens, click on the Settings menu and select
APheartrespiration. (if APheartrespiration is not visible in the Settings menu then select Load Group and load the APiworx group, then the APheartrespiration file will be visible in the Settings menu)
8. Labscribe will reconfigure to the correct settings showing 3 channels
9. Click Start in the upper right corner of the screen, and after a few seconds click
Autoscale found just after the ECG channel title (If the ECG appears to be upside down at this point, right click on the ECG tracing and select Invert; it should now be right-side up).
10. If the tracing of the ECG is too clumped together or really spread out, press Stop
and use the Half display time or Double display time buttons (they are picture buttons found at the top 4th & 3rd from the right; Half display time looks like a single mountain and Double display time looks like two mountains) to adjust the tracing to the desired level. Then press Start again.
11. After you have a good tracing, type “XYZ’s resting ECG” (where XYZ is the
volunteer’s name) in the comment line to the right of the Mark button. Press the Enter key on the keyboard to attach the comment to the data.

Updated, 1/15/2009
30
12. Click Stop to halt recording. Your data should look something like this:
13. Click the 2-Cursor icon (a picture button 2nd from the right at the top with little
red waves and 2 blue vertical lines) and 2 blue vertical lines will appear over the recording window.
14. Drag the lines left and right so that 3-4 complete heart beat cycles are located
between the two blue lines (see picture above).
15. Click the Analysis icon (a picture button at the top located immediately to the right of the dark green picture with a wave on it) to open the Analysis window.
16. On the left side of the screen in the Display Channel list, click (select) the ECG
channel only so it is the only data displayed.
17. Drag the two blue cursor lines around the analysis window to measure:
a. The amplitude (V2-V1 from Q to R) of three QRS complexes. b. The amplitude (V2-V1 from base to peak) of three P waves c. The amplitude (V2-V1 from base to peak) of three T waves d. The time interval (T2-T1) between three adjacent R waves; you should
have 2 values. Remember the Display time can be halved (as in the Main window) to expand the horizontal axis and obtain a very accurate time measurement. The trace can be scrolled horizontally using the arrows in the lower margin of the Analysis window. Record all these measured values on the data table provided on page 38.

Updated, 1/15/2009
31
18. Measure and Calculate the following values and record them on the data table on
page 38:
a. The average amplitude of the P wave, the QRS complex, and the T wave. b. The average time interval (or beat period) between adjacent R waves, in
seconds. c. The heart rate, in beats per minute, is calculated from the equation:
Heart Rate (BPM) = 60/average beat period
Questions:
1. Is the amplitude of each wave (P, QRS, T) always the same in different cardiac cycles?
2. Which wave has the largest amplitude? 3. What is the average resting heart rate of the subject?

Updated, 1/15/2009
32
Appendix B
iWORX Respiratory Physiology Lab
Exp. 29: Breathing Parameters at Rest and After Exercise
Background: page 32 Ex. 1: Breathing in a Resting Volunteer, pages 35-37 Data Table: Page 38
Breathing Parameters at Rest (Experiment 29-iWorx) Background: The amount of air that moves in or out of the lungs during any one breathing cycle is called the tidal volume. After normal inspiration, it is possible to breathe in additional air—this is called the inspiratory reserve volume. Similarly, after a normal expiration, it is possible to exhale additional air from the lungs—this is the expiratory reserve volume. Even if the expiratory reserve volume is fully expelled from the lungs, there is still a volume of air in the lungs, called the residual volume, that cannot be exhaled. The residual volume has very low oxygen and high carbon dioxide concentrations. Upon inhalation, fresh air mixes with stale air from the residual volume to create air in the alveoli that still has gas concentrations that facilitate the diffusion of oxygen into and carbon dioxide out of the capillaries. The respiration center in the medulla insures that gaseous exchange at the lung matches the requirements of the body. During times of increased demand, the tidal volume can be increased, using some of the reserve lung volumes to bring more fresh air into the body. In addition, the rate of breathing and the rate of air movement in and out of the lungs can be changed. In this lab you will measure these parameters in a volunteer at rest.

Updated, 1/15/2009
33
Setup & Experiment-Breathing at Rest:
1. Click the Main icon to return to the main recording window from the Analysis screen.
2. On the right side of the tracing for the Volume channel just past the Value=…
there are 2 red arrows that are almost overlapping (there is another set of them above this for the heart stuff, don’t worry about those). Use the cursor to drag those 2 red arrows away from each other until a hidden channel labeled Flow appears.
3. Right click on the word Flow and find the Spirometry menu. Under the
spirometry menu is a Calibrate function (do not hit the calibrate to 1L function); click on Calibrate and a new window pops up.
4. There is a number written on the piece of tape holding your spirometer (the little
black box attached to channel 4) to the desk. Put this number in the box provided and click OK (you may want to check this number after you hit OK to ensure that it is correct).
5. You can now hide that channel again by bringing the red arrows back together.
You will not be looking at flow for this exercise.
6. A few points before beginning this exercise:
a. The spirometer will monitor breathing from a volunteer. It is important that the volunteer is healthy and has no history of respiratory or cardiovascular problems
b. The outlets on the flow head should always be in the upright position to avoid problems with condensation developing in the airflow tubes.

