latest phl
TRANSCRIPT

8/6/2019 Latest Phl
http://slidepdf.com/reader/full/latest-phl 1/27
Introduction and history
Contents- equipment and personnel
Functions and services
Tests conducted
Accreditation
Conclusion
Definition -A place equipped for the performance of tests, and for the preparation of reagents,therapeutic chemical materials, aimed at discovery of the infection foci of naturallycommunicable diseases, channels of disease spread, prevention and control of disease and
improvement of the community¶s health .
History
Established in 1892, the Public Health Laboratory was the world's first Municipal BacteriologicalLaboratory. In the century since its first campaign, to control diptheria in New York City, the bureauhas expanded to provide a wide variety of clinical and environmental laboratory testing services.Today, the Public Health Laboratory performs a total of over two million tests on the more than fourhundred thousand specimens it receives each year.
Mission Statement:
To ensure the health of all New York City residents by providing quality laboratory testing serviceswhich address the needs of the NYC DOHMH and its partner agencies as they respond to clinical andenvironmental public health concerns.
E ven though the role of pathogenic bacteria and viruses in human health was defined in thenineteenth century, the first public health laboratories in the United States were called chemicallaboratories and only performed elementary analyses of milk, water, and other substances. TheMinnesota Board of Health established the first public health chemical laboratory in 1873, and in1881 the New York legislature established the first state chemical laboratory. By 1869, most of the larger cities in Massachusetts had health boards that were actively involved in the area of sanitary engineering. The state's public health laboratory, established in 1886, was intended
primarily to perform chemical analysis, though it was called a "hygienic" laboratory. Michiganfollowed Massachusetts' lead, moving into the regulation of food and water, and in 1887, theMichigan State Laboratory of Hygiene was established, with Dr. Victor C. Vaughn as director.
Both the Massachusetts and Michigan state hygienic laboratories began working on theconnection between the public water supply and typhoid fever. This was probably the firstapplication of bacteriology to sanitary science in the United States. By 1890 a number of state
History-Phl dates back to the bacteriological labs of the 18 th century, however one of the reliable records can be traced to two sources- provincial medical association at Calgary, Alberta, august 19, 1909 and Secretary,department of public health, letter to Montana physicians, October, 1917
In October 1917, the Montana state health department announced theopening of a public health laboratory ³« the lab will be ready 2 receivespecimens embracing the following: any cultures, smears, or material for smear, for bacteriological determination in the diagnosis of diphtheria,
pneumonia, meningitis, tuberculosis, neisserian infection, ophthalmianeonatorium, etc.´ 1 the one-person staff at that time analysed andreported (sometimes by telegram, sent ³collect´) about 100 tests per month. Today a staff of about 35 persons does the work-about 14,000
8/6/2019 Latest Phl
http://slidepdf.com/reader/full/latest-phl 2/27
and local laboratories were established, with many of them doing both chemical and bacterialanalysis.
The nation's first diagnostic public health laboratory was the result of work by Drs. Hermann M.Biggs and T. Mitchell Prudden. In 1887, these two physicians were able to isolate Vibrio
cholerae , the bacterium that causes cholera, from the feces of ill passengers on an immigrantship anchored in New York City harbor, and they were anxious to promote their technique as aroutine diagnostic measure. It was not until a cholera scare in 1892, however, that they were ableto convince the city health department of the need to establish a laboratory to develop and usediagnostic methods. On September 9 of that year, the New York City Department of Health'sDivision of Pathology, Bacteriology, and Disinfection was created, with Dr. Biggs as thedirector.
Biggs soon had a second disease upon which to focus his attention. Cases of diphtheria peaked inthe 1890s in New York City, and Biggs was ready with a bacteriological diagnostic technique.He used this technique to demonstrate that half the patients in the New York City diphtheria
hospital had been misdiagnosed. Because of this high rate of misdiagnosis, he stressed thatlaboratory testing to confirm a diagnosis would be cheaper than disinfecting and quarantining thehomes of every case of suspected diphtheria. The health board agreed, and the first officialmedical bacteriologist in the United States, Dr. William H. Park, was appointed. Meanwhile,Biggs continued the expansion of the laboratory's diagnostic capabilities. He began routinelaboratory bacteriological testing on every suspected tuberculosis case, despite his colleagues'skepticism of its value. In 1895, Biggs added vaccine production to the laboratory. He and hisassistant, Park, refined the methods for production of the smallpox vaccine, and of diphtheria andtetanus antitoxins.
The New York City public health laboratory became a model for other public health
departments. Within a few years, the diagnostic public health laboratory had become an essentialcomponent of an effective health department.
HISTORICAL SCOPE
The laboratory added a new dimension to public health department activities. The ability toisolate and identify disease-producing organisms immeasurably strengthened the prevention andcontrol role of the department. However, this new health department tool of diagnostic
bacteriology was not readily accepted by the general medical profession. Duffy, in "TheSanitarians," quoted from an 1884 J AMA journal article on Robert Koch and the tuberculosis(TB) bacillus that concludes a "too ready acceptance of the bacillus doctrine" was likely to do
more harm than good and that "neither phthisis nor any form of tuberculosis (was) contagious."
Biggs and his associates in New York City met strong resistance from physicians to the city's board of health requirement to report all cases of tuberculosis. The attitude of New York physicians was duplicated around the country as more and more health departments institutedthis requirement. Through perseverance and laboratory expertise, health departments wereeventually able to convince the public and physicians that tuberculosis was communicable andnot an hereditary disease related to environmental conditions.
8/6/2019 Latest Phl
http://slidepdf.com/reader/full/latest-phl 3/27
As the diagnostic expertise of the laboratories grew, the ability of the public health dpeartmentsto control disease was bolstered. The ability to culture disease-causing organisms fromasymptomatic people led to recognition of the carrier state and a reexamination of isolation
practice. Laboratory-supported disease control efforts resulted in significant reductions in diseasemortality by the early twentieth century.
By mid-century, most of the laboratories had evolved in service provision to the same generalscope provided today: testing support of the communicable disease programs, chemical and
bacteriologic testing of drinking water, analysis of food and milk, and limited non-communicabledisease testing. As continuing advances in technology enhanced the diagnostic capabilities of thelaboratories, the public health department core functions of assessment, policy development, andassurance were significantly strengthened.
Development of federal public health laboratories was slower than at the state level, although thenucleus of what would evolve into the National Institutes of Health was established in 1887. Inthat year Joseph Kinyoun founded the Laboratory of Hygiene, a bacteriology research laboratory
at the Marine Hospital on Staten Island. In 1891, this laboratory was moved to Washington,D.C., where it expanded into what became the National Institutes of Health (NIH) forty yearslater. The NIH laboratories still focus primarily on research and are not usually considered frontline public health laboratories. The Centers for Disease Control and Prevention (CDC), which isthe acknowledged apex of the public health laboratory system, was established even later thanthe NIH. In 1942 the Office of Malaria Control in War Areas (MCWA) was established. In 1946the MCWA was converted to the Communicable Disease Center. It was renamed the Centers for Disease Control in 1980, and in 1992 became the Centers for Disease Control and Prevention.The CDC has since matured into a collective group of laboratories and programs that isdedicated to preserving the health and wellbeing of the public. The testing performed by CDC, inconjunction with local and state laboratories, has been essential to the provision of safe drinkingwater, an increased awareness of the importance of environmental health issues, and the declineof communicable diseases such as syphilis.
As the laboratory sciences of microbiology, chemistry,and molecular biology advanced during the1900s, many new roles were created for PHLs, andorganizations took on housing their own laboratories,as testing originally performed solely in PHLs transitionedto specialized laboratories. Many governmentlaboratories charged with regulating and assuring foodand environmental safety were relocated from publichealth to new environmental or agricultural agencies.Appreciation that these are still PHLs is evident in the
name and membership of the leading advocacy organizationrepresenting PHLs in the U.S.²the APHL.Vaccine production and diagnostic-test developmenttransitioned to the private sector and academia. PHLs,however, retained many roles, including data management 11
and applied research, with some state PHLs as part of university systems.Applied research is the basis for evidence-basedPHL practice, as evidenced in this supplement byBaker et al., who describe scientific, technical, ethical,
8/6/2019 Latest Phl
http://slidepdf.com/reader/full/latest-phl 4/27
and policy issues that must be addressed prior tothe addition of a new condition to a state newbornscreening test panel. 12 The authors present findingsof the recent experience in adding a test for severecombined immunodeficiency (SCID) to Wisconsin¶s
panel of newborn screening tests.Baker MW, Laessig RH, Katcher ML, Routes JM, Grossman WJ,Verbsky J, et al. Implementing routine testing for severe combinedimmunodeficiency within Wisconsin¶s Newborn Screening Program.Public Health Rep 2010;125(Suppl 2):88-95.
The Evolving Public HealthLaboratory System
Functions
ROLE OF THE PUBLIC HEALTH LABORATORY
Initially, the role of the public health laboratory (PHL) was simply to serve any of the perceivedlaboratory needs of the various jurisdictions. Over time this role was defined more precisely,although still ambiguously, under general categories. The PHL became a recognized central partof the public health infrastructure and was charged with supporting this infrastructure in each of the three core public health functions²assessment, assurance, and policy development. BecausePHLs differ dramatically in complexity, dependent largely on the population served, the testmenus of the laboratories differ greatly. In general, all laboratories support the following corefunctions: testing information relevant to monitoring the environment; assessing the population'shealth status; investigating and controlling disease outbreaks; treating and controllingcommunicable diseases like tuberculosis, syphilis, gonorrhea, and chlamydia; acting as areference laboratory for private sector laboratories; and assuring the safety of food and water. Inaddition, many PHLs have ongoing applied research programs directed toward improving thereliability and efficiency of testing, and identifying and controlling emerging problems.
