laparoscopic aortic surgery
TRANSCRIPT
J.-B Ricco, J. Cau, A. Valagier, G Régnault de la MotheUniversity hospital, Poitiers, France
XV. ULUSAL VASKÜLER CERRAHi KONGRESİ
No conflict of interest to declare
LAPAROSCOPIC AORTIC SURGERYAORTOiLiAK TIKAYICI HASTALIKLAR iÇiN
LAPAROSKOPiK CERRAHi
A Failed Innovation ?

PURPOSE
The purpose of laparoscopic vascular surgery
is to replicate the good and durable results of
the classical open approach in patients with
TASC D lesions or with AAA not amenable to
endovascular treatment

FEASIBILITY
1993: Dion et al. in Surg Laparosc Endosc
First laparoscopy-assisted aortobifemoral bypass
1993-2011: 45 publications (29 from EU)• 1244 patients
830 for occlusive disease
414 for aneurysm

STUDY QUALITY
• All studies were observational, no RCT’s
• Heterogeneity of the studies
• Inadequate description of the study population
• Suspected selection bias of patients
Nio et al. Eur J Vasc Endovasc Surg 2007Nio et al. Eur J Vasc Endovasc Surg 2007

A LESS INVASIVE PROCEDURE !

LAPAROSCOPIC REVOLUTION ?LAPAROSCOPIC REVOLUTION ?

TOTAL LAPAROSCOPY
Coggia et al. Eur J Vasc Endovasc Surg. 2002;24:274-5.

RETROCOLIC PRERENAL APPROACH

AORTIC OCCLUSIVE DISEASE-TASC D

AORTIC OCCLUSIVE DISEASE

LEFT RENAL ARTERY RESTENOSIS

AORTIC ANEURYSM
JUXTA RENAL AORTIC ANEURYSM

LUMBAR ARTERY PLUG

A NEW SURGICAL EXPERTISE ?A NEW SURGICAL EXPERTISE ?

CLINICAL STUDYThis study was planned by a group of vascular
surgeons trained in laparoscopic aortic surgery
to identify potential differences in the 30-day
complication rate of total laparoscopic vs. open
approach for aortic surgery.
Cau J, Ricco JB et al. Total laparoscopic aortic repair for occlusive and aneurysmal disease: first 95 cases. Eur J Vasc Endovasc Surg. 2006
Cau J, Ricco JB. Laparoscopic aortic surgery: Techniques and results. J Vasc Surg 2008 Cau J, Ricco JB. Total laparoscopic renal artery bypass. J Vasc Surg. 2011

METHODS January 2006 to December 2009 228 consecutive patients with AAA or occlusive disease Total laparoscopic aortic surgery =83 open repair =145
Prospective study with propensity scoring
Endpoint : composite adverse event at 30-day:
Death, bleeding, graft thrombosis, MI, respiratory failure,
colon ischemia, evisceration.


VARIABLES OPEN REPAIR(n=145)
LAPAROSCOPY(n=83)
p
Female gender 19 (13.1) 11 (13.3) 0.97
Body mass index 25.6±4.1 25.1±4.4 0.38
COPD 45 (31.0) 24 (28.9) 0.74
Diabetes 12 (8.3) 7 (8.4) 0.97
Dyslipidemia 96 (66.2) 55 (66.3) 0.99
Coronary disease 54 (37.2) 26 (31.3) 0.39
Values in parentheses are percentages
BASELINE CHARACTERISTICS

