lab tests in hsct
TRANSCRIPT
Lab tests in HSCT
HedayatiHedayatiHedayatiHedayati AslAslAslAsl A.A.A.A.HedayatiHedayatiHedayatiHedayati AslAslAslAsl A.A.A.A.Pediatrics Hematologist & Pediatrics Hematologist & Pediatrics Hematologist & Pediatrics Hematologist & OncologistOncologistOncologistOncologistMAHAK Children’s Cancer Hospital MAHAK Children’s Cancer Hospital MAHAK Children’s Cancer Hospital MAHAK Children’s Cancer Hospital

Lab tests in HSCTHematology
Biochemistry
Virology
CoagulationCoagulation
Culture
Flow cytometry
HLA
Cytogenetic Study
Chimerism(





Other important additional information:
Name of Clinician/Consultant requesting the
testtest
2. Tests requested
3. Clinical details
4. Date of sample

Laboratory test required for donor selection shall be done by accredited laboratory and include at least the following:
• HLA-A, B, DR typing and other appropriate compatibility tests as
indicated by an accredited laboratory.
• ABO group and Rh type. Anti-A and Anti-B titre• ABO group and Rh type. Anti-A and Anti-B titrewhere appropriate.
• Infectious disease screening shall minimally include the following:
• HIV-1, HIV-2 HBV, HCV, CMV and syphilis. Where appropriate, additional test for HTLV-1, HTLV-2, EBV, HAV, VZV, HSV-I, HSVII , toxoplasmosis and cryptosporidium may be performed.

COLLECTION OF SPECIMENS
• VENIPUNCTURE PROCEDURE• Method: Percutaneous Venipuncture
• 1. Identify self to patient.• 2. Properly identify the patient using two unique identifiers. Acceptable
identifiers are patient first and last name and one of the following: date of birth, medical record number, social security number, or driver’s license number.number.
• 3. Verify diet restrictions.• 4. Position patient lying on back with face up or sitting with the appropriate
site exposed.• 5. Wash hands thoroughly and apply clean gloves.• 6. Select venipuncture site.• a. DO NOT USE an extremity with an A-V shunt or status/post mastectomy.• b. DO NOT USE a site with extensive scarring.• c. DO NOT USE a site with a hematoma.• d. DO NOT USE a site with an IV.

7. Prep overlying skin with alcohol using a circular motion. Chloraprep
may be used if patient is allergic to alcohol.
8. Before using, tap all tubes that contain additives to ensure that the
entire additive is dislodged from the stopper and the wall of the tube.
9. Make sure patient’s arm or other venipuncture site is in a downward
position to prevent reflux.
10. Apply tourniquet to extremity 2 inches proximal to desired site.10. Apply tourniquet to extremity 2 inches proximal to desired site.
11. Identify target vein with palpation and visualization.
12. Use thumb to apply tension downward distal to insertion site.
13. Verbally state to patient that the venipuncture is starting and insert
the needle at a 15-30˚ angle and ¼ to ½ inches below the intended
entry into the vein.

Venipuncture procedure when evacuated tubes are used:1. Insert blood collection tube into holder and onto needle up to the recessed
guideline on the Vacutainer® adapter.
2. Position the needle with the bevel up and the shaft parallel to the path of the vein.
3. Insert needle through skin at 15-30˚ angle and ¼ to ½ inches below intended entry
into vein.
4. Grasp the flange of the needle adapter and push the collecting tube forward until
the needle punctures the stopper. Observe for flow of blood into stopper. Maintain
tube below the needle.tube below the needle.
5. Remove tourniquet as soon as possible once blood flow is established.
6. Keep constant, slight forward pressure on the end of the tube to prevent release of
shut-off valve and stop of blood flow.
7. Fill the tube until the vacuum is exhausted and blood flow ceases.
8. When blood flow ceases, remove the tube from the holder. The shut-off valve
recovers the point, stopping blood flow until the next tube is inserted.
9. Tubes containing additives should be mixed immediately upon draw by inverting 5-
10 times. To avoid hemolysis, do not mix vigorously.
10. To obtain additional specimens, insert the next tube into the holder and repeat
steps 7-9.