PHL support for assessment and assurance functions are the most diverse. Laboratory testing tosupport assessment may involve specimens from people, animals, insects, fomites (inert vectors),and environmental sources. E xamples of this type of activity are varied, but one of the mostcommon is to support the investigation of disease outbreaks. It is the laboratory's role to isolateand identify the causative agent and to identify the source of the infection, which may be other individuals, insect or animal vectors, water, food, or dirt. For example, in a food poisoningincident associated with restaurant meals, the laboratory is pivotal in the determination of whether the incident is localized (caused by poor food handling procedures or infected staff in aspecific restaurant) or widespread (caused by contaminated food distributed to many placeslocally or nationally).
Population surveillance studies for assessment of disease prevalence in a community also rely ontesting and information provided by the PHL. Neonatal screening for metabolic disorders,immune status screening, screening for sexually transmitted diseases, and screening for chronicdiseases are examples of this aspect of information gathering by PHLs.
8/6/2019 Latest Phl
http://slidepdf.com/reader/full/latest-phl 5/27
Rabies, botulism, and plague are examples of rare but important diseases of public healthsignificance that are not identified except in public health laboratories. Rabies is routinelyidentified by dissecting out specific portions of the brain of suspect animals to look for thecharacteristic lesions produced by the rabies virus. Rabies testing may be performed as routinesurveillance of the wild animal population or as a necessary adjunct to contact between an
individual and a suspect animal. Testing for Clostridium botulinum toxin (which causes botulism) in food or humans requires, at present, the use of animals. This requirement is the basisfor the restriction of this assay to PHLs. Plague surveillance is routinely done by PHLs in areaswhere plague is endemic in the animal population. If antibodies to plague are found in an animal
population that may have contact with humans, such as ground squirrels near a picnic area, thearea is closed to the public until an eradication effort is successful.
Support of the PHL for the assurance function of public health is probably the mostunrecognized and underappreciated facet of its role. Some of the testing cited under theassessment function has elements of assurance, such as the con- firmatory reference testing thatis offered to all private laboratories without charge. Private sector laboratories having difficulty
identifying a microorganism²confirming the true antibody status of a patient or defining theresistance pattern of Mycobacterium tuberculosis , for example²are able to request help from aPHL. But the most important role of assurance testing is to assure that community water suppliesare safe to drink. In addition to testing drinking water for chemical and microbiological safety,recreational water is tested to insure the safety of swimmers and bathers.
Another assurance function, not readily apparent to the public, is the screening of food handlersin restaurants and other facilities. Food poisoning events trigger this function if an organism issuspected or identified that can be transmitted through contamination of food by a food handler.The food facility staff is screened for suspect pathogens by the PHL, and any individuals foundto be infected are removed from the job until subsequent testing assures that they no longer areinfected.
The facet of assurance that is most often thought of in connection with PHLs is the provision of certain testing services to the indigent population and to other individuals who might nototherwise be able to afford tests. This aspect of PHL testing varies from state to state dependingupon local laboratory resources or the availability of specimen transport to the state laboratory.
Participation of PHLs in the third core function, policy development, is largely throughconsultation or regulatory services. PHL staff is involved in policy development that impactsresearch and technology needs as well as health issues such as HIV/AIDS (humanimmunodeficiency virus/acquired immunodeficiency syndrome), sexually transmitted diseases,and tuberculosis. Policies to solve environmental problems are often developed primarily byPHL staff. Some state PHLs develop and implement regulations that govern all aspects of privateclinical and local public laboratory operations within the state. This includes laboratory
personnel and facility licensure requirements and environmental monitoring requirements.
In summation, the primary role of PHL is as a service unit providing timely information tofacilitate the public health department's mission to protect the health of the community. Toadequately perform this role, the laboratory must be functionally integrated within the health
8/6/2019 Latest Phl
http://slidepdf.com/reader/full/latest-phl 6/27
depart- ment's relevant programs so that the needs and requirements of these programs are met.The unbiased information and laboratory data provided by a PHL are necessary adjuncts to aneffective public health department.
COST OF SERVICES
Health care funding continues to increase, but, according to Health and Human Servicesestimates, public health spending is only about 1 percent of the total, and the expenditure for PHLs is only 3 percent to 5 percent of the public health allocation. This demonstrates thatfederal, state, and county governments are making a very cost- effective investment in PHLs.The cost savings of population-based interventions based on PHL testing information isestimated to be analogous to the cost savings (ten dollars for every one dollar spent) of aneffective immunization program. This estimate is derived from potential medical costs savedversus screening costs for population-based surveillance testing, including that done for rabies,lead poisoning, sexually transmitted diseases, environmental carcinogens and pathogens, andmetabolic disorders in newborns.
LABORATORY STRUCTURE AND ORGANIZATION
Because of the wide variability in population between and within states, there is diversity in boththe structure and testing services of the PHLs in the individual states. All fifty states and theDistrict of Columbia operate their own PHLs, and some states have local laboratories, whichmay be autonomous or simply local extensions of the state PHL. The CDC functions primarily asa reference laboratory for the state PHLs, providing confirma- tory and esoteric testing servicesthat the state laboratories do not have the resources to perform. The CDC also funds assessmentand assurance studies at the local level to investigate issues of particular public healthimportance. The CDC is an integral part of the PHL system, and plays an important role innational disease surveillance.
Although the Food and Drug Administration (FDA) laboratories are public in the sense of being part of a government organization, they are not public health laboratories because they are not part of a public health department. Both the E nvironmental Protection Agency ( E PA) and theU.S. Department of Agriculture (USDA) also impact PHL operations. Much of theenvironmental monitoring done by PHLs follows E PA guidelines, and USDA regulations maydirectly or indirectly play a role in PHL operations. The other federal agency that has recentlyassumed a major role in PHLs is the Health Care Financing Administration (HCFA), which isinvolved in the development and implementation of federal regulations that affect all diagnosticlaboratories. These regulations are part of the Clinical Laboratory Improvement Amendments of 1988 (CLIA), which supersede all state regulations governing laboratories unless the stateregulations are more stringent. PHLs that have state regulations governing them in addition tothe federally mandated CLIA regulations are subject to inspections on a regular basis todetermine if they are in compliance with these laws. The CLIA regulations impact all aspects of laboratory operations. One of the biggest changes for PHLs is the regulation for a laboratorydirector. All PHLs function in an organization led by a health officer, but the training andacademic preparation requirements for the role of laboratory director have varied by jurisdiction.In several states, the laboratory director does not need to have a scientific background or an
8/6/2019 Latest Phl
http://slidepdf.com/reader/full/latest-phl 7/27
advanced degree; in others, an advanced degree in a scientific discipline is required. CLIAregulations stipulate that the laboratory director of each PHL must be a physician or a doctoral-level clinical scientist qualified by training, expertise, and experience in the areas of testingoffered by the laboratory. In addition, physicians may qualify to direct a laboratory performinghigh complexity tests (PHLs perform high complexity tests) if they have two years of experience
directing or supervising high complexity testing. The only exceptions to these requirements areunder a grandfather clause that states that those individuals who are qualified or could havequali- fied as director before February 28, 1992, under federal regulations or state law areeligible to function as laboratory director.
State population needs and resources largely dictate the size and complexity of state PHLs interms of staff and test menu. The Lewin Group's report P ublic Health Laboratories and HealthSystem Change , commissioned in 1997 by the United States Department of Health and HumanServices, gives figures that illustrate this diversity. According to this report, in fiscal year 1996the Tennessee state PHL had 186 full-time staff members and a budget of $9.5 million, whereasthe Florida state PHL had 354 full-time staff members and a budget of $21 million.
In addition to the state PHL, many states also have regional, county, or city PHLs that provide aquicker response network, but which may forward some samples to the central state laboratoryfor testing or confirmation of results. The regional laboratories may be extensions of the statePHL or autonomous PHLs funded by the local jurisdiction. For example, Tennessee has four regional state branch laboratories in addition to the central state laboratory located in Nashville.This state PHL organization provides testing services for eighty-nine rural health departmentsand six metropolitan health departments. One regional laboratory has only two staff membersand performs microbiology tests exclusively. In contrast, California operates thirty-nine PHLs inaddition to the state laboratory. All of the local laboratories are autonomous and all but three arecounty health department laboratories. In contrast to this extensive PHL network, other states,such as Oregon and Wyoming, operate only a central state PHL.
Another major difference among state PHLs is the extent to which their resources are utilized intesting primary patient specimens, doing reference testing, training laboratory personnel,monitoring the environment, doing applied research, and functioning as a regulatory agency.Some state laboratories devote a major portion of their resources to direct patient specimentesting; others do very little testing of primary patient specimens and concentrate on referencetesting, applied re- search, and regulatory and epidemiological roles.
Overall, the public health laboratory infrastructure comprises a large number of basically diversefederal, state, and local laboratories that, under the guidance of the CDC, are beginning tofunction as a network in areas of national public health concern such as food safety and
bioterrorism. Individually, however, state PHLs are the major link between national healthinitiatives and delivery at the local level, where laboratory information is mandatory for success.Despite the variability in resource focus and complexity, all state health department laboratorieshave a responsibility to support the core public health functions either directly or in coordinationwith local or regional PHLs.