(*) All variables included in a regression model for propensity score
VARIABLESOPEN REPAIR
(n=145)LAPAROSCOPY
(n=83)p
* Age (years) 67.5±9.8 59.5±11.1 <0.001
* Smoker 88 (60.7) 64 (77.1) 0.01
* eGFR (mL/m/1.73m2) 85±28 96±26 0.005
* AAA 109 (75.2) 30 (36.1) <0.001
* Aortic clamping LevelSupra: 44 (30.3)Infra: 101 (69.7)
Supra: 9 (10.8)Infra: 74 (89.2)
0.007
* ASA classes
ASA 1: 0ASA 2: 36 (24.8)ASA 3: 90 (62.1)ASA 4: 19 (13.1)
ASA 1: 2 (2.4)ASA 2: 30 (36.1)ASA 3: 44 (53.0)ASA 4: 7 (8.4)
0.056
BASELINE CHARACTERISTICS
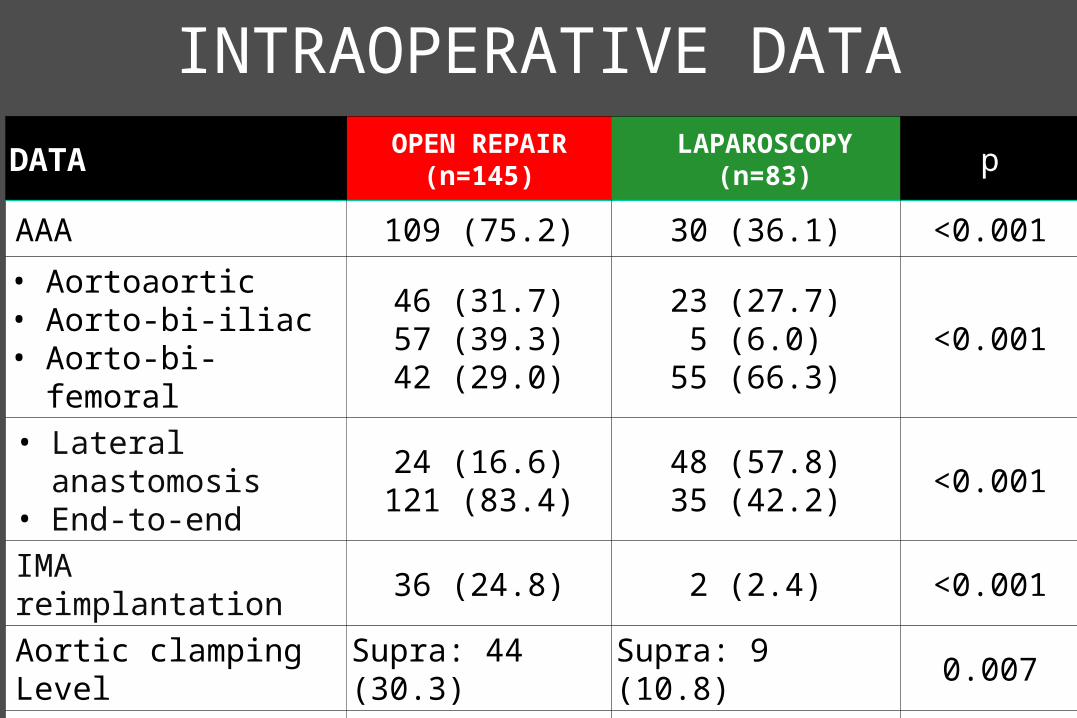
DATA OPEN REPAIR(n=145)
LAPAROSCOPY(n=83) p
AAA 109 (75.2) 30 (36.1) <0.001
• Aortoaortic• Aorto-bi-iliac• Aorto-bi-femoral
46 (31.7)57 (39.3)42 (29.0)
23 (27.7)5 (6.0)
55 (66.3)<0.001
• Lateral anastomosis• End-to-end
24 (16.6)121 (83.4)
48 (57.8)35 (42.2)
<0.001
IMA reimplantation 36 (24.8) 2 (2.4) <0.001
Aortic clamping Level Supra: 44 (30.3) Supra: 9 (10.8) 0.007
Operative time (min) 243±76 282±97 0.002
Aortic clamping time 100±33 116±34 <0.001
INTRAOPERATIVE DATA

RESULTS IN OVERALL SERIES
VARIABLESOPEN REPAIR
(n= 145)LAPAROSCOPY
(n= 83)p
30-day mortality 1 (0.7) 2 (4.1%) 0.14
30-day composite adverse endpoint *
8 (5.5) 23 (27.7) <0.001
Bleeding (mL) 1239±848 1343±1228 0.46
Respiratory complications 23 (15.9) 7 (8.4) 0.11
Any reintervention 6 (4.1) 13 (15.7) 0.002
Graft patency 142 (97.9) 79 (95.2) 0.26
Intensive care unit stay (days)
1.5±6.0 1.0±4.5 0.51
In-hospital stay 11.1±7.3 8.9±5.9 <0.001
* Endpoint : composite adverse event at 30-day: Mortality, Bleeding, graft thrombosis, MI, respiratory failure,
colon ischemia, evisceration, reoperation.

