latent acidosis as a cause of chronic disases - vivalis
TRANSCRIPT

Acid-Base Homeostasis:Latent Acidosis as a Cause of Chronic DiseasesLatest findings on the beneficial disease-modifying aspects of an adequate dietary base supply
Jürgen Vormann, Thomas Goedecke
Institut für Prävention und Ernährung, DE-Ismaning
In the healthy human being, the bloodhas a pH value of 7.4. Even slight
deviations from this value may lead tosevere disturbances in metabolismwhich may even be life-threatening. Itis for this reason that the body`s exten-sive buffer systems ensure that theblood pH is maintained between thevery narrow limits of 7.37 and 7.43.These buffer systems bind and neu-tralize the additional protons (H+ ions)or hydroxide ions (OH– ions) respec-tively associated with excessive acidityor alkalinity and thereby prevent themfrom immediate and marked influ-ences on metabolism. In order tomaintain the optimal metabolic func-tioning and therefore the bufferingcapacity on a long-term basis, theorganism is also dependent on the con-stant regeneration of the buffer sys-tems.
Physiological regulation ofacid–base homeostasis
What has been said above presuppos-es precise regulation of the acid–basehomeostasis which involves many fac-tors (Fig. 1). Apart from the bufferingcharacteristics of the blood and theextracellular and intracellular com-partments, the gas exchange in thelungs and the excretion mechanisms ofthe kidneys are essential componentsof this regulatory system all of whichare in functional equilibrium witheach other. The bicarbonate system isof primary importance for maintaininga constant blood pH, but plasma pro-teins as well as the hemoglobin andthe phosphate buffer also play a role
Background: A prerequisite for the proper functioning of the enzyme-controlled meta-bolic processes of the human organism is the regulation of pH both inside and outsideof the cells. The ratio of acids to bases is not only important for a healthy metabolism,it also determines the structure and function of proteins, the permeability of cell mem-branes, the distribution of electrolytes, and the function of connective tissue.Currently, long-term disturbances of the natural acid–base homeostasis are receivingincreasing attention as risk factor for chronic diseases. Objective: To determinewhether there is causal evidence for the pathobiochemical effects of a low-gradechronic metabolic (latent) acidosis and the beneficial disease-modifying aspects of awell-balanced acid-base homeostasis. Methods: The recent scientific literature onlatent acidosis and its impact on human health is systematically reviewed. Results: Alatent acidosis resulting from a gradual reduction of the buffer reserves, mainly due tonutritional influences, does not produce major changes of blood pH because of com-pensatory mechanisms through urinary acid excretion. However, there is causal evi-dence that this compensation, in the long term, inevitably leads to loss of bone sub-stance and impairs the structure and function of the connective tissue. Conclusion: Inthe past, the pH regulation was taken for granted in persons not being severely ill andthe required buffering capacity of the organism was accepted as being virtually inex-haustible. But today latent acidosis resulting from a gradual reduction of the bufferreserves is increasingly in the focus of interest for the development and progressionof chronic diseases such as osteoporosis and rheumatoid disorders.
Key Words: Acid-base homeostasis, latent acidosis, osteoporosis, rheumatoid disor-ders, nutrition, evolution
Säure-Basen-Haushalt:Latente Azidose als Ursache chronischer Erkrankungen
Aktuelle Erkenntnisse über die positiven gesundheitlichen Aspekte einer ausrei-chenden Basenzufuhr
Hintergrund: Die Regulation des pH-Wertes innerhalb und außerhalb der Zellen isteine wesentliche Vorraussetzung für die Funktionsfähigkeit der enzymatisch gesteuer-ten Stoffwechselvorgänge unseres Organismus. Das Verhältnis von Säuren zu Basenist nicht nur für einen gesunden Stoffwechsel von Bedeutung, sondern entscheidetauch über die Struktur und Funktion von Proteinen, die Permeabilität von Zellmembra-nen, die Verteilung von Elektrolyten sowie die Funktion des Bindegewebes. Langfri-stige Störungen des natürlichen Säure-Basen-Gleichgewichtes finden aufgrund des ge-genwärtigen wissenschaftlichen Erkenntnisstandes als Risikofaktor für chronische Er-krankungen zunehmend Beachtung. Fragestellung: Lassen sich die pathobiochemi-schen Auswirkungen einer geringgradigen chronischen metabolischen (latenten) Azi-dose und die positiven gesundheitlichen Aspekte eines ausgeglichenen Säure-Basen-Haushalts kausal belegen? Methoden: Systematische Auswertung der wissenschaft-lichen Literatur über die latente Azidose und deren Einfluss auf die Gesundheit. Ergebnisse: Eine latente Azidose als Folge einer schleichenden Verminderung der Puf-ferreserven, überwiegend bedingt durch Ernährungseinflüsse, ruft aufgrund der Kom-pensation durch die Säureausscheidung über die Nieren keine wesentlichen Verände-rungen des Blut-pH hervor. Allerdings führt diese Kompensation auf lange Sicht unaus-
Schweiz. Zschr. GanzheitsMedizin Jg.18, Heft 5, September 2006
Schweiz. Zschr. GanzheitsMedizin 18, ...–... (2006). © Verlag für GanzheitsMedizin, Basel. www.ganzheitsmedizin.ch
Übersichtsarbeiten � Review Articles

as H+ or OH– scavengers. The highlyrapid responsiveness of the buffer sys-tems produces an extremely fast andconstant regulation of the blood pH.
Apart from water, transient carbondioxide – the intermediate productfrom the protonation of bicarbonate(HCO3
–) – is produced by the dissocia-tion of carbonic acid; it is expired viathe lungs and, as a result, H+ ions areeffectively eliminated. However, sinceHCO3
– is also removed at the sametime, net acid excretion does not takeplace. Even though acute acidosis canusually be avoided by carbon dioxideexpiration, the buffer systems of thekidneys are primarily responsible forthe net excretion of the H+ ionsreleased from the breakdown of variousacids.
This excretion is necessary becausethe production of protons (e.g. viametabolizing sulphur-containing aminoacids from protein) from a normalmixed diet exceeds the absorption ofalkaline substances. In the moderndiet, mainly the proportionately highconsumption of protein compared withthat of base-supplying fruit and veg-etables contributes to the daily acidifi-cation of the body. A particular exam-ple of acidification is that from imbib-ing phosphoric acid-containing bever-ages. Fasting (i.e. reducing body weightby not eating) increases the acidifica-tion of the body via the increased for-mation of keto acids from the break-down of fatty acids, and so does theincreased production of lactic acidunder anaerobic conditions as the endproduct of glycolysis during sportsactivities.