8/6/2019 Latest Phl
http://slidepdf.com/reader/full/latest-phl 8/27
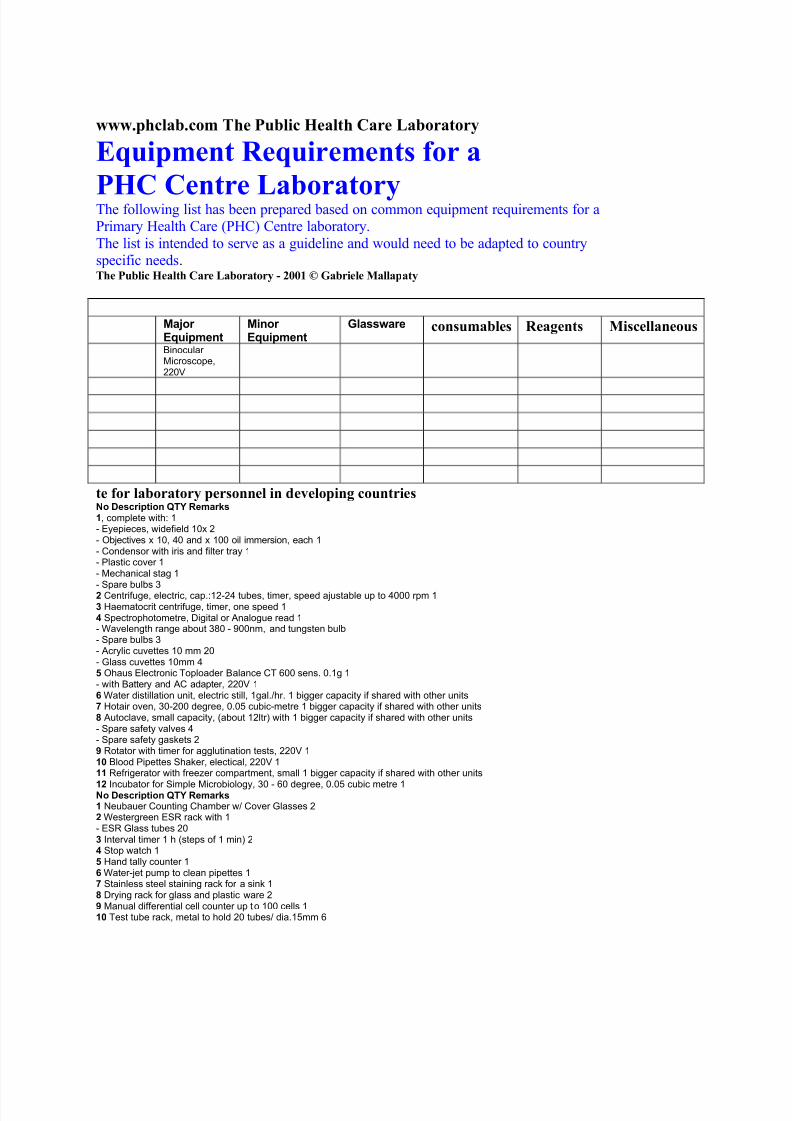
www.ph clab .com T he Public H ealt h Car e Laboratory
Equi pm ent R equir em ents for a
PHC C entr e LaboratoryThe following list has been prepared based on common equipment requirements for aPrimary Health Care (PHC) Centre laboratory.The list is intended to serve as a guideline and would need to be adapted to countryspecific needs .The Public H ealt h Car e Laboratory - 2001 © Gabri ele Malla p aty
Major Equipment
Minor Equipment
Glassware consumabl es R eag ents Misc ellan eousB inocular Microscope,220V
te for laboratory pe rsonn el in d eve lop ing countri esN o Description QTY Remarks1, complete with: 1- Eyepieces, widefield 10x 2- Objectives x 10, 40 and x 100 oil immersion, each 1- Condensor with iris and filter tray 1- Plastic cover 1- Mechanical stag 1
- Spare bulbs 32 Centrifuge, electric, cap.:12-24 tubes, timer, speed ajustable up to 4000 rpm 13 Haematocrit centrifuge, timer, one speed 14 Spectrophotometre, Digital or Analogue read 1- Wavelength range about 380 - 900nm, and tungsten bulb- Spare bulbs 3- Acrylic cuvettes 10 mm 20- Glass cuvettes 10mm 45 Ohaus Electronic Toploader B alance CT 600 sens. 0.1g 1- with B attery and AC adapter, 220V 16 Water distillation unit, electric still, 1gal./hr. 1 bigger capacity if shared with other units7 Hotair oven, 30-200 degree, 0.05 cubic-metre 1 bigger capacity if shared with other units8 Autoclave, small capacity, (about 12ltr) with 1 bigger capacity if shared with other units- Spare safety valves 4- Spare safety gaskets 29 Rotator with timer for agglutination tests, 220V 110 B lood Pipettes Shaker, electical, 220V 111 Refrigerator with freezer compartment, small 1 bigger capacity if shared with other units
12 Incubator for Simple Microbiology, 30 - 60 degree, 0.05 cubic metre 1N o Description QTY Remarks1 Neubauer Counting Chamber w/ Cover Glasses 22 Westergreen ESR rack with 1- ESR Glass tubes 203 Interval timer 1 h (steps of 1 min) 24 Stop watch 15 Hand tally counter 16 Water-jet pump to clean pipettes 17 Stainless steel staining rack for a sink 18 Drying rack for glass and plastic ware 29 Manual differential cell counter up t o 100 cells 110 Test tube rack, metal to hold 20 tubes/ dia.15mm 6
8/6/2019 Latest Phl
http://slidepdf.com/reader/full/latest-phl 9/27
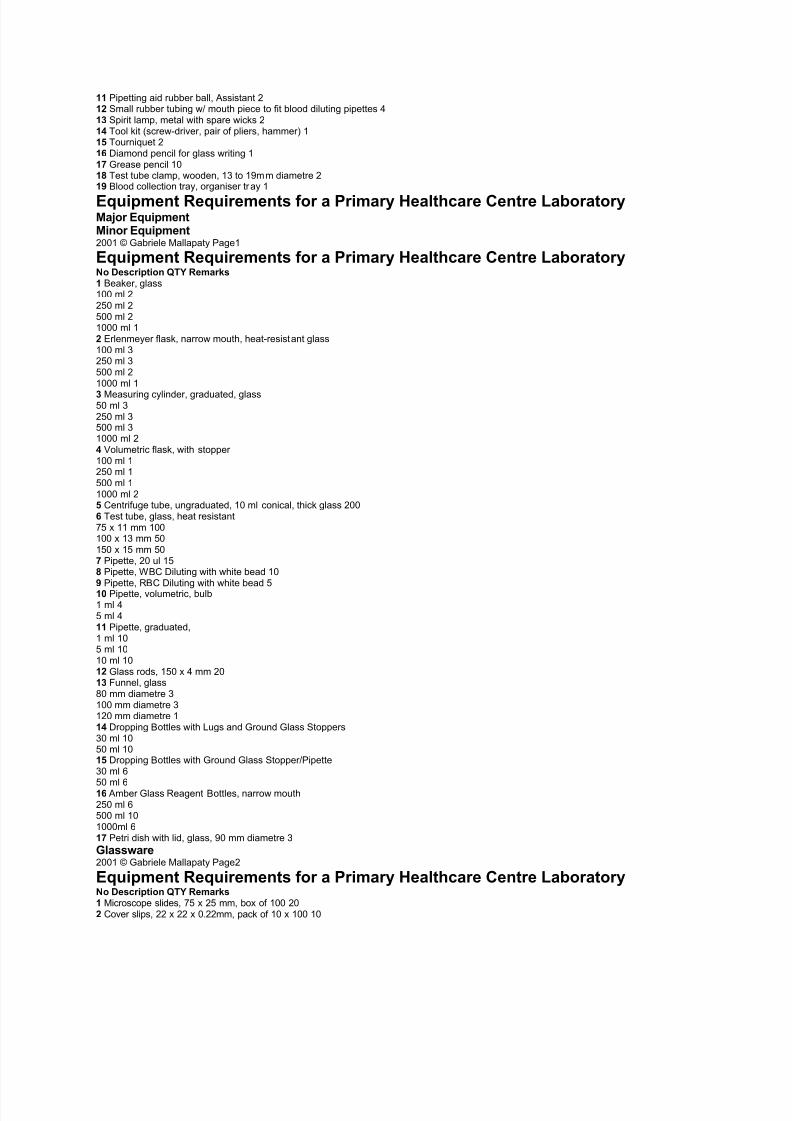
11 Pipetting aid rubber ball, Assistant 212 Small rubber tubing w/ mouth piece to fit blood diluting pipettes 413 Spirit lamp, metal with spare wicks 214 Tool kit (screw-driver, pair of pliers, hammer) 115 Tourniquet 216 Diamond pencil for glass writing 117 Grease pencil 1018 Test tube clamp, wooden, 13 to 19mm diametre 219 B lood collection tray, organiser tr ay 1
Equipment Requirements for a Primary Healthcare Centre LaboratoryMajor EquipmentMinor Equipment2001 © Gabriele Mallapaty Page1
Equipment Requirements for a Primary Healthcare Centre LaboratoryN o Description QTY Remarks1 B eaker, glass100 ml 2250 ml 2500 ml 21000 ml 12 Erlenmeyer flask, narrow mouth, heat-resist ant glass100 ml 3250 ml 3500 ml 21000 ml 13 Measuring cylinder, graduated, glass50 ml 3250 ml 3500 ml 31000 ml 24 Volumetric flask, with stopper 100 ml 1250 ml 1500 ml 11000 ml 25 Centrifuge tube, ungraduated, 10 ml conical, thick glass 2006 Test tube, glass, heat resistant75 x 11 mm 100100 x 13 mm 50150 x 15 mm 507 Pipette, 20 ul 158 Pipette, W B C Diluting with white bead 109 Pipette, R B C Diluting with white bead 510 Pipette, volumetric, bulb1 ml 45 ml 411 Pipette, graduated,1 ml 105 ml 1010 ml 1012 Glass rods, 150 x 4 mm 2013 Funnel, glass80 mm diametre 3100 mm diametre 3120 mm diametre 114 Dropping B ottles with Lugs and Ground Glass Stoppers30 ml 1050 ml 1015 Dropping B ottles with Ground Glass Stopper/Pipette30 ml 6
50 ml 616 Amber Glass Reagent B ottles, narrow mouth250 ml 6500 ml 101000ml 617 Petri dish with lid, glass, 90 mm diametre 3Glassware2001 © Gabriele Mallapaty Page2
Equipment Requirements for a Primary Healthcare Centre LaboratoryN o Description QTY Remarks1 Microscope slides, 75 x 25 mm, box of 100 202 Cover slips, 22 x 22 x 0.22mm, pack of 10 x 100 10
8/6/2019 Latest Phl
http://slidepdf.com/reader/full/latest-phl 10/27
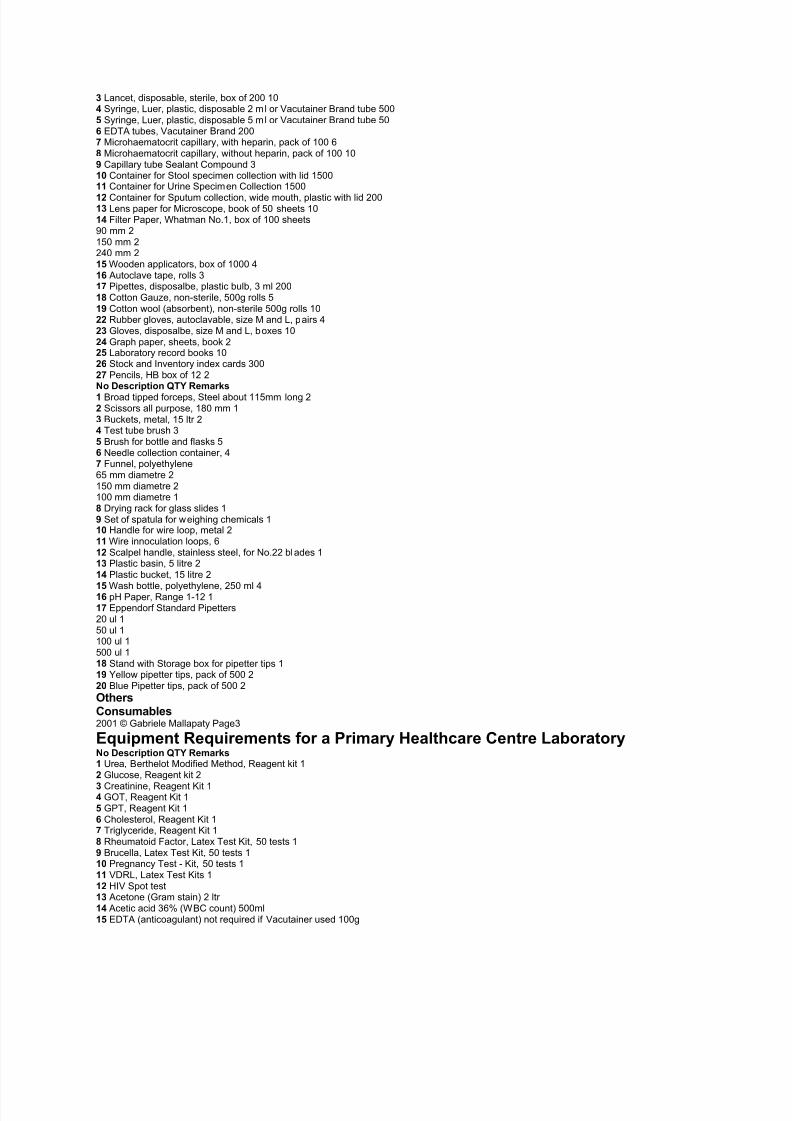
