lecture 13 tennyson diarrhea - columbia universitycauses of acute diarrhea infectious medications...
TRANSCRIPT
DiarrheaDiarrhea
Christina Tennyson, M.D.Assistant Professor of MedicineAssistant Professor of Medicine
Division of GastroenterologyColumbia UniversityColumbia University


DIARRHEADIARRHEASymptom: stool frequency, liquidity y p q y, q y
Sign: > 200-250 g/day
Acute Chronic
Time < 2-4 weeks > 4 weeks
Cause infection or drug manyCause infection or drug many
Outcome self-limited treat specific disease
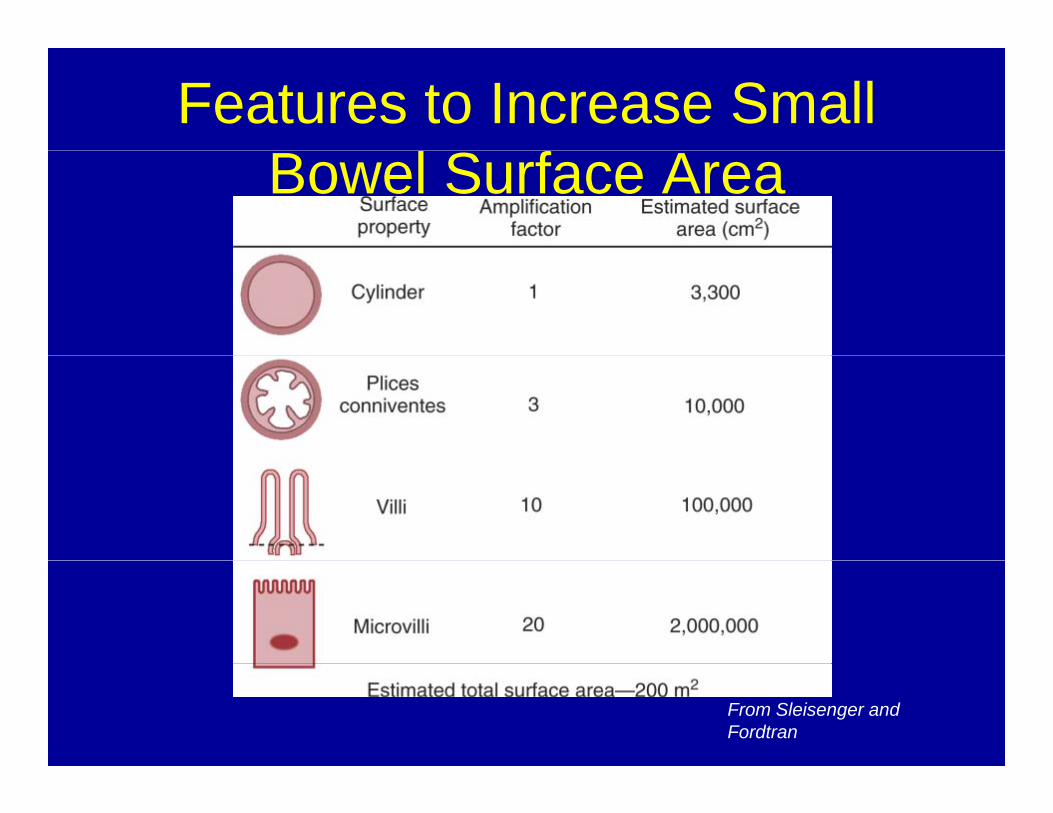
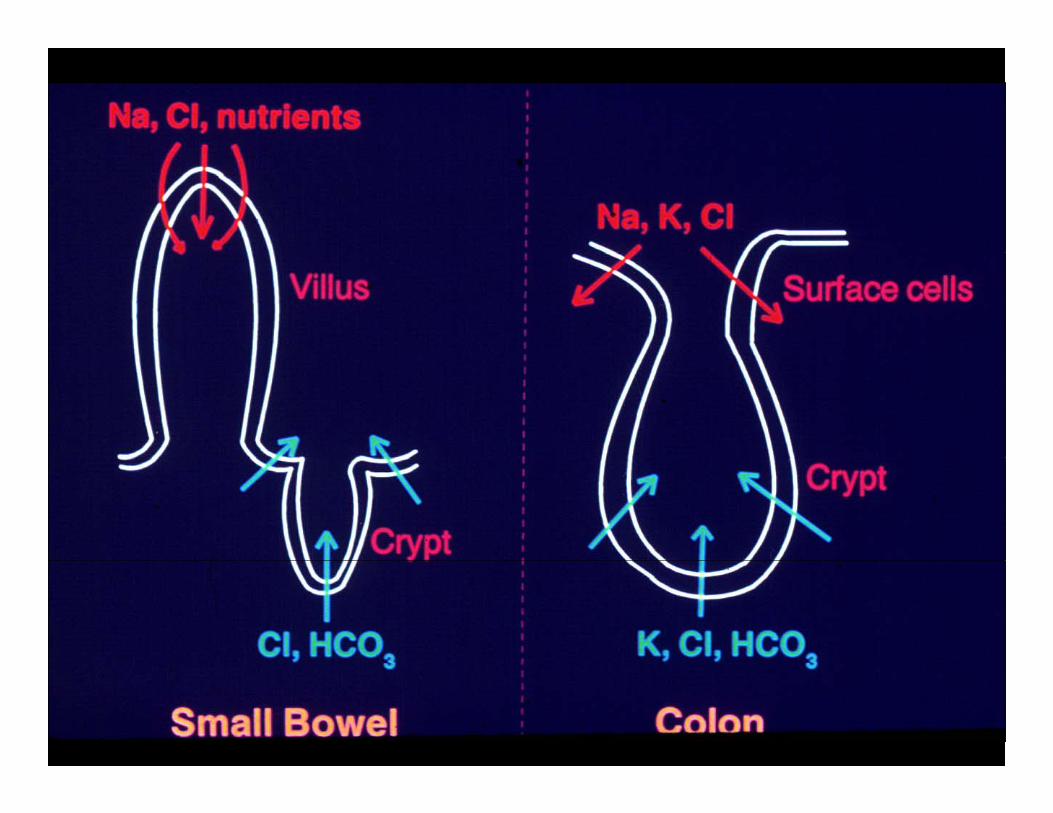
Features to Increase Small Bowel Surface Area
From Sleisenger and Fordtran



Normal mucosaNormal mucosa