With regard to the buffering of H+
ions, of major importance are thosealkaline vegetable substances in theform of metabolizable organic anionsthat can neutralize the acid producedfrom protein metabolism. During the
dissociation of these salts, organicanions are released which can then –depending on the dissociation constantof the acid group – accept H+ ions. Theorganic acids produced are neutrallymetabolized to water and carbon diox-ide (CO2) and ensure in this way thatprotons are eliminated from theorganism. As is shown for the exampleof sodium citrate (Fig. 2), the remain-
ing cations (e.g. Na+) are available forreabsorption from the primary urinein the kidney in exchange for H+ ions.By this means, the charge neutrality ismaintained and acid is eliminatedfrom the body. It can thus be seen thatthe level of intake of organic anionsrepresents a major factor in regulatingacid–base homeostasis.
Definition of latent acidosisand its manifestations
Compared with the clinically ratherrare manifestation respiratory or meta-bolic acidosis, which is characterizedby a decrease in the blood pH, latentacidosis is much more commonly
Schweiz. Zschr. GanzheitsMedizin Jg.18, Heft 5, September 2006
Übersichtsarbeiten � Review Articles
Fig. 1. Regulation of the acid–base homeostasis.
Fig. 2. Function of organically bound minerals in the elimination of acids as shown forthe example of sodium citrate.
weichlich zu einem Verlust von Knochensubstanz und beeinträchtigt die Struktur undFunktion des Bindegewebes. Schlussfolgerung: In der Vergangenheit wurde die pH-Regulation bei Personen, die nicht ernsthaft erkrankt sind, als Selbstverständlichkeitaufgefasst und die hierzu erforderliche Pufferkapazität des Organismus als beinahe un-erschöpflich erachtet. Heute wird zunehmend erkannt, dass die latente Azidose alsFolge einer allmählichen Abnahme der Pufferreserven für die Entstehung und den Ver-lauf chronischer Erkrankungen wie z.B. Osteoporose und Rheuma von Bedeutung ist.
Schlüsselwörter: Säure-Basen-Haushalt, latente Azidose, Osteoporose, rheumatischeErkrankungen, Ernährung, Evolution
observed. In most cases, there is aslight shift of the blood pH in the aciddirection within the normal range andthe total buffering capacity of theblood is reduced. The term “latent”refers to a chronic condition which iswithout acute symptoms and is clini-cally detectable only by determiningthe intracellular and extracellularbuffer capacity and the renal net acidexcretion.
It is mentioned here that latent aci-dosis affects a wide cross-section ofthe population. The cause of increasedacidification is, above all, the high pro-tein content in food which, when cou-pled with the declining renal functionassociated with increasing age, leadsto latent acidosis [1]. With increasingage, the ability of the kidneys to excreteacids progressively decreases [2, 3]. Asis shown in Fig. 3, the blood pHdeclines within the normal range overthe years, but at the same time theconcentration of plasma bicarbonatebuffer bases also decreases.
This in turn not only results in an
increased consumption of bufferingminerals from the bone reservoir, butalso in detrimental effects on variousmetabolic functions such as theincreased muscle breakdown which isfrequently observed in senior citizens[3]. The age-related renal functionaldecline together with a constantlyhigh protein intake exacerbates latentacidosis and its harmful influences onhealth.
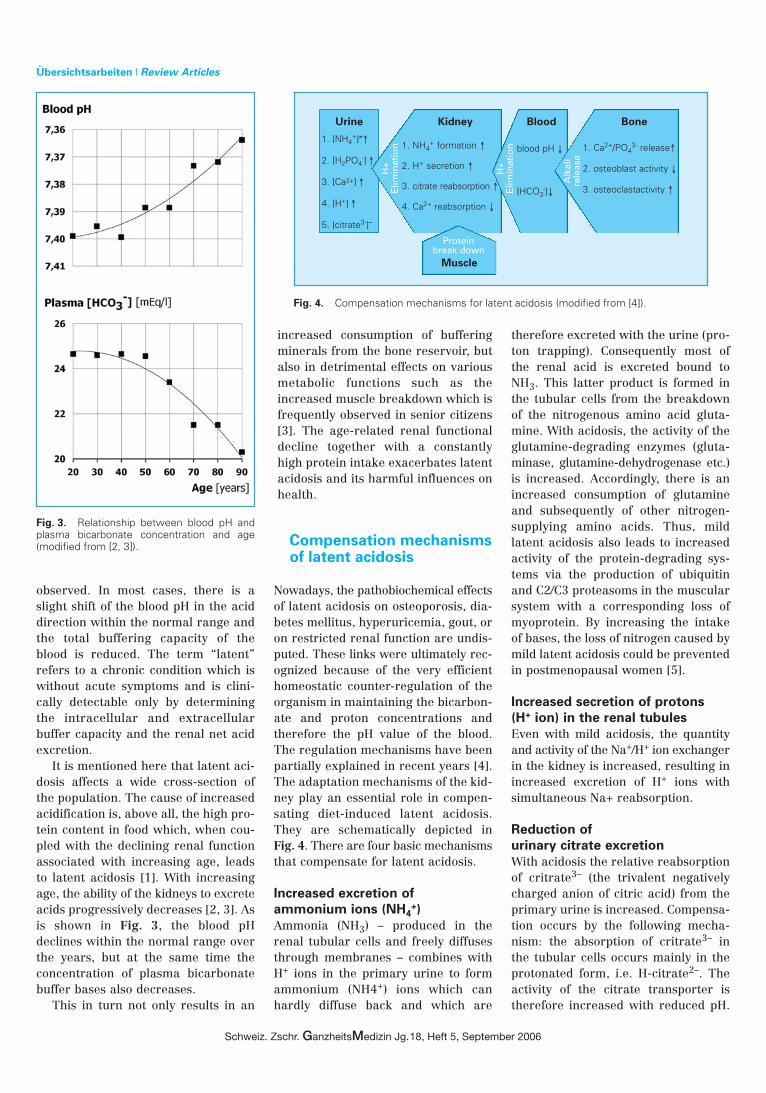
Compensation mechanismsof latent acidosis
Nowadays, the pathobiochemical effectsof latent acidosis on osteoporosis, dia-betes mellitus, hyperuricemia, gout, oron restricted renal function are undis-puted. These links were ultimately rec-ognized because of the very efficienthomeostatic counter-regulation of theorganism in maintaining the bicarbon-ate and proton concentrations andtherefore the pH value of the blood.The regulation mechanisms have beenpartially explained in recent years [4].The adaptation mechanisms of the kid-ney play an essential role in compen-sating diet-induced latent acidosis.They are schematically depicted in Fig. 4. There are four basic mechanismsthat compensate for latent acidosis.