3 Lancet, disposable, sterile, box of 200 104 Syringe, Luer, plastic, disposable 2 ml or Vacutainer B rand tube 5005 Syringe, Luer, plastic, disposable 5 ml or Vacutainer B rand tube 506 EDTA tubes, Vacutainer B rand 2007 Microhaematocrit capillary, with heparin, pack of 100 68 Microhaematocrit capillary, without heparin, pack of 100 109 Capillary tube Sealant Compound 310 Container for Stool specimen collection with lid 150011 Container for Urine Specimen Collection 150012 Container for Sputum collection, wide mouth, plastic with lid 20013 Lens paper for Microscope, book of 50 sheets 1014 Filter Paper, Whatman No.1, box of 100 sheets90 mm 2150 mm 2240 mm 215 Wooden applicators, box of 1000 416 Autoclave tape, rolls 317 Pipettes, disposalbe, plastic bulb, 3 ml 20018 Cotton Gauze, non-sterile, 500g rolls 519 Cotton wool (absorbent), non-sterile 500g rolls 1022 Rubber gloves, autoclavable, size M and L, pairs 423 Gloves, disposalbe, size M and L, boxes 1024 Graph paper, sheets, book 225 Laboratory record books 1026 Stock and Inventory index cards 30027 Pencils, H B box of 12 2N o Description QTY Remarks1 B road tipped forceps, Steel about 115mm long 22 Scissors all purpose, 180 mm 13 B uckets, metal, 15 ltr 24 Test tube brush 35 B rush for bottle and flasks 56 Needle collection container, 47 Funnel, polyethylene65 mm diametre 2150 mm diametre 2100 mm diametre 18 Drying rack for glass slides 19 Set of spatula for weighing chemicals 110 Handle for wire loop, metal 211 Wire innoculation loops, 612 Scalpel handle, stainless steel, for No.22 bl ades 113 Plastic basin, 5 litre 214 Plastic bucket, 15 litre 2
15 Wash bottle, polyethylene, 250 ml 416 pH Paper, Range 1-12 117 Eppendorf Standard Pipetters20 ul 150 ul 1100 ul 1500 ul 118 Stand with Storage box for pipetter tips 119 Yellow pipetter tips, pack of 500 220 B lue Pipetter tips, pack of 500 2OthersConsumables2001 © Gabriele Mallapaty Page3
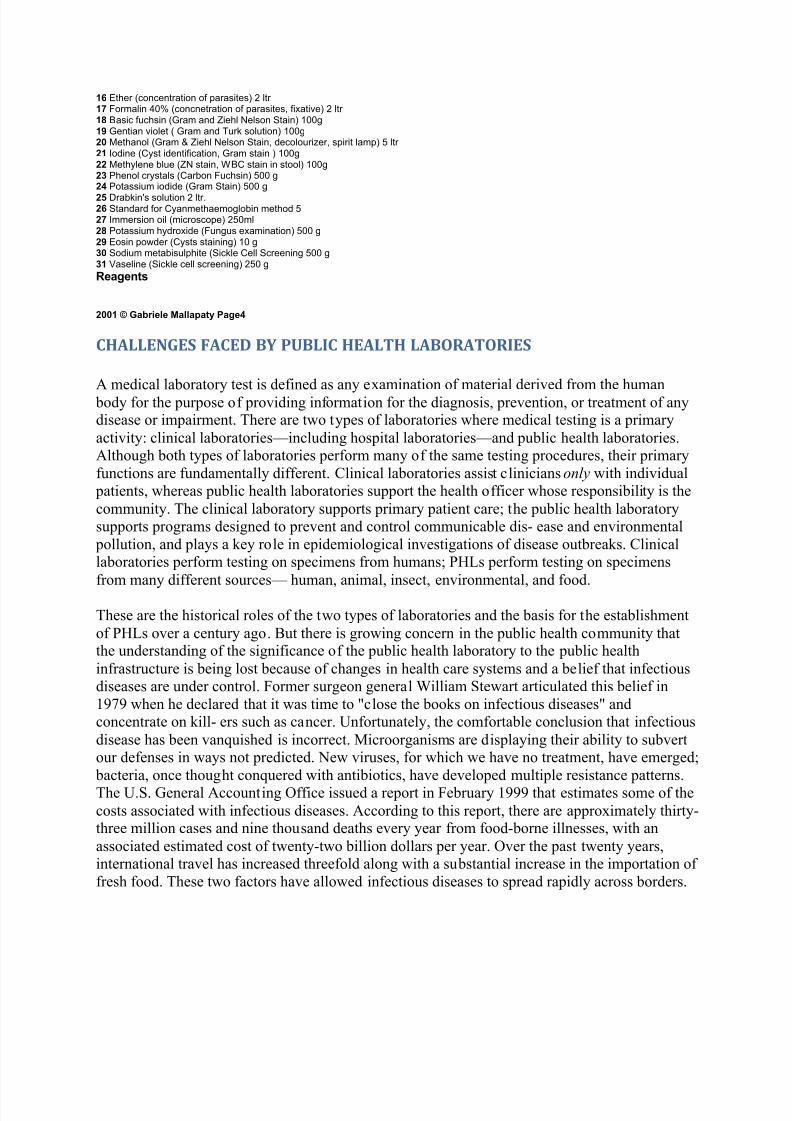
Equipment Requirements for a Primary Healthcare Centre LaboratoryN o Description QTY Remarks1 Urea, B erthelot Modified Method, Reagent kit 12 Glucose, Reagent kit 2
3 Creatinine, Reagent Kit 14 GOT, Reagent Kit 15 GPT, Reagent Kit 16 Cholesterol, Reagent Kit 17 Triglyceride, Reagent Kit 18 Rheumatoid Factor, Latex Test Kit, 50 tests 19 B rucella, Latex Test Kit, 50 tests 110 Pregnancy Test - Kit, 50 tests 111 VDRL, Latex Test Kits 112 HIV Spot test13 Acetone (Gram stain) 2 ltr 14 Acetic acid 36% (W B C count) 500ml15 EDTA (anticoagulant) not required if Vacutainer used 100g
8/6/2019 Latest Phl
http://slidepdf.com/reader/full/latest-phl 11/27
16 Ether (concentration of parasites) 2 ltr 17 Formalin 40% (concnetration of parasites, fixative) 2 ltr 18 B asic fuchsin (Gram and Ziehl Nelson Stain) 100g19 Gentian violet ( Gram and Turk solution) 100g20 Methanol (Gram & Ziehl Nelson Stain, decolourizer, spirit lamp) 5 ltr 21 Iodine (Cyst identification, Gram stain ) 100g22 Methylene blue (ZN stain, W B C stain in stool) 100g23 Phenol crystals (Carbon Fuchsin) 500 g24 Potassium iodide (Gram Stain) 500 g25 Drabkin's solution 2 ltr.26 Standard for Cyanmethaemoglobin method 527 Immersion oil (microscope) 250ml28 Potassium hydroxide (Fungus examination) 500 g29 Eosin powder (Cysts staining) 10 g30 Sodium metabisulphite (Sickle Cell Screening 500 g31 Vaseline (Sickle cell screening) 250 gReagents
2001 © Gabriele Mallapaty Page4
CHALLENGES FACED BY PUBLIC HEALTH LABORATORIES
A medical laboratory test is defined as any examination of material derived from the human body for the purpose of providing information for the diagnosis, prevention, or treatment of anydisease or impairment. There are two types of laboratories where medical testing is a primaryactivity: clinical laboratories²including hospital laboratories²and public health laboratories.Although both types of laboratories perform many of the same testing procedures, their primaryfunctions are fundamentally different. Clinical laboratories assist clinicians only with individual
patients, whereas public health laboratories support the health officer whose responsibility is thecommunity. The clinical laboratory supports primary patient care; the public health laboratorysupports programs designed to prevent and control communicable dis- ease and environmental
pollution, and plays a key role in epidemiological investigations of disease outbreaks. Clinicallaboratories perform testing on specimens from humans; PHLs perform testing on specimensfrom many different sources² human, animal, insect, environmental, and food.