Updated, 1/15/2009
34
c. Turbulence in the flow head will produce a noisy signal. To reduce turbulence, the subject should place their lips around the outside of the opening of the mouthpiece.
d. If you can’t prevent air passing through your nose without help, there is a noseclip provided. Air that passes through the nose is not included in the volume measurements and causes errors in these values.
e. The settings file displays airflow of the spirometer on channel 4, and the Volume on channel 5. The settings file activates an algorithm designed specifically to convert the airflow data of iWorx SP-304 spirometer to volume data
f. Right-click on the Volume channel. Select Spirometry and be sure that the Volume option is checked. If it is not checked, select it now.
g. Allow the SP-304 to warm up for 10 minutes before recording for the first time (if you did the cardiovascular exercises first, this should not be a problem). Do not hold the spirometer amplifier in your hand; the heat of yoru hand will alter the volumes recorded.
h. Determine which opening of the flowhead should be used to make the deflection on the airflow channel go up as the subject inhales. Open the Window menu, and select Preview. A window displaying the signal coming into Channel 1 of the iWorx unit appears. Click on the arrows above the display to change the channel being viewed int eh diplay to the Flow channel. Watch the display as the subject inhales. To increase the size of the trace, click Autoscale. The trace on the display should go up as the subject inhales. If the trace goes down during inhalation, breathe through the other end of the flowhead (the white thing).
7. The subject should sit quietly and become accustomed to breathing through the
spirometer. They should be breathing normally before any recordings are made. Remember to hold the flowhead so that the outlets are on top.
8. Have the subject remove the flowhead from their mouth. They should hold it at
the same level as their mouth, but in a position that prevents their breath or any other airflow from moving through the flow head. (Labscribe will zero the Volume channel during the first 5 seconds of recording after you click Start. NO AIR should be moving through the flow head during this time. If you forget this step the resulting trace will look like a runaway wave that perpetually rises or falls).
9. Click Start. Type “Resting” in the comment line to the right of the Mark button.
After waiting five seconds for the Volume channel to zero, have the subject place the flowhead in their mouth and begin breathing. Press the Enter key on the

Updated, 1/15/2009
35
keyboard. Click Autoscale on the Volume channel. Notice the slowly moving wave on the Volume channel. Record 5 breaths, which normally takes about 30
seconds. During this time, the Volume channel may automatically reset itself to zero; which it will do every 30 seconds after the recording begins. (Remember you can adjust the Display Time to increase or decrease the number of breaths on the screen).
10. Type “Maximum” on the comment line. Press the Enter key on the keyboard as
the subject inhales as much as possible. As quickly as possible after reaching their maximum inhalation volume, the subject should exhale as quickly and as completely as possible.
11. The volunteer should return to normal breathing through the spirometer.
12. Click Stop to halt recording.
13. Scroll the data until the beginning of the first breathing cycle appears on the
Main window. Adjust the Display Time so that at least 2 complete breathing cycles appear on the window (if you haven’t already).
14. Click the 2-Cursor icon, so that two blue vertical lines appear over the recording
window.
15. Drag the blue cursor lines left and right so that the two complete breathing cycles are located between the two blue lines.
16. Click the Analysis icon to open the Analysis window.
17. In the Display Channel list click on Volume so that it is the only channel
displayed in the data window. On the left side of the Analysis window in the Table Functions list hold down the control key and select Title, V2-V1, and T2-T1. They should already be selected, but if they are not you must select them in this step.

Updated, 1/15/2009
36
18. Click and drag the cursors over each of the five breathing cycles to measure the following parameters:
a. Tidal Volume (TV): the amplitude of the breathing cycle. Place the one
cursor in the trough prior to the inhalation, and the second cursor to the peak of the cycle. The value, V2-V1, is the Tidal Volume
b. Period: the duration of each breathing cycle. The duration is easiest to measure between peaks or troughs on the Volume record. The value, T2-T1 is the Period.
19. Average the data for each parameter. 20. Scroll the data in the Analysis window until the “Maximum” breathing cycle
appears in the window. Adjust the Display Time so the complete cycle appears on the window, from the normal tidal volume (or baseline) before the maximum inhalation to the flat line after the subject has completely expelled all the air from their lungs. Your data may look something like this:

Updated, 1/15/2009
37
21. Click the 2-Cursor icon, so that two blue vertical lines appear over the analysis
window.
22. Drag the blue cursor lines left and right to measure; Tidal Volume (TV), Inspiratory Reserve (IR), Expiratory Reserve (ER), and the Vital Capacity (VC).
Record three measurements for each lung volume. Record these on the data sheet provided on page 38. Average the three values and record this average on the data table.
a. Use the mean duration of the breathing cycles to measure breathing rate: Breathing Rate (breaths/minute)=60/breathing period
b. Multiply the mean tidal volume by the breathing rate to calculate the volume of air passing in and out of the resting subject’s lungs each minute=MRV. Record this result on the data table on page 38.

Updated, 1/15/2009
38
Data Tables: ECG and Lung Volumes
ECG Data QRS amplitude
P-wave amplitude
T-wave amplitude
R to R interval
1st measurement
2nd measurement
3rd measurement
Average Heart Rate
Calculation: HR = 60/avg. R to R interval
Lung Volume Data Measurement One
Measurement Two
Measurement Three
Average
Breath Period (secs/breath)= T2-
T1
Resp. Rate= 60 (sec/min)/breath
Period(sec/breath)
Tidal Volume (mls. breath)
MRV= minute resp. vol=TV x
Resp. Rate
Inspiratory Reserve Volume
Expiratory
Reserve Volume
Vital Capacity= TV + IRV+ ERV