laparoscopic left adrenalectomy
TRANSCRIPT

Laparoscopic Left Adrenalectomy
Jacques Marescaux, MD, FRCS, Francesco Rubino, MD, andDidier Mutter, MD, PhD
The ideal surgical approach to the adrenal gland hasrepresented a balance between adequate exposure of
deeply located anatomic structures on one hand and thepain and morbidity inherent to some surgical approaches onthe other. Since the initial report by Gagner in 1992,1 lapa-roscopic adrenalectomy has rapidly become the procedureof choice for the treatment of benign adrenal lesions. Lapa-roscopic adrenalectomy generally results in less postopera-tive pain and morbidity, as well as improved cosmetic resultswith respect to its open counterpart.2,3
As in open surgery, the laparoscopic technique can beperformed through a transabdominal or retroperitonealapproach. Whatever the approach of choice, thoroughknowledge of anatomic details and a perfect standardiza-tion of the different steps of the procedure represent thekey for successful performance of this operation.
Laparoscopic adrenalectomy can at times be challeng-ing in obese patients, where even tumoral glands might bedifficult to identify. We consider careful dissection of theadrenal veins, which represent constant landmarks foridentification of the gland, to be of paramount impor-tance. This ‘vascular approach‘ allows safe adrenal vascu-lar control and gland dissection even when the glandcannot be readily identified, as in obese patients.
The left adrenal gland often poses more challenges thanthe right gland laparoscopically. Early in our experience,before determining a precise strategy of vascular dissec-tion, one patient had to be converted to an open-proce-dure because of the inability to clearly identify the adrenalgland in the perirenal fat. This difficulty has been de-scribed by Miccoli,4 who suggested the use of laparo-scopic ultrasonographic exploration. For these reasons,we have tried to define a precise operative strategy thatcan allow complete dissection of the adrenal area withoutthe need for routine gland identification.
INDICATIONS ANDCONTRAINDICATIONS
Previous surgery, especially when performed on the kid-ney, pancreas, or spleen can cause significant adhesionsin the operative area and may render the transperitonealapproach challenging especially for surgeons with limitedlaparoscopic experience. Most authors set the size limit ofthe adrenal gland to be removed at 10 cm for an easy andsafe dissection.5 The laparoscopic approach in cancer pa-tients is a source of concern, as the benefit of the laparo-scopic route must be balanced against the risk of cancerdissemination. Recent reports suggest that this concernmight be unjustified; for instance, local and port-site re-currence after laparoscopic colon cancer resection arenow believed to be dependent on inadequate laparoscopicexperience and inappropriate handling of the tumor siteduring laparoscopy, rather than being the result of thelaparoscopic approach per se. However, adrenal cancer isparticularly aggressive, and the adrenal capsule and tissueare easy to fracture when inappropriately handled, thus,we do not recommend laparoscopic adrenalectomy whenthere is a preoperative suspicion of adrenal cancer. As anexample, feminizing tumors, which are most often malig-nant, should probably be considered as a contraindicationfor laparoscopic resection.
Several studies have demonstrated that laparoscopicresection of pheochromocytoma can be performed safelyand without specific complications.6,7
The optimal indications for a laparoscopic approachare incidentalomas, Conn adenomas, benign Cushingtumors (adenomas), and virilizing tumors. These areusually small (1.0 to 5.0 cms in diameter) and easy todissect.
Because of its lower morbidity and better cosmesis,there is a ‘risk’ that the laparoscopic technique might beerroneously proposed for incidentalomas that would nototherwise be considered surgical. Incidentalomas have afrequency of about 1.3% of all patients undergoing ab-dominal computed tomography (CT) and this frequencymay rise as high as 8% in necropsy series. The incidenceof adrenocortical carcinoma, however, is rare at1/800,000. Larger lesions (�6.0 cm) are associated withan increased risk of malignancy. Although there is nodoubt that an incidentaloma larger than 6 cm should beremoved, no indications for operation are present when
From the IRCAD-EITS (European Institute of Telesurgery), University LouisPasteur, Strasbourg, France.
Address reprint requests to Dr Jacques Marescaux IRCAD-EITS (EuropeanInstitute of Telesurgery), University Louis Pasteur, 1 Place de l’Hopital, 67091Strasbourg, France.
Copyright 2002, Elsevier Science (USA). All rights reserved.1524-153X/02/0404-0108$35.00/0doi:10.1053/otgn.2002.00000
309Operative Techniques in General Surgery, Vol 4, No 4 (December), 2002: pp 309-321

