lead & mercury toxicity2
TRANSCRIPT

8/8/2019 Lead & Mercury Toxicity2
http://slidepdf.com/reader/full/lead-mercury-toxicity2 1/34
Lead Toxicity

8/8/2019 Lead & Mercury Toxicity2
http://slidepdf.com/reader/full/lead-mercury-toxicity2 2/34
± Lead may be the oldest recognized chemical toxin.
± It has been used in making batteries, pottery, solder, pesticides, cooking
utensils, plumbing, and ³the one that is getting so much attention now´
household paint.
± Another big source of lead in the environment comes from gasoline thatcontains lead.

8/8/2019 Lead & Mercury Toxicity2
http://slidepdf.com/reader/full/lead-mercury-toxicity2 3/34
A. Nature of Jobs exposed to
Lead
Battery manufacturing
Chemical industry

8/8/2019 Lead & Mercury Toxicity2
http://slidepdf.com/reader/full/lead-mercury-toxicity2 4/34
A. Nature of Jobs exposed to
Lead
Building construction
Pipe fitters

8/8/2019 Lead & Mercury Toxicity2
http://slidepdf.com/reader/full/lead-mercury-toxicity2 5/34
A. Nature of Jobs exposed to
Lead
Plastic industry

8/8/2019 Lead & Mercury Toxicity2
http://slidepdf.com/reader/full/lead-mercury-toxicity2 6/34
Major O at ons and Industr s ssociat d it
ad O r osur
att r anuf actur ing
ical industr onstr uction or r s
D olition or r s
Fir ing-r ange instr uctor s
Foundr or er s
Gas-station attendants
Gasoline additives r od.
eweler s
ead iner s
ead smelter s and r ef iner s
igment manuf actur ing
ipe f itter s lastics industr
otter wor er s
r inter s
Radiator r epair
Rubber industr
Solder ing of lead pr od.
Solid waste pr oduction
Stained-glass maker s
Welder s
. Natur e of obs exposed to
ead

8/8/2019 Lead & Mercury Toxicity2
http://slidepdf.com/reader/full/lead-mercury-toxicity2 7/34
B. Clinical Presentation
Pharmacokinetics Absorption:
The two principal exposure routes are
respiratory system inhaled in dust and fumes
gastrointestinal system especially ingestion of contaminated
food. The ma jor target organs are the central and peripheral nervous
systems, kidneys, and blood.
Distribution:
95% of lead exists in the BCs (half -life = 35 days)
± About 10% of the total body lead burden equilibriates in soft tissue
(half -life = 40 days).
± 90% of the total body lead burden existing in skeleton (half -life =
20-30 years).
Elimination:
The kidney accounts for 75% of daily lead loss.

8/8/2019 Lead & Mercury Toxicity2
http://slidepdf.com/reader/full/lead-mercury-toxicity2 8/34
A. Hematologic effects
± Impaired heme biosynthesis
± lead blocks the conversion of d-aminolevulinic acid to
porphobilinogen
± Lead inhibits the enzyme (ferrochelatase) during the
formation of heme; results in elevated free
erythrocyte protoporphyrin ( EP) levels
Pathophysiology

8/8/2019 Lead & Mercury Toxicity2
http://slidepdf.com/reader/full/lead-mercury-toxicity2 9/34
Signs & Symptoms
A. Hematologic effects
± Anemia most common
± Basophilic stippling
uncommon but highly
suggestive of lead
intoxication. Eosinophilia in
lead-intoxicated patients

8/8/2019 Lead & Mercury Toxicity2
http://slidepdf.com/reader/full/lead-mercury-toxicity2 10/34
B. Neurologic effects
± In adults, peripheral neuropathy is the most commonmanifestation
± encephalopathy appears more frequently in children(passes the BBB more easily in children)
± Cerebral edema is a late complication of leadencephalopathy,
±S
ubtle neuropsychiatric changes (e.g. hyperactivity,learning disorders, and fine motor dysfunction) mayrepresent subclinical neuropathy.
Pathophysiology

8/8/2019 Lead & Mercury Toxicity2
http://slidepdf.com/reader/full/lead-mercury-toxicity2 11/34
B. Neurologic effects
± classic motor neuropathy
± Extensor weakness (wrist drop) at high levels ± paresthesias are uncommon
± Motor conduction velocities and distal latency may beprolonged, but sensory conduction velocities are usuallynormal
± Acute encephalopathy occurs infrequently in adults ±seizures, obtundation, and confusion are the mostcommon signs
± Subtle effects on personality, memory, learning, reactiontime, psychomotor function, and motor coordination
Signs & Symptoms