These are the historical roles of the two types of laboratories and the basis for the establishmentof PHLs over a century ago. But there is growing concern in the public health community thatthe understanding of the significance of the public health laboratory to the public healthinfrastructure is being lost because of changes in health care systems and a belief that infectiousdiseases are under control. Former surgeon general William Stewart articulated this belief in1979 when he declared that it was time to "close the books on infectious diseases" andconcentrate on kill- ers such as cancer. Unfortunately, the comfortable conclusion that infectiousdisease has been vanquished is incorrect. Microorganisms are displaying their ability to subvertour defenses in ways not predicted. New viruses, for which we have no treatment, have emerged;
bacteria, once thought conquered with antibiotics, have developed multiple resistance patterns.The U.S. General Accounting Office issued a report in February 1999 that estimates some of thecosts associated with infectious diseases. According to this report, there are approximately thirty-three million cases and nine thousand deaths every year from food-borne illnesses, with anassociated estimated cost of twenty-two billion dollars per year. Over the past twenty years,international travel has increased threefold along with a substantial increase in the importation of fresh food. These two factors have allowed infectious diseases to spread rapidly across borders.
8/6/2019 Latest Phl
http://slidepdf.com/reader/full/latest-phl 12/27
In addition to the incorrect premise that infectious disease has been conquered, rapid changes inthe health care environment have profoundly affected traditional services delivered by PHLs.
Until the early 1970s, PHLs were the leaders in microbiology technology. The CDC scientific re-search laboratories developed improved assays for various organisms and transferred the
technology to the PHLs. In turn, the PHLs functioned as training centers for the private clinicallaboratory staff. This function, in conjunction with their reference service ability, gave PHLs anelevated status in the community. This status began to erode as private companies entered the
biological research and development market. No longer was CDC the leader in reagent andtechnology development. Biotechnology companies began emerging at a rapid pace as the
potential market for improved diagnostic technology became apparent. These companies selldirectly to private clinical laboratories, supplying any necessary training along with the newtechnology. PHLs are no longer the conduit. In addition, private clinical laboratories, because of the highly competitive marketplace in which they operate, have surpassed most PHLs in servicesand information infrastructure.
These changing dynamics of the laboratory services marketplace accelerated during the 1990swith the growth of managed care, consolidation of laboratories, shrinking of public resources,and the direct competition of clinical laboratories. While more sophisticated technology hasraised testing costs, managed care organizations (MCOs) and other providers have demandedthat laboratories lower their fees for service. This has served to intensify competition amonglaboratories and stimulated a quest for more efficient and faster service modes. In general the
private laboratories that have survived this competitive pressure have decreased their coststhrough economies of scale, increased their capacity for quick turnaround of results, anddeveloped better information handling. PHLs have been slow in responding to the need tochange, partially because of the resource issues, but also because of bureaucratic inertia. Theresult is a continuing erosion of stature and a decreasing volume of testing, with a perceived lossin surveillance data for community protection.
FUTURE OF PUBLIC HEALTH LABORATORIES
Image, in the form of perceived importance, is the key to the survival of the public healthlaboratory system. PHLs must be understood and viewed by the public, by public officials, and
by the private sector laboratory professionals as an invaluable resource that contributes in aunique way to the maintenance of health in the population. PHLs must be responsive to changingneeds and once again become technological leaders of the laboratory community.
At present, the public health laboratory system is composed of autonomous laboratories linked at
the state level, and linked at the federal level to CDC, but not linked to each other or to privatediagnostic laboratories. The concept of forming a true national laboratory network, comprised of both private and public laboratories, originated in the late 1960s and is being expressed in arudimentary way through bioterrorism initiatives and national surveillance for food-bornediseases, antimicrobial resistance patterns, and emerging infectious disease concerns. Tocontinue the momentum to build a strong national network and to focus public awareness on theintegral role of public health laboratories in such a system, the Association of Public HealthLaboratories (APHL) is developing a strategic plan that will encompass elements of public
8/6/2019 Latest Phl
http://slidepdf.com/reader/full/latest-phl 13/27
relations as well as the objectives and steps involved in the development of a national laboratorysystem. This is a difficult and momentous undertaking, yet it is essential to the provision of health protection at the national as well as at the local level. A critical role for the public healthlaboratory is to provide the leader- ship and initiative to create this vital laboratory system.
SYDNE
Y M. HARVE
Y
(SEE ALSO: Assurance of Laboratory Testing Quality ; Centers for Disease Control and P revention ; Clinical Laboratories Improvement Act ; Laboratory Technician ; Reference Laboratory ; Research in P ublic Health Laboratories ; Screening )
BIBLIOGRAPHY
Association of Public Health Laboratories (1999). Core Functions and Capabilities of State P ublic Health Laboratories. Washington, DC: Author.
Cordts, J. R. (1995). "The Laboratory as a Model Public Health Function." CDC/NCID Focus (March).
Duffy, J. (1996). The Sanitarians: A History of American P ublic Health. Urbana: University of Illinois Press.
Getchell, J. P. (1996). "The Role of the Public Health Laboratory and the Definition of PublicHealth Laboratory Services." The Nation's Health (September):19±21.
Lewin Group (1997). P ublic Health Laboratories and Health System Change.
Skeels, M. R. (1995). "Public Health Laboratories Build Healthy Communities." Laboratory Medicine 26:588±592.
