laser tissue interaction class - biophotonics labbiophotonics.gist.ac.kr/course materials/laser...
TRANSCRIPT

Laser in OphthamologyLaser – Tissue Interaction Class
Hoang Phuong Lien
20161009
Department of Biomedical Science and Engineering
Single Molecule Biology and Cellular Dynamics Lab

Content
Introduction
Structure of a human eye
LASER
Application of laser in Ophthamology
Photothermal therapy
Photodynamic therapy
Photomechanical interaction

Introduction: Structure of human eye
Fig 1. Scheme of a human eye
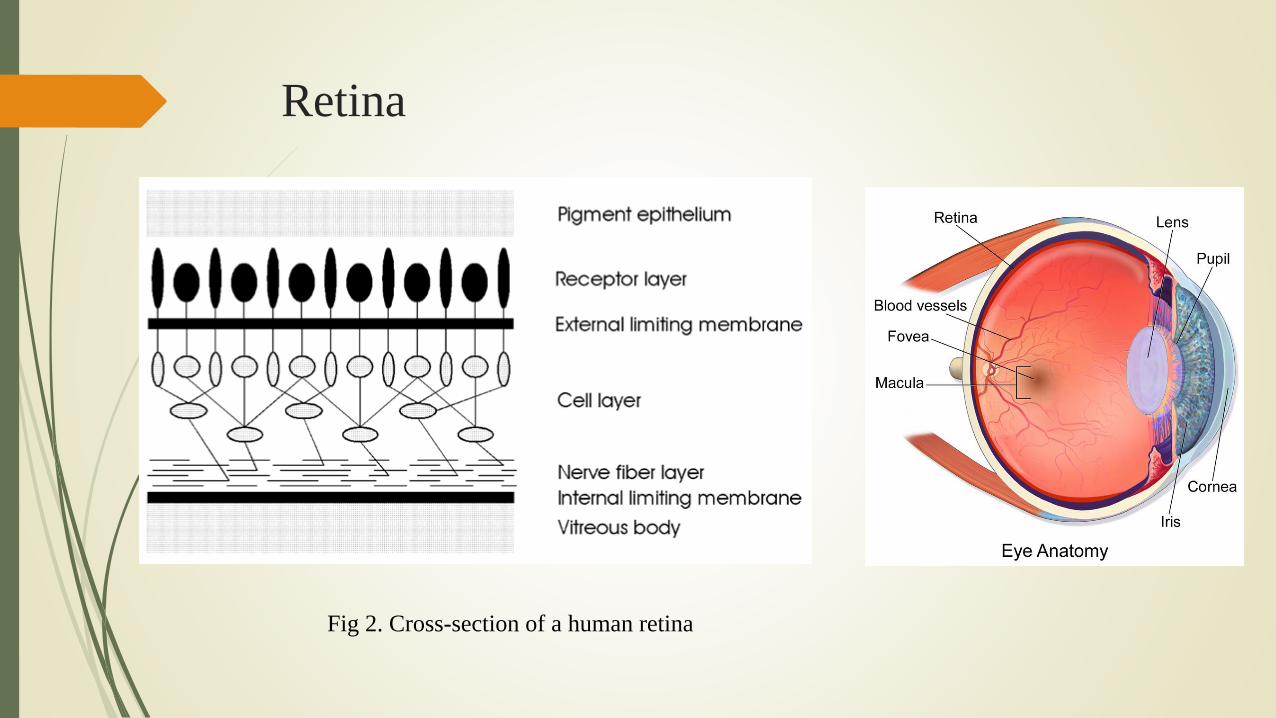
Retina
Fig 2. Cross-section of a human retina
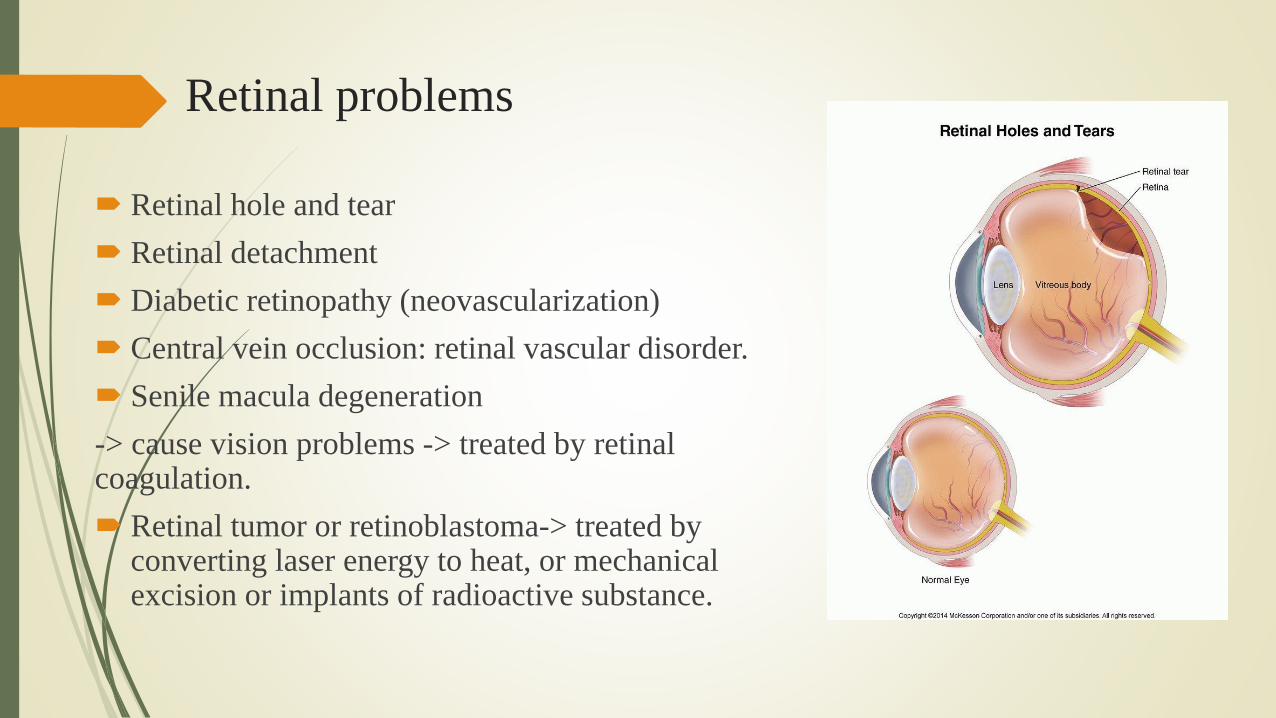
Retinal problems
Retinal hole and tear
Retinal detachment
Diabetic retinopathy (neovascularization)
Central vein occlusion: retinal vascular disorder.
Senile macula degeneration
-> cause vision problems -> treated by retinal coagulation.
Retinal tumor or retinoblastoma-> treated by converting laser energy to heat, or mechanical excision or implants of radioactive substance.