Venipuncture procedure when using needle and syringe:1. Position the needle with the bevel up and the shaft parallel to the path of the vein.
2. Insert sterile needle or butterfly through the skin at a 15-30˚ angle ¼ to ½ inches below the
intended entry into the vein.
3. Pull back on plunger or syringe slowly until sufficient volume of sample is achieved.
4. Release tourniquet.
5. Withdraw needle and syringe.
6. Apply pressure to site with gauze pad.6. Apply pressure to site with gauze pad.
7. Pierce stopper of collection tube with needle; the evacuated tube will fill to the correct
amount of blood.
8. Immediately activate the safety feature according to manufacturer instructions and discard
without assembly into a sharps container.
9. Check patient’s arm to ensure bleeding has stopped.
10. Apply gauze pad secured lightly with tape to the puncture site.
11. Instruct patient to leave bandage in place for at least 15 minutes.
12. Label all blood tubes at patient’s time of draw.
13. Place labeled specimens in biohazard bag.
14. Discard gloves and wash hands.
15. Place specimen at courier pickup station for processing.

Blood culture collection procedure:
1. For each request for blood cultures on adults when a time or location is not specified by the
doctor, two sets of two bottles will be drawn. Each set of aerobic and anaerobic blood culture
bottles will be obtained from two different sites. Samples will NOT be taken from an arterial
line, heparin lock or a subclavian IV unless specifically ordered by the attending physician.
2. After selecting a good phlebotomy site, the tourniquet will be released and the site disinfected.
3. The site will be cleansed first with chloraprep® using a concentric spiral motion moving from
the site outward.the site outward.
4. Prep the site using an iodine prep using the same motion working from the site outward. Allow
the iodine to dry before drawing specimen.
NOTE: If the patient is allergic to iodine, another topical disinfectant may be used. Any deviation
from routine collection should be noted on the request form or sample bottles.
5. Perform the venipuncture and draw the sample according to procedure. Sample should flow
freely.
6. Carefully change syringe needle and blood transfer device and place 8-10mL of blood into each
vial using aseptic technique. Be sure not to contaminate bottle tops before entering bottle
with needle. Label and send to lab as soon as possible.