Increased excretion of
ammonium ions (NH4+)
Ammonia (NH3) – produced in therenal tubular cells and freely diffusesthrough membranes – combines withH+ ions in the primary urine to formammonium (NH4+) ions which canhardly diffuse back and which are
therefore excreted with the urine (pro-ton trapping). Consequently most ofthe renal acid is excreted bound toNH3. This latter product is formed inthe tubular cells from the breakdownof the nitrogenous amino acid gluta-mine. With acidosis, the activity of theglutamine-degrading enzymes (gluta-minase, glutamine-dehydrogenase etc.)is increased. Accordingly, there is anincreased consumption of glutamineand subsequently of other nitrogen-supplying amino acids. Thus, mildlatent acidosis also leads to increasedactivity of the protein-degrading sys-tems via the production of ubiquitinand C2/C3 proteasoms in the muscularsystem with a corresponding loss ofmyoprotein. By increasing the intakeof bases, the loss of nitrogen caused bymild latent acidosis could be preventedin postmenopausal women [5].
Increased secretion of protons
(H+ ion) in the renal tubules
Even with mild acidosis, the quantityand activity of the Na+/H+ ion exchangerin the kidney is increased, resulting inincreased excretion of H+ ions withsimultaneous Na+ reabsorption.
Reduction of
urinary citrate excretion
With acidosis the relative reabsorptionof critrate3– (the trivalent negativelycharged anion of citric acid) from theprimary urine is increased. Compensa-tion occurs by the following mecha-nism: the absorption of critrate3– inthe tubular cells occurs mainly in theprotonated form, i.e. H-citrate2–. Theactivity of the citrate transporter istherefore increased with reduced pH.
Schweiz. Zschr. GanzheitsMedizin Jg.18, Heft 5, September 2006
Übersichtsarbeiten � Review Articles
Fig. 3. Relationship between blood pH andplasma bicarbonate concentration and age(modified from [2, 3]).
Fig. 4. Compensation mechanisms for latent acidosis (modified from [4]).
Urine Kidney Blood Bone
1. NH4+ formation ↑
2. H+ secretion ↑
3. citrate reabsorption ↑
4. Ca2+ reabsorption ↓
1. [NH4+]≠↑
2. [H2PO4-] ↑
3. [Ca2+] ↑
4. [H+] ↑
5. [citrate3-]–
1. Ca2+/PO43- release↑
2. osteoblast activity ↓
3. osteoclastactivity ↑
blood pH ↓
[HCO3-]↓
H+
Elim
inat
ion
Proteinbreak down
H+
Elim
inat
ion
Alk
ali
rele
ase
Muscle

Intracellularly, critrate3– is convertedby the acceptance of additional pro-tons to uncharged citric acid, which isthen pH-neutrally broken down intocarbon dioxide and water. By theabsorption of one molecule of citrate3–
from the primary urine, 3 H+ ions cantherefore be eliminated. As a result,the concentration of citrate in the pri-mary urine decreases (see Fig. 4).However, citrate is essential for com-plexing calcium ions (Ca2
+). The lackof formation of soluble calcium-cit-rate-complexes increases the urinaryconcentration of free Ca2
+ ions andtherefore the availability of calcium toform renal calculi, e.g. with oxalic acid.
Increased release of minerals
from the bones
On the one hand, mild acidosis leads tothe removal of minerals from the bonematrix; on the other hand, acidosisresults in an increase in the activity ofthe bone-decomposing osteoclasts andinhibition of the activity of the bone-forming osteoblasts (see Fig. 10). All inall, increased renal excretion of Ca2
+
ions takes place with the consequenceof the increased risk of formation ofrenal calculi, as described above.
Effects of latent acidosis on calcium and bone metabolism
Epidemiology and
dietary implications
With experimental acidosis, first areduction of the blood buffering capac-ity occurs, then, with further increaseof acid load a reduction of the intracel-lular buffering capacity and a strain onthe buffering capacity of bone occurs.And finally, with increasing acid loadbuffering is achieved by the release ofminerals from bone [6]. This and com-parable investigations led already inthe sixties to the hypothesis, that oneof the significant causes of osteoporo-sis is a high dietary acid load [7].
Numerous epidemiological studiesare available on the obvious relation-ship between the type of diet and thedevelopment of osteoporosis. Theinfluence of a vegetarian diet on bonemineral density is based on the signif-
icant effect of dietary content of acidand base: a higher base content is cor-related with a higher bone mineraldensity [8]. A comparative study onomnivorous and vegetarian women [9]showed that a high proportion of basegenerating foodstuffs leads to a clearlyimproved calcium balance in vegetari-ans. In spite of equal calcium intake inboth groups, the women who ate amixed diet showed not only a signifi-cantly higher excretion of acid but alsoa significantly higher excretion of cal-cium. For premenopausal women acorrelation was shown between theintake of alkaline foods and bone min-eral density [10]. Although the intakealkaline food components (especiallypotassium and magnesium) and thehigh consumption of fruit and vegeta-bles were correlated with an increasedbone mineral density in a study onelderly subjects, this was not the casefor the calcium content of the con-sumed food [11]. No associations withother food components , e.g. the cal-cium intake or the total caloric intake,
were found in this study. Recent epidemiological studies on
the nutritional effects on bone lossduring menopausal transition demon-strated that with decreasing endoge-nous acid production femoral bonemineral density of pre- and perimeno-pausal women significantly increased[12], see Fig. 5.
Another epidemiological studyshowed the beneficial effect of cal-cium, alcohol, and fruit and vegetableintake and the detrimental effect offatty acids. The authors conclude thatalthough menopausal status and hor-mone replacement therapy dominatewomen's bone health, diet may influ-ence early postmenopausal bone losswith fruit and vegetable intake pro-tecting against premenopausal boneloss [13]. These findings are confirmedby the results of a study which investi-gated the relationship between dietarypotassium and protein intake, netendogenous acid production andpotential renal acid load and markersof bone health. Low dietary potassium
Schweiz. Zschr. GanzheitsMedizin Jg.18, Heft 5, September 2006
Übersichtsarbeiten � Review Articles
Fig. 5. Mean (± SEM) bone mineral density of pre- and perimenopausal women byquartile of net endogenous non-carbonic acid production (NEAP). *Significantly differentfrom quartile 4, p<0.04. Modified from [12].