Vitreous Body
Transparent gel,
Consists of 98-99.7 % of waters
The formation of new membranes and
neovascularizations extending from retina into
vitreous body could be problems.
-> Thermally acting lasers should be used for treatment
due to the direct vicinity of the retina.
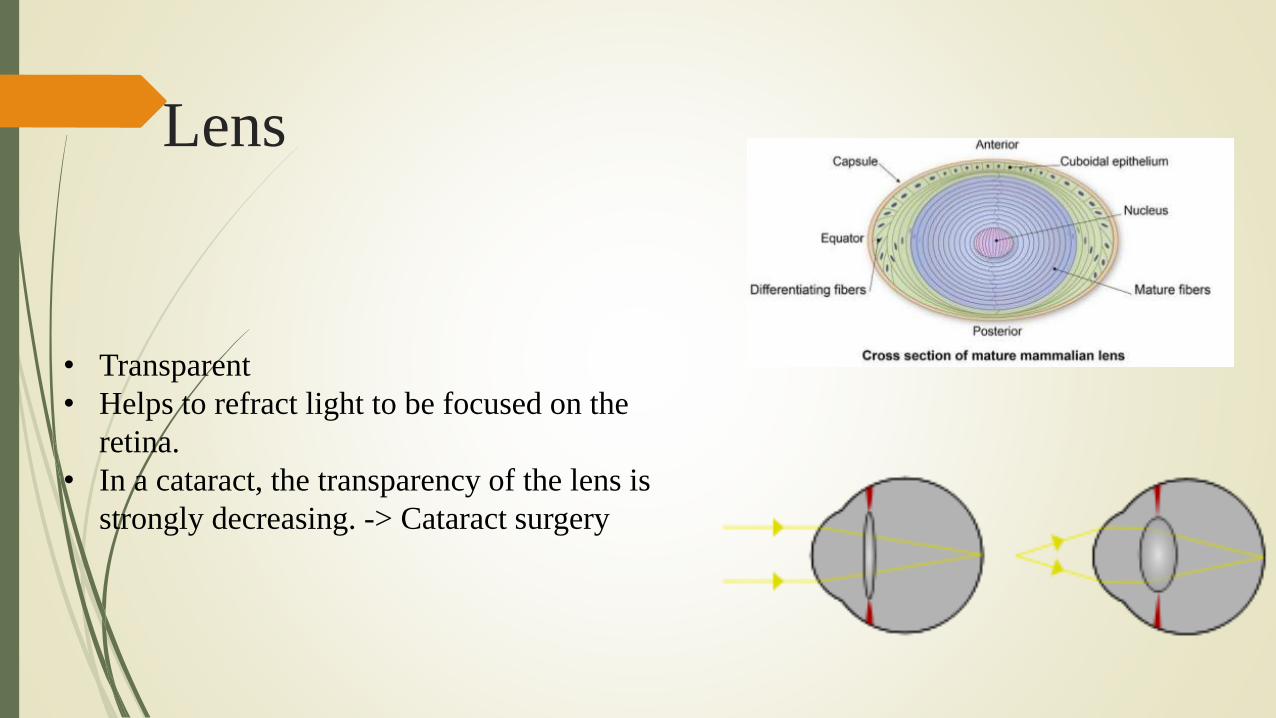
Lens
• Transparent
• Helps to refract light to be focused on the
retina.
• In a cataract, the transparency of the lens is
strongly decreasing. -> Cataract surgery
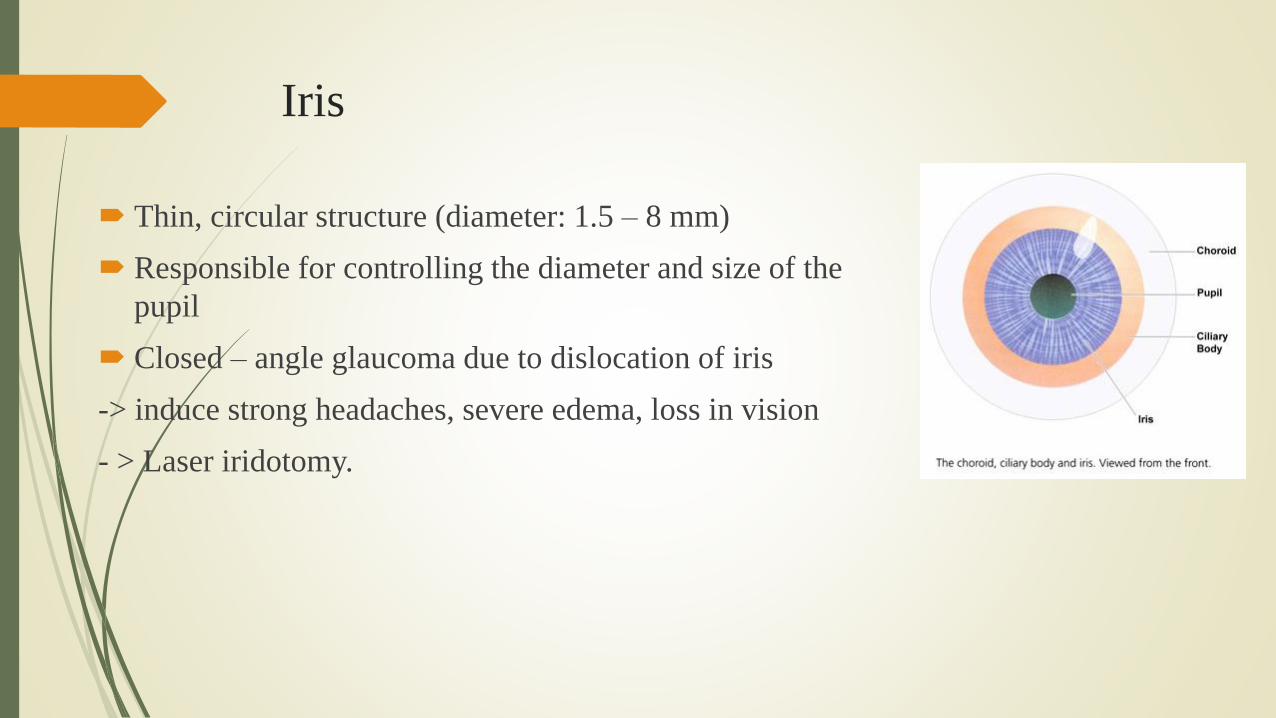
Iris
Thin, circular structure (diameter: 1.5 – 8 mm)
Responsible for controlling the diameter and size of the