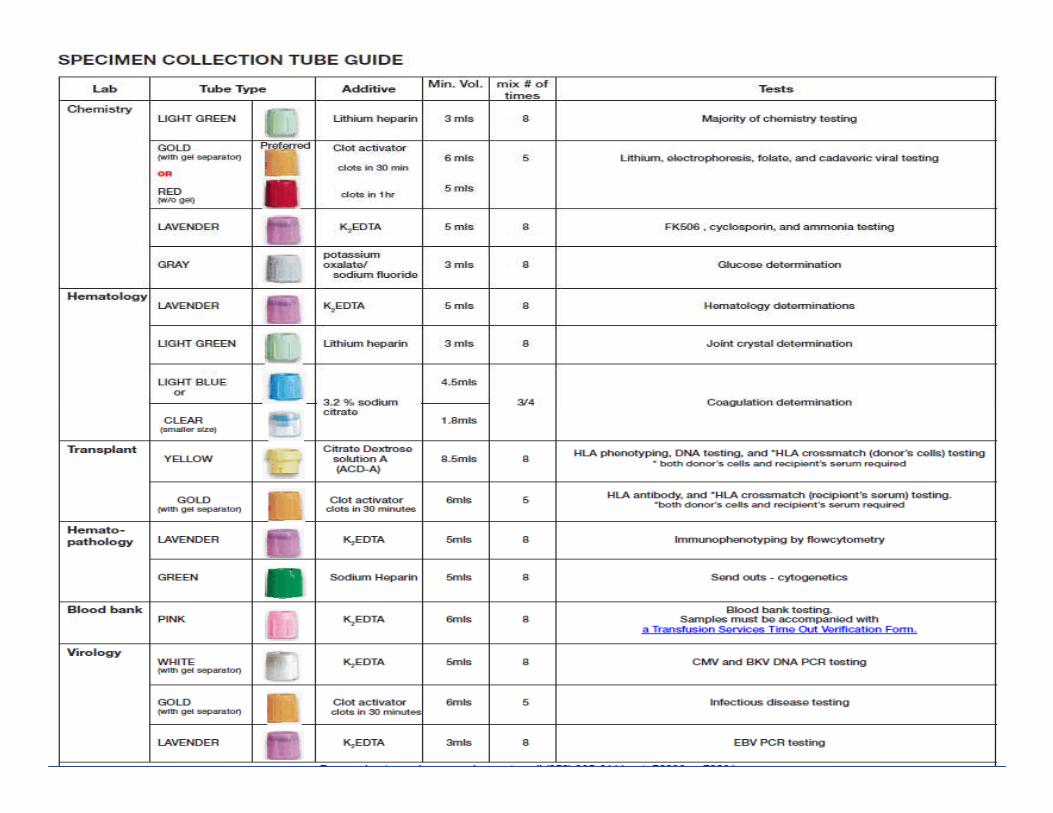
WHOLE BLOOD, SERUM or PLASMA COLLECTION
• The most common sample of laboratory testing is whole blood serum or plasma. The preferred collection method for adults is venipuncture using vacuum collection tubes. The method of collection is similar for whole blood, serum or plasma except for the anticoagulant used. The color of the stopper of the collection tube specifies the anticoagulant content.anticoagulant content.
• Blood should be obtained from a freely flowing venipuncture performed according to current nursing or laboratory venipuncture procedure. Tubes should be collected in the following stopper color order – red, blue, other. All tubes, except red top tubes, should be inverted gently several times in order to mix the anticoagulant. Adequate volume should be collected for the number and types of tests requested. Minimum blood volumes are noted in the collection manual for each test. If insufficient volume is collected, call the laboratory before sending.


LABORATORY TESTS

Lab evaluation
a) Hematology:
CBC with differential CBC with differential
PT/INR/PTT
ABO group and Rh type
antibody screen

A. Complete blood cell counts (CBC),
differential and platelet counts should be
• Measured at each office visit. Patients
receiving ganciclovir (or valganciclovir), daily
Trimethoprim/Sulfamethoxazole (TMP/SMX), Trimethoprim/Sulfamethoxazole (TMP/SMX),
Cellcept (mycophenolate mofetil), and
other myelosuppressive medication should
have a CBC at weekly intervals or more often
• when counts are low.


Blood Smear - Normal



b) Chemistry:
Sodium, Potassium, Chloride, Bicarbonate Glucose Calcium, Albumin Magnesium Phosphate Phosphate BUN, CreatinineTotal Bilirubin (direct and indirect if total bilirubin is elevated) Alkaline PhosphataseAST, ALT Total Protein LDH, Uric Acid

. Liver function tests (LFT's) (alkaline phosphatase, ALT, AST, LDH and total bilirubin)
• Should be measured at each office visit.
Patients receiving immunosuppressive
medications or other hepatotoxic drugs such medications or other hepatotoxic drugs such
as itraconazole, voriconazole, INH, should
have LFT's measured at two-week intervals or
more often when abnormalities are
• present.

Renal evaluation:
Urine analysis 24 hour urine for creatinine24 hour urine for creatinineclearance

Renal function tests (serum creatinine, BUN, and magnesium) should be measured at
• Each office visit. Patients receiving cyclosporine,
tacrolimus (formerly known as FK506),
amphotericin or other nephrotoxic drugs should amphotericin or other nephrotoxic drugs should
have renal function monitored at weekly intervals
or more often when abnormalities are present.
• Dose adjustment may be needed for medications
such as cyclosporine, tacrolimus, ganciclovir,
valciclovir, acyclovir, among others.