U.S. Senate Subcommittee on Public Health (1999). Emerging Infectious Diseases: Consensuson Needed Laboratory Capacity Could Strengthen Surveillance. Washington, DC: GeneralAccounting
PR E AMBL E
ORGANISATIONAL STRUCTUR E
8/6/2019 Latest Phl
http://slidepdf.com/reader/full/latest-phl 14/27
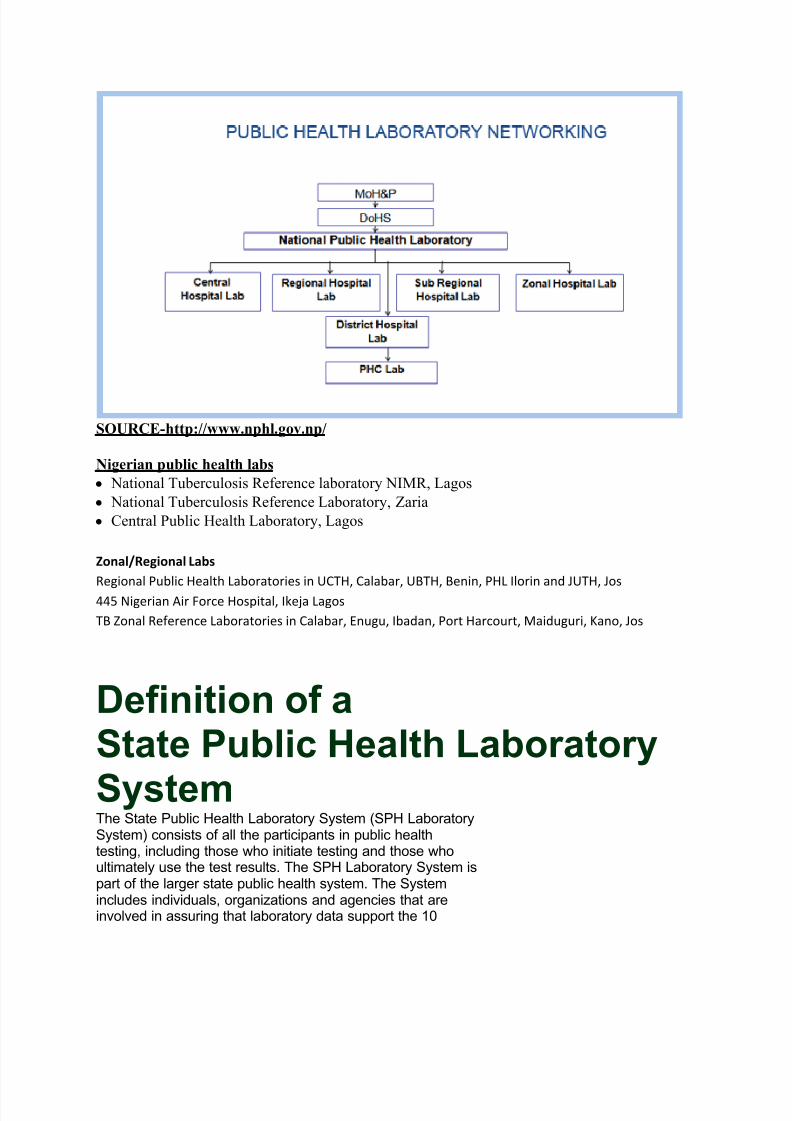
SOURCE- h tt p://www. n ph l.gov. n p/
Nig erian p ublic he alt h labsy National Tuberculosis Reference laboratory NIMR, Lagosy National Tuberculosis Reference Laboratory, Zariay Central Public Health Laboratory, Lagos
Zonal/Regional Labs Regional Public Health Laboratories in UCTH, Calabar, UBTH, Benin, PHL Ilorin and JUTH, Jos445 Nigerian Air Force Hospital, Ikeja LagosTB Zonal Reference Laboratories in Calabar, Enugu, Ibadan, Port Harcourt, Maiduguri, Kano, Jos
Definition of aState Public Health LaboratorySystemThe State Public Health Laboratory System (SPH LaboratorySystem) consists of all the participants in public healthtesting, including those who initiate testing and those whoultimately use the test results. The SPH Laboratory System ispart of the larger state public health system. The Systemincludes individuals, organizations and agencies that areinvolved in assuring that laboratory data support the 10
8/6/2019 Latest Phl
http://slidepdf.com/reader/full/latest-phl 15/27
Essential Services of Public Health. The concepts of a SPHLaboratory System are also embodied in the APHL CoreFunctions and Capabilities of State Public Health Laboratories.These documents are available on the APHL website atwww.aphl.org. Within the SPH Laboratory System areprimary stakeholders who are directly involved in creatingand using laboratory data. Additional stakeholders includethose who are concerned with complementary Essential Services,such as Training and Education and Public HealthRelated Research. A successful National Laboratory System isdependent on the creation of fully integrated and coordinatednetworks in every state. The goals of the National LaboratorySystem are to support voluntary, interdependent partnershipsof clinical, environmental, agricultural and veterinary laboratoriesthrough public-private collaboration, for assurance of quality laboratory services and public health surveillance.The SPH Laboratory System should assure that:1. public health threats are detected and intervention istimely2. stakeholders are appropriately informed of potentialthreats3. reportable conditions are monitored in a comprehensivestatewide system4. specimens and isolates for public health testing are sufficientto provide comprehensive public health surveillanceand response5. public health laboratory data are transmitted to appropriatestate and federal agencies responsible for diseasesurveillance and control.A ssociation of Public Health Laboratories June 2007The state public health laboratory (SPHL) has a leadershiprole in developing and promoting the SPH LaboratorySystem through active collaboration with stakeholders,including epidemiologists; first responders; environmentalprofessionals in water, food and air surveillance activities;private clinical and environmental laboratories; and localpublic health laboratories. The SPHL provides leadership toassure that essential and state-of-the-art laboratory servicesare provided and that clinical laboratories that perform publichealth testing on reportable infectious diseases submit resultsto the public health surveillance system using national testingguidelines. To provide leadership, the SPHL monitors essential
components of the SPH Laboratory System, such ascompleteness of reporting and accuracy of laboratory testingresults. The SPHL also assures that accurate results arereported in a manner that is appropriate and sufficientlytimely for effective public health response. An effective SPHLaboratory System requires proactive leadership by the SPHLto monitor public health testing processes by clinical andenvironmental in-state laboratories. To assure that the SPHLaboratory System is effective, the SPHL should at a
8/6/2019 Latest Phl
http://slidepdf.com/reader/full/latest-phl 16/27
minimum:1.maintain an integrated information system that includesall stakeholders that rely on accurate laboratory data2.employ a full-time public health laboratory system coordinator 3.create a standing public health laboratory advisorycommittee4.provide an interactive website or other electronic systemto maintain regular communication channels for systempartners.This document was developed by a subcommittee of the APHLLaboratory Systems & Standards Committee. It was adopted by the APHL Board on May 24, 2007.
THE CORE FUNCTIONS OF STATEPUBLIC HEALTHLABORATORIES Revised in 2010
The core functions of state public health laboratories were first adopted and published by APHL in 2000. This revision of the original document was createdin order to update and standardize the description of each core functionand to reflect the changes that have occurred since 2000 with respect to state
public health laboratory systems.A PHL Cor e Functions R ev ision Workgrou p Burton Wilcke, Jr., PhD, Chair (VT)Modupe Osinubi, DVM, PhD (APHL/CDC International E mergingInfectious Diseases Fellow)Rodger Silletti, PhD, D(ABMM) (Nassau County)Bertina Su, MPH (APHL)
Paula (Snippes) Vagnone, MT(ASCP) (MN)Anne Weber, MS (MT)APHL thanks Carol Fridlund, MT(ASCP), and Celine Taboy, PhD, of theLaboratory Systems Development Branch, Centers for Disease Control andPrevention, for their contributions and support to this project.This publication was supported by Cooperative Agreement Number #U60/CD303019 from Centers for Disease Control and Prevention(CDC). Its contents are solely the responsibility of the authorsand do not necessarily represent the official views of CDC.©2010 by the Association of Public Health Laboratories.Core Functions of State Public Health Laboratories 1
B ackgroundAccording to the Institute of Medicine (IOM) report, The Future of P ublic Health, published in 1988, ³Public health is what we, as a society, do collectivelyto assure the conditions in which people can be healthy.´ 1 This definitionof public health and its overarching core functions, (i.e., assessment,
policy development and assurance), which were identified in that report,have led to further descriptions of the many important components of
public health. The authors of the 1988 IOM report felt that only if public
8/6/2019 Latest Phl
http://slidepdf.com/reader/full/latest-phl 17/27
health is clearly defined and understood would it be adequately supported.In 1994, E dward L. Baker et al. published the results of a working groupthat described the 10 essential public health services. 2 These services have
provided the framework for a national public health performance standardssystem 3 that measures the performance of state and local public health
agencies. The extent to which these state and local public health agencies provide comprehensive services, such as laboratory services in support of the 10 essential public health services, has been the major focus of thenational public health performance standards.In 2000, the Association of Public Health Laboratories (APHL) developeda white paper entitled Core Functions and Capabilities of State P ublic Health
Laboratories. The 11 core functions of state public health laboratories weresubsequently published in Morbidity and Mortality Weekly Report in 2002. 4 Areport that followed several years later demonstrated how state public healthlaboratories, through their core functions, support the 10 essential publichealth services. 5 Since 2002, it has become clear that a broader, inclusive State
Public Health (SPH) Laboratory System is more effective in assuring that1. Institute of Medicine, The Future of Public Health (Washington, DC: National Academy Press): 1988.2. E dward L. Baker, et al., ³Health Reform and the Health of the Public,´ Journal of the American Medical Association 272 (1994): 1276-823. ³National Public Health Performance Standards Program (NPHPSP)´ National Public Health Performance Standa rds Program (NPHPSP),http://www.cdc.gov/od/ocphp/nphpsp/4. Joyce Witt-Kushner, et al., ³Core Functions and Capabilities of State Public Health Laboratories: a Report of the Association of PublicHealth Laboratories,´ Morbidity and Mortality Weekly Report 51(2002):1-8.5 Burton W. Wilcke, Jr., et al., ³Tracking Laboratory Infrastructure in Support of Public Health,´ (presentation, 135th American Public HealthAssociation Annual Meeting and E xposition, Washington, D.C., November 3-7, 2007).2 Core Functions of State Public Health Laboratories
the core functions are fulfilled. 6 Within the last decade, work has been donein measuring the laboratory infrastructure in support of the essential publichealth services, creating performance standards for public health entities,identifying public health workforce needs and addressing quality systems asthey apply to public health laboratory services.As we move into the 21 st century, these 11 core functions of state publichealth laboratories remain unchanged. However, what has emerged is therealization that laboratory services in support of public health are dependentupon synergistic and effective interactions among many different partners atthe state and national level. This revision of the Core Functions of State P ublic
Health Laboratories more clearly defines the responsibilities of the StatePublic Health Laboratory (SPHL) within the SPH Laboratory System.Just as the onset of the Human Immunodeficiency Virus epidemic of the1980s highlighted the important role of SPHLs in a public health crisis, theanthrax attacks of 2001 and the influenza pandemic of 2009 further accentuatedthe role of SPHLs as key players in public health emergencies. Numerousexamples of SPHLs¶ contributions have played out over the last decade,including the characterization of the E. coli spinach outbreak of 2006, theexpansion of life-saving testing assays in newborn screening, and the morerecent involvement of SPHLs in environmental and food testing in responseto the Gulf oil spill of 2010. These events reinforce the necessity of having analliance of laboratories and other partners that collectively make up the publichealth laboratory system in each state. The response to these events changedthe dynamic in the state laboratory system and positively influenced the
8/6/2019 Latest Phl
http://slidepdf.com/reader/full/latest-phl 18/27
building of relationships between public and private laboratories.In its role to assure that the 11 core functions are carried out, the SPHLengages the entire healthcare community to varying degrees in a partnershipthat has come to be called the SPH Laboratory System. The SPH Laboratory6. Stan L. Inhorn, et al., ³The State Public Health Laboratory System,´ Public Health Reports 125 Supplement 2 (2010): 4-17.Core Functions of State Public Health Laboratories 3
System is defined as ³an alliance of laboratories and other partners withina state that supports the 10 essential public health services under the aegisof the state public health laboratory. The system members and stakeholdersoperate in an interconnected and interdependent way to facilitate theexchange of information, optimize laboratory services, and help control and
prevent disease and public health threats.´ The SPHL has a leadership rolein developing and promoting the SPH Laboratory System as well as assuringthat essential and state-of-the-art laboratory services are provided. SPHLaboratory Systems, in the most general terms, consist of all the participantsin public health testing, including those who initiate testing and those whoultimately use the test results. 7 The specific makeup of the ³system´ varies
by state, but typically includes the state public health laboratory and the local public health laboratories in that state. In addition, the system may includeclinical, environmental, veterinary, and agricultural laboratories as well asother governmental, non-private, or private facilities, performing laboratorytesting of public health significance. In addition, the system includes partnersthat rely on laboratory test results to inform specific public health programsor responses. The laboratory community as a whole benefits from stronger linkages between all stakeholders. Strengthening state public healthlaboratory systems is, therefore, a key component to strengthening theoverall National Laboratory System in support of improved healthoutcomes and preparedness activities.
