latino foster parent health perceptions of chronic conditions: a qualitative exploration
TRANSCRIPT
ORIGINAL PAPER
Latino Foster Parent Health Perceptions of Chronic Conditions:A Qualitative Exploration
Sandra H. Jee • Mary Del Balso Salter •
Jacquelyn Gonka • Nancy P. Chin
� Springer Science+Business Media New York 2013
Abstract Prior work using nationally representative data
of children in the child welfare system suggested that
Latino foster parents were less likely to identify children in
their care as having chronic conditions. Hispanics comprise
over one-fifth of children in foster care, the majority of
whom have special health care needs, and there is a
growing need to recruit qualified Latino families into the
child welfare system. Little is known about Latino parents’
health perceptions regarding chronic conditions, and
potential reasons for differing identification rates of chil-
dren with special health care needs. We conducted 17
home-based, in-depth interviews with Latino foster parents
to explore health perceptions and cultural beliefs for chil-
dren in their care around the concept of chronic illness. We
found that Latino foster parents’ understanding of condi-
tions that occurred ‘‘over and over again’’ related to emo-
tional and behavioral health problems. In contrast, their
perception of ‘‘chronic’’ was associated with terminal,
biological conditions that had limited treatment options,
such as cancer, HIV, and hepatitis. Latino foster parents did
not interpret the survey question on chronic illness as it was
intended, and their view of recurrent conditions did not
reflect chronic health conditions. Developing survey
questions that are culturally sensitive should improve
accuracy in assessing chronic health conditions for this
high-risk population. Sensitivity to cultural interpretation
for this high-needs population is vital to enhancing com-
munication between families and health providers caring
for children in foster care.
Keywords Foster care � Latino � Foster parents � Chronic
health condition � Culture
Introduction
There are approximately 400,540 children in the foster care
system (U.S. Department of Health and Human Services
2011), the majority of whom have been neglected and/or
abused prior to entering the system (Simms et al. 2000;
Szilagyi 1998). Prior work has demonstrated that children
in foster care have a high prevalence of chronic health
issues, developmental delays, and psychiatric disorders
(Almgren and Marcenko 2001; Chernoff et al. 1994;
Hansen et al. 2004; Halfon et al. 1995, 2002; Pasztor et al.
2006). Previous local and state-level analyses have esti-
mated the prevalence of chronic conditions among children
in foster care to be between 44 and 82 % (Jee et al.
2006).To assess the prevalence of chronic health conditions
of children in foster care using the first nationally repre-
sentative sample of children in the child welfare system,
our research group used the NSCAW (National Survey of
Child and Adolescent Well- Being) (Jee et al. 2006). One
key finding of this study was that compared to other ethnic
groups Latino caregivers were significantly less likely to
S. H. Jee (&)
Division of General Pediatrics, Department of Pediatrics,
University of Rochester, Rochester, NY 14642, USA
e-mail: [email protected]
M. D. B. Salter
Solid Organ Transplant Division, Department of Surgery,
University of Rochester, Rochester, NY 14642, USA
J. Gonka
Stony Brook Medical Center, Stony Brook, NY, USA
N. P. Chin
Department of Public Health Sciences, University of Rochester,
Rochester, NY 14642, USA
123
J Child Fam Stud
DOI 10.1007/s10826-013-9719-0

report caring for a child with a chronic illness. This was a
provocative finding that received both local and national
attention. We believe there are two possible explanations
for this finding: (1) the NSCAW question did not correctly
assess the presence of ‘‘chronic illness’’ among Latino
families which the survey described as illness which
occurred ‘‘over and over again’’; and/or (2) Latino specific
health perceptions and practices have a positive impact on
the management of chronic conditions in foster children so
they did not occur over and over again. To our knowledge,
there was no previous published work that had examined
Latino health perceptions and practices for this at-risk
population of children in foster care.
It is important to understand Latino health perceptions
and practices, especially with respect to children in foster
care. Latinos are not only one of the largest and fastest
growing minority populations in the U.S., but Latino
families have also markedly increased their rates of adop-
tion of children in foster care (Mikhail 1994; Riche 2000;
Flores et al. 2002). In 2004, the U.S. Department of Health
and Human Service’s Administration for Children and
Families reported that Latino families adopted nearly 5,300
children from foster care, a jump of almost 20 % in 5 years
(U.S. Department of Health and Human Services 2007).
Most recent data indicates that Hispanics comprise 21 % of
children who entered foster care in 2011, and public
agency adoptions of Hispanic children has increased to
15.5 % over the past decade (U.S. Department of Human
Services 2011). The need in our current child welfare
system for qualified Latino families who share cultural
identity and language is exceeded by the number of Latino
children in the system; hence, ongoing campaigns are
actively recruiting more Latino families to become foster
parents (Casey Foundation Leadership Group 2012).