Drug levels:
Cyclosporine
tacrolimus (FK506)
Sirolimus (rapamycin)
Itraconazole blood levels should be monitoredItraconazole blood levels should be monitored
KETOCONAZOLE OR VORICONAZOLE SHOULD NOT BE
COADMINISTERED WITH SIROLIMUS.

Blood cultures should be drawn whenever clinically indicated.
• For high risk patients
(i.e., treatment with prednisone at a dose of
more than 1 mg/kg/day), weekly surveillance
blood cultures may be beneficial.blood cultures may be beneficial.
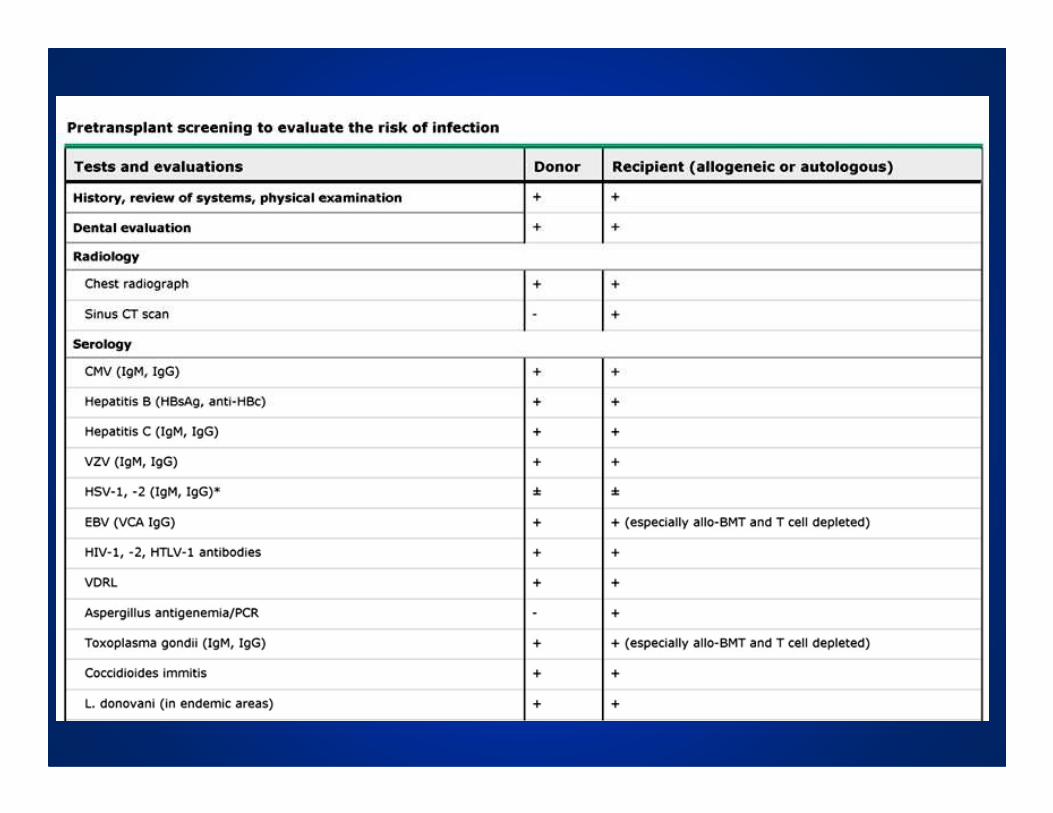
c) Serology: (must be documented within 30
days prior to first day of stem cell collection)
• Cytomegalovirus serology (*Anti-CMV IgG)
• Herpes simplex virus serology (HSV I & II)
• Varicella zoster virus (VZV) serology
• HIV serology (*Anti-HIV-1, *Anti-HIV-2)
• *HIV-1 Antigen
• *Anti-HTLV 1 and 2
• Serologic test for syphylis:
*RPR • *RPR
• Hepatitis A:
• Anti-HAV IgM and IgG
• Hepatitis B:
• *HbsAg - surface antigen
• *Anti-HBc
• Anti-HBs - surface antibody
• Hepatitis C:
• *Anti-HCV