8/8/2019 Lead & Mercury Toxicity2
http://slidepdf.com/reader/full/lead-mercury-toxicity2 12/34
seizure confusion

8/8/2019 Lead & Mercury Toxicity2
http://slidepdf.com/reader/full/lead-mercury-toxicity2 13/34
C. Renal effects
± Lead toxicity produces lesions of the proximal tubule
and loops of Henle
± A anconi syndrome develops, which includes
aminoaciduria, phosphaturia, glycosuria, and renal
tubular acidosis.
± Lead decreases tubular secretion of uric acid, causing
higher incidence of gout
Pathophysiology

8/8/2019 Lead & Mercury Toxicity2
http://slidepdf.com/reader/full/lead-mercury-toxicity2 14/34
C. Renal effects
± enal disease can be
asymptomatic until thelate stages and may not
be detected without
specific testing.
Signs & Symptoms

8/8/2019 Lead & Mercury Toxicity2
http://slidepdf.com/reader/full/lead-mercury-toxicity2 15/34
D. Endocrine Effects
± Lead impedes vitamin conversion into its hormonal form,1,25-dihydroxyvitamin , impairing cell growth, maturation,and tooth and bone development.
± Chronic lead exposure could adversely affect the thyroid
over time.
E. Cardiovascular (Hypertension) Effects
± onset and development of hypertension ± systolic blood pressure may rise 1±2 mm with each
doubling of blood lead,
± blood lead can account for a 1 to 2% variance in bloodpressure
± renal failure and hypertension can exacerbate each other
Pathophysiology

8/8/2019 Lead & Mercury Toxicity2
http://slidepdf.com/reader/full/lead-mercury-toxicity2 16/34
F. Reproductive and Developmental Effects
M ale Reproductive Effects
± decrease sperm count totals
± increase abnormal sperm frequencies
± Long-term lead exposure ± may diminish sperm concentrations, total sperm
counts, and total sperm motilityP regnancy Outcomes
± increased frequency of miscarriages and stillbirths (chronic exposure)
Developmental Effects
± pregnancy issues (e.g., premature births and low birth weights)
± congenital abnormalities ± postbirth effects on growth or neurologic development
± readily crosses the placenta, adversely affects fetus viability as well as fetal and
early childhood development
± Prenatal exposure to low lead levels increases risk of reduced birth weight and
premature birth
Pathophysiology
8/8/2019 Lead & Mercury Toxicity2
http://slidepdf.com/reader/full/lead-mercury-toxicity2 17/34
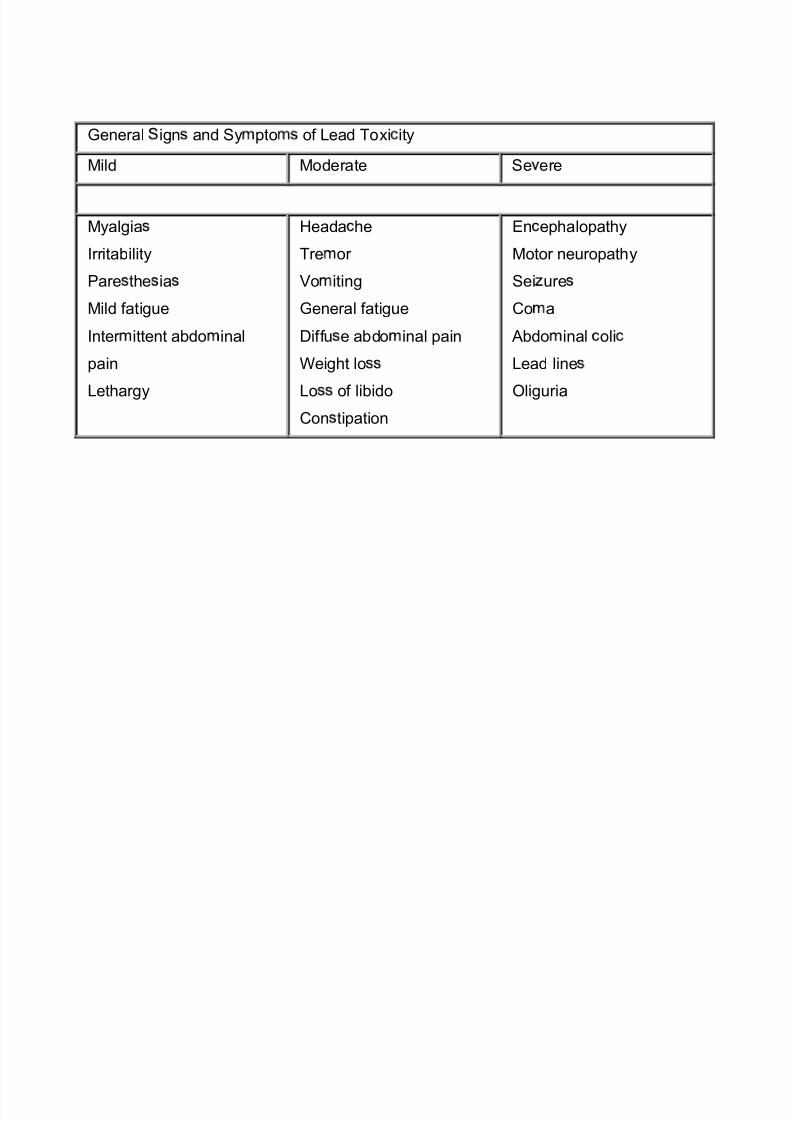
General ign and Sy pto of Lead Toxi ity
Mild Moderate Se ere
Myalgia
Irr itability
Pare the ia
Mild fatigue
Inter ittent abdo inal
pain
Lethargy
Heada he
Tre or
Vo iting
General fatigue
Diffu e abdo inal pain
Weight lo
Lo of libido
Con tipation
En ephalopathy
Motor neuropathy
Sei ure
Co a
Abdo inal oli
Lead line
Oligur ia