Latino foster parents represent a rapidly growing subset of
caregivers in the child welfare system who have unique,
culturally informed health perspectives that may impact their
interpretation and management of chronic illness by seeking
traditional methods of care (Rogers 2010). Prior work
examining foster parent perspectives has demonstrated that
transcultural foster care placements may impact the family
relationships and cultural identity (Brown et al. 2009);
moreover, the presence of disabilities or special health needs
for children in foster care affects service needs (Brown et al.
2005; Brown and Rodger 2009; Lauver 2008). Our goal in
this study was to understand why Latino foster parents might
have reported caring for fewer children with chronic diseases
by creating a provisional explanatory model of chronic dis-
ease management for Latino foster families. Specifically we
sought: (1) to explore Latino foster parents’ perceptions of
health; (2) to understand the Latino concept of chronic
conditions; and 3) to assess the validity of the NSCAW
question within the Latino population.
Method
Recruitment to Study
We received a list of all Latino foster parents (n = 18) in
our county population from our county Department of
Human Services. We mailed recruitment letters to all
potential participants, and then used follow up telephone
calls to schedule home-based interviews. Latino caregivers
who participated in the project received a $20 gift card.
Two investigators with expertise in qualitative data
research and Spanish language and culture, conducted the
home interviews for this study.
Interview Procedure
Our research team developed a semi-structured interview
guide to collect demographic information and to explore
beliefs and perceptions regarding personal and foster care
related health conditions and health management. The
interview script covered three main domains using open-
ended questions: (1) The caregiver’s personal health, (2)
The caregiver’s experience and perceptions of their foster
children’s health, and (3) The caregiver’s belief about
chronic conditions. Interviews were conducted in subjects’
homes, lasted approximately 60 min, and were audio-taped
for verbatim transcription. Researchers also took field notes
during the interviews and asked unscripted follow-up
probes as needed to clarify subject responses. All inter-
views were conducted in English, although researchers
were able to speak Spanish; if there were language barriers,
a dictionary was available to assist the participant.
Data Analysis
The analytic team was comprised of two research-experi-
enced individuals (M.A.D. and S.H.J.), with a third
supervisory qualitative methods mentor (N.P.C.). We used
the framework approach, using a matrix based method,
(Ritchie and Lewis 2003), to develop open-ended questions
for our interview guide. All data were analyzed using the
thematic framework approach, in which analysts looked for
common themes or patterns that fit into three domains: (1)
Caregiver’s personal health; (2) Caregiver’s perception of
foster child health; and (3) Caregiver’s understanding of
what comprises a chronic illness. Interviews were analyzed
separately by two independent readers (M.A.D. and S.H.J.)
who then met together to determine themes and categorize
data. Readers listened to audio-tapes as needed to verify
emphasis of speech in the transcribed interviews. Dis-
agreements were corrected through debate and review
with the supervisory qualitative methods mentor (N.P.C.)
to ensure reliability of analyses. We used constant
J Child Fam Stud
123
comparison to check that each coded item. (Pope et al.
2000). New sub-domains were added to the above frame-
work as a result of several validation meetings. Some
disagreements in domain categorization brought up the
issue of inappropriate categorization for certain themes.
New themes were established, which allowed for the
addition of two new domains; role of religious faith and
cultural practices related to home remedies impacting
health perceptions.
A cross classification matrix, using a thematic frame-
work approach (Ritchie and Lewis 2003), allowed for
further examination of how all five domains relate, and
helped to organize the data into key themes, concepts, and
emergent categories. It was determined that many domains
were interrelated and potentially sequential. For example,
view of health and wellness can be understood in terms of
its influence on behavioral health status and holistic view
of the child, and chronic health conditions can be under-
stood in terms of a foster parent’s past experience with
managing complex health problems for themselves and for
others. Closer examination of domains called for re-cate-
gorization that would better reflect these main themes and
the interdependent process. As a result, all new domains
were identified to reflect the themes that became evident
after the initial coding and analysis of data. We recoded all
the transcripts according to these new themes. The fol-
lowing analysis reflects this final coding.
Results
Participant Demographics
We contacted the entire population of registered Latino
foster parents who were in the Monroe County’s foster
system at the time of the study. Our study sample included
17 out of the 18 Latino foster parents in the county. The
home interviews lasted approximately 60 min each. Study
participants (see Table 1) ranged in age from 30 to
66 years old. The majority of the parents were female, born
in Puerto Rico, and many contained a high school educa-
tion or less. The length of time of being a foster parent
ranged from 9 months to 26 years.