CMV monitoring in blood should be:
CMV surveillance tests:
CMV monitoring can be performed using
CMV DNA by PCR or hybrid capture,
pp67 mRNA, or pp65 antigenemiapp67 mRNA, or pp65 antigenemia
(culture based assays are not
appropriate for monitoring.)
PCR is recommended over pp65
antigenemia

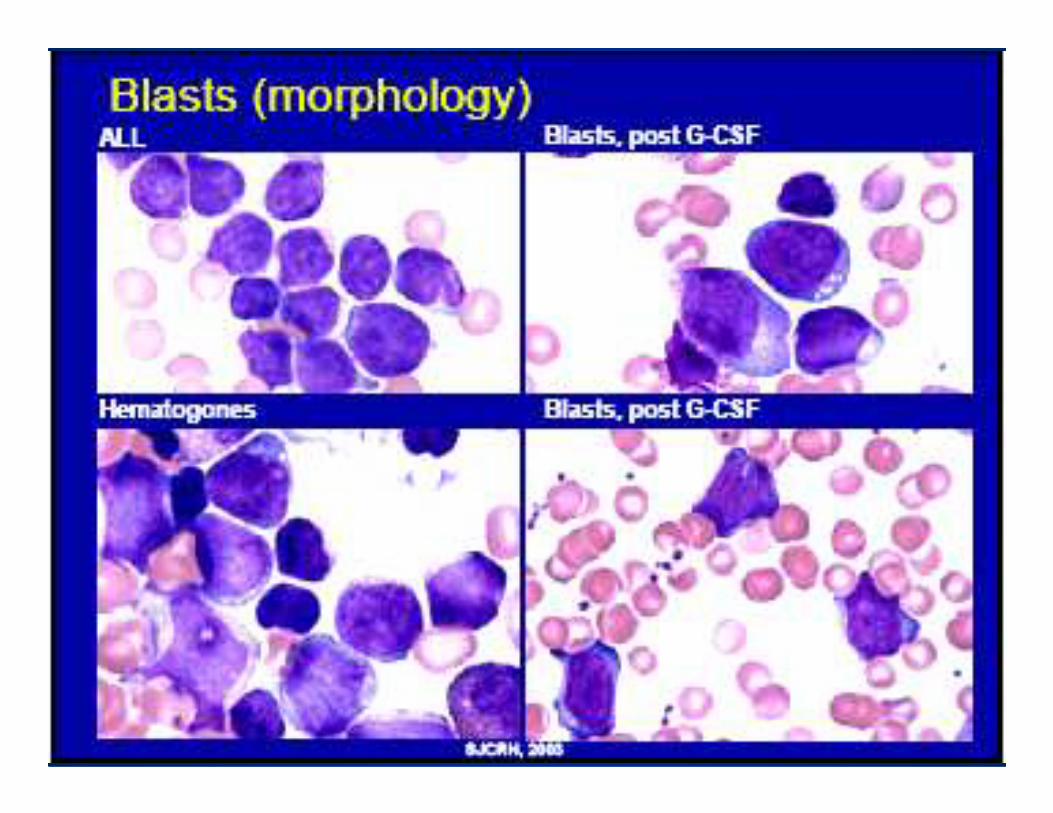
Bone marrow should be evaluated as clinically
indicated and according to specific protocol
Testing should include evaluation of morphology,
immunophenotyping, BCR/abl transcripts or other markers
of minimal residual disease, and cytogenetics as applicable.
Patients transplanted for chronic myeloid leukemia (CML) or Patients transplanted for chronic myeloid leukemia (CML) or
Philadelphia chromosomepositive acute lymphocytic
leukemia (Ph-positive ALL) should have blood tested for
BCR/abl transcripts at 6 month intervals for the first 2 years
after transplant and then at yearly intervals.
When BCR/abl transcripts are detected in the blood, a marrow
aspirate should be evaluated by cytogenetic testing,
morphology and molecular testing of blood samples should
be continued at 6-month intervals.