intakes and high dietary estimates ofnet endogenous acid production werefound to be associated with low bonemineral density at the femoral neckand lumbar spine in premenopausalwomen (Fig. 6) and increased markersof bone resorption in post-menopausalwomen [14].
On the whole, the epidemiologicaldata indicate a correlation of theintake of alkaline acting-substancesfrom fruits and vegetables and the cor-responding dietary acid load over theyears and their effects on calcium andbone metabolism from the viewpoint ofosteoporosis.
Confirmation
by intervention studies
Intervention studies largely confirmthe physiological effects of latent aci-dosis. In animal experiments it wasshown that due solely to a high-proteindiet, the bone formation in young ratswas impaired [15]. Another study (seeFig. 7) shows that an excess acid loadwas artificially caused by an increase
of the protein intake [16]. As expected,increased renal net acid excretion (asthe sum of ammonium and titratableacids) and calcium excretion were firstobserved. However, because of theconcomitant intake of sodium bicar-bonate as a base supplier, a negativecalcium balance could be preventedand the protein-induced over-acidifi-cation of the organism was neutral-ized. The positive effects of a highintake of base-forming substancescould also be proved in interventionstudies with postmenopausal women:increased alkaline intake broughtabout both a reduction in the break-down of bone and an increase in boneformation [17]. Thanks to a reductionof the protein intake, the calciumexcretion and therefore the risk ofrenal calculi could be reduced inhypercalciuric patients [18]. In aplacebo-controlled study comparingtreatment with alkaline minerals to aplacebo group for almost all syn-dromes involving the gastrointestinaltract, musculoskeletal system, cardio-
vascular system, skin, and a tendencyto become easily exhausted, a consid-erable improvement of the symptomswas shown [19]. Moreover, laboratoryparameters (e.g. acid excretion, serumcholesterol) were significantly improvedby means of the alkaline therapy.
Treatment with alkaline salts suchas potassium citrate is even able toreduce bone resorption. This effect ofpotassium citrate supplementation onbone metabolism was investigated in46 postmenopausal women with lowbone density. One group received a 3-month course of potassium citratesupplementation (0.08 – 0.1 g/kg bodyweight daily), another group served ascontrol. Evaluation of electrolyte andacid-base homeostasis-related para-meters, and markers of bone turnoverand of renal function showed a signifi-cant decrease in net acid excretiononly upon citrate supplementation.Moreover, urinary excretion of boneresorption markers decreased thusindicating that citrate ingestion posi-tively affects bone health [20]. Theequimolar replacement of dietary sodi-um chloride and potassium chloridewith alkaline sodium and potassiumbicarbonate under metabolic homeosta-sis conditions, thus neutralising dietaryacid load, not only resulted in signifi-cant calcium retention and reducedrenal excretion of bone markers butalso decreased mean daily plasma cor-tisol and urinary excretion of tetra-hydrocortisol [21]. Other endocrinefactors relevant to bone such as para-thyroid hormone or vitamin D werenot affected. Therefore, mild metabolicacidosis may be associated with a stateof cortisol excess. These acidosis-induced increases in cortisol secretionand plasma concentration may play arole in mild acidosis-induced alter-ations in bone metabolism as well.
Dieting and Fasting
Dieting and fasting are critical tochanges of acid–base homeostasis. Forexample, solely because of the intakeof sodium bicarbonate, the calciumrelease from the bone in young womenwho had developed ketoacidosis as aresult of fasting could be prevented[22]. Generally speaking, modern dietscontribute to an increase in metabolic
Schweiz. Zschr. GanzheitsMedizin Jg.18, Heft 5, September 2006
Übersichtsarbeiten � Review Articles
Fig. 6. Mean (± SEM) bone mineral density at the femoral neck and lumbar spine withincreasing quartiles of energy-adjusted potassium intake for premenopausal women(n=336) (Modified from [22]).

acidosis and to greater bone loss asdemonstrated for low-carbohydrate,high-protein diets (Atkins). Consumptionof such a diet for six weeks may in facthelp an individual to lose weight, but itconsiderably increases acid load andresults in latent acidosis withincreased risk of kidney stone forma-tion, negative calcium balance, andincreased risk of bone loss, as demon-strated in Fig. 8 [23]. Table 1 illus-trates the dietary scheme applied forthree different phases:
Is animal or vegetable protein
detrimental to bone health?
Judging from the most recent studies,food protein from different sourcesseems to have different effects on bonemetabolism. Elderly women who havea high proportion of animal protein intheir diet showed a more rapid loss ofbone density and a higher risk of hipfractures than women with a low pro-portion [24]. In the latter group (lowproportion of animal protein), it wasfound that fewer women sustained ahip fracture during the observationperiod of 7 years. Animal foods containpredominantly acid-forming substanceswhereas protein in vegetable foods isaccompanied by base-forming sub-stances.
The protective function that anincreased consumption of vegetable asopposed to animal protein may havehas also been confirmed in interna-tional studies. The incidence of hipfractures differs in the populations ofdifferent countries, and it is directly
Schweiz. Zschr. GanzheitsMedizin Jg.18, Heft 5, September 2006
Übersichtsarbeiten � Review Articles
Tab. 1. Composition of normal diet, severely carbohydrate-restricted induction diet andmoderately carbohydrate-restricted maintenance diet. Modified from [23]
(g/day) Duration Carbo- Protein Fat Body weight
(weeks) hydrates (kg, n=10)
Normal 2 285 81 90 81.3
Induction 2 19 164 133 78.4
Maintenance 4 33 170 136 77.2
Fig. 7. Renal acid and calcium excretion with different protein intakes [g/day] with andwithout sodium bicarbonate substitution [70 mEq/day] (modified from [16]).
Fig. 8. Effect of low-carbohydrate, high-protein diet (Atkins diet) on renal net acid excretion, renal calcium excretion and serum osteocal-cin. Patients had been on a normal non-weight-reducing diet, then a severely carbohydrate-restricted induction diet for 2 weeks, after whichthey followed a moderately carbohydrate-restricted maintenance diet for 4 weeks as depicted above (n=10). Modified from [23].