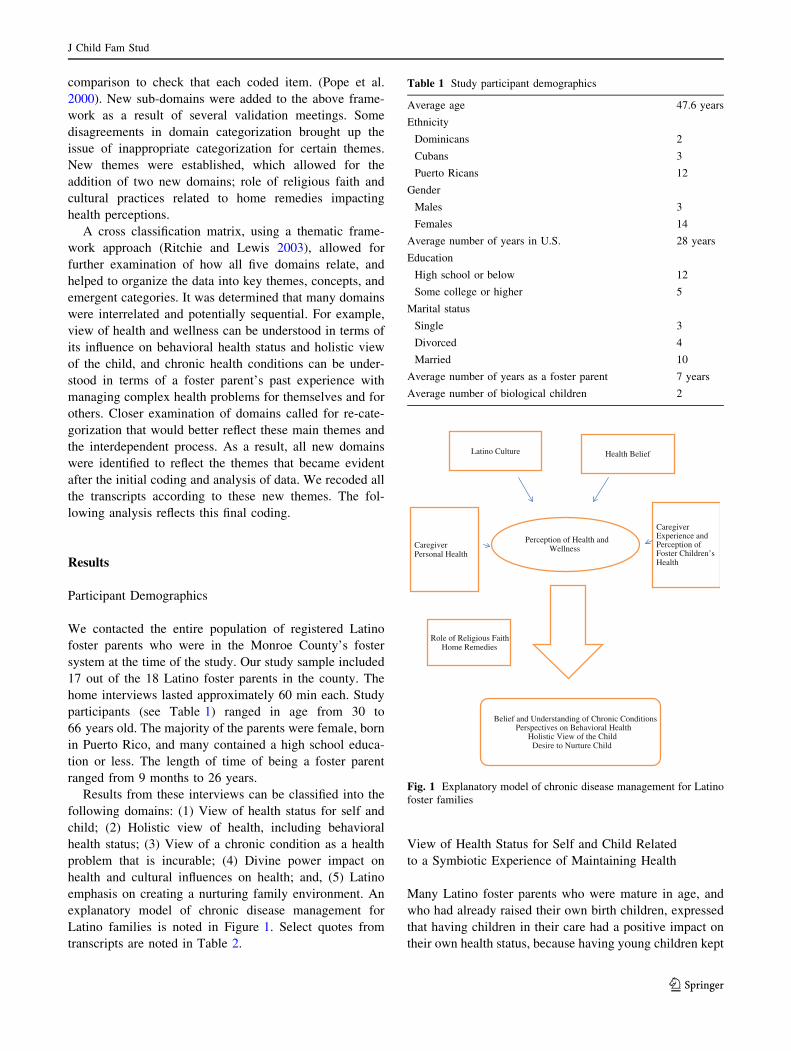
Results from these interviews can be classified into the
following domains: (1) View of health status for self and
child; (2) Holistic view of health, including behavioral
health status; (3) View of a chronic condition as a health
problem that is incurable; (4) Divine power impact on
health and cultural influences on health; and, (5) Latino
emphasis on creating a nurturing family environment. An
explanatory model of chronic disease management for
Latino families is noted in Figure 1. Select quotes from
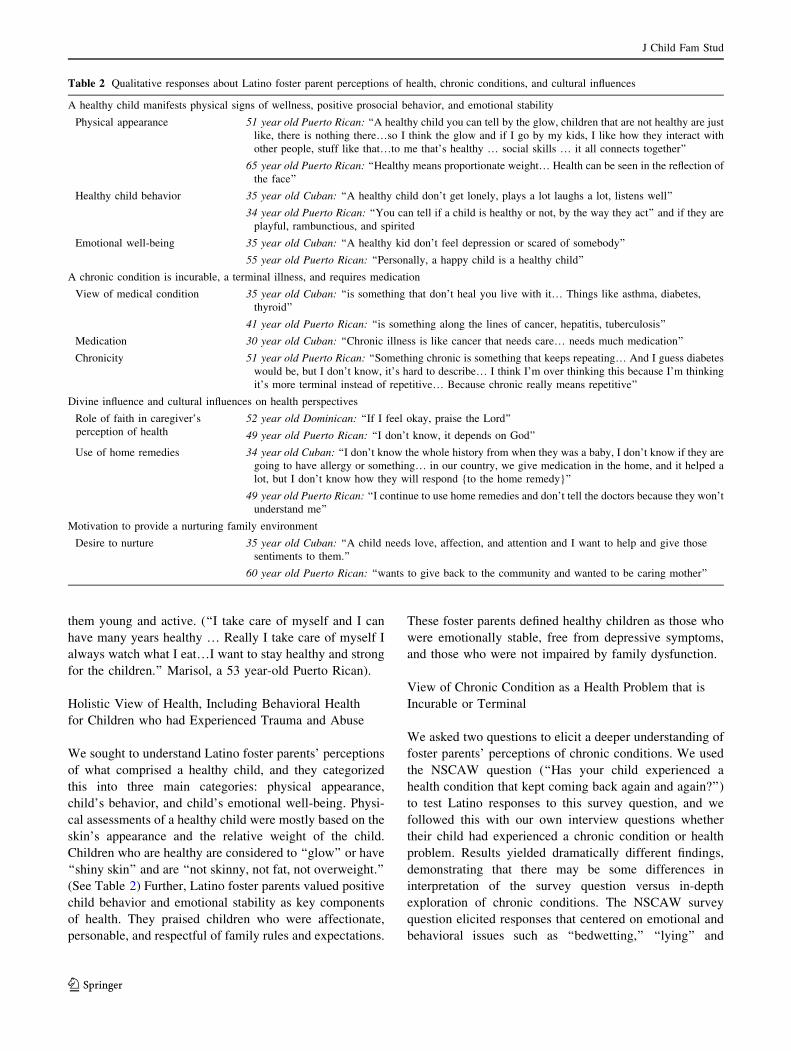
transcripts are noted in Table 2.
