lasik what are the limits ? a.marinho,md phd departamento de cirurgia refractiva hospital arrabida -...
TRANSCRIPT

LASIKWhat are the Limits ?
A.Marinho,MD PhD Departamento de Cirurgia RefractivaDepartamento de Cirurgia Refractiva
Hospital Arrabida - Universidade do PortoHospital Arrabida - Universidade do Porto

Corneal Refractive Surgery
LASIK and Surface Ablation are the most widely practiced and “popular” forms of refractive surgery
However, even if perfectly performed,but in a defective indication can lead to catastrophic situations
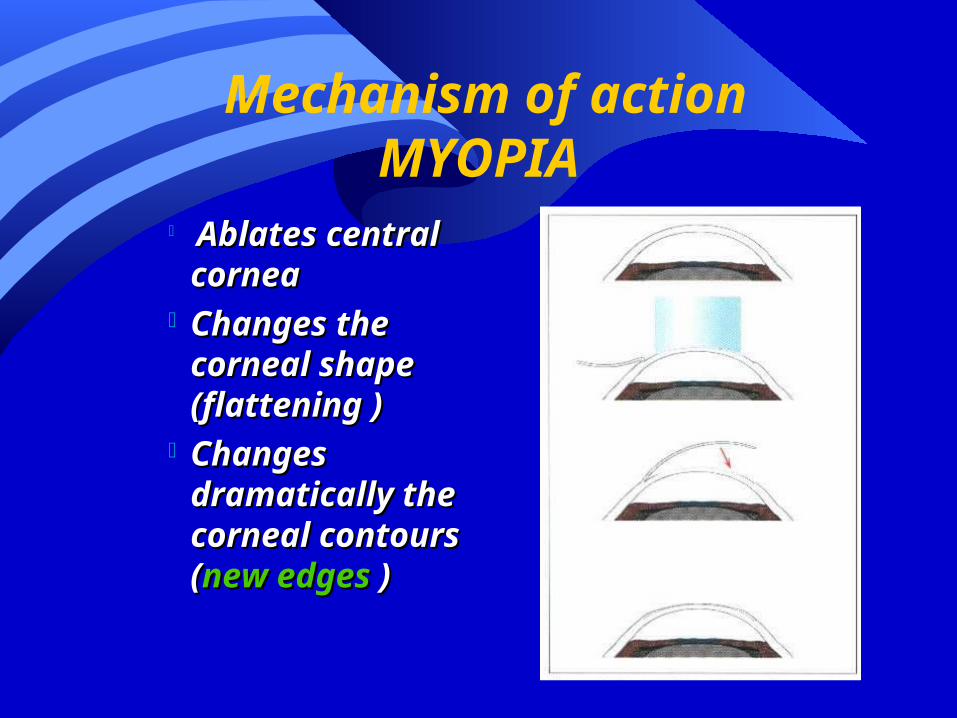
Mechanism of actionMYOPIA
Ablates central Ablates central corneacornea
Changes the Changes the corneal shape corneal shape (flattening(flattening ))
Changes Changes dramatically the dramatically the corneal corneal contours (contours (new new edgesedges ) )
Limits
The normal cornea
Central thickness mean 520 (480 to 600)
Curvature mean 43D (39 to 46)
Aspheric shape with no edges