The 11 core functions provide a foundation for measurement of a varietyof SPHL quality systems goals. One example is the re-established HealthyPeople 2020 laboratory objective (Healthy People 2010, objective 23-13)to ³increase the proportion of tribal and state public health agencies that
provide or assure comprehensive laboratory services to support essential public health services,´ and the newly established objective to ³increase the7. ³Definition of a State Public Health Laboratory System,´ Association of Public Health Laboratories, http://www.aphl.org/aphlprograms/lss/
projects/performance/Documents/Definition_of_a_state_public_health_laboratory_system_June2010.pdf 4 Core Functions of State Public Health Laboratories
proportion of public health laboratory systems (including state, tribal, andlocal) that perform at a high level of quality in support of the 10 essential
public health services.´ The Comprehensive Laboratory Services Survey 8
(CLSS), created by a committee of APHL in collaboration with the Centersfor Disease Control and Prevention (CDC) and distributed biennially, is basedon the 11 core functions. Given that the term ³comprehensive laboratory services´was not defined in Healthy People 2010, APHL adopted the positionthat such services reflect the full range of activities, not just analytical services,which are carried out by SPHLs and their system partners. In effect, APHLconcluded that the fulfillment of all 11 core functions represented the provisionof ³comprehensive laboratory services to support essential public healthservices.´ The CLSS was created to measure the extent to which state public

8/6/2019 Latest Phl
http://slidepdf.com/reader/full/latest-phl 19/27
health laboratories were meeting the Healthy People 2010 objective and willalso be used to measure the Healthy People 2020 objective. Since the baselinesurvey in 2006, it has been demonstrated that state public health laboratorieshave essentially met or exceeded the targets for some core functions (such asdisease surveillance and reference testing) but were in need of improvement
in other areas (such as food safety, as well as training and education).Additionally, this core functions document, along with the 10 essential public health services document, provides the basis for the LaboratorySystem Improvement Program (L-SIP). 9 L-SIP was first implemented in2006 10 as a means for all states¶ system stakeholders to measure system
performance, plan system improvements, implement improvement strategies,and periodically evaluate and reassess while continuously focusing onthe goal of quality improvement. Finally, the core functions could well drivethe development of standards that could be used for public health laboratoryaccreditation purposes.8. Burton W. Wilcke, Jr., et al. ³Laboratory Services in Support of Public Health: A Status Report,´ Public Health Reports 125 Supplement 2(2010): 40-46.9. ³Promoting System Improvement, ´ Association of Public Health Laboratories, http://www.aphl.org/aphlprograms/lss/projects/performance/
Pages/default.aspx10. Kathleen C. Milne and Thomas L. Milne, ³Public Health Laboratory System Improvement Program: Development and Implementation,´Public Health Reports 125 Supplement 2 (2010): 31-39.Core Functions of State Public Health Laboratories 5
This document represents an updated perspective on the 11 core functions.For example, the renamed ³Public Health Preparedness and Response´ corefunction now incorporates the multiple Laboratory Response Networks.³Public Health Related Research´ is given greater emphasis, challenging the
public health laboratory community to support innovative research in thearea of public health laboratory systems and services. The future of publichealth laboratory practice is dependent upon new and progressive ways of defining and showcasing the value and importance of SPHLs and the SPHLaboratory Systems they lead. This document also supports a greater role inadvocacy and outreach for SPHLs, consistent with APHL¶s strategic plan.In summary, this revised document emphasizes the reality that the SPHLaboratory System²and not the SPHL alone²is responsible for assuringlaboratory services in support of public health. It is acknowledged that SPHLaboratory Systems vary significantly, ranging from small state systemswith no local laboratories and relatively few partners to large, complex statesystems with regional laboratories, many county laboratories and multiple
partners. Regardless of the structure of the individual SPH LaboratorySystem, the SPHL plays a central role in providing or assuring throughits system partners the full range of laboratory services required insupport of public health.6 Core Functions of State Public Health Laboratories
The Eleven Core Functions of State PublicHealth Laboratories 11
Dis eas e Pr eve ntion, Control and Sur ve illanc e Int egrat ed Data Manag em entR ef er enc e and S pe cializ ed T estingEn vironm ental H ealt h and Prot ection
8/6/2019 Latest Phl
http://slidepdf.com/reader/full/latest-phl 20/27
Food Saf etyLaboratory Im pro ve ment and R egulationPolicy D eve lop mentPublic H ealt h Pr ep ar edn ess and R espons e Public H ealt h R elat ed R esearc h Training and EducationPartn ers hips and Communication
Descriptions of the eleven core functions are following:11. Not listed in order of priority or importance.Core Functions of State Public Health Laboratories 7
Disease Prevention, Control and Surveillance Provide accurate and precise analytical data in a timely manner insupport of the:
Prevention and control of infectious, communicable, genetic andchronic diseases, and environmental exposure. This may includetesting for emerging and re-emerging microbial agents, immune
status, antibiotic resistance, screening for inherited neonatalmetabolic disorders, environmental toxins, and heavy metalssuch as blood lead.
Recognition of outbreaks and other events of public healthsignificance, by the identification and characterization of thecausative agents of disease and their origin.
Population-based surveillance for conditions of public healthimportance and to guide programmatic decisions. E arly detection of congenital disorders in newborns leading to timely
diagnosis and treatment.Monitoring of low incidence and/or high risk diseases, such as
antibiotic-resistant tuberculosis, influenza, botulism and rabies.Investigation and control of communicable or environmentaldiseases when testing is not available in the private sector.8 Core Functions of State Public Health Laboratories
Integrated Data Management Serve as the conduit for scientific data and information in support of public health programs through the:
Capturing of laboratory data essential for public healthanalysis and decision making, including detecting trendsand sentinel events.
Use of standardized data formats.Influencing public health policy.Participation in statewide disease reporting networks.Linkage with CDC and other national and international
surveillance databases.Collaboration with state and national laboratory systems.Continuous improvement of laboratory data systems.
Core Functions of State Public Health Laboratories 9
Reference and Specialized Testing Serve as centers of excellence using their expertise, reference and resources
8/6/2019 Latest Phl
http://slidepdf.com/reader/full/latest-phl 21/27
in the areas of biological, chemical and radiologic issues of public healthimportance to:
Support the diagnosis of and surveillance for unusualand emerging pathogens.
Confirm atypical laboratory test results.
Verify results of other laboratories¶ tests.Provide reference services to laboratories that may not havethe capability to fully identify disease agents of publichealth importance.
Provide diagnostic testing for diseases of public health importancedirectly to providers when testing is not readily available.
Test for diseases of public health importance that are too rareand unusual for other laboratories to maintain capacity.10 Core Functions of State Public Health Laboratories
Environmental Health and ProtectionCollaborate with partners to coordinate and ensure scientific analysisof environmental and human samples to identify, quantify and monitor potential threats to health by:
Testing for toxic chemical, radiological, and microbiological contaminantsin air, water, soil and hazardous waste.
Conducting biomonitoring of human specimens in the assessment of toxic chemical exposure.
Testing of environmental samples in support of federal and state regulations,aiding in the compliance with those regulations.
Industrial hygiene/occupational health testing to assist in efforts to protect indoor air quality and worker health, such as routine analysis of asbestos, lead, pesticides and radon.
Participating in the Chemical Laboratory Response Network (LRN-C)and the E nvironmental Response Laboratory Network ( E RLN).Core Functions of State Public Health Laboratories 11
Food SafetyCollaborate in the detection, monitoring, and response to food safetyissues by:
Testing samples from persons, food and beverages implicatedin food-borne illness outbreaks to detect and identify potentialfood-borne pathogens.
Characterizing isolates and participating in national straincharacterization databases, such as PulseNet, to informepidemiologic investigations.
Analyzing food specimens to detect, identify and quantify toxiccontaminants such as pesticide residues, heavy metals andvolatile organic compounds.
Monitoring for radioactive contamination.Participating in the Food E mergency Response Network (F E RN).
12 Core Functions of State Public Health Laboratories
Laboratory Improvement and Regulation Provide leadership for laboratory improvement in areas of public health
8/6/2019 Latest Phl
http://slidepdf.com/reader/full/latest-phl 22/27
importance by:Promoting quality improvement programs for partner laboratories
through activities such as training, consultation, and proficiency testing.
Developing and overseeing statewide laboratory improvement
programs to ensure the reliability of laboratory data used for environmental monitoring and communicable diseasesurveillance and control.
Promoting safe laboratory practice through education, training,and consultation.
Assessing and improving the State Public Health LaboratorySystem by implementing the Laboratory SystemImprovement Program (L-SIP).
Guiding the creation of and supporting enforcement of regulations and laws that contribute to laboratory improvement.Core Functions of State Public Health Laboratories 13
Policy Development Play a role in the development of state and federal health policy by:
Generating scientific evidence that informs public health practice and law.
Monitoring the impact of public health laboratory practice onhealth outcomes.
Serving as centers of expertise, reference and resources inthe areas of biological, chemical and radiologic issues of
public health importance.Participating in the development and evaluation of standards
related to the operation and performance of laboratories involvedin public health testing.