8/8/2019 Lead & Mercury Toxicity2
http://slidepdf.com/reader/full/lead-mercury-toxicity2 18/34
Diagnosis
A. hole Blood Lead concentration
Most widely used screening test Best measure for recent exposure
Interpretation of lead levels:
less than 10 ug/dL - not considered indicative of lead poisoning
10-14 ug/dL - border zone
15-19 ug/dL - mandates more careful follow-up
20-69 ug/dL - calls for full medical evaluation, detailed enviromentaland behavioral history, physical examination, and test for iron-deficiency
70 ug/dL constitutes medical emergency
B. ree Erythrocyte Protoporphyrin Test ( EP)
best screening test for chronic but not acute lead intoxication
Elevation of EP persists long after the cessation of lead exposure
All children between 9 months and 6 years of age should receive aEP test
better measure of body-lead burden than blood-lead but still, bothtests should be used
EP level higher than 35 ug/dL and a blood-lead level higher than 10ug/dL indicate excess lead exposure and require further medicalevaluation and environmental investigation
8/8/2019 Lead & Mercury Toxicity2
http://slidepdf.com/reader/full/lead-mercury-toxicity2 19/34
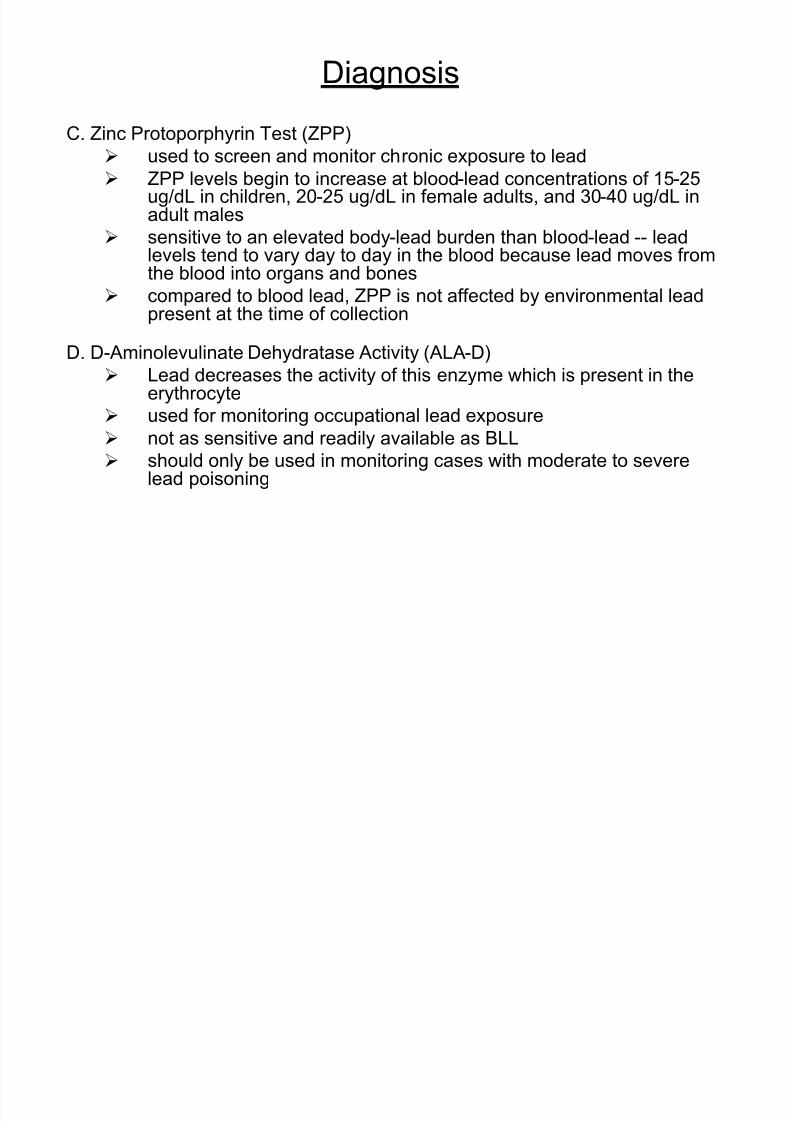
C. Zinc Protoporphyrin Test (ZPP) used to screen and monitor chronic exposure to lead
ZPP levels begin to increase at blood-lead concentrations of 15-25ug/dL in children, 20-25 ug/dL in female adults, and 30-40 ug/dL inadult males
sensitive to an elevated body-lead burden than blood-lead -- leadlevels tend to vary day to day in the blood because lead moves from
the blood into organs and bones compared to blood lead, ZPP is not affected by environmental lead
present at the time of collection
D. D- Aminolevulinate Dehydratase Activity (ALA-D)
Lead decreases the activity of this enzyme which is present in theerythrocyte
used for monitoring occupational lead exposure not as sensitive and readily available as BLL
should only be used in monitoring cases with moderate to severelead poisoning
Diagnosis