View of Health Status for Self and Child Related
to a Symbiotic Experience of Maintaining Health
Many Latino foster parents who were mature in age, and
who had already raised their own birth children, expressed
that having children in their care had a positive impact on
their own health status, because having young children kept
Table 1 Study participant demographics
Average age 47.6 years
Ethnicity
Dominicans 2
Cubans 3
Puerto Ricans 12
Gender
Males 3
Females 14
Average number of years in U.S. 28 years
Education
High school or below 12
Some college or higher 5
Marital status
Single 3
Divorced 4
Married 10
Average number of years as a foster parent 7 years
Average number of biological children 2
Latino Culture Health Belief
Perception of Health and WellnessCaregiver
Personal Health
Caregiver Experience and Perception of Foster Children’s Health
Belief and Understanding of Chronic Conditions Perspectives on Behavioral Health
Holistic View of the ChildDesire to Nurture Child
Role of Religious FaithHome Remedies
Fig. 1 Explanatory model of chronic disease management for Latino
foster families
J Child Fam Stud
123
them young and active. (‘‘I take care of myself and I can
have many years healthy … Really I take care of myself I
always watch what I eat…I want to stay healthy and strong
for the children.’’ Marisol, a 53 year-old Puerto Rican).
Holistic View of Health, Including Behavioral Health
for Children who had Experienced Trauma and Abuse
We sought to understand Latino foster parents’ perceptions
of what comprised a healthy child, and they categorized
this into three main categories: physical appearance,
child’s behavior, and child’s emotional well-being. Physi-
cal assessments of a healthy child were mostly based on the
skin’s appearance and the relative weight of the child.
Children who are healthy are considered to ‘‘glow’’ or have
‘‘shiny skin’’ and are ‘‘not skinny, not fat, not overweight.’’
(See Table 2) Further, Latino foster parents valued positive
child behavior and emotional stability as key components
of health. They praised children who were affectionate,
personable, and respectful of family rules and expectations.
These foster parents defined healthy children as those who
were emotionally stable, free from depressive symptoms,
and those who were not impaired by family dysfunction.
View of Chronic Condition as a Health Problem that is
Incurable or Terminal
We asked two questions to elicit a deeper understanding of
foster parents’ perceptions of chronic conditions. We used
the NSCAW question (‘‘Has your child experienced a
health condition that kept coming back again and again?’’)
to test Latino responses to this survey question, and we
followed this with our own interview questions whether
their child had experienced a chronic condition or health
problem. Results yielded dramatically different findings,
demonstrating that there may be some differences in
interpretation of the survey question versus in-depth
exploration of chronic conditions. The NSCAW survey
question elicited responses that centered on emotional and
behavioral issues such as ‘‘bedwetting,’’ ‘‘lying’’ and
Table 2 Qualitative responses about Latino foster parent perceptions of health, chronic conditions, and cultural influences
A healthy child manifests physical signs of wellness, positive prosocial behavior, and emotional stability
Physical appearance 51 year old Puerto Rican: ‘‘A healthy child you can tell by the glow, children that are not healthy are just
like, there is nothing there…so I think the glow and if I go by my kids, I like how they interact with
other people, stuff like that…to me that’s healthy … social skills … it all connects together’’
65 year old Puerto Rican: ‘‘Healthy means proportionate weight… Health can be seen in the reflection of
the face’’
Healthy child behavior 35 year old Cuban: ‘‘A healthy child don’t get lonely, plays a lot laughs a lot, listens well’’
34 year old Puerto Rican: ‘‘You can tell if a child is healthy or not, by the way they act’’ and if they are
playful, rambunctious, and spirited
Emotional well-being 35 year old Cuban: ‘‘A healthy kid don’t feel depression or scared of somebody’’
55 year old Puerto Rican: ‘‘Personally, a happy child is a healthy child’’
A chronic condition is incurable, a terminal illness, and requires medication
View of medical condition 35 year old Cuban: ‘‘is something that don’t heal you live with it… Things like asthma, diabetes,
thyroid’’
41 year old Puerto Rican: ‘‘is something along the lines of cancer, hepatitis, tuberculosis’’
Medication 30 year old Cuban: ‘‘Chronic illness is like cancer that needs care… needs much medication’’
Chronicity 51 year old Puerto Rican: ‘‘Something chronic is something that keeps repeating… And I guess diabetes
would be, but I don’t know, it’s hard to describe… I think I’m over thinking this because I’m thinking
it’s more terminal instead of repetitive… Because chronic really means repetitive’’
Divine influence and cultural influences on health perspectives
Role of faith in caregiver’s
perception of health
52 year old Dominican: ‘‘If I feel okay, praise the Lord’’
49 year old Puerto Rican: ‘‘I don’t know, it depends on God’’
Use of home remedies 34 year old Cuban: ‘‘I don’t know the whole history from when they was a baby, I don’t know if they are
going to have allergy or something… in our country, we give medication in the home, and it helped a
lot, but I don’t know how they will respond {to the home remedy}’’
49 year old Puerto Rican: ‘‘I continue to use home remedies and don’t tell the doctors because they won’t
understand me’’
Motivation to provide a nurturing family environment
Desire to nurture 35 year old Cuban: ‘‘A child needs love, affection, and attention and I want to help and give those
sentiments to them.’’