General limits of corneal refractive surgery
We cannot change the shape and thickness of cornea indefinetely
The early ideas of corrections up to -30.00 proved wrong
Biomechanics of the cornea shows that trying to correct high ametropias lead almost always to important regression and reduced quality of vision
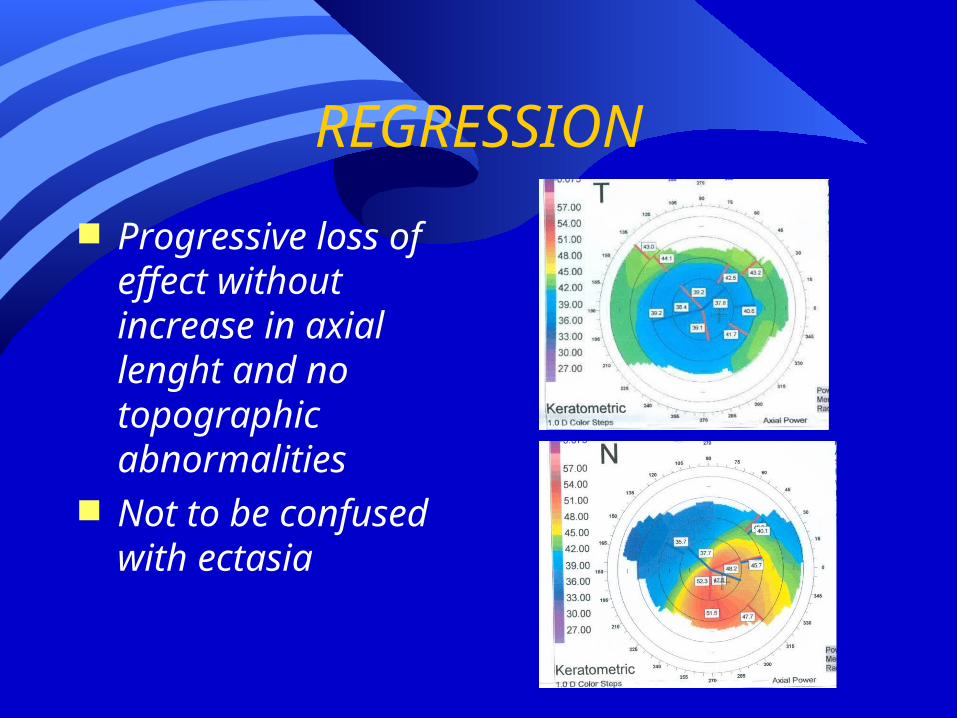
REGRESSION
Progressive loss of effect without increase in axial lenght and no topographic abnormalities
Not to be confused with ectasia

Why Regression ?
Epithelial hyperplasia
Corneal remodeling

Quality of Vision
Excellent quality of vision can only be achieved up to -5.00
Some decrease up to -8.00
Poor in high myopia
General limits of corneal refractive surgery
Most papers dealing with high ametropia surgery have 6 months to 1 year follow-up……
So,in an ideal cornea ,we should not attempt to correct more than:
- 8.00 (S.E.) or +4.00 (SE)
VERY IMPORTANT
Wave front ablations Tissue Saving Nomograms Aspheric Ablations
Improve qualty of vision, BUT DO NOT CHANGE the BASICS of corneal behaviour
Limits of LASIK
In myopias lower than -8.00 or hyperopias > +4.00, the limits are defined by the following:
Corneal Thickness Corneal Curvature Pupil Size
Limits of CRS
Inclusion criteria
Total corneal thickness at least 500 micra(Lasik) (480 micra if using FS flaps)
Stromal bed after ablation must be 250 Final corneal curvature must be between 33
and 47D Full corrected optical zone must be at least
equal to pupil diameter in mesopic conditions (ray tracing methods)
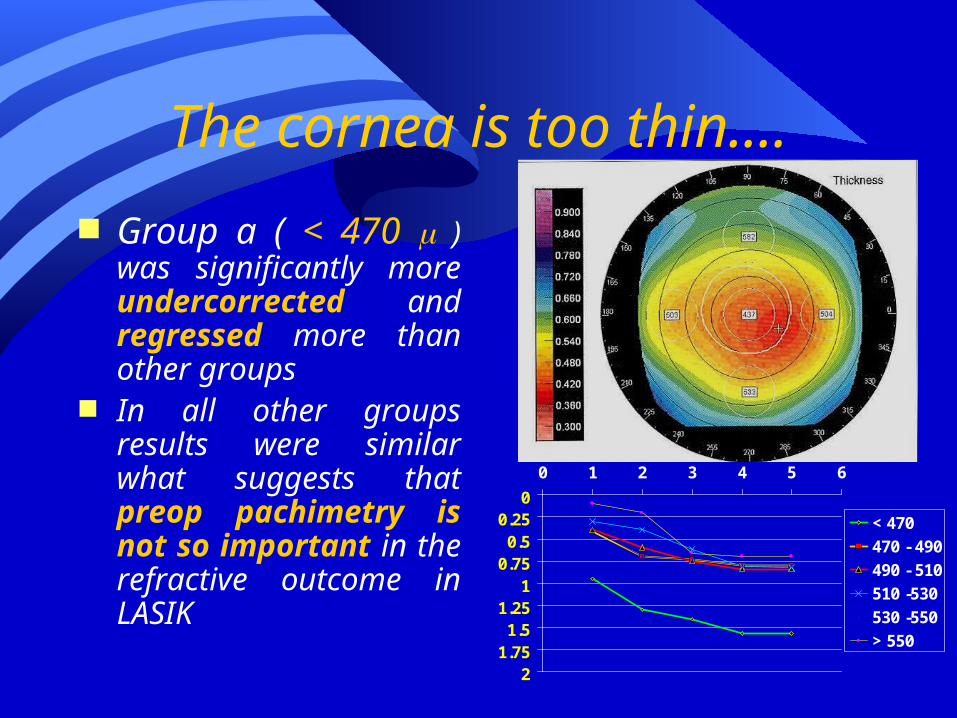
The cornea is too thin....
Group a ( < 470 ) was significantly more undercorrected and regressed more than other groups
In all other groups results were similar what suggests that preop pachimetry is not so important in the refractive outcome in LASIK
00.250.5
0.751
1.251.5
1.752
0 1 2 3 4 5 6
< 470
470 - 490
490 - 510
510 -530
530 -550
> 550