8/8/2019 Lead & Mercury Toxicity2
http://slidepdf.com/reader/full/lead-mercury-toxicity2 20/34
A. ut decontamination
B. Elimination enhancement
± hemodialysis enhance excretion of calcium disodium EDTA chelated lead
± whole bowel irrigation remove lead from I tract
C.S
upportive measures ± screening: free erythrocyte protoporphyrin test
± radiology
± blood-lead levels: 20-24 ug/dL, 25-44 ug/dL, 45-69 ug/dL, >70 ug/dL
D. Antidotes
± calcium disodium EDTA
± dimercaprol
± DMPS
± DMS A
± D-penicillamine
Treatment

8/8/2019 Lead & Mercury Toxicity2
http://slidepdf.com/reader/full/lead-mercury-toxicity2 21/34
Mercury Toxicity

8/8/2019 Lead & Mercury Toxicity2
http://slidepdf.com/reader/full/lead-mercury-toxicity2 22/34
± Mercury is a metal found in various forms:
a. rganic mercury
Mercury combined with carbon
b. Inorganic mercury
Compounds which contain mercury in combination with non-carbonsubstances such as chlorine, oxygen, or sulfur
c. Elemental mercury
± Common ways in which people are exposed include breathing
contaminated air, eating contaminated fish, and through the use of mercury
based amalgams (fillings) in dental treatments.
± Can also enter the body through direct skin contact

8/8/2019 Lead & Mercury Toxicity2
http://slidepdf.com/reader/full/lead-mercury-toxicity2 23/34
A. Nature of Jobs exposed to
Mercury
Battery manufacturing
Disinfectant industry

8/8/2019 Lead & Mercury Toxicity2
http://slidepdf.com/reader/full/lead-mercury-toxicity2 24/34
A. Nature of Jobs exposed to
Mercury
armer
ur makers