pupil
Closed – angle glaucoma due to dislocation of iris
-> induce strong headaches, severe edema, loss in vision
- > Laser iridotomy.
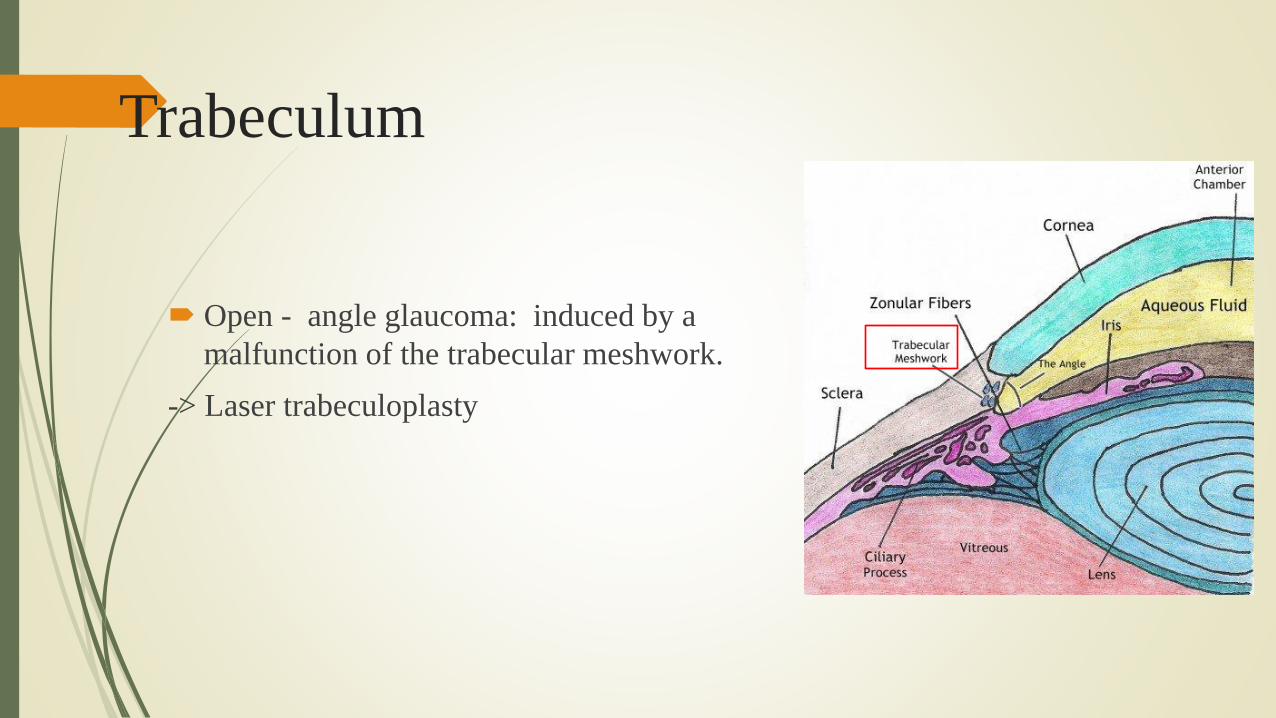
Trabeculum
Open - angle glaucoma: induced by a
malfunction of the trabecular meshwork.
-> Laser trabeculoplasty
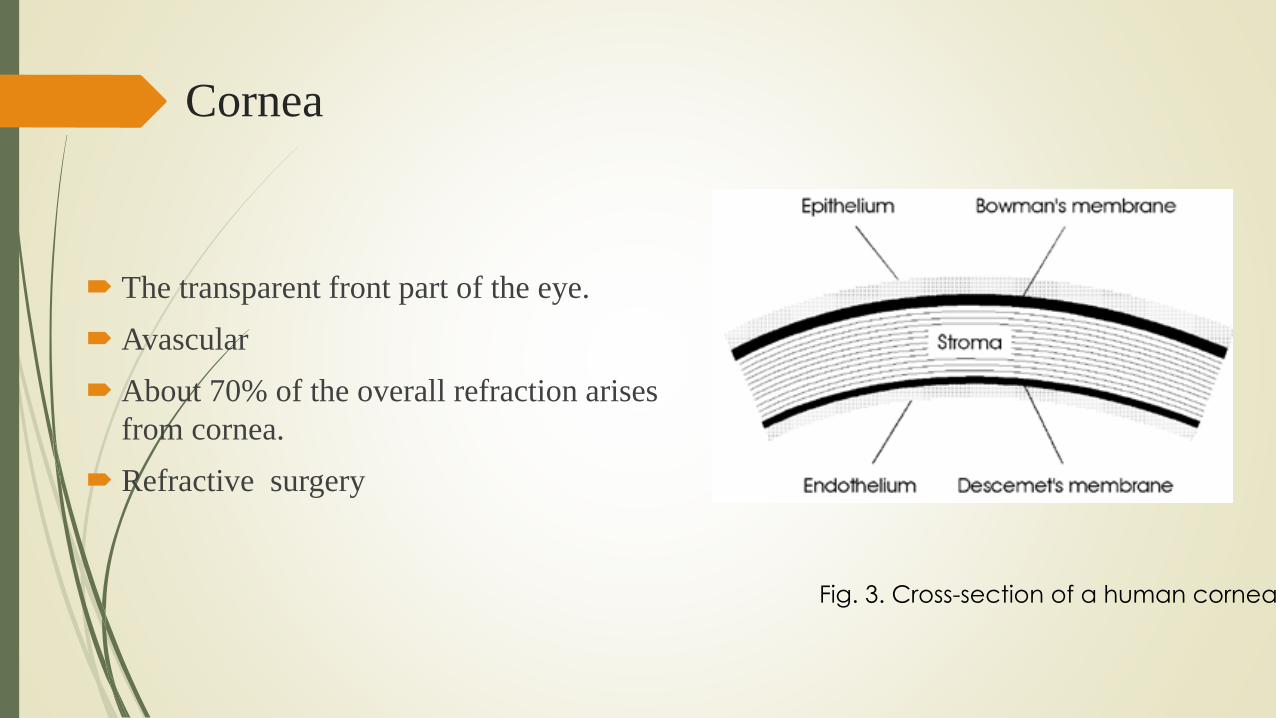
Cornea
The transparent front part of the eye.
Avascular
About 70% of the overall refraction arises
from cornea.
Refractive surgery
Fig. 3. Cross-section of a human cornea
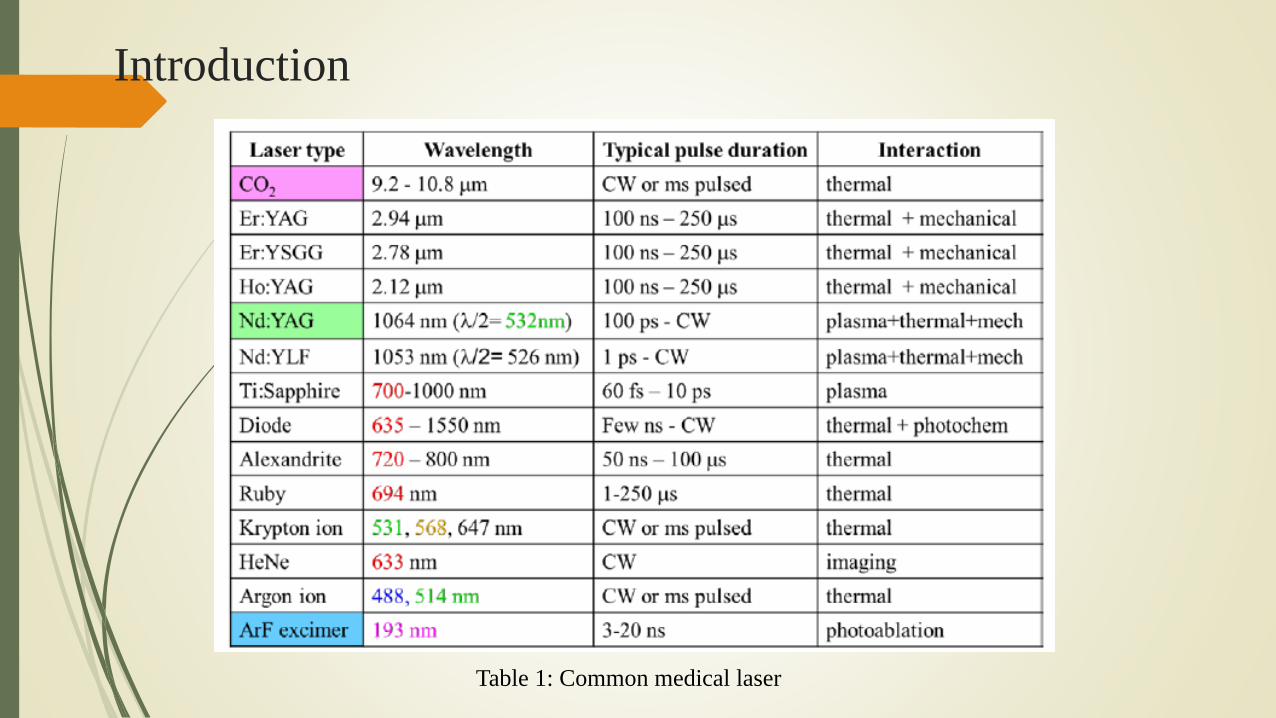
Introduction
Table 1: Common medical laser