Stem Cell Laboratory
The Stem Cell Laboratory processes peripheral stem cell and bone marrow products for transplantation purposes. Services provided include:
• Cryopreservation, thawing, and infusion of bone • Cryopreservation, thawing, and infusion of bone marrow, stem cells, and donor lymphocytes
• Red cell depletion and volume reduction of bone marrow products
• Performance of specific cell isolation procedures on peripheral stem cell and bone marrow products


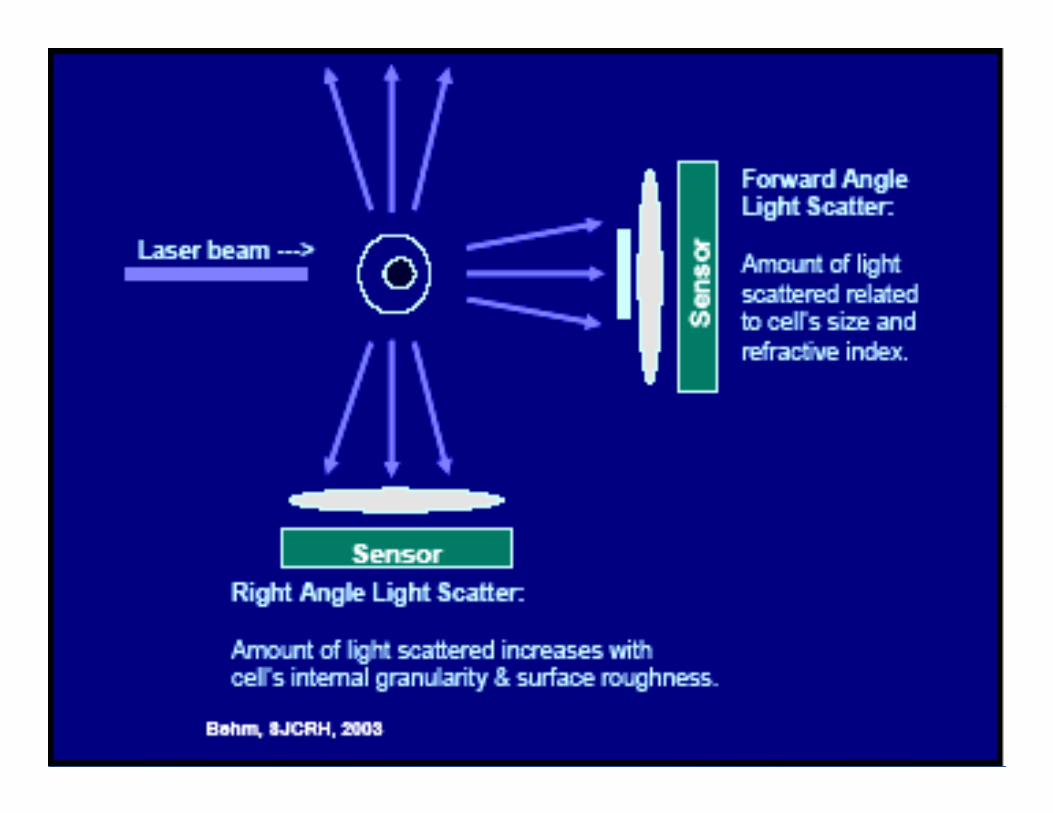
Flow Cytometry Laboratory
The Flow Cytometry laboratory performs flow cytometric analysis used by clinicians in diagnosing, monitoring, and treating patients with the following disorders:
acute and chronic leukemia, lymphoproliferative disease, multiple myeloma, immune deficiencies, multiple sclerosis, and paroxysmal nocturnal hemoglobinuria.
• Acute and chronic leukemia immunophenotyping• Acute and chronic leukemia immunophenotyping
• Lymphoproliferative disorder immunophenotying
• Multiple Myeloma Immunophenotyping
• Paroxysmal Nocturnal Hemoglobinuria testing
• T-cell and T-subset quantitation
• CD3 and CD20 quantitation
• CD34 (Stem Cell) quantitation
• T-cell, B-cell, NK-cell quantitation
