tumors are smaller than 3 cm. Miccoli and co-workers8
have recently documented an increase in the number ofpatients referred for adrenalectomy since the introduc-tion of laparoscopic adrenalectomy. Interestingly, dataavailable suggest that although the criteria for patientselection have not changed, more patients with adrenal
metastases and incidentalomas are being operated onlaparoscopically.
Other general contraindications for laparoscopic adrenal-ectomy include cranial hypertension, noncorrectable bleed-ing disorders, or cardiovascular and respiratory diseases thatwould be contraindications to surgery in general.
ANATOMY OF THE LEFT ADRENAL GLAND
1 The left adrenal gland varies in shape but it is generally smaller than theright. It is located within the renal fossa, above the upper part of the medialaspect of the left kidney. The arterial blood supply of the left adrenal isessentially composed of three pedicles. The left superior pedicle originates inmost cases from the left inferior phrenic artery and branches in short de-scending vessels that enter the upper pole of the gland. The left middlepedicle is situated behind the accessory adrenal vein and originates directlyfrom the aorta in most cases. It branches into short vessels that enter thecentral part of the gland. The left inferior pedicle is located in an anteriorposition with respect to the plane of the gland. It originates from the left renalartery and branches into short vessels that enter the inferior part of the gland.The left adrenal gland is drained mostly by the main adrenal vein, whichreceives the left inferior phrenic vein. The main adrenal vein enters the leftrenal vein.
310 Marescaux et al

OPERATIVE TECHNIQUE
2 Instruments. Atraumatic graspers, scissors, coagulating hook, and au-tomatic clip applier are common to many laparoscopic procedures. Morespecific for adrenalectomy are small peanut swabs placed at the tip ofgraspers, allowing smooth mobilization of the gland. A right-angled grasperor vascular clamp should be ready on the operative table. A large atraumaticgrasper can be used for the mobilization of the adrenal gland to avoidbleeding during its manipulation. A needle holder must be available toperform intracorporeal laparoscopic suturing should it be required to repairvessel injury. Safe dissection requires the highest quality three-chip CCDcamera. The operation is performed using a 0° angled endoscope.
311Laparoscopic Left Adrenalectomy

3 The procedure is performed under general anesthesia, with musclerelaxation and controlled ventilation. The patient is placed in a full lateralright decubitus position. A cushion is placed under the right flank. The tableis angled to maximize exposure of the space between the costal margin andthe iliac crest, taking care to avoid excessive tension of the abdominal wallmuscles, which may reduce distention of the abdominal wall during insuf-flation and thus reducing the working space. The patient’s legs are bent toavoid stretching of the crural nerve. The surgeon stands on the abdominalside of the patient, facing the monitor at the head of the patient. Theassistant stands next to the surgeon. If a second monitor is available, theassistant may stand opposite the surgeon, facing the monitor placed behindthe surgeon.
312 Marescaux et al

4 Pneumoperitoneum is induced by an open approach at the site of thefirst trocar. CO2 insufflation is maintained at a pressure of 12 mm Hg. Fourtrocars are used. A 10 mm trocar is inserted in the subcostal space at theanterior axillary line for the introduction of a 10 mm 0-degree laparoscope.Two other 10 mm trocars are inserted under direct vision about 7 cm oneach side of the first trocar below the costal margin. They receive graspersfor exposure of the operative field, for the introduction of atraumatic grasp-ers, hook, retractors, instruments with peanut swabs and coagulating scis-sors. The fourth trocar is inserted below the first one, at a distance of 4 to 5cm. Through this trocar, several instruments can be passed, such as hook,scissors or clip applier as well as a peanut swab placed into a grasper’s jawswhich is used for gentle retraction.
313Laparoscopic Left Adrenalectomy