Introduction
Fig 4A. Absorption spectra of the major ocular
chromophores
Fig 4B: Absorption spectra of the major ocular chromophores in
the visible part of the spectrum, including Hemoglobin, Melanin
and Xantrophyll.

Content
Introduction
Structure of a human eye
LASER
Application of laser in Ophthamology
Photothermal therapy
Photodynamic therapy
Photomechanical interaction

Photothermal Therapy:
Photothermal Interaction

Photocoagulation
Laser energy : Absorbed primarily by
Melanin in the RPE and choroid
Hemoglobin in blood.
Common lasers in photocoagulation
Frequency-doubled Nd:YAG (532 nm)
Yellow semiconductor lasers (577 nm).
Safe and effective for proliferative diabetic retinopathy.
Beetham (1970) observed that patients with retinal scars (lack photoreceptors) do not develop neovascularization.
Figure 5. Histology of the rabbit retina, with major
chromophores, and the fraction of the laser beam absorbed in
various retinal layers. CH- horiocapillaris, PC – pigmented
choroid, NPC – non-pigmented choroid.
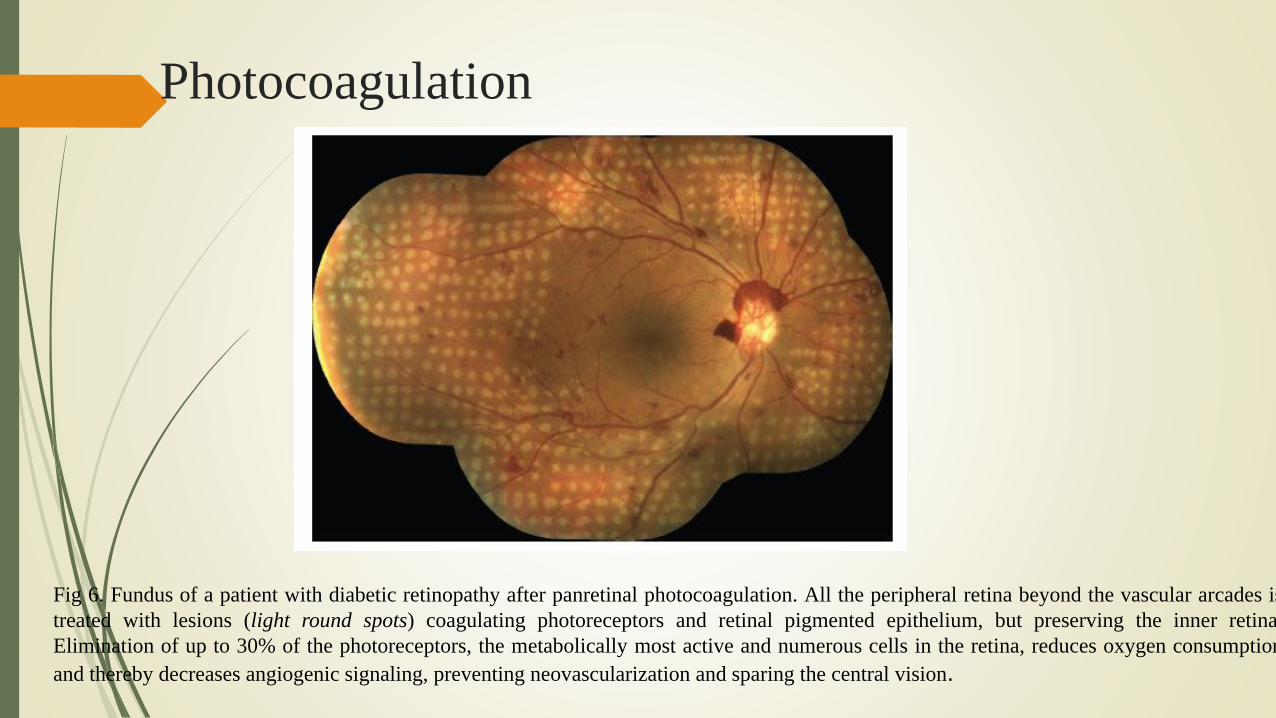
Photocoagulation
Fig 6. Fundus of a patient with diabetic retinopathy after panretinal photocoagulation. All the peripheral retina beyond the vascular arcades is
treated with lesions (light round spots) coagulating photoreceptors and retinal pigmented epithelium, but preserving the inner retina.
Elimination of up to 30% of the photoreceptors, the metabolically most active and numerous cells in the retina, reduces oxygen consumption
and thereby decreases angiogenic signaling, preventing neovascularization and sparing the central vision.

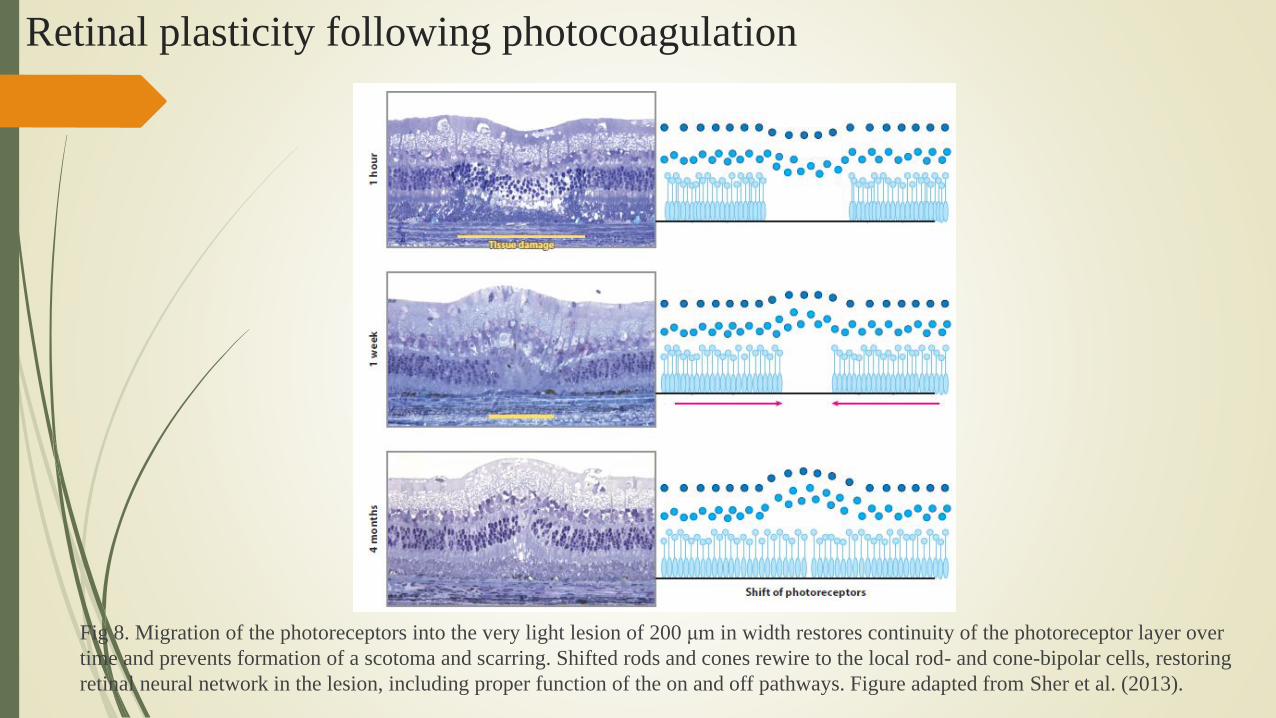
Retinal plasticity following photocoagulation
Fig 7. Intense burn (a, b), and light burn (c, d) (100ms laser pulses)
Retinal plasticity following photocoagulation
Fig 8. Migration of the photoreceptors into the very light lesion of 200 μm in width restores continuity of the photoreceptor layer over
time and prevents formation of a scotoma and scarring. Shifted rods and cones rewire to the local rod- and cone-bipolar cells, restoring
retinal neural network in the lesion, including proper function of the on and off pathways. Figure adapted from Sher et al. (2013).