The cornea is too flat...
Group c ( K < 34 )
– 10 eyes
– Myopia: - 8.81 + 1.84
Group d ( K > 34 ) – 20 eyes – Myopia: - 7.14 + 1.43
11,151,3
1,451,6
1,751,9
2,052,2
2,352,5
2,65
D C
Log CS

Pupil Size
Pupil size is important and sometimes overlooked
Lasik full corrected optical zone must be at least equal to the mesopic pupil
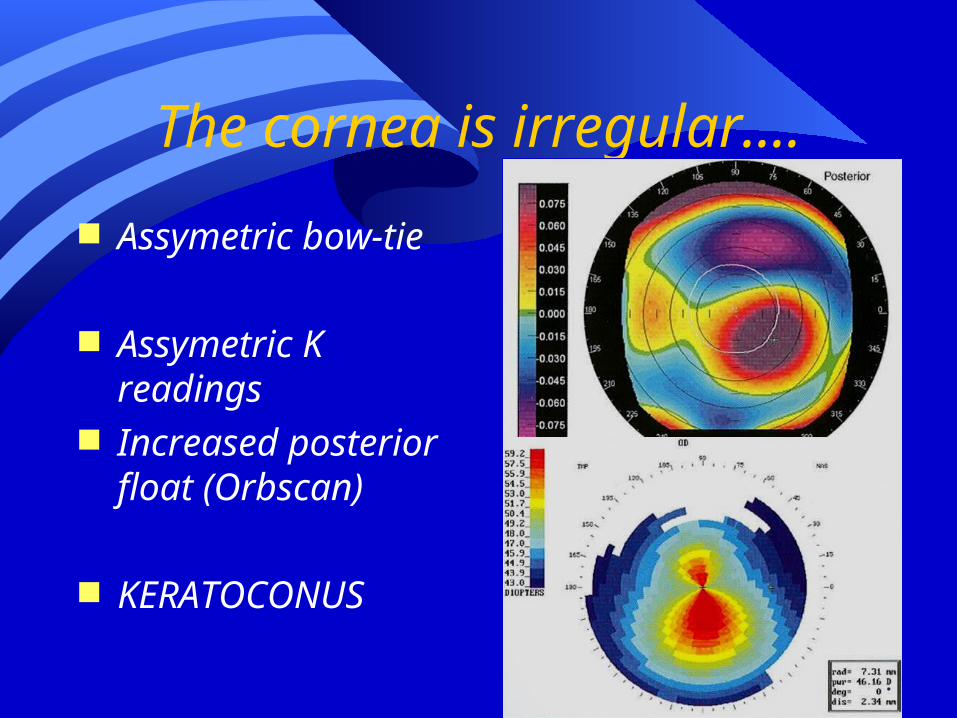
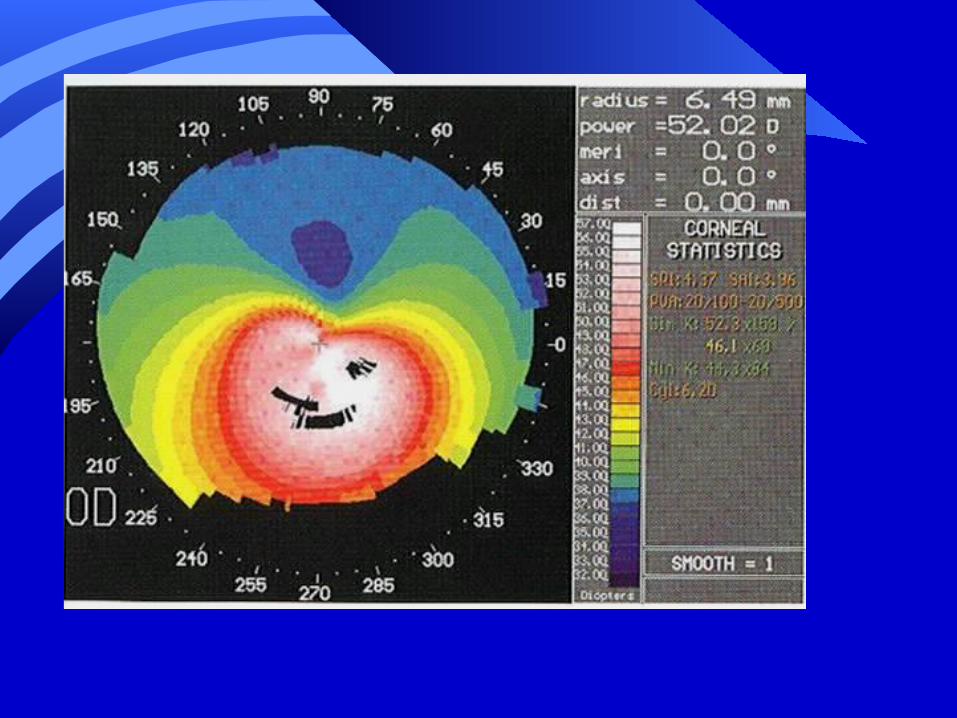
The cornea is irregular....
Assymetric bow-tie
Assymetric K readings