5 Excellent exposure of the operative field is the key to success. Severalparietal or splenocolic adhesions need to be freed to avoid bleeding or injuryduring introduction of the instruments. The procedure starts with incisionof the splenoparietal ligament using coagulating scissors or hook. Dissec-tion starts at the posterior and inferior edge of the spleen. A margin of 2 cmof peritoneum must be left along the lateral and posterior edge of the spleenand used to retract the organ to expose its posterior surface. This dissectionis performed all the way up to the diaphragm, far enough to visualize thegreater curvature of the stomach and the left crus of the diaphragm. For thisstep, a 30-degree endoscope is utilized.
314 Marescaux et al
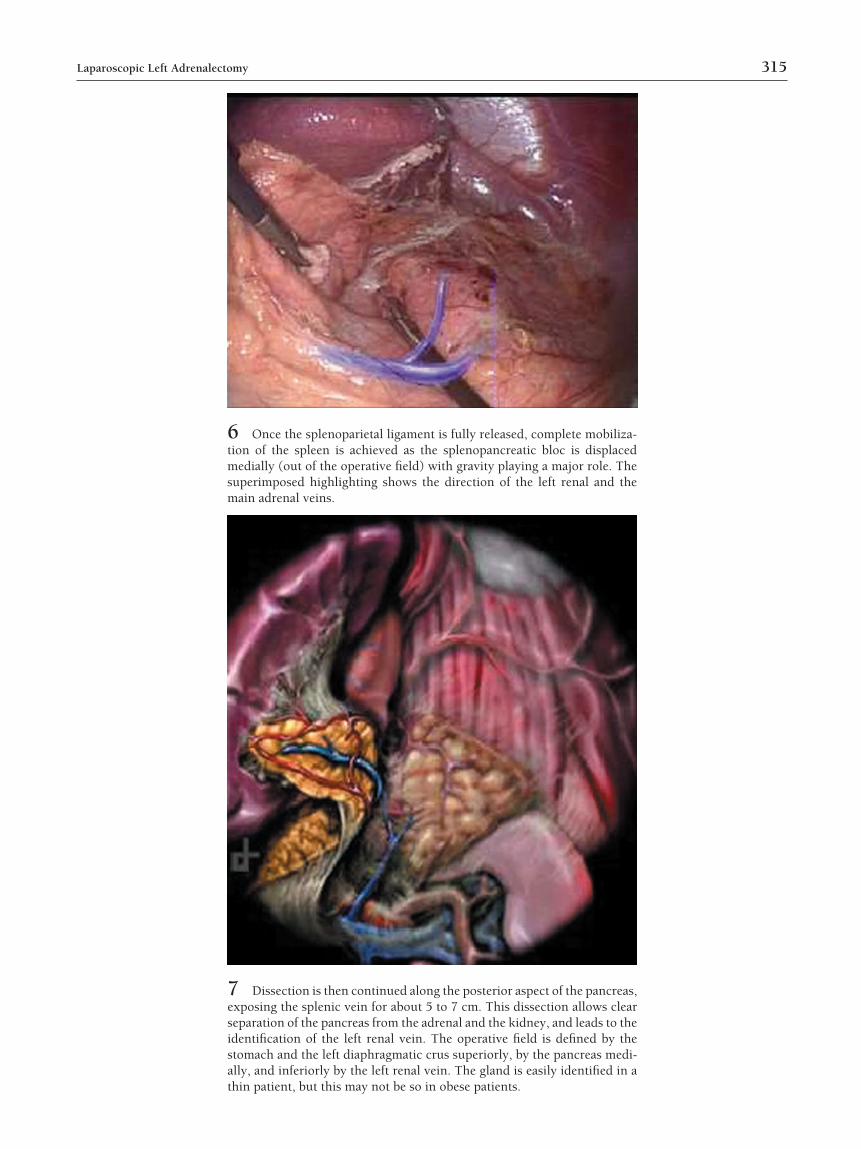
6 Once the splenoparietal ligament is fully released, complete mobiliza-tion of the spleen is achieved as the splenopancreatic bloc is displacedmedially (out of the operative field) with gravity playing a major role. Thesuperimposed highlighting shows the direction of the left renal and themain adrenal veins.
7 Dissection is then continued along the posterior aspect of the pancreas,exposing the splenic vein for about 5 to 7 cm. This dissection allows clearseparation of the pancreas from the adrenal and the kidney, and leads to theidentification of the left renal vein. The operative field is defined by thestomach and the left diaphragmatic crus superiorly, by the pancreas medi-ally, and inferiorly by the left renal vein. The gland is easily identified in athin patient, but this may not be so in obese patients.
315Laparoscopic Left Adrenalectomy