Optimization of pulse duration
Fig 9. (a) Laser power required to create retinal lesions increases with decreasing pulse duration (measured with 132-μm spot
size on the retina). (b) The range of powers between photocoagulation and rupture (the therapeutic window) decreases with
decreasing pulse duration, making visible photocoagulation unsafe with pulses shorter than 10 ms.
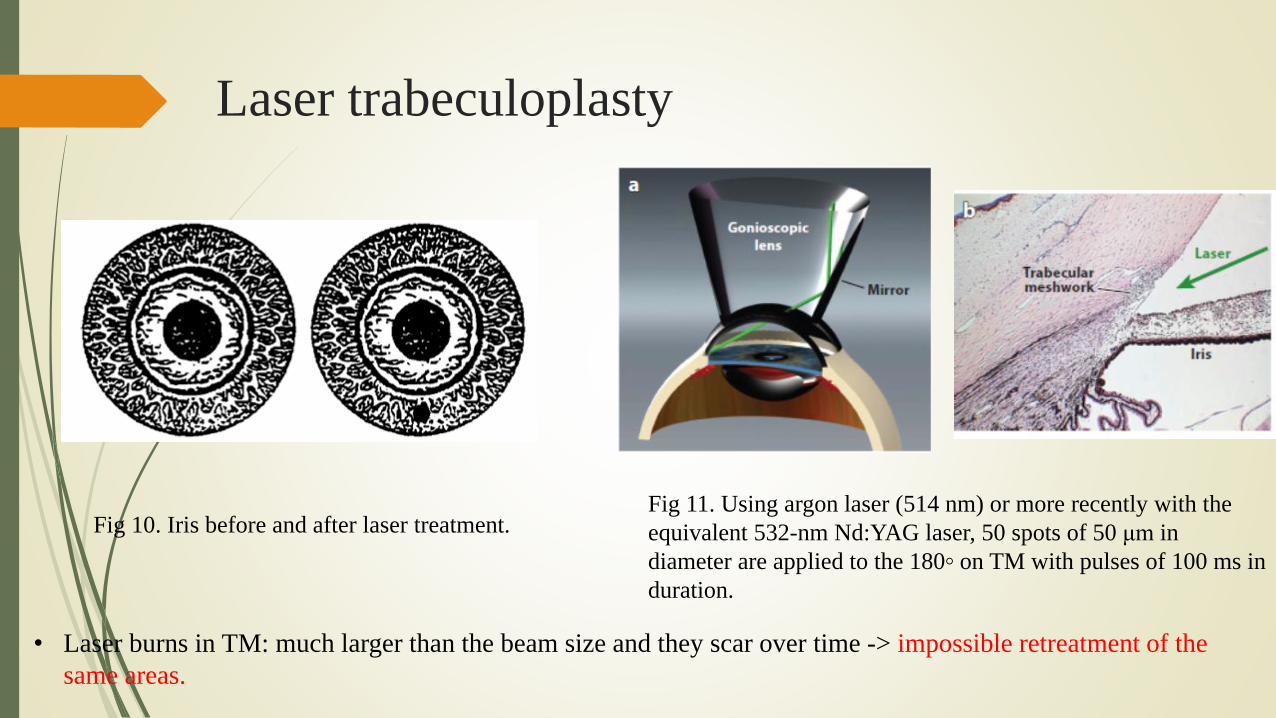
Laser trabeculoplasty
Fig 11. Using argon laser (514 nm) or more recently with the
equivalent 532-nm Nd:YAG laser, 50 spots of 50 μm in
diameter are applied to the 180◦ on TM with pulses of 100 ms in
duration.
Fig 10. Iris before and after laser treatment.
• Laser burns in TM: much larger than the beam size and they scar over time -> impossible retreatment of the
same areas.