Increased posterior float (Orbscan)
KERATOCONUS

Limits of LASIK
Inclusion criteria Example
Refraction - 7.00– Case 1
Pachymetry 580 K readings 45 D Pupil size 4.0mm
– Case 2 Pachymetry 490 K readings 40 D Pupil size 6.5mm
GOOD
BAD

Limits of LASIK
Inclusion criteria
Failure to follow these guidelines lead to irreversible complications
corneal ectasia loss of lines of BCVA ( typical of high myopia
and mainly in hyperopia ) severe glare and halos
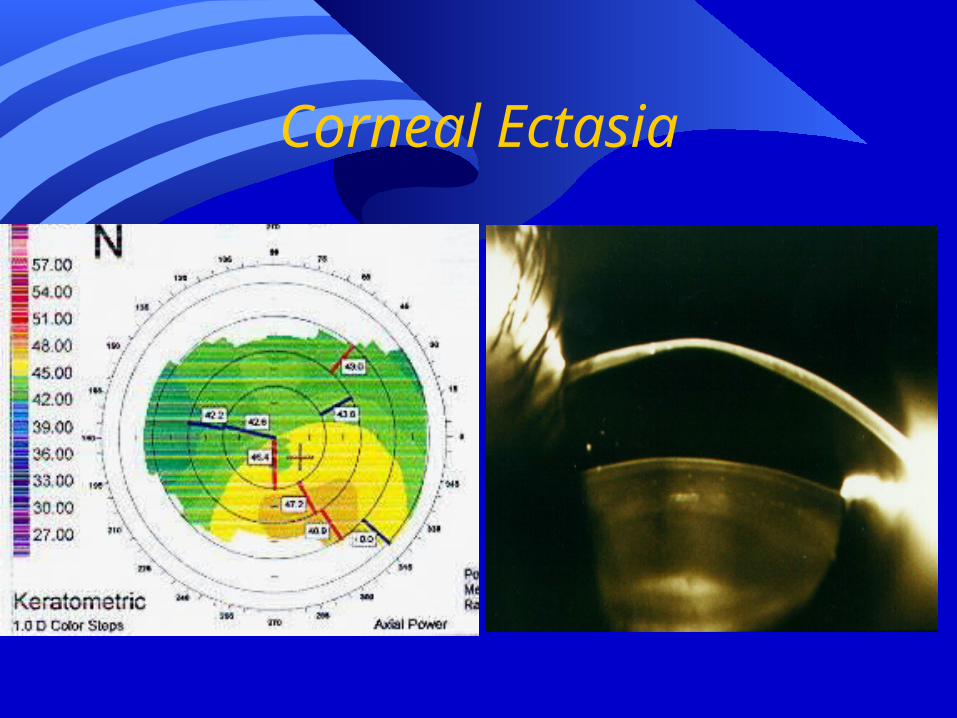
Corneal Ectasia