8/8/2019 Lead & Mercury Toxicity2
http://slidepdf.com/reader/full/lead-mercury-toxicity2 25/34
A. Nature of Jobs exposed to
Mercury
Insecticide makers Embalmers

8/8/2019 Lead & Mercury Toxicity2
http://slidepdf.com/reader/full/lead-mercury-toxicity2 26/34

8/8/2019 Lead & Mercury Toxicity2
http://slidepdf.com/reader/full/lead-mercury-toxicity2 27/34
B. Clinical PresentationPharmacokinetics
Absorption:
± mercury distributes to all parts of the body on absorption (peak over 1-2 days)
± widely distributed to the liver, kidney, blood and muscle
± After inhalation, elemental mercury is readily absorbed through the alveolar
membrane and is transported by blood to the brain and other tissues of the
nervous system.
Distribution:
± Elemental mercury easily penetrates the BBB and accumulates in brain tissue
± same areas of the brain are affected by both inorganic and organic mercury
± High levels accumulate in the cerebellum, brain stem (inferior olive nucleus,
subthalamic nucleus) and choroid plexus.
Elimination:
± converted in blood to mercuric ions, then excreted in the urine and feces.
± Elimination of elemental mercury primarily in the urine (half -life = 60 days).
± The loss of mercury from the lungs (half -life = 1.7 days), from the kidney (half -
life = 64 days), and from the head (half -life = 21 days).
8/8/2019 Lead & Mercury Toxicity2
http://slidepdf.com/reader/full/lead-mercury-toxicity2 28/34
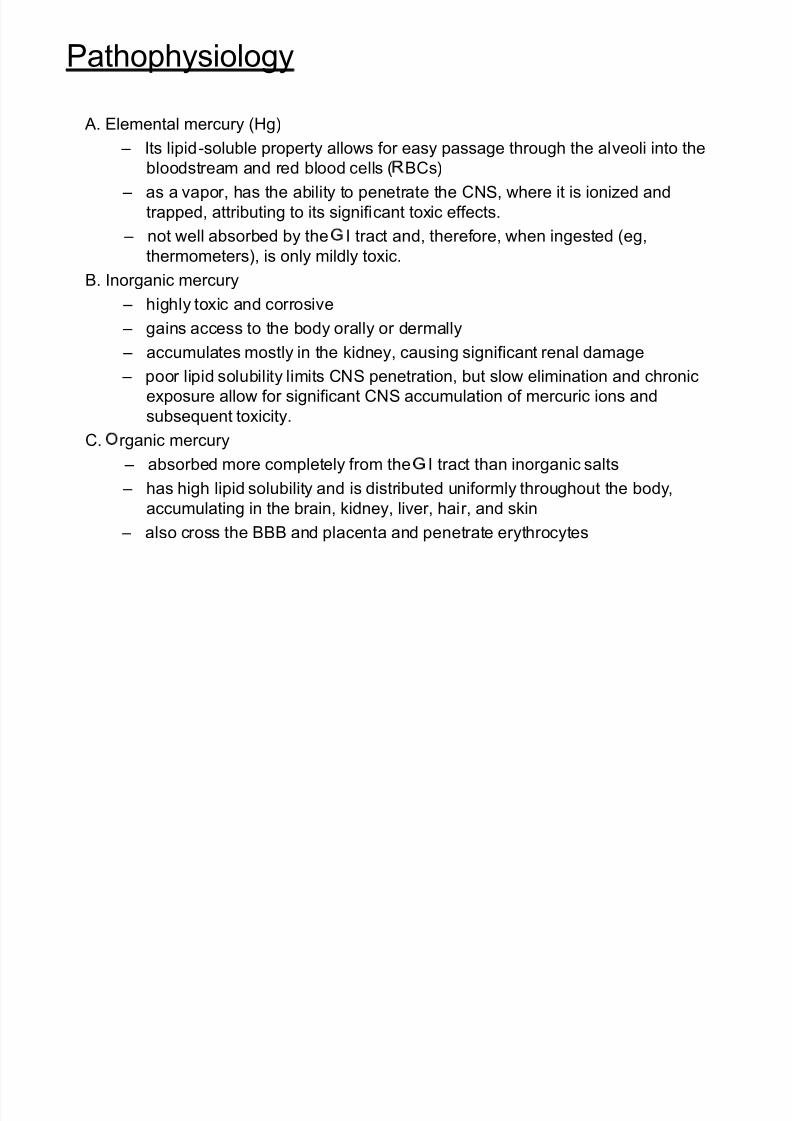
Pathophysiology
A. Elemental mercury (Hg)
± Its lipid-soluble property allows for easy passage through the alveoli into thebloodstream and red blood cells ( BCs)
± as a vapor, has the ability to penetrate the CNS, where it is ionized and
trapped, attributing to its significant toxic effects.
± not well absorbed by the I tract and, therefore, when ingested (eg,
thermometers), is only mildly toxic.
B. Inorganic mercury ± highly toxic and corrosive
± gains access to the body orally or dermally
± accumulates mostly in the kidney, causing significant renal damage
± poor lipid solubility limits CNS penetration, but slow elimination and chronic
exposure allow for significant CNS accumulation of mercuric ions and
subsequent toxicity.C. rganic mercury
± absorbed more completely from the I tract than inorganic salts
± has high lipid solubility and is distributed uniformly throughout the body,
accumulating in the brain, kidney, liver, hair, and skin
± also cross the BBB and placenta and penetrate erythrocytes