MAJOR HISTOCOMPATIBILITY CLASSES
� Prior to discussing those aspects of T cell function
relevant to the pathogenesis of GVHD, it is helpful
to first briefly review the major Histocompatibility
Complex (MHC) or HLA (for Human Leukocyte Complex (MHC) or HLA (for Human Leukocyte
Antigens) in humans since these molecules
underlie the recognition of antigen by T cells.
� The MHC is highly polymorphic from individual
to individual, and segregates in families in a
Mendelian codominant fashion.

HLA Laboratory
The Histocompatibility (HLA) Laboratory provides HLA-related compatibility testing for solid organ transplants, bone marrow transplants, platelet transfusions, and HLA-associated diseases.
Services include:
• HLA low-resolution serological and low and high-resolution • HLA low-resolution serological and low and high-resolution PCR-based typing for solid organ and stem cell transplantation
• Compatibility testing services for deceased organ donor recovery and allocation
• HLA typing for diseases association
• HLA typing/matching and antibody screening for platelet transfusion and non-hemolytic transfusion Reactions

HLA
�The genes of the HLA locus encode two distinct classes of cell surface molecules, classes I and II.
�Class I molecules are expressed on the surfaces of virtually all nucleated cells at varying densities, while class II molecules are more restricted to cells of the immune system, primarily B lymphocytes and monocytes. system, primarily B lymphocytes and monocytes.
�There are three different class I (HLA-A, -B, -C) and class II (HLA-DQ, -DR, -DP) antigens. HLA-A, -B and -DR antigens appear to be the most important loci determining whether transplanted cells initiate a graft versus host reaction

Tissue typing
• HLA – Human Leucocyte Antigen
• Co-dominant expression of maternal and
paternal epitopes on all leucocytes
• HLA: class 1 ABC, class 2 DR(Q,P,T) class 3 • HLA: class 1 ABC, class 2 DR(Q,P,T) class 3
others
• Blood group can be different
• Sex does not have to be matched

HLA complex

HLA

Human MHC (chromosome 6)
Human MHC
GLO DN DM TAP LMP DO C4B C4A Bf C2 HSP TNF E J H G F
DP DQ DR B C A
Class II Class III Class I
Genes Ags

Family HLA Inheritance

Class I(HLA A, B, Cw)- Found on most nucleated cells & platelets-Present endogenous synthesized antigenic peptides- interact with CD8 on T cells

HLA class II molecules
Class II(DR)
-Found on B cells, monocytes, macrophage, dendritic cells and activated T cells-Present antigenic peptide derived from exogenous proteins - interact with CD4 on T cells

�For each full sibling, a patient has a one in four (25%) chance of a full match.a full match.
�The chance of having a donor is 1-(3/4)n ,where n is the number of siblings ..