Real-time monitoring of tissue temperature
To provide uniform outcomes, because:
The strong variation in fundus pigmentation
Different transparency
Transducer: detect acoustic waves generated in
melanosomes irradiated with nanosecond laser
pulses (Schuele et al. 2004)
Fig 12. Setup for optoacoustic measurements during selective RPE
treatment. A standard contact lens is modified with a piezoelectric
transducer
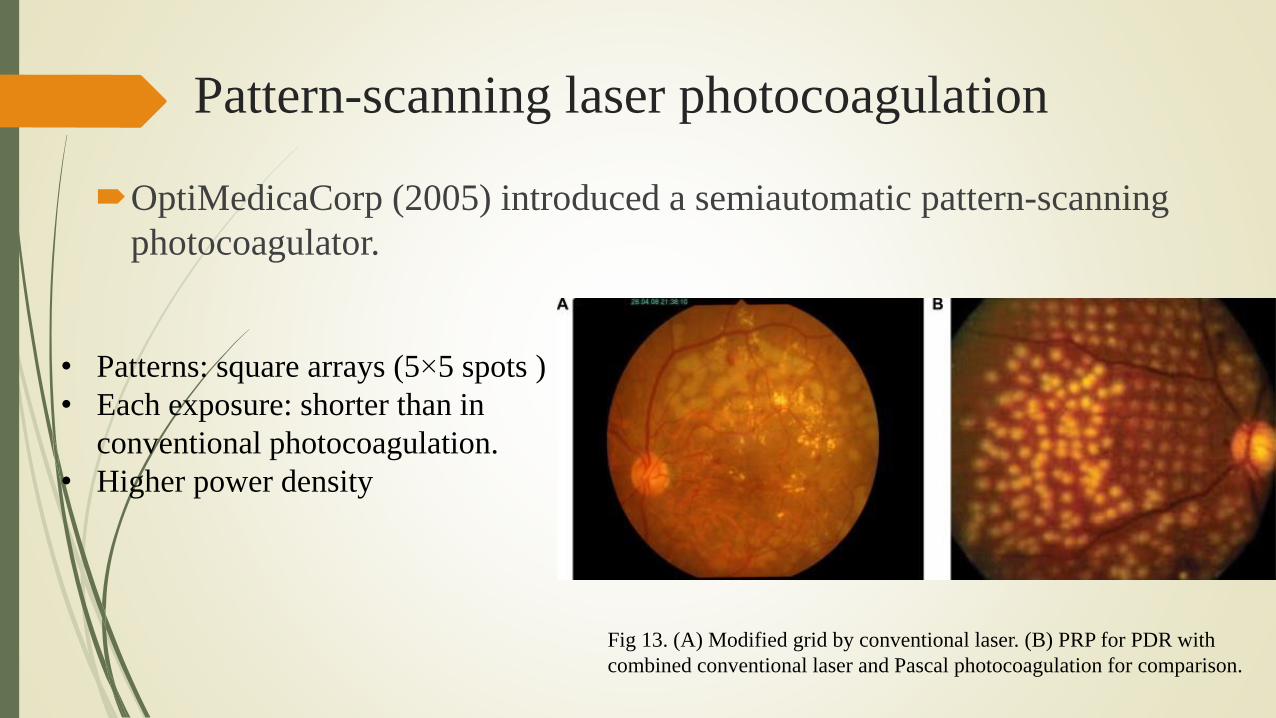
Pattern-scanning laser photocoagulation
OptiMedicaCorp (2005) introduced a semiautomatic pattern-scanning
photocoagulator.
• Patterns: square arrays (5×5 spots )
• Each exposure: shorter than in
conventional photocoagulation.
• Higher power density
Fig 13. (A) Modified grid by conventional laser. (B) PRP for PDR with
combined conventional laser and Pascal photocoagulation for comparison.
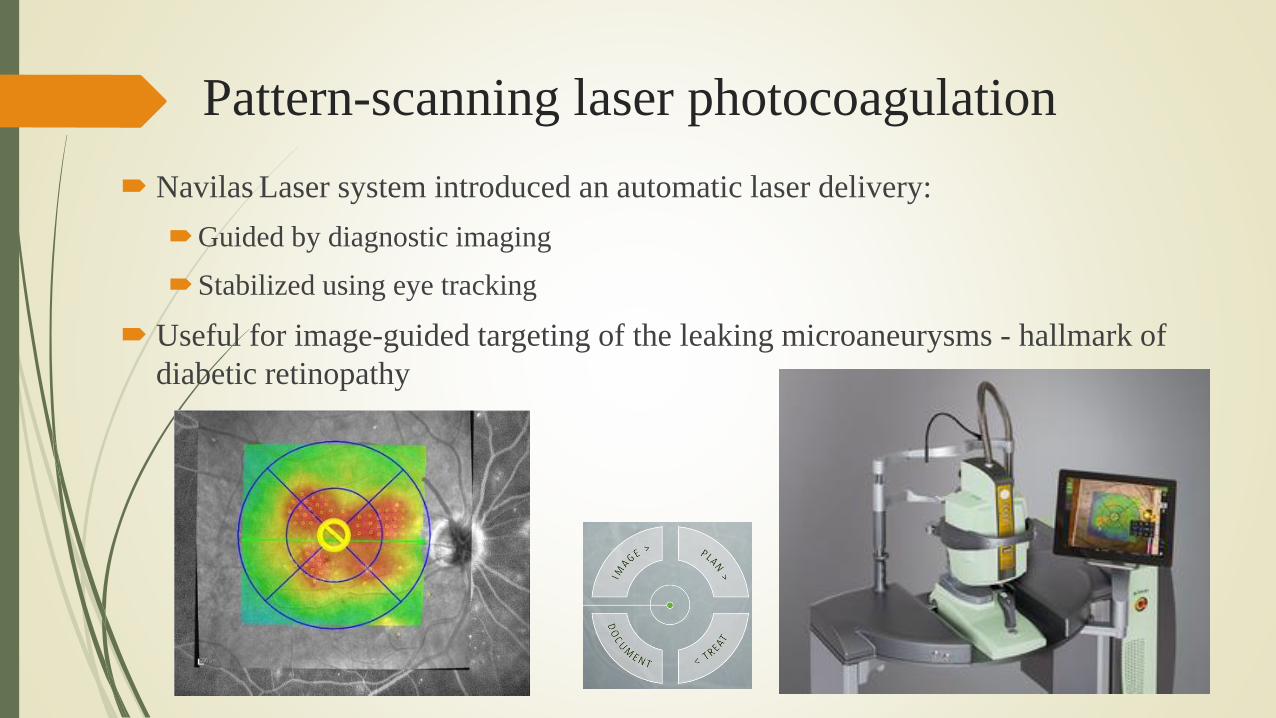
Pattern-scanning laser photocoagulation
Navilas Laser system introduced an automatic laser delivery:
Guided by diagnostic imaging
Stabilized using eye tracking
Useful for image-guided targeting of the leaking microaneurysms - hallmark of
diabetic retinopathy
Nondamaging Laser Therapy of the Macula
Intense photocoagulation outcome:
Destroys the invading vasculature
Leaves a chorioretinal scar -> blind spot (scotoma).
Reichel (1999) attemped to make the nondamaging approach to retinal laser
therapy
Using near-infrared diode laser (810 nm)
Very long exposures (60 s)
A millimeter-wide spot on the retina
Hypothesis: a selective damaging effect of heating on actively dividing cells
in newly formed blood vessels owing to their higher susceptibility to thermal
injury than nondividing cells have in normal tissue.
Difficulties with reliable titration -> frequent occurrences of significant
retinal damage (Benner et al. 2002).
Nondamaging Laser Therapy of the Macula
Nondamaging retinal therapy: using a pulsed version of near-infrared diode laser
(micropulse laser )
Smaller spot size (125 μm) was applied to.
100–300-ms long bursts composed of 0.1- to 0.3-ms pulses
Repeated at a 500-Hz rate.
Sivaprasad (2010) showed significant advantages of the nondamaging retinal
phototherapy
The absence of scotomata and scarring,
The ability to treat foveal areas, and
Improved preservation of color vision and contrast sensitivity.
Nondamaging Laser Therapy of the Macula
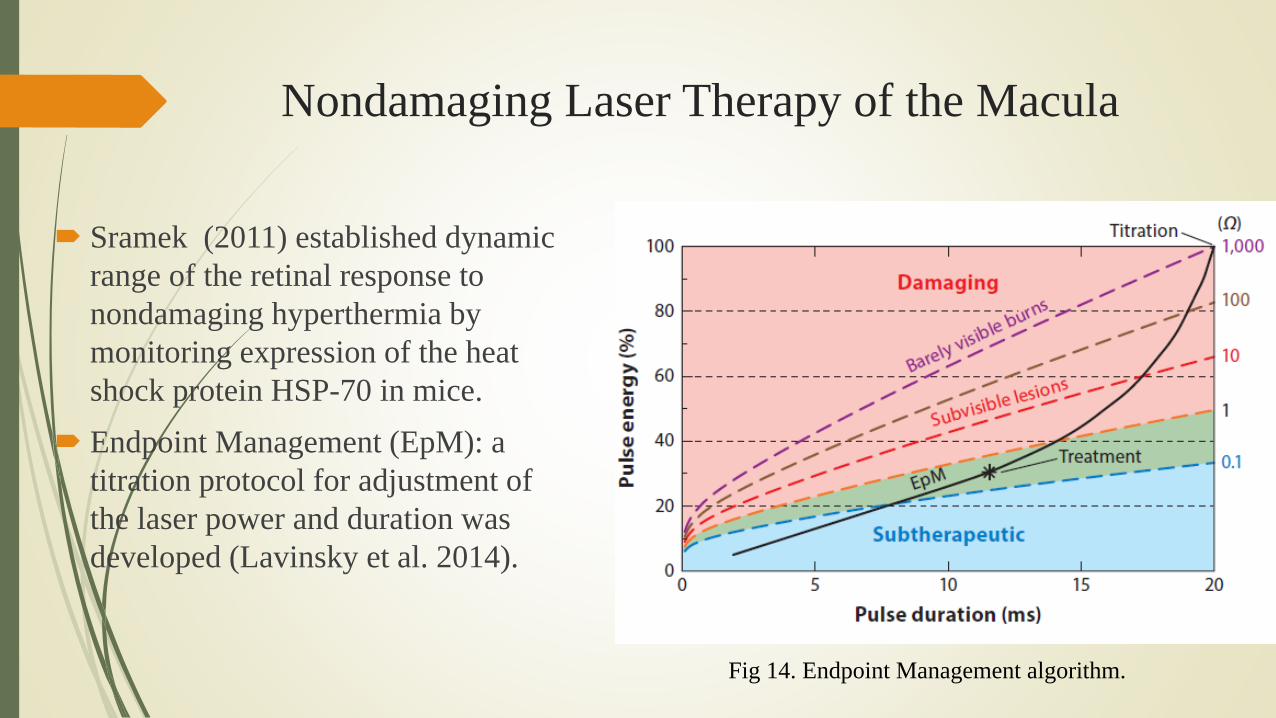
Sramek (2011) established dynamic
range of the retinal response to
nondamaging hyperthermia by
monitoring expression of the heat
shock protein HSP-70 in mice.
Endpoint Management (EpM): a
titration protocol for adjustment of
the laser power and duration was
developed (Lavinsky et al. 2014).
Fig 14. Endpoint Management algorithm.

Nondamaging Laser Therapy of the Macula
Fig. 15. Resolution of subretinal fluid in a patient with chronic central serous chorioretinopathy after nondamaging retinal laser
therapy. Approximately 400 spots have been applied at 30% Endpoint Management energy, and no tissue damage has been detected
during the 12-month follow-up. Figure adapted from Lavinsky & Palanker (2015).

Patterned laser trabeculoplasty
Computer guides patterns
Dense coverage of TM with 5-ms-long subvisible
exposures - a strategy similar to the nondamaging
retinal laser therapy.
Laser power is titrated to a barely visible burn in the
area of highest pigmentation (the inferior segment)
using 10-ms pulses,
Pulse duration is decreased by half to reduce the
energy below the visible damage threshold.

Patterned laser trabeculoplasty
Reduction in IOP following this treatment (∼25%) was similar to the results of ALT
(Turati et al. 2010) and, owing to lack of tissue scarring, it allows periodic retreatments.
PHOTOCHEMICAL INTERACTIONS:
PHOTODYNAMIC THERAPY
Photochemical interactions: based on nonthermal light-
induced chemical reactions.
PDT is performed at very low power densities (typically
<1W/cm2) and using minute-long exposures.
This differential accumulation is the basis for selectivity
of PDT against neovascularization, compared with the
normal choroidal and retinal vasculature

PHOTOCHEMICAL INTERACTIONS:
PHOTODYNAMIC THERAPY
The far-red peak (688–691 nm) of the verteporfin absorption spectrum is typically
utilized in clinical practice because of the lower retinal sensitivity and its superior
penetration into the choroid (Woodburn et al. 2002).
Schmidt-Erfurth (1994) showed closure of the abnormal blood vessels occurs within
approximately 6-12 weeks inmost patients
Reperfusion is common, and multiple treatments are often required.
Since the recent advent of anti-vascular endothelial growth factor pharmacotherapy,
which has proven to be much more efficient in the prevention of neovascularization,
PDT has fallen out of favor (Oh & Yu 2015).