correlated with the level of consump-tion of animal protein of the differentcultures. Analysis of the data on theincidence of hip factures in 33 coun-tries in relation to the respective coun-try-specific characteristics of the percapita consumption of animal and veg-etable foods (Fig. 9) showed that theincidence of hip fractures is the lowestin countries with a low intake of ani-mal protein [25].
However, the latest studies withchildren indicate that protein con-sumption is not generally detrimentalto bone health because in childrenlong-term dietary protein intakeappears to act anabolically on diaphy-seal bone strength during growth. Thismay at least partly be negated if thedietary potential renal acid load ishigh, i.e. if the intake of base-formingminerals, as provided by a high con-sumption of fruit and vegetables, islow. Children with higher dietarypotential renal acid load (PRAL), how-ever, had significantly lower bone min-eral content and long-term calciumintake was not associated with anybone variable. Protein and alkalinisingminerals are thus increasinglydescribed as playing a major role ininfluencing bone status in children andadolescents [26].
Mechanisms of the effects of acid
on bone cell function
The homeostasis for the maintenanceof a stable physiological pH environ-ment often functions only at theexpense of the bone mineral contentbecause latent acidosis causes therelease of calcium from bone, therebybuffering the additional protons.Metabolic acidosis first stimulates thephysicochemical release of minerals(decrease of the sodium, potassium,carbonate, and phosphate content ofbones) and subsequently the cell-mediated absorption of bone, as isschematically depicted in Fig. 10.Acidosis results in an increase in theactivity of bone-decomposing or respec-tively bone-resorbing cells (osteoclasts)and inhibition of the bone-formingcells (osteoblasts).
Genes that regulate the early “imme-diate reaction” of the osteoblasts areinhibited as are genes that control the
Schweiz. Zschr. GanzheitsMedizin Jg.18, Heft 5, September 2006
Übersichtsarbeiten � Review Articles
Fig. 9. Worldwide incidence of hip factures (modified from [25]).
Fig. 10. Schematic diagram of the effects of latent acidosis on bone (modified from[27]).

formation of bone matrix; gene inhibi-tion leads to an overall reduction ofbone remodelling and formation.Several in vitro studies with artificiallycultured bone cells confirmed theircharacteristics as potent acid buffers[27].
Figure 11 shows the dependence ofthe net calcium flux of cultured bonecells on the pH value of the surround-ing medium. With a physiologicallyacidic pH value below 7.4, calciumflows out of the bone cells into themedium, whereas a net absorption ofcalcium was only detectable with a pHvalue above 7.4.
Growth and maturation of the osteo-clasts is dependent on the interplay ofa number of factors. One of the expla-nations of the mechanisms of latentacidosis on bone cell function is theinduction of osteoblastic prostaglandinsynthesis, which is activated by meta-bolic acidosis and is followed by theinduction of a “receptor activatedNFkB ligand” (RANKL). This increasein RANKL is expected to augment osteo-clastic bone resorption by interactionwith the osteoclastic cell-surfacereceptor RANK as shown in Fig. 12.The RANKL/RANK interaction not onlyinitiates a differentiation cascade ofpre-osteoclasts to osteoclasts, that cul-
minates in mature bone-resorbingosteoclasts, but also increases theresorptive capacity and survival ofosteoclasts [28]. This acidosis-inducedincrease in RANKL is expected to aug-ment osteoclastic bone resorption andoffers an appropriate explanation forthe increase in cell-mediated net cal-cium efflux as described above.
Finally, thanks to the mechanismsof compensation dietary-induced latentacidosis does not provoke any signifi-cant changes of blood pH but the com-pensation inevitably consumes thebody’s reservoir of buffering sub-stances. When excess intake of animalprotein and deficient dietary base sup-ply persists for a longer time this willhave a negative impact on bone mass.The undoubted positive influence of adiet rich in fruit and vegetables can beexplained not only by a high intake ofmicronutrients and secondary herbalingredients but also by the positiveeffects of an adequate base supply.
Effects of latent acidosis onconnective tissue function
Connective tissue is an important tran-sit pathway for metabolic productssuch as oxygen, carbon dioxide, nutri-ents, electrolytes, water, acids and
bases. Even slight changes of the bloodpH lead to a change in the physico-chemical characteristics of the proteo-glycans, the branched protein-saccha-ride constituents of connective tissue.These proteoglycans directly exchangewith the extracellular fluid.
Proteoglycans are composed of aprotein component and a glucosamino-glycan component, which contains amultitude of negatively charged func-tional groups (e.g. sulphate residuesR~O-SO3
–). This negative charge enablesthe binding of water molecules whichcontribute to the elasticity and flexibil-ity of the connective tissue. In latentacidosis the negative charge of the sul-phate residues is neutralised and thewater binding capacity is decreasingthereby reducing the elasticity andflexibility of the connective tissue.
In cartilage as well, proteoglycanswith the hyaluronic acid moleculesthat are bound to them represent ahigh-molecular-weight polyanioniccomplex that forms the importantcompressible component of cartilagebecause of the high water-bindingcapacity [29]. The water-binding capac-ity of the extracellular matrix proteinsis very much determined by the degreeof dissociation of the functional acidresidues whose dissociation is againhighly pH-dependent. Acidosis of the
Schweiz. Zschr. GanzheitsMedizin Jg.18, Heft 5, September 2006
Übersichtsarbeiten � Review Articles
Fig. 11. Effects of the pH of the medium onthe net calcium flux in cultured bone cells. Apositive value shows a net calcium flow out ofthe bone cells into the surrounding medium,negative values indicate net calcium influx(modified from [27]).
Fig. 12. Scheme of acidosis induced activation of RANKL/RANK interaction initiating thedifferentiation cascade of pre-osteoclasts and increasing bone resorptive capacity andsurvival of osteoclasts (modified from [28]).

synovial fluid therefore decreases car-tilage elasticity due to reduced waterbinding. Effects of latent acidosis onthe function of cartilage can beexplained in this way. At present, how-ever, the complex structure of the
extracellular matrix does not allowdirect measurement of the function ofcartilaginous tissue with differentdegrees of dissociation. In patientswith rheumatoid arthritis the pH of theknee joint’s synovial fluid is signifi-
cantly more acidic compared to thenormal range (pH 7.4 – 7.8), as shownin Fig. 13 [30]. Consequently, acidosisencourages joint cartilage abrasion bymechanical stress that promotes thevicious circle of deformation andinflammation. Acidosis might alsoimpair the filtration effect of the con-nective tissue which may, in turn,additionally contribute to a deteriora-tion in the nutrient supply of this poor-ly perfused tissue. Finally the wholelocomotor system is involved becauseof acidosis-induced impairment of theligaments and tendons.