60 year old Puerto Rican: ‘‘wants to give back to the community and wanted to be caring mother’’
J Child Fam Stud
123

‘‘depression.’’ Our interview question using the word
‘‘chronic’’ brought forth answers that defined ‘‘cancer,’’
‘‘HIV,’’ and ‘‘tuberculosis’’ as chronic conditions. Within
this category three themes emerged, (1) types of specific
medical conditions, (2) medication and treatment, and (3)
chronicity of symptoms. (see Table 2). Foster parents dif-
ferentiated between health conditions or states that were
recurrent (asthma) versus conditions that were more clearly
defined diagnoses (HIV, Hepatitis), which were viewed as
‘‘chronic.’’ ‘‘Chronic’’ health conditions were considered
more serious, or less amenable to treatment.
Divine Power Impact on Health and Cultural Influences
on Health Perspectives
Within this domain, which was inter-related to the concepts
of a healthy child and health status, we found that many
Latino caregivers mentioned divine influence on health
outcomes. While answering other open-ended questions,
many foster parents casually mentioned how religious
influences impacted their own health: ‘‘Thanks to God I am
healthy’’, ‘‘God decides my future health’’, or ‘‘If I feel
okay, praise the Lord’’. Of note, these foster parents
independently mentioned divine influence on health with-
out any prompting from our interview guides.
One subtheme that was related to cultural influence on
health and management of illness was use of home reme-
dies. Most of the Latino caregivers reported that when they
were children their parents had used home remedies for
minor ailments (i.e. use of alcohol on the forehead) and
herbal medications on them. Although all subjects inter-
viewed were parents of children who had ready access to
medical care in our health clinic, many parents still
reported relying on cultural home remedies for minor ail-
ments such as headaches and fevers.
Latino Influence on Creating a Nurturing Family
Environment
When asked to explain why they became foster parents,
most caregivers expressed their fondness for caring for
children, a desire to contribute to the community, and a
wish to feel a sense of purpose. Also, the sentiment of
‘‘treat them like your own’’ appeared in several interviews.
Most importantly, there was a these caregivers expressed a
general feeling of pride because they were able to improve
their child’s health. They appreciated the opportunity to
provide a nurturing supportive home for children in their
care. (‘‘A child needs love, affection, and attention, and I
want to help and give those sentiments to them.’’ Cary,
35 year old Cuban) These feelings of having contributed
something positive for the child, however, occasionally
created a tension between biological and foster parent
relationships. This was especially relevant when children
returned from a visit with biological parents and had
exacerbating behavioral and health problems. For instance
some foster parents noted an aggravation of a child’s
asthma symptoms after a home visit that included exposure
to secondhand smoke. Hence, foster parents felt they had
limited control over their child’s health, but prioritized the
opportunity to create a nurturing home environment.
Discussion
Based on prior work investigating prevalence of chronic
conditions among children in foster care, we explored
Latino caregivers’ perceptions of chronic conditions. The
findings from this qualitative evaluation suggest that Latino
respondents did not interpret the NSCAW question about
chronic illness in the way it was intended. Our results
suggest that the NSCAW question elicited responses
relating to emotional and behavioral health issues rather
than the biological issues it was designed to address. Fur-
thermore, when our research question was given, which
replaced the NSCAW wording of ‘‘over and over again’’
with ‘‘chronic’’, responses elicited more serious conditions
such as, HIV and cancer, which are more likely or often
‘‘terminal.’’ We surmise that this discrepancy may be
attributable to having a cultural barrier, as well as under-
lying differences in what constitutes a chronic condition.