PHOTOMECHANICAL INTERACTIONS
Vapor bubbles produced when tissue temperature exceeds the
vaporization threshold may rupture cells within a zone comparable
to the bubble size.
Temperature for vaporization:100 - 305◦C, depending on pulse
duration and on the presence of the bubble nucleation sites
(Vogel&Venugopalan 2003).
For efficient heating, the energy should be delivered fast enough to
avoid heat diffusion during the pulse, a condition called thermal
confinement.

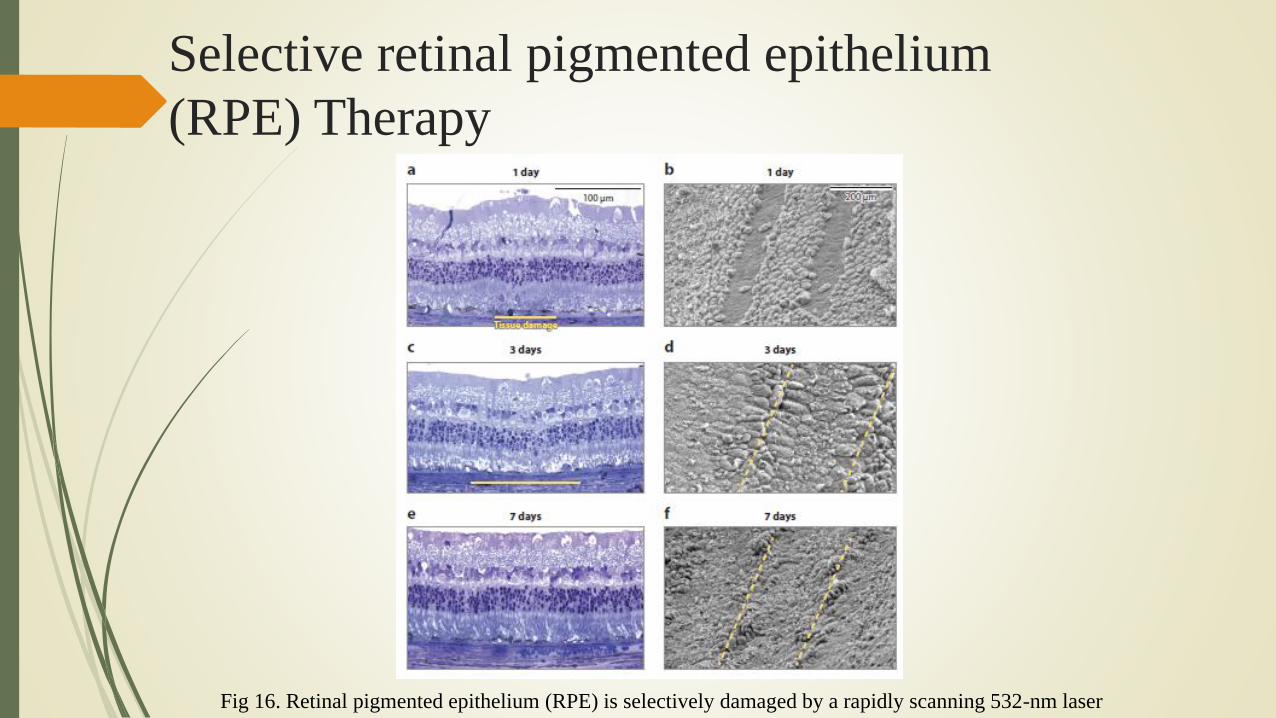
Selective retinal pigmented epithelium
(RPE) Therapy
Light is strongly absorbed by melanosomes in the RPE (μa ≈8,000
cm−1) (Brinkmann et al. 2000).
Application of microsecond laser pulses allows for confinement of
the thermal and mechanical effects of this absorption within the RPE
layer, thus sparing the photoreceptors and the inner retina (Roider et
al. 1992, 1993).
Microsecond and nanosecond pulses can selectively damage RPE by
formation of small cavitation bubbles around melanosomes (Schuele
et al. 2005).
Selective retinal pigmented epithelium
(RPE) Therapy
Fig 16. Retinal pigmented epithelium (RPE) is selectively damaged by a rapidly scanning 532-nm laser
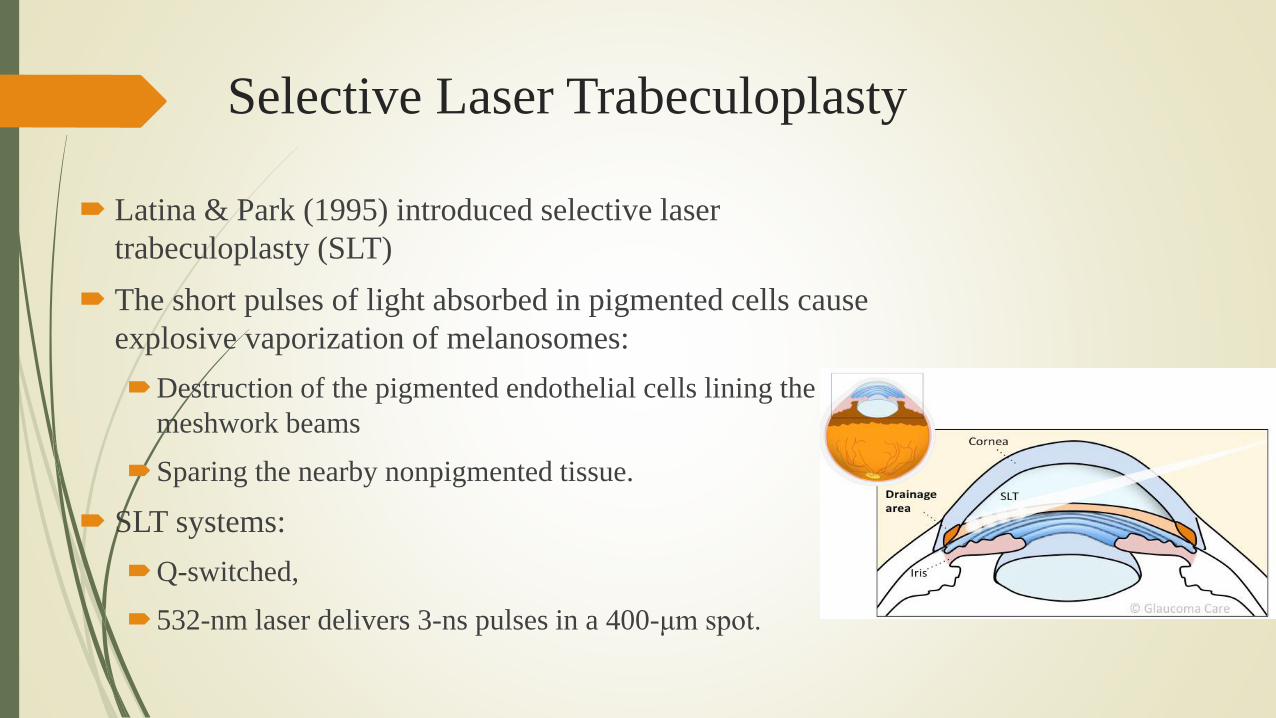
Selective Laser Trabeculoplasty
Latina & Park (1995) introduced selective laser
trabeculoplasty (SLT)
The short pulses of light absorbed in pigmented cells cause
explosive vaporization of melanosomes:
Destruction of the pigmented endothelial cells lining the
meshwork beams
Sparing the nearby nonpigmented tissue.
SLT systems:
Q-switched,
532-nm laser delivers 3-ns pulses in a 400-μm spot.