Patients with chronic low back painwithout radicular involvement benefit-ed from a 4-week supplementary diettherapy by taking alkaline minerals:both the pain as well as the physicalmobility improved significantly (seeFig. 14), and the consumption of non-steroidal, anti-inflammatory drugs(NSAID), which may cause severe sideeffects when applied chronically, couldbe clearly reduced [31]. Indeed, longterm balancing of acids and bases isrequired for a complete regenerationof the connective tissue and to notice-ably relieve the chronic pain.
In a recent study, patients withrheumatoid arthritis of at least twoyears’ duration were shown to havebenefited from alkaline mineral sup-plementation (see Fig. 15). At the endof a 12-weeks study there was a signif-icant decrease in disease activity score(DAS-28) and in pain level measuredon a visual analogue scale (VAS) onlyin the group supplemented with 30 g/day of an alkaline food supplement(Basica Vital®) compared to the controlgroup. Moreover, the steroid or NSAIDmedication could be reduced withalkaline supplementation whereas noreduction of medication was consid-ered to be possible for the controlgroup [32].
Another important impact on acid-base homeostasis with long-term effectson the functions of the connective tis-sue occurs with chronic intake of pro-ton pump inhibitors for the treatmentof gastroesophageal reflux. After mealsthe parietal cells produce hydrochloricacid to enable the digestion of foods.At the same time bicarbonate is gener-ated and transferred into the blood
Schweiz. Zschr. GanzheitsMedizin Jg.18, Heft 5, September 2006
Übersichtsarbeiten � Review Articles
Fig. 13. Mean H+ ion concentration in the synovial fluid from the knee joints of patientswith different forms of arthritis (Modified from [30]).
Fig. 14. Effects of alkaline mineral supplementation on patients with chronic low backpain. Arhus low back pain rating scale before and after supplementation with Basica®
(n=82). Modified from [31].

stream from where it afterwards istransported via the bile ducts into theintestine to neutralize or alkalize thegastric mash. This closed system doesnot exert any net effect on acid–basehomeostasis, but acts as a kind of tem-poral effect reflected by the “alkalinefloods” after each meal. These alkalinefloods provide an important physiolog-ical process for removing the acidsbound to sulphated residues of con-nective tissue proteoglycanes. Chronicintake of proton pump inhibitors suchas omeprazol interfere with this sys-tem and may suppress the essential“purification process”.
Evolutionary aspects ofacid–base homeostasis
There is a growing awareness that theprofound changes in the environmentincluding diet and other life-style con-ditions that began with the introduc-tion of agriculture and animal hus-bandry approximately 10,000 yearsago, occurred too recently on an evo-lutionary time scale for the humangenome to adjust. In conjunction withthis discordance between our ancient,
genetically determined biology and thenutritional, cultural, and activity pat-terns of contemporary Western popu-lations, many of the so-called diseasesof civilization have emerged. In partic-ular, agriculture and food-processingprocedures introduced during theNeolithic Period and during theIndustrial Period fundamentally alteredcrucial nutritional characteristics ofthe diets of our ancestors: in additionto changes in the glycemic load, fattyacid composition, macronutrient com-position, micronutrient density, sodi-um-potassium ratio, and fibre content,considerable changes have taken placein the acid-base homeostasis. Comparisonof the estimated net endogenous acidproduction (NEAP) from 159 retro-spective ancestral preagricultural dietswith contemporary diets clearly demon-strates that 87% were net base-pro-ducing with a mean NEAP of –88 ± 82meq/day [33].
The average contemporary Americandiet provides an acid surplus of 48meq/day and is characterized by animbalance of nutrient precursors ofhydrogen and bicarbonate ions there-by inducing a lifelong, low-grade path-ogenically significant systemic meta-
bolic acidosis. The historical shift fromnegative to positive NEAP was account-ed for by the displacement of highlyalkalising plant foods in the ancestraldiet by cereal grains and energy-dense, nutrient-poor foods in the con-temporary diet – neither of which arenet base-producing. Therefore theevolutionary collision of our ancientgenome with the nutritional qualitiesof recently introduced foods mayunderlie many of the chronic diseasesof Western civilization [34].
Further research fields related to acid–base homeostasis
In sportsmen and sportswomen, fre-quent lactate acidosis increases thesusceptibility to physical injury. In con-trast, it is suggested that an adequatebase supply may have a beneficialimpact on performance by delayingthe onset of lactate acidosis but also byavoiding physical impairment. Muscleactivity during sports performance isin fact known to be associated with anincrease in both intra- and extracellu-lar proton concentration. It is known
Schweiz. Zschr. GanzheitsMedizin Jg.18, Heft 5, September 2006
Übersichtsarbeiten � Review Articles
Fig. 15. Percent change of disease activity score DAS-28 (left) and percent change of VAS pain index (right) of rheumatoid arthritis patients(*p<0.05, **p<0.01). Modified from [32].

that alkaline sodium citrate ingestioncould reduce plasma proton concen-tration and improve physical perfor-mance [35, 36, 37].
Extracellular pH affects mineralcation flux through cell membranes aswell. It seems that there is a strongcorrelation between interstitial protonconcentration and the potassiumrelease from muscle cells during exer-cise since potassium efflux is regulatedby voltage-dependent K channels andpH-dependent KATP channels. Potas-sium efflux and accumulation in theinterstitium is not only important formuscle function but also for the devel-opment of fatigue resulting from exer-cise. Microdialysis measurements haverecently demonstrated that sodium cit-rate ingestion (300 mg/kg body weight)reduces the exercise-induced inter-sti-tial acidosis in human skeletal muscle(Fig. 16) [38].
It was also shown by the latterauthors that this reduction of H+ ionconcentration was associated with areduced interstitial accumulation ofpotassium during muscle activity.These results accordingly suggest adelayed onset of muscle fatigue andsustained muscle performance byalkaline sodium citrate ingestion priorto exercise in sports.
Of considerable interest was thefinding, in a study on 42 boys [39], of asignificant positive correlation betweenthe pH in the brain and the intelligencequotient (IQ), i.e. the lower the actualacid concentration in the brain, thehigher the IQ.