Terazaki plate
Ab

Different Alleles
– Class IHLA A 451 allelesHLA B 782 allelesHLA C 238 allelesHLA C 238 alleles
– Class IIHLA DR 525 allelesHLA DQ 105 allelesHLA DP 147 alleles

PlasmaPlasma
PBLPBL
FicollFicoll
Ficoll Density=Ficoll Density=11..077077
RBCsRBCs
BuffyBuffy coatcoat
PMNPMN

The laboratory aims to meet the
following targets in reporting results.
• HLA Type 1-2 weeks
• (HLA-A,B,C,DR,DQ and DP, where applicable)
HLA Antibody Screening 1-2 weeks• HLA Antibody Screening 1-2 weeks
• Post transplant antibody monitoring 1-2 days
• HLA Type of local donor 4-5 hours
• Platelet testing (initial screen) 1-2 days

HLA TESTING FOR RECIPIENTS OF AUTOLOGOUSHAEMATOPOIETIC STEM CELL TRANSPLANTS
• The laboratory provides HLA class I typing and HLA antibody screening for patients requiring autologous haematopoietic stem cell transplant.
• This is to ensure that data is available should • This is to ensure that data is available should the patient become refractory to random donor platelet transfusions.
• Samples required are:10mls EDTA for PCR class I typing10mls Clotted Sample for HLA antibody testing

HLA TYPING FOR HAEMATOPOIETIC STEM CELL TRANSPLANT RECIPIENTS AND POTENTIAL DONORS
• Related family members who are being considered as potential donors are also HLA typed.
• On the request form for the potential donor it should be noted who the patient is.
• HLA typing is performed by both serological assays and • HLA typing is performed by both serological assays and PCR based assays depending on the level of resolution required.
• Samples required are:
• 10mls EDTA for PCR class I and II typing
• 10mls Clotted Sample for HLA antibody testing
• Potential Donor 10mls EDTA for PCR class I (and II typing if compatible for class I)


�ز����� ژ����
Master Mix Preparation
Pre - PCR
Post - PCR

� وا�� Master Mix Preparation
pre-PCRا�� وا�� ��� ���د� ��زي ����ل ��اي ���
� �ات ��� :
Vortexfugeد�"!�� �Vortexfugeد�"!�� �
د�"!�� ������#���
$��ز���'!�� ژ%"

� وا�� Pre-PCR
در ا�� وا�� ����ل ه�ي ���د� +�� در وا�� (�) �� DNA و RNA آ. از ����ران 0�/". +�� ��� ا%��م
�� ه�ي ژ%"�#) ���4ط �) +�د
�ات ��� :
� Real time PCR systemد�"!��
� heating blockد�"!��
� د�"!�� ��#�و��%"��5��ژ
$��ز���'!�� ژ%"

� وا�� Post-PCR
ا�� وا�� ��� 89�� ��7 %"��6 �� ه�ي وا�� (�) �. آ�ر ���ود
�ات ��� :
� �Gel documentationد�"!�� Gel documentationد�"!��
� د�"!�� ا:#"�و/�رز ��
� Heater
$��ز���'!�� ژ%"



(25%in pre-B)
( 25%)






MIXED CHIMERIC STATE
• In the field of HCT, mixed chimerism is defined as the concurrent presence of donor and recipient hematopoietic cells. Several methods have been used to assess mixed chimerism after hematopoietic cell hematopoietic cells. Several methods have been used to assess mixed chimerism after hematopoietic cell transplantation, including determination of the variable number of tandem repeats (VNTR) by restriction fragment length polymorphism (RFLP) analysis, polymerase chain reaction (PCR), and, if applicable, fluorescence in situ hybridization (FISH) for the Y chromosome .

• Engraftment status was routinely analyzed in
the bone marrow at one, two, six, and 12
months after HCT.

Transient mixed chimerism
• Transient chimerism is a dynamic condition
limited to the first two years after HCT. One limited to the first two years after HCT. One
risk factor is the cyclophosphamide dose used
in the conditioning regimen, with mixed
chimerism being less frequent at the full dose
of 200 mg/kg than at lower doses .

Persistent mixed chimerism
• After the second year of follow up, the persistently chimeric patients were submitted to yearly assessment of chimerism status for 2 to 11 years.
• Mixed chimerism was present in bone marrow at the same level as in the peripheral blood, with the exception of one patient in whom there were 25 percent donor cells in the bone marrow, but approximately 70 percent donor cells in the peripheral blood.