Selective Laser Trabeculoplasty
Hypothesis:
Remove clogging the TM
Improved permeability to aqueous outflow,
Leading to reduction of IOP.
Latina (1998), Melamed (2003), Nagar (2005)
shown effeciency of SLT in treatment of open angle
glaucoma
Improve permeability of TM to aqueous flow
Without destruction of its microstructure.

Selective Laser Trabeculoplasty
The IOP-lowering effect of SLT lasts for several years, but it also diminishes over
time.
Lack of scarring in SLT allows retreatment.
.

REFRACTIVE SURGERY
Lendeer Jans Lans (1896) published the first ideas for reshaping the
cornea to correct refractive errors
Using penetrating corneal cuts to correct astigmatism.
In 1981, Srinivasan and Wynne put turkey cartilage under the laser
beam (193-nm ArF excimer) and observed a beautiful crater formed
by ablation—much cleaner than any other laser they had tested
(Srinivasan et al. 1983).

REFRACTIVE SURGERY
Fig 17. Radial keratotomy Fig 18. Photorefractive keratectomy
Problems of slow and rather uncomfortable recovery of the epithelial layer.

REFRACTIVE SURGERY
Laser-assisted in situ keratomileusis (LASIK)
(Pallikaris et al. 1991).
REFRACTIVE SURGERY
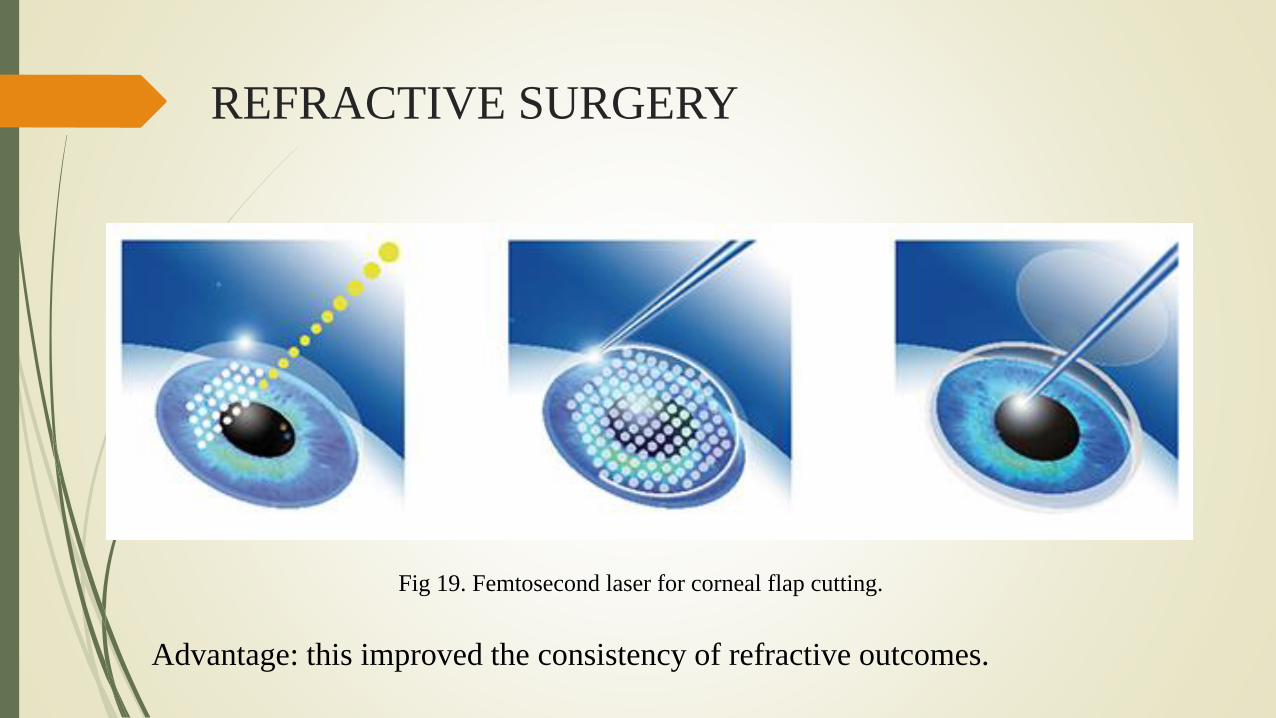
Fig 19. Femtosecond laser for corneal flap cutting.
Advantage: this improved the consistency of refractive outcomes.

TRANSPARENT TISSUE SURGERY WITH
ULTRASHORT - PULSE LASERS
Dielectric breakdown:
Using extremely high irradiances (108–1011 W/cm2), short-pulsed (ns or fs)
tightly focused laser beam (nanosecond Nd:YAG lasers)
Transparent material can be ionized, and ions absorbing the laser light reach very
high temperatures.

Cataract Surgery
Fig 20. Posterior Capsulotomy: using ultrashort-pulse laser

Cataract Surgery
Fig 21. Anterior capsulotomy: Left: system diagram, including the OCT and femtosecond laser combined by a common
scanner. Right: Side and top views of the eye, with overlay of the planned laser patterns.

Cataract Surgery
Fig 22. A scanning femtosecond laser for anterior capsulotomy
References
Daniel Palanker. 2016. Evolution of Concepts and Technologies in Ophthalmic Laser
Therapy, Annu. Rev. Vis. Sci. 2:295–319
http://web.stanford.edu/~palanker/publications/Ophthalmic_Laser_Therapy.pdf
https://en.wikipedia.org/wiki/Retinoblastoma
http://www.summitmedicalgroup.com/library/adult_health/oph_retinal_holes_and_tears/
http://www.slideshare.net/FUTUREDESIGNER/anatomy-of-the-lens-38752158
http://www.selectspecs.com/info/structure-of-the-eye/
https://www.od-os.com/en-US/home/
http://portal.faf.cuni.cz/Groups/Azaphthalocyanine-group/Research-
Projects/Photodynamic-therapy/
Thank you!


Paper: Noninvasive optoacoustic temperature determination at
the fundus of the eye during laser irradiation (Schuele et al. 2004)
Nanosecond laser pulses melanosome thermal
expansion Thermoelastic pressure wave.
Acoustic transducer: detect pressure wave.
Using a constant pulse energy, the amplitude of the
pressure wave increases linearly with an increase in the
base temperature of between 30 and 80°C.
Fig 12. Setup for optoacoustic measurements during selective RPE treatment.
A standard contact lens is modified with a piezoelectric transducer

Paper: Noninvasive optoacoustic temperature
determination at the fundus of the eye during laser
irradiation (Schuele et al. 2004)Sigrist showed that the maximum peak pressure is proportional to the laser intensity I0 and to the Gru¨neisen
parameter Γ under conditions of no acoustic confinement but thermal confinement.For small variations in the
laser intensity I0 , it follows that
For water, Γ increases nearly linearly in the temperature range from 20
to 60°C.Therefore the maximum pressure amplitude emitted after
pulsed heating increases linearly with the base temperature in this
range. A linear approximation (1) leads to
(1)
(2)

Paper: Noninvasive optoacoustic temperature determination at the
fundus of the eye during laser irradiation (Schuele et al. 2004)
B0: determined by the first laser pulse applied, if the start temperature T0 and TRPEp=0 are known.
Applying I0 and measuring P0 max , B0 is given by
T0: the body temperature
(3)

Paper: Noninvasive optoacoustic temperature determination at the
fundus of the eye during laser irradiation (Schuele et al. 2004)
The increase in the baseline temperature at the i’th laser pulse:
(4)
In the case of repetitive laser irradiation with a repetition rate f rep, the baseline temperature of the i’th laser
pulse is determined at time ti = i*1/f rep . The mean temperature achieved by the previous laser pulses sums
to Trep(ti), which is given by

Grüneisen parameter
The Grüneisen parameter, a constitutive parameter in photoacoustics, is usually measured from isobaric
thermal expansion. It tells us how temperature varies
(where β is the isobaric volume expansion coefficient, Cp is the specific heat, vs is the acoustic
speed, κ is the isothermal compressibility, and ρ is the mass density)