Conditions representing physiologi-cal acidosis in vitro induced the aggre-gation of human Ab amyloid proteins[40]. Metal ions such as copper, zincand iron are enriched in the amyloidplaques in Alzheimer's disease andunlike other biometals tested at maxi-mal biological concentrations, markedcopper-induced aggregation of Abemerged as the pH of the surroundingsolution was lowered from 7.4 to 6.8.The reaction was completely reversiblewith either chelation or alkalinization.Since a mildly acidic environmenttogether with increased copper andzinc concentrations are common fea-tures of inflammation, it is suggestedthat Ab aggregation by these factorsmay be a response to local injury andthat metabolic acidosis may also play arole in the development of Alzheimer’sdisease.
The acid–base homeostasis depen-dent modulation of cortisol output mayinfluence the risk of insulin resistancesyndrome. This hypothesis appears to
be consistent with previous epidemio-logical reports correlating high potas-sium consumption, or a high intake offruits and vegetables, with a reducedrisk for diabetes and coronary disease.Metabolic acidosis is known to pro-mote renal acid excretion by theinduction of ammonia-generating glut-aminase and other enzymes in therenal tubules (see earlier: Compensationmechanisms of latent acidosis). Thisprocess is also strongly correlated withincreased cortisol and aldosteroneproduction. Since cortisol promotes thedevelopment of visceral obesity, andhas a direct negative impact on insulinfunction throughout the body, even amodest sustained up-regulation of cor-tisol production may have the potentialto increase the risk of insulin resis-tance syndrome and type 2 diabetes[41]. Future prospective epidemiologyshould assess whether the estimatedacid–base homeostasis of habitualdiets correlates with the risk of insulinresistance syndrome and diabetes.
Conclusion
To what extent the diet can affect theacid–base homeostasis has been thesubject of controversy for many years.Acute acidosis or alkalosis cannot beproduced by the consumption of cer-tain foods. However, the pathobio-chemical effects of latent acidosis onimpaired renal function, diabetes mel-litus, hyperuricemia, or gout areundisputed. Based on new scientificfindings, causal evidence has also nowbeen furnished for the positive effectsof a well-balanced acid–base equilibri-um empirically established in natur-opathy. Although diet-induced latentacidosis does not produce majorchanges in the blood pH because of thecompensation mechanisms of the kid-ney, this compensation inevitably leadsto the consumption of endogenousbuffer reserves and, therefore, pre-dominantly to a loss of bone substanceif the increased acidification caused bya surplus of animal protein and ashortage of alkaline substances in thediet exists for a long period of time. Adisturbance of the muscle proteinmetabolism as well as the structure
Schweiz. Zschr. GanzheitsMedizin Jg.18, Heft 5, September 2006
Übersichtsarbeiten � Review Articles
Fig. 16. Mean (± SEM) interstitial proton concentration during ingestion, exercise period(solid line: citrate ingestion; dotted line: placebo) and recovery from exercise (n=7). *Sig-nificant difference between citrate ingestion (CIT) and placebo (PLA). Modified from [38].

and function of cartilage are othernegative consequences of the endoge-nous compensation, which can alsoaggravate degenerative diseases suchas arthrosis or rheumatism.
Our Stone Age ancestors preferreda more or less mixed diet which inspite of containing a high proportion ofanimal protein was also characterizedby a surplus of base-forming sub-stances. In contrast, the diet in today’sWestern industrial nations is charac-terized by a large quantity of acid-forming nutrients, above all due to thesurplus of animal protein. On the otherhand, a high proportion of fresh fruitand vegetables in the diet contributesto the formation of the surplus of basesin the body.
Literature
1. Frassetto L, Todd, KM, Morris RC, SebastianA: Estimation of net endogeneous noncar-bonic acid production in humans from dietpotassium and protein content. Am J ClinNutr 1998;68:576–583.
2. Frassetto L, Morris RC, Sebastian A: Effect ofage on blood acid–base composition in adulthumans: role of age-related renal functionaldecline. Am J Physiol 1996;271:F1114–F1122.
3. Frassetto L, Sebastian A: Age and systemicacid–base equilibrium: analysis of publisheddata. J Gerontol 1996;51A:B91–B99.
4. Alpern RJ, Sakhaee K: The clinical spectrumof chronic metabolic acidosis. Homeostaticmechanisms produce significant morbidity.Am J Kidney Disease 1997;29:291–302.
5. Frassetto L, Morris RC, Sebastian A: Potassi-um bicarbonate reduces urinary nitrogenexcretion in postmenopausal women. J ClinEndocrin Metab 1997;82:254–259.
6. Lemann, J Jr, Litzow JR, Lennon EJ: Theeffects of chronic acid loads in normal man:Further evidence for the participation of bonemineral in the defense against chronic meta-bolic acidosis. J Clin Invest 1966;45:1608–1614.
7. Wachman A, Bernstein DS: Diet and Osteo-porosis. Lancet 1968;958–959.
8. Marsh AG, Sanchez, TV, Michelsen O, Chaf-fee FL, Fagal, SM: Vegetarian lifestyle andbone mineral density. Am J Clin Nutr 1988;48:837–841.
9. Ball D, Maughan RJ: Blood and urineacid–base status of premenopausal omnivo-rous and vegetarian women. Br J Nutr 1997;78:683–693.
10. New SA, Bolton-Smith C, Grubb DA, ReidDM: Nutritional influences on bone mineraldensity: A cross-sectional study in pre-menopausal women. Am J Clin Nutr 1997;65:1831–1839.
11. Tucker KL, Hannan MT, Chen H, Cupples LA,Wilson PW, Kiel DP: Potassium, magnesium,and fruit and vegetable intakes are associatedwith greater bone mineral density in elderlymen and women. Am J Clin Nutr 1999;69:727–736.
12. New SA, MacDonald HM, Campbell MK,Martin JC, Garton MJ, Robins SP, Reid DM:
Lower estimates of net endogenous non-car-bonic acid production are positively associat-ed with indexes of bone health in pre-menopausal and perimenopausal women.Am J Clin Nutr 2004;79:131–138.
13. Macdonald HM, New SA, Golden MH, Camp-bell MK, Reid DM: Nutritional associationswith bone loss during the menopausal transi-tion: evidence of a beneficial effect of calci-um, alcohol, and fruit and vegetable nutrientsand of a detrimental effect of fatty acids. AmJ Clin Nutr 2004;79:155–165.
14. Macdonald HM, New SA, Fraser WD, Camp-bell MK, Reid DM: Low dietary potassiumintakes and high dietary estimates of netendogenous acid production are associatedwith low bone mineral density in pre-menopausal women and increased markersof bone resorption in postmenopausalwomen. Am J Clin Nutr 2005;81:923–933.