Our findings suggest that Latino foster parents may
dichotomize chronic conditions into those that are terminal
and those that are amenable to treatment. Most Latino
caregivers recognized asthma to be a categorically defined
chronic condition, but moved it to this category only if the
child did not respond to treatment. This variation is due to
the fact that many of these Latino caregivers report that
they have been able to ‘‘cure’’ and ‘‘heal’’ children in foster
care with asthma issues. Foster parents who feel that their
care has resulted in managing conditions such as asthma
effectively, may not uniformly identify asthma as a chronic
illness. A previous study by Becker et al. (1998), which
conducted a 5 year qualitative study on 61 Latino elders,
further proves this notion of ‘‘symptom remission’’ as a
cure to a chronic condition. However, the curing of the
illness was, ‘‘contingent on the continued taking of medi-
cation’’ (Becker et al. 1998). This is consistent with find-
ings from a study with Latinos who initially did not
perceive diabetes to be a chronic condition because they
were able to control symptoms with medication. Many
participants initially viewed diabetes as an acute illness,
and only defined it as a chronic condition after having the
disease for many years (Heuer and Lausch 2006). Simi-
larly, we found that participants identified terminal ill-
nesses, especially those that were incurable and required
J Child Fam Stud
123
ongoing care, such as HIV, as a chronic condition. Simi-
larly, health conditions with limited treatment options were
considered chronic. This is consistent with the World
Health Organization definition of a chronic illness or
condition as a health issue that persists over a long period
of time that often requires comprehensive health services
(Epping-Jordan et al. 2004). Our study findings supported
that the perceived ability to manage or control a chronic
health condition affected Latino foster parents’ concept of
chronic conditions.
Ongoing management and symptom remission were
important components of what defined a chronic illness;
however, other important themes related to the intertwined
relationship of child and caregiver health, and divine
influences on health. Some foster parents noted that they
felt younger and healthier while caring for healthy children
(i.e., synergistic effect of health and child health), and
others made references to a divine power having control
over their health. Many stated that the status of their future
health conditions would be determined by God. Other work
have suggested that Latinos may perceive the cause of their
chronic illnesses to be a result of ‘‘God’s will’’ or ‘‘pun-
ishment from God’’ (Brown et al. 2009b; Quatromoni et al.
1994; Zaldı́var and Smolowitz 1994). Many perceived that
their illness was the result of doing something wrong, of
which God disapproved, and that therefore their illness is
the punishment for their crimes. We are unsure how this
might impact the day-to-day management of a child’s
chronic condition, but believe this warrants further study.
Another important finding relates to the cultural asso-
ciation of Latinos being a nurturing population, which
supports previous literature (Kolobe 2004; Wong 2006).
Latinos have ranked high on the nurturing scale, when
tested using the Parent Behavioral Checklist (Wong 2006).
Caregivers within our study population stated that they
treated their foster children, ‘‘like their own’’, and were
‘‘praised’’ for their care. Strong family cohesion, and a
nurturing environment, has proven to have a positive cor-
relation on a child’s health (Kolobe 2004). Perhaps the
nurturing environment of the Latino community and
extended kinship care translates into methods of care that
truly reduce, if not eliminate the presence of a chronic
illness.
It is important to recognize the relative strengths of this
research study. Our study contained the entire population of
Latino caregivers within Monroe County, which allowed for
a wide range of opinions and a highly representative sample.
The general Latino population in Monroe County accounts
for about 5 % of the population (Department of Human
Services, personal communication). In addition, the nature of
this qualitative research provided an opportunity to explore
the quantitative NSCAW data on a personal level, using an
open-ended approach, which resulted in many robust
findings. Nonetheless, the broader applicability of our
research findings is limited by several factors. Data were
collected from a single county population, and it is possible,
although unlikely, that some foster parents had limited
experience with children who have chronic health conditions.
All participants were able to speak in English, but the occa-
sional use of a Spanish dictionary to assist with translation
may have affected some subtle nuance of their opinions.
Prior work has shown that Latino health perceptions are
affected by cultural orientations that differ from the
mainstream, which may not be rooted in the biomedical
model (Arcia 1998; Garcia et al. 2007, Becker et al. 1998).
This may be attributed to the profound effect that cultural
beliefs have in the use of home remedies and on how
certain ailments are treated (Becker et al. 1998; Hatcher
and Whittemore 2007; Riche 2000). Latinos may interpret
an illness as a consequence of experiencing strong emo-
tions, or having spiritual significance (Hatcher and Whit-
temore 2007).Moreover, the use of alternative medicine
and home remedies is higher within the Latino population,
as compared to other ethnic groups (Bearison et al. 2002;
Mikhail 1994; Schoenberg et al. 2004). Becker’s et al.
study revealed that Latino’s possess lower levels of
knowledge about chronic illnesses (Becker et al. 1998). All
of these factors may impact Latino foster parent health
perceptions around chronic conditions. Further, Latino
foster parents who are caring for children under the aus-
pices of the social services may be less likely to admit to
using cultural practices, or less comfortable with applying
non-traditional remedies that they might otherwise use with
their own biological children.
Conclusion
Major implications from this project relates to enhancing
cultural awareness and competency. More effective
research tools are needed to understand how culture and
foster care health intersect. If Latinos are truly improving
the health status of children in foster care, we should
identify the factors that contribute to this method of care.