VASCULAR DISSECTION
8 Venous Landmarks. (A) The renal vein, the principal landmark thatleads to the adrenal vein, is exposed along its anterior and superior aspect.The adrenal vein usually has an oblique orientation but can sometimes bedisplaced horizontally in case of bulky tumors and may easily be confusedwith the renal vein. (B) Once the adrenal vein is identified, it is isolated,often using a right angled dissector, and doubly clipped and divided.
316 Marescaux et al

9 (A) Dissection is then directed to the superior and medial side of themain adrenal vein where this is often joined by an accessory vein (inferiorphrenic). (B) This vein is clipped and divided with the main venous con-nections of the gland transected, the dissection is now aimed at identifica-tion and control of the arterial pedicles.
317Laparoscopic Left Adrenalectomy

10 Arterial Control. The medial adrenal artery (1), arising from theaorta, can be identified just below the accessory vein. It is dissected andclipped.
318 Marescaux et al

11 At this point, the right side of the gland is dissected superiorly to thediaphragm in an avascular plane, the gland being gently retracted to the left.The diaphragmatic artery can be recognized at the upper pole of the dissec-tion, leading to the superior adrenal artery which is dissected and dividedafter clip applications. The superimposed highlighting shows the positionand direction of the superior adrenal artery (2). The lateral and posterioraspects of the gland are then freed by progressive dissection of the fat.
319Laparoscopic Left Adrenalectomy

12 (A) Dissection is continued along the inferior edge of the gland,which is freed by coagulation of multiple attachments. The gland can bemobilized upward using a peanut swab mounted on atraumatic graspers.When the dissection is performed on the right side of the gland, the inferiorartery can be identified; it frequently branches in two vessels, which can bedivided separately after clip application. B shows the same detail withsuperimposed highlighting identifying the underlying position and direc-tion of the inferior adrenal artery (3).
320 Marescaux et al

Postoperative ManagementThe patient can ambulate on the same day. Liquid intakeis resumed on the night of the day of operation. Normaldiet is started on the first postoperative day. Patients areusually discharged from the hospital on the second orthird day postoperatively.
AcknowledgmentThe authors thank Websurg® for the drawings and picturesof this article.
REFERENCES1. Gagner M, Lacroix A, Bolte E: Laparoscopic adrenalectomy in
Cushing’s syndrome and pheochromocytoma. N Engl J Med327(14):1033, 1992
2. Hazzan D, Shiloni E, Golijanin D, Jurim O, Gross D, Reissman P:Laparoscopic vs. open adrenalectomy for benign adrenal neo-plasm. Surg Endosc (11):1356-8, 2001
3. MacGillivray DC, Shichman SJ, Ferrer FA, Malchoff CD: A com-parison of open vs laparoscopic adrenalectomy. Surg Endosc Oct;10(10):987-90, 1996
4. Miccoli P, Iacconi P, Conte M, Goletti O, Buccianti P: Laparo-scopic adrenalectomy. J Laparoendosc Surg (4):221-6, 1995
5. Gagner M: Laparoscopic adrenalectomy. Surg Clin North Am76(3):523-37, 1996
6. Gaur DD: Rretroperitoneal surgery of the kidney. Ureter and ad-renal gland. End Surg 3:3-8, 1995
7. Eigelberger MS, Duh QY: Pheochromocytoma. Curr Treat Op-tions Oncol (4):321-9, 2001
8. Miccoli P, Raffaelli M, Berti P, Materazzi G, Massi M, Bernini G:Adrenal surgery before and after the introduction of laparoscopicadrenalectomy. Br J Surg 89(6):779-82, 2002
13 Dissection is continued along the upper pole of the kidney using ahook, coagulating scissors, or ultrasonic shears. The adrenal gland can becompletely freed and inserted into an extraction bag before being removedthrough one of the trocar sites. Trocar sites can be slightly enlarged ifneeded to accommodate large adrenal lesions. A drain can be placed andremoved within 24 to 48 hours. Careful port site closure is recommended toavoid incisional hernias.
321Laparoscopic Left Adrenalectomy