RESULTS IN OVERALL SERIES
End-point: 30-day mortality
• Logistic regression showed that ASA class was the only
independent predictor [OR 8.5, 95%CI 1.3-54.2].
Laparoscopic repair showed a tendency toward higher
mortality risk [OR 7.9, 95%CI 0.76-83.5]
• The small number of patients with AAA prevented
sensitivity analysis in subgroups of patients (AAA vs.
PAOD)

RESULTS IN OVERALL SERIES
End-point: Composite adverse events
• Logistic regression showed that laparoscopic repair was
the only independent predictor of composite adverse
events [OR 7.1, 95%CI 2.9 - 17.6]

PROPENSITY SCORE
The treatment groups differed markedly to
some variables
Need to develop a propensity score by logistic
regression
The calculated propensity score was employed
for a one-to-one matching as well as to adjust
for other variables

MATCHING BASED ON PROPENSITY SCOREMATCHING BASED ON PROPENSITY SCORE
PS Trt A vs. Trt B
Compare treatments based on matched pairs This methodology simulates a RCT
PS1
PS2
PSm

PROPENSITY SCORE-MATCHED PAIRS
VARIABLESOPEN REPAIR
(n=49/145)LAPAROSCOPY
(n=49/83)p
* Age (years) 64.0±10.6 64.0±10.6 0.98
* Smoker 38 (77.6) 32 (65.3) 0.18
* eGFR (mL/m/1.73m2) 96±30 90±25 0.19
* AAA 20 (40.8) 21 (42.9) 0.84
* Aortic clamping LevelSupra: 5 (10.2)Infra: 44 (89.8)
Supra: 6 (12.2)Infra: 43 (87.8)
0.60
* ASA classes
ASA 1: 0ASA 2: 15 (30.6)ASA 3: 27 (55.1)ASA 4: 7 (14.3)
ASA 1: 2 (2.4)ASA 2: 17 (34.7)ASA 3: 27 (55.1)ASA 4: 5 (10.2)
0.84

RESULTS - MATCHED PAIRS
VARIABLESOPEN REPAIR
(n=49/145)LAPAROSCOPY
(n=49/83)p
30-day mortality 0 2 (4.1%) 0.50
30-day composite adverse endpoint *
1 (2.0) 17 (34.7) <0.001
Bleeding (mL) 1210±761 1611±1380 0.30
Respiratory complications 7 (14.3) 4 (8.2) 0.52
Any reintervention 1 (2.0) 10 (20.4) 0.008
Graft patency 47 (95.9) 45 (91.8) 0.68
Intensive care unit stay (days)
1.5±6.9 0.9±3.6 0.74
In-hospital stay 10.7±8.2 9.5±5.7 0.029
* Endpoint : composite adverse event at 30-day: Mortality, Bleeding, graft thrombosis, MI, respiratory failure,
colon ischemia, evisceration, reoperation.

PROPENSITY SCORELOGISTIC REGRESSION
• Patient’s age, indication for surgery and suprarenal
clamping were independent predictors for assigning
patients to laparoscopic or open repair group
• Laparoscopic repair was associated with a higher risk of
30-day composite adverse events [OR 6.5, 95%CI 2.7-
15.5]
• Laparoscopic repair was not associated with lower risk of
respiratory complications [OR 0.76, 95%CI 0.28 – 2.04]

CONCLUSIONS
This study suggests that total laparoscopic
aortic surgery even in well trained hands is not
as safe as open surgery to treat abdominal
aortic aneurysms and TASC D aortic disease.

MINIMALLY INVASIVE AORTIC SURGERY