If, however, Latinos are misinterpreting standardized sur-
vey questions on chronic conditions, and have a unique
cultural view of chronic health conditions, then researchers
need to rephrase standardized questions and use follow-up
probes to ensure that survey respondents understand the
questions. Further, health care providers need to expand
educational efforts around chronic condition identification
and management, and reframe chronic conditions as ill-
nesses that will require ongoing intervention, and not just
acute symptom management. For the foster care system, it
is vital to identify children in foster care with chronic
conditions, (Jee et al. 2006) and those who may benefit
J Child Fam Stud
123
from active case management to avoid unnecessary emer-
gency department visits, (Jee et al. 2005) and apply stan-
dardized screening measures (Jee et al. 2010a, b, c, 2011a,
b). Foster parent training programs, which can impact
access to care, should take into account unique cultural
aspects that can impact health beliefs and behaviors.
Acknowledgments We gratefully acknowledge the support of the
Monroe County Department of Human Services and especially Susan
McClean in assisting with this project. Supported in part by the
Robert Wood Johnson Physician Faculty Scholars Program (S.H.J.).
References
Almgren, G., & Marcenko, M. (2001). Emergency room use among a
foster care sample: The influence of placement history, chronic
illness, psychiatric diagnosis, and care factors. Brief Treatmentand Crisis Intervention, 1(1), 55–64.
Arcia, E. (1998). Latino parents’ perception of their children’s health
status. Social Science and Medicine, 46(10), 1271–1274.
Bearison, D. J., Minian, N., & Granowetter, L. (2002). Medical
management of asthma and folk medicine in a Hispanic
community. Journal of Pediatric Psychology, 27(4), 385–392.
Becker, G., Beyene, Y., Newsom, E. M., & Rodgers, D. V. (1998).
Knowledge and care of chronic illness in three ethnic minority
groups. Family Medicine, 30(3), 173–178.
Brown, J. D., Moraes, S., & Mayhew, J. (2005). Service needs of
foster families with children who have disabilities. Journal ofChild and Family Studies, 14(3), 417–529.
Brown, J. D., & Rodger, S. (2009). Children with disabilities:
Problems faced by foster parents. Children and Youth ServicesReview, 31(1), 40–46.
Brown, J. D., St. Arunalt, D., George, N., & Sintzel, J. (2009).
Challenges of transcultural placements: Foster parent perspec-
tives. Child Welfare, 88(3), 103–126.
Casey Latino Leadership Group Fact Sheet Latino Children in Child
Welfare. (2012). Retrieved from November 10, 2012. http://
www.casey.org/Resources/Publications/pdf/LatinoChildren.pdf.
Chernoff, R., Combs-Orme, T., Risley-Curtiss, C., & Heisler, A.
(1994). Assessing the health status of children entering foster
care. Pediatrics, 93(4), 594–601.
Epping-Jordan, J., Pruit, D., Bengoa, R., & Wagner, E. H. (2004).
Improving the quality of health care for chronic conditions.
Quality and Safety in Health Care, 13(4), 299–305.
Flores, G., Fuentes-Afflick, E., Barbot, O., Carter-Pokras, O., Claudio,
L., Lara, M., et al. (2002). The health of Latino children: urgent
priorities, unanswered questions, and a research agenda. Journalof the American Medical Association, 288(1), 82–90.
Garcia, C., Duckett, L., Saewyc, E., & Bearinger, L. H. (2007).
Perceptions of health among immigrant Latino adolescents from
Mexico. Journal of Holistic Nursing, 25(2), 81–91.
Halfon, N., Flint, R., & Inkelas, M. (2002). Child health agency roles
in health services for children in foster care. UCLA Center forHealthier Children, Families, and Communities, 3, 1–12.
Halfon, N., Mendonca, A., & Berkowitz, G. (1995). Health status of
children in foster care. The experience of the center for the
vulnerable child. Archives of Pediatrics and Adolescent Medi-cine, 149(4), 386–392.
Hansen, R. L., Mawjee, F. L., Barton, K., et al. (2004). Comparing the
health status of low-income children in and out of foster care.
Child Welfare, 83(4), 367–380.
Hatcher, E., & Whittemore, R. (2007). Hispanic adults’ beliefs about
type 2 diabetes: Clinical implications. Journal of the AmericanAcademy of Nurse Practitioners, 19(10), 536–545.
Heuer, L., & Lausch, C. (2006). Living with diabetes: Perceptions of
Hispanic migrant farmworkers. Journal of Community HealthNursing, 23(1), 49–64.
Jee, S. H., Antonucci, T. C., Aida, M., Szilagyi, M. A., & Szilagyi, P.
G. (2005). Emergency department utilization by children in
foster care. Ambulatory Pediatrics, 5(2), 102–106.