8/8/2019 Lead & Mercury Toxicity2
http://slidepdf.com/reader/full/lead-mercury-toxicity2 29/34
Signs and Symptoms
Three signs characterize the diagnosis of industrial mercurialism:
gingivitis, tremor of extremities, and emotional instability.
A. Neurologic Effects
± Tremor, rigidity and truncal unsteadiness impairing gait may
produce a Parkinsonian syndrome (basal ganglia and cerebellum
involved) ± Defects in memory (temporal lobe involved)
B. Ophthalmologic Effects
± brown reflex ± bilateral, symmetrical and varies in intensity from
light brown to coffee brown (mercurialentis).
± ine punctate opacities present bilaterally and most evident inanterior cortex of lens.
± ell-marked vascularity is observed at the corneo-scleral junction.

8/8/2019 Lead & Mercury Toxicity2
http://slidepdf.com/reader/full/lead-mercury-toxicity2 30/34
Signs and Symptoms
C . Renal Effects ± overt renal tubular damage
± The nephro-toxicity manifested as an acute tubular necrosis or as
an immune complex glomerulo-nephritis.
± two types of proteinuria
lomerular proteinuria - characterized by the leakage of serum proteins(predominantly high-molecular weight) through damaged glomeruli
Tubular proteinuria - consists of a variety of proteins and enzymes.
Many of these markers are low-molecular weight proteins normally
filtered through the glomerulus and then reabsorbed in the proximal
tubules.

8/8/2019 Lead & Mercury Toxicity2
http://slidepdf.com/reader/full/lead-mercury-toxicity2 31/34
Chronic, Low-Dose E posure
y Erethism (ner ousness, irritabilit ,mood instabilit , blushing)
y remor
y Personalit change
y Suicidal tendenc
y Paraesthesia
y Impaired hearingy Speech disorders
y Visual disturbance
y Abnormal refle es
y Disturbed gait
y ingi itis (inflammation of the gums)
y Impaired ner e conduction
y enal damage
y Ad erse outcome of pregnancy Infertilit
y Pneumonitis (lung disease)
y lioblastoma (brain cancer)
y Immune s stem d sfunction
Clinical Symptoms of Mercury Toxicity

8/8/2019 Lead & Mercury Toxicity2
http://slidepdf.com/reader/full/lead-mercury-toxicity2 32/34
Clinical Symptoms of Mercury Toxicity
Acute, High-Dose Exposure
astroenteritis (stomach upset)
Mouth pain Abdominal pain
Vomiting
Excessive salivation Anuria (urine production stops)
Uraemia (urine products appearing in the
blood)
Nephritis (kidney disease leading to
kidney failure) Anorexia (lack of appetite)
Ataxia (difficulty in moving)

8/8/2019 Lead & Mercury Toxicity2
http://slidepdf.com/reader/full/lead-mercury-toxicity2 33/34

8/8/2019 Lead & Mercury Toxicity2
http://slidepdf.com/reader/full/lead-mercury-toxicity2 34/34
A. ut decontamination
± should be with protected airway
B. ral Chelation Therapy
± attaching--or chelating--to metallic ions and minerals, then move
them into the body's waste disposal pathways and flush them out. Dimercaprol
DMPS
DMS A
D-Penicillamine
Treatment