LASIK IN HIGH AMETROPIA
Deep ablation – Thin cornea– Unstable cornea---Regression (ectasia)
Small optical zone---glare and halos-low mesopic vision
Flattened (or steepned)cornea---distorted vision—loss of lines of BCVA—low mesopic vision
Lasik in high ametropia---an unfulllfilled promise
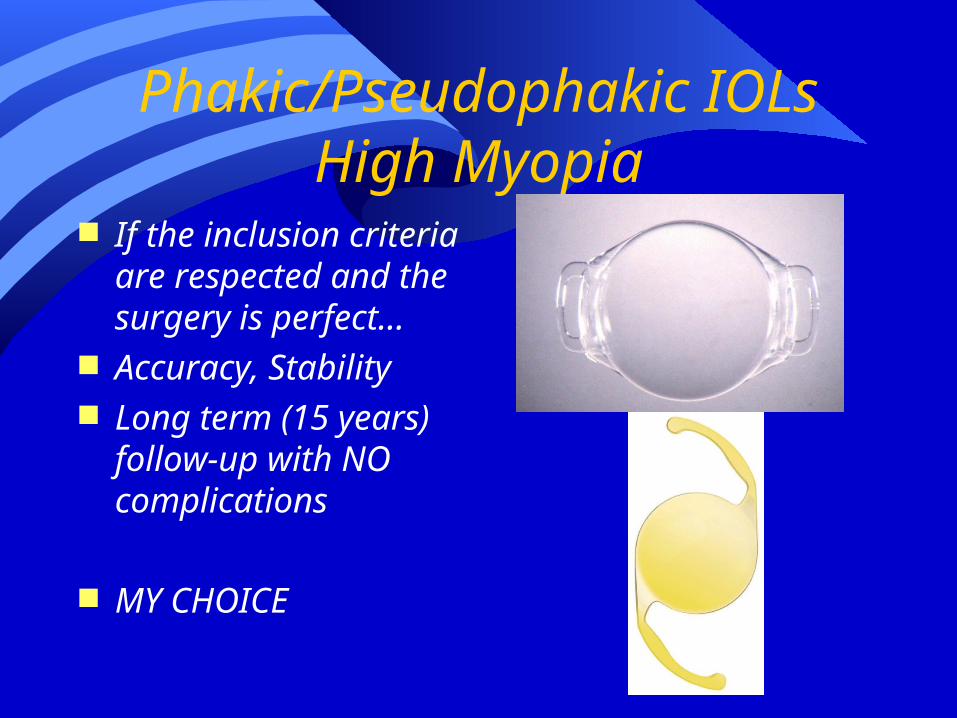
Phakic/Pseudophakic IOLs High Myopia
If the inclusion criteria are respected and the surgery is perfect…
Accuracy, Stability Long term (15 years)
follow-up with NO complications
MY CHOICE
Conclusions
Limits (Absolute and Particular) of Lasik must be respected
Selection of patients is the key for success
Classicaly Lasik : 80% MK 20% Laser Today: 50% Selection 50% Surgery