Advocating for the use of sound reasoning in the application of laboratory science and system infrastructure sustainment. E ngaging in strategic planning at local, state and national levels.
14 Core Functions of State Public Health Laboratories
Public Health Preparedness and ResponseFulfill a key partnership role in local, state and national disaster
preparedness and response by:Functioning as a Laboratory Response Network (LRN)
Reference laboratory for biological agents and as an LRNChemical Laboratory at a level designated by CDC.
Assuring the triaging of environmental samples for the rapididentification of threat agents (chemical, biological, radiological,and nuclear ± CBRN); and food samples as a part of the FoodE mergency Response Network (F E RN).
Planning for and ensuring that surge capacity is available duringa public health emergency.
Having a Continuity of Operations Plan in the event of adisruption of laboratory services.
Participating in the E nvironmental Response Laboratory
8/6/2019 Latest Phl
http://slidepdf.com/reader/full/latest-phl 23/27
Network ( E RLN).Core Functions of State Public Health Laboratories 15
Public Health Related Research Engage in research to improve and expand the scientific and policy basisof public health laboratory practice and assure their optimal application
in support of the public health system by:Developing, evaluating and implementing new technologiesand methodologies.
Partnering with other public health disciplines.Collaborating with academic institutions to carry out clinical
and translational science.Conducting public health systems and service research.Working with the private sector to foster scientific innovation.
16 Core Functions of State Public Health Laboratories
Training and EducationFacilitate access to training and education by:
Sponsoring training opportunities to improve scientific andtechnical skills within the public health laboratory system.
Supporting management and leadership development opportunities.Participating in the training of both domestic and
international scientists.Partnering with academia to provide experiential learning
opportunities.Providing continuing education in the area of laboratory practice.
Core Functions of State Public Health Laboratories 17
Partnerships and Communication Support their respective state public health laboratory systems by:
Highlighting the importance of laboratory contributions in supportof public health.
Maintaining a strong communication plan that links allsystem partners.
Utilizing information technology for robust connectivity. E ngaging traditional and non-traditional partners.Coordinating activities through the use of a laboratory program
advisor, (i.e., laboratory system coordinator).Linking the SPH Laboratory System to appropriate national
surveillance networks.18 Core Functions of State Public Health Laboratories
Association of Public Health Laboratories
8515 Georgia Avenue Suite 700 Silver Spring, MD 20910Phone: 240.485.2745 Website: www.aphl.org E-mail: [email protected]
8/6/2019 Latest Phl
http://slidepdf.com/reader/full/latest-phl 24/27
Laboratory A ccreditationChecklistFor Clinical and Public Health LaboratoriesSOURCE- W HO AFRO Accreditation Checklist, December 2009
AFRO-AFRICA REGIONAL OFFICE 1.0 I N TRODUCTIO N Laboratory services are an essential component in the diagnosis and treatment of personsinfected with the humanimmunodeficiency virus (HIV), malaria, Mycobacterium tuberculosis (MTB )., sexuallytransmitted infections, and other infectious diseases. Presently, the laboratory infrastructure and test quality for all types of clinical laboratories remains
weak in most countries in Africa. There is therefore an urgent need to strengthen laboratoryservices and systems.The establishment of an accreditation scheme is a valuable tool for countries to use toimprove, and strengthen thecapacity and quality of services of their laboratories.To strengthen laboratory systems of its member countries in a stepwise fashion, WHO-
AFRO has established anaccreditation scheme in accordance with its core functions of setting norms and standardsand building institutionalcapacity. Accreditation provides documentation that the laboratory has the capability andthe capacity to detect,identify, and promptly report all diseases of public health significance that may be present inclinical and researchspecimens. This is also in line with Resolution AFR/RC58/R2 on Public Health LaboratoryStrengthening adopted bythe Member States during the 58 th session of the Regional Committee in September 2008 inYaoundé, Cameroon, andthe Maputo Declaration to strengthen laboratory systems. The accreditation process further provides a learningopportunity, a pathway for continuous improvement, a mechanism for identifying resourceand training needs, ameasure of progress, and a link to the WHO-AFRO National Health Laboratory ServiceNetworks.
Accreditation of clinical and public health, and reference laboratories is reviewed annuallyby WHO AFRO and is basedon laboratory performance during the immediately preceding 12 months relying on completedata, usually from thepast 1-13 months to 1 month prior to evaluation. Accreditation is given for the upcomingcalendar year.2.0 Scope
8/6/2019 Latest Phl
http://slidepdf.com/reader/full/latest-phl 25/27
This checklist specifies requirements for quality and competency aimed to develop andimprove laboratory services toraise quality to uniform national standards using a tiered WHO AFRO Accreditation scheme.The elements of this checklist are based on ISO standard 15189:2007(E) and, to a lesser extent, CLSI guidelineGP26-A3.W HO AFRO Accreditation Checklist, December 2009 23.0 Criteria for A ccreditation1. Test results are reported by the laboratory on at least 80% of specimens within theturnaround timespecified (and documented) by the laboratory in consultation with its clients.Turnaround time to beinterpreted as time from receipt of specimen in laboratory until results reported.2. A sufficient number of tests are performed to maintain laboratory competency.3. Internal quality control (IQC) procedures are practiced for all testing methods usedby the laboratoryOrdinarily, each test kit has a set of positive and negative controls that are to be included in
each test run. Thesecontrols included with the test kit are considered internal controls, while any other controlsincluded in the run arereferred to as external controls. QC data sheets and summaries of corrective action areretained for documentationand discussion with assessor.4. The scores on the two most recent WHO AF RO approved proficiency tests are 80%or better.Proficiency test (PT) results must be reported within 15 days of panel receipt. Laboratoriesthat receive less than80% on two consecutive PT challenges will lose their accreditation until such time that theyare able tosuccessfully demonstrate achievement of 80% or greater on two consecutive PTchallenges. Unacceptable PTresults must be addressed and corrective action taken.NOTE: A laboratory that has failed to demonstrate achievement of 80% or greater on thetwo most recent PT challenges will not be awarded any stars, regardless of the checklist score they received upon assessment.5. A ccreditation is provided in a 5 star tiered accreditation approach, based on anannual onsite assessmentof laboratory operating procedures and practices.The inspection checklist score will correspond to the number of stars awarded to a
laboratory in the followingmanner:N o Stars(0 ± 137 pts)< 55%1 Star (138 ± 160 pts)55 ± 64%
8/6/2019 Latest Phl
http://slidepdf.com/reader/full/latest-phl 26/27
2 Stars(161 ± 185 pts)65 ± 74%3 Stars(186 ± 211 pts)75 ± 84%4 Stars(212 ± 236 pts)85 ± 94%5 Stars(237 ± 250 pts)>95%
A laboratory that achieves less than the passing score on any one of the applicable criteriawill work withthe Regional Office Laboratory Coordinator to:� Identify areas where improvement is needed.� Develop and implement a work plan.
� Monitor laboratory progress.� Provide for re-testing where required.� Continue steps to achieve full accreditation.W HO AFRO Accreditation Checklist, December 2009 34.0 Parts of the A ssessmentThis laboratory assessment consists of four parts.Part IIncludes worksheets to determine and record laboratory performance for Criteria 1-4 for theimmediatelypreceding 12 months where data is complete. Selection of the most recent 12-month period,rather thanthe most recent calendar year as a basis for calculation, provides an assessment of currentperformanceand permits inspection of laboratories at any time during the calendar year.Part IIProvides a profile of the laboratory and serves to identify resource needs.Part IIIContains the assessment checklist for evaluation of laboratory operating procedures andpractices for Criteria 5.Part IVSummarizes the findings of the accreditation assessment and action planning worksheet.
International accreditation
In 2007, Haim Hacham et al. published a paper addressing the need for and the process of international standardised accreditation for laboratory proficiency in Israel. Their practice is aninvaluable experience for all in the sector [1]. With the similar efforts, both the JapanAccreditation Board for Conformity Assessment (JAB) and the E uropean CommunitiesConfederation of Clinical Chemistry and Laboratory Medicine ( E C4) have validated and

8/6/2019 Latest Phl
http://slidepdf.com/reader/full/latest-phl 27/27
convened ISO 15189, respectively [2], [3]. However, Spitzenberger and E delhäuser have expressedtheir concerns in that ISO accreditation may include obstacles rising from new emerging medicaldevices and the new approach of assessment, indicating the time dependence of the standards [4].
[edit ] References and notes
1. ^ Hacham, Haim et al. ; Tetro, Nurit; Kochavi-Azolai, Salit; Stern, Nava; Mizrahi, Dana; Lisenker,Anna; Gazit, Emanuel (2007). "Unification of the quality assurance systems of public healthlaboratories conformed to ISO 17025, ISO 15189, and ISO 9000: a major organizational change".
Accreditation and Quality Assurance: Journal for Quality, Comparability and Reliability inChemical Measurement (Elsevier ) 12 (8): 409 413. doi :10.1007/s00769-007-0262-9 .
RECOMMENDATIONS
The State Public Health Laboratory System (SPH LaboratorySystem) consists of all the participants in public healthtesting, including those who initiate testing and those whoultimately use the test results. The SPH Laboratory System ispart of the larger state public health system. The Systemincludes individuals, organizations and agencies that areinvolved in assuring that laboratory data support the 10Essential Services of Public Health. The concepts of a SPHLaboratory System are also embodied in the APHL CoreFunctions and Capabilities of State Public Health Laboratories.These documents are available on the APHL website atwww.aphl.org. Within the SPH Laboratory System areprimary stakeholders who are directly involved in creatingand using laboratory data. Additional stakeholders includethose who are concerned with complementary Essential Services,such as Training and Education and Public HealthRelated Research.
SOURCE :Definition of aState Public Health Laboratory System APHL-IssuesInBrief2.qxd