15. Weiss RE, Gorn A, Dux S, Nimni ME: Influ-ence of high protein diets in cartilage andbone formation in rats. J Nutr 1981;111:804–816.
16. Lutz J: Calcium balance and acid–base statusof women as affected by increased proteinintake and by sodium bicarbonate ingestion.Am J Clin Nutr 1984;39:281–288.
17. Sebastian A, Harris ST, Ottaway JH, ToddKM, Morris RC Jr: Improved mineral balanceand skeletal metabolism in postmenopausalwomen treated with potassium bicarbonate.N Engl J Med 1994;330:1776–1781.
18. Giannini S, Nobile M, Sartori L, Dalle Car-bonare L, Ciuffreda M, Corro P, D´Angelo A,Calo L, Crepaldi G: Acute effects of moderatedietary protein restriction in patients withidiopathic hypercalciuria and calciumnephrolithiasis. Am J Clin Nutr 1999;69:267–271.
19. Witasek A, Traweger C, Gritsch P, Kogelnig R,Trötscher G: Einflüsse von basischen Miner-alsalzen auf den menschlichen Organismusunter standardisierten Ernährungsbedingun-gen. Erfahrungsheilkunde 1996;45:477–488.
20. Marangella M, Di Stefano M, Casalis S,Berutti S, D'Amelio P, Isaia GC: Effects ofpotassium citrate supplementation on bonemetabolism. Calcif Tissue Int 2004;74:330–335.
21. Maurer M, Riesen W, Muser J, Hulter HN,Krapf R: Neutralization of Western dietinhibits bone resorption independently of Kintake and reduces cortisol secretion inhumans. Am J Physiol Renal Physiol 2003;284:F32–F40.
22. Grinspoon SK, Baum HBA, Kim V, Coggins C,Klibanski A: Decreased bone formation andincreased mineral dissolution during acutefasting in young women. J Clin EndocrinMetab 1995;80:3628–3633.
23. Reddy ST, Wang CY, Sakhaee K, Brinkley L,Pak CY: Effect of low-carbohydrate high-pro-tein diets on acid–base balance, stone-form-ing propensity, and calcium metabolism. AmJ Kidney Dis 2002;40:265–274.
24. Sellmeyer DE, Stone KL, Sebastian A, Cum-mings SR: A high ratio of dietary animal tovegetable protein increases the rate of boneloss and the risk of fracture in post-menopausal women. Am J Clin Nutr 2001;73:118–122.
25. Frassetto LA, Todd KM, Morris RC Jr., Sebas-tian A: Worldwide incidence of hip fracture inelderly women: relation to comsumption ofanimal and vegetable foods. J Gerontol 2000;55A:M585–M592.
26. Alexy U, Remer T, Manz F, Neu CM, Schoe-nau E: Long-term protein intake and dietarypotential renal acid load are associated withbone modeling and remodeling at the proxi-
mal radius in healthy children. Am J Clin Nutr2005; In press.
27. Bushinsky DA, Frick KK: The effects of acidon bone. Curr Opin Nephrol Hypertens 2000;9:369–379.
28. Frick KK, Bushinsky DA: Metabolic acidosisstimulates RANKL RNA expression in bonethrough a cyclo-oxygenase-dependent mech-anism. J Bone Miner Res 2003;18:1317–1325.
29. Garret RH, Grisham CM: Biochemistry. Saun-ders College Publishing, Orlando, Florida1995;345–350.
30. Farr M, Garvey K, Bold AM, Kendall MJ,Bacon PA: Significance of the hydrogen ionconcentration in synovial fluid in rheumatoidarthritis. Clin Exp Rheumatol 1985;3:99–104.
31. Vormann J, Worlitschek M, Goedecke T, Sil-ver B: Supplementation with alkaline miner-als reduces symptoms in patients with chron-ic low back pain. J Trace Elem Med Biol 2001;15:179–183.
32. Cseuz RM, Bender T, Vormann J: Alkalinemineral supplementation for patients withrheumatoid arthritis. Rheumatology 2005;44(Supplement 1):i79.
33. Sebastian A, Frassetto LA, Sellmeyer DE,Merriam RL, Morris RC Jr.: Estimation of thenet acid load of the diet of ancestral preagri-cultural Homo sapiens and their hominidancestors. Am J Clin Nutr. 2002;76:1308–16.
34. Cordain L, Eaton SB, Sebastian A, Mann N,Lindeberg S, Watkins BA, O'Keefe JH, Brand-Miller J: Origins and evolution of the Westerndiet: health implications for the 21st century.Am J Clin Nutr 2005;81:341–354.
35. Greenleaf JE, Looft-Wilson R, Wisherd JL,McKenzie MA, Jensen CD, Whittam JH: Pre-exercise hypervolemia and cycle ergometerendurance in men. Biol Sport 1997;14:103–14.
36. Oopik V, Saaremets I, Medijainen L, KarelsonK, Janson T, Timpmann S: Effects of sodiumcitrate ingestion before exercise onendurance performance in well trained col-lege runners. Br J Sports Med 2003;37:485–489.
37. Shave R, Whyte G, Siemann A, Doggart L:The effects of sodium citrate ingestion on3,000-meter time-trial performance. J StrengthCond Res 2001;15:230–234.
38. Street D, Nielsen JJ, Bangsbo J, Juel C:Metabolic alkalosis reduces exercise-inducedacidosis and potassium accumulation inhuman skeletal muscle interstitium. J Physiol2005;566:481–489.
39. Rae C, Scott RB, Thompson CH, Kemp GJ,Dumughn I, Styles P, Tracey I, Radda G.: IspH a biochmical market of IQ? Proc. R. Soc.London 1996;B 263,1061–1064.
40. Atwood CS, Moir RD, Huang X, Scarpa RC,Bacarra NM, Romano DM, Hartshorn MA,Tanzi RE, Bush AI: Dramatic aggregation ofAlzheimer abeta by Cu(II) is induced by con-ditions representing physiological acidosis. JBiol Chem 1998;273:12817–12826.
41. McCarty MF: Acid–base balance may influ-ence risk for insulin resistance syndrome bymodulating cortisol output. Med Hypotheses2005;64:380–384.
Korrespondenzadresse:
Prof. Dr. rer. nat. Jürgen VormannInstitut für Prävention und Ernährung Adalperostrasse 37, DE-85737 [email protected]
Schweiz. Zschr. GanzheitsMedizin Jg.18, Heft 5, September 2006
Übersichtsarbeiten � Review Articles