Jee, S. H., Barth, R. P., Szilagyi, M. A., Szilagyi, P. G., Aida, M., &
Davis, M. M. (2006). Factors associated with chronic conditions
among children in foster care. Journal of Health Care for thePoor and Underserved, 17(2), 328–341.
Jee, S. H., Conn, A. M., Blumkin, A., Szilagyi, P. G., Baldwin, C. D.,
& Szilagyi, M. A. (2010a). Identification of social-emotional
problems among young children in foster care. Journal of ChildPsychology and Psychiatry, 51(12), 1351–1358.
Jee, S. H., Halterman, J. S., Szilagyi, M. A., Conn, A. M., Alpert-
Gillis, L., & Szilagyi, P. G. (2011a). Enhanced detection of
social-emotional problems among youth in foster care. AcademicPediatrics, 11(5), 409–413.
Jee, S. H., Szilagyi, M. A., Blatt, S. D., Meguid, V., Auinger, P., &
Szilagyi, P. G. (2010b). Timely identification of mental health
problems in two foster care medical homes. Children and YouthServices Review, 32(5), 685–690.
Jee, S. H., Szilagyi, M. A., Conn, A. M., Nilsen, W. J., Toth, S.,
Baldwin, C. D., et al. (2011b). Assessing and validating office-
based screening for psychosocial strengths and difficulties
among youths in foster care. Pediatrics, 127, 904–910.
Jee, S. H., Szilagyi, M. A., Ovenshire, C., Norton, A., Conn, A. M.,
Blumkin, A., et al. (2010c). Improved detection of developmen-
tal delays among young children in foster care. Pediatrics,125(2), 282–289.
Kolobe, T. H. (2004). Childrearing practices and developmental
expectations for Mexican-American mothers and the develop-
mental status of their infants. Physical Therapy, 84(5), 439–453.
Lauver, L. S. (2008). Parenting foster children with chronic illness
and complex medical needs. Journal of Family Nursing, 14(1),
74–96.
Mikhail, B. I. (1994). Hispanic mothers’ beliefs and practices
regarding selected children’s health problems. Western Journalof Nursing Research, 16(6), 623–638.
Pasztor, E. M., Hollinger, D. S., Inkelas, M., & Halfon, N. (2006).
Health and mental health services for children in foster care: the
central role of foster parents. Child Welfare, 85(1), 33–57.
Pope, C., Ziebland, S., & Mays, N. (2000). Qualitative research in
health care. Analysing qualitative data. British Medical Journal,320, 114–116.
Quatromoni, P. A., Milbauer, M., Posner, B. M., Carballeria, N. P.,
Brunt, M., & Chipkin, S. R. (1994). Use of focus groups to
explore nutrition practices and health beliefs of urban Caribbean
Latinos with diabetes. Diabetes Care, 8, 869–873.
Riche, M. F. (2000). America’s diversity and growth: Signposts for
the twenty first century. Population Bulletin, 55(2), 1–43.
Ritchie, J., & Lewis, J. (2003). Qualitative research practice. A guidefor social science students and researchers. USA: Sage
Publications.
Rogers, A. (2010). Exploring health beliefs and care-seeking behav-
iors of older USA-dwelling Mexicans and Mexican-Americans.
Ethnicity and Health, 15(6), 581–599.
Schoenberg, N. E., Stoller, E. P., Kart, C. S., Perzynski, A., & Chapleski,
E. E. (2004). Complementary and alternative medicine use among a
multiethnic sample of older adults with diabetes. Journal ofAlternative and Complementary Medicine, 10(6), 1061–1066.
J Child Fam Stud
123

Simms, M. D., Dubowitz, H., & Szilagyi, M. A. (2000). Health care
needs of children in the foster care system. Pediatrics, 106(4
Suppl), 909–918.
Szilagyi, M. (1998). The pediatrician and the child in foster care.
Pediatrics in Review, 19(2), 39–50.
U.S. Department of Health and Human Services (DHHS) (2011).
Administration for Children Families (ACF), Administration on
children, youth and families, children’s bureau. Adoption and
foster care analysis and reporting system (AFCARS). The
AFCARS Report # 19: preliminary estimates for FY 2011 as of
July 2012. Washington, D.C.: ACF. Retrieved from November 12,
2012. http://www.acf.hhs.gov/sites/default/files/cb/afcarsreport19.
pdf.
U.S. Department of Health and Human Service’s Administration for
Children and Families Adoption & Foster Care. (2007).
Retrieved from March 31, 2007. http://www.acf.hhs.gov/.
Wong, S. T. (2006). The relationship between parent emotion, parent
behavior, and health status of young African American and
Latino children. Journal of Pediatric Nursing, 21(6), 434–442.
Zaldı́var, A., & Smolowitz, J. (1994). Perceptions of the importance
placed on religion and folk medicine by non-Mexican-American
Hispanic adults with diabetes. Diabetes Educator, 20(4), 303–306.
J Child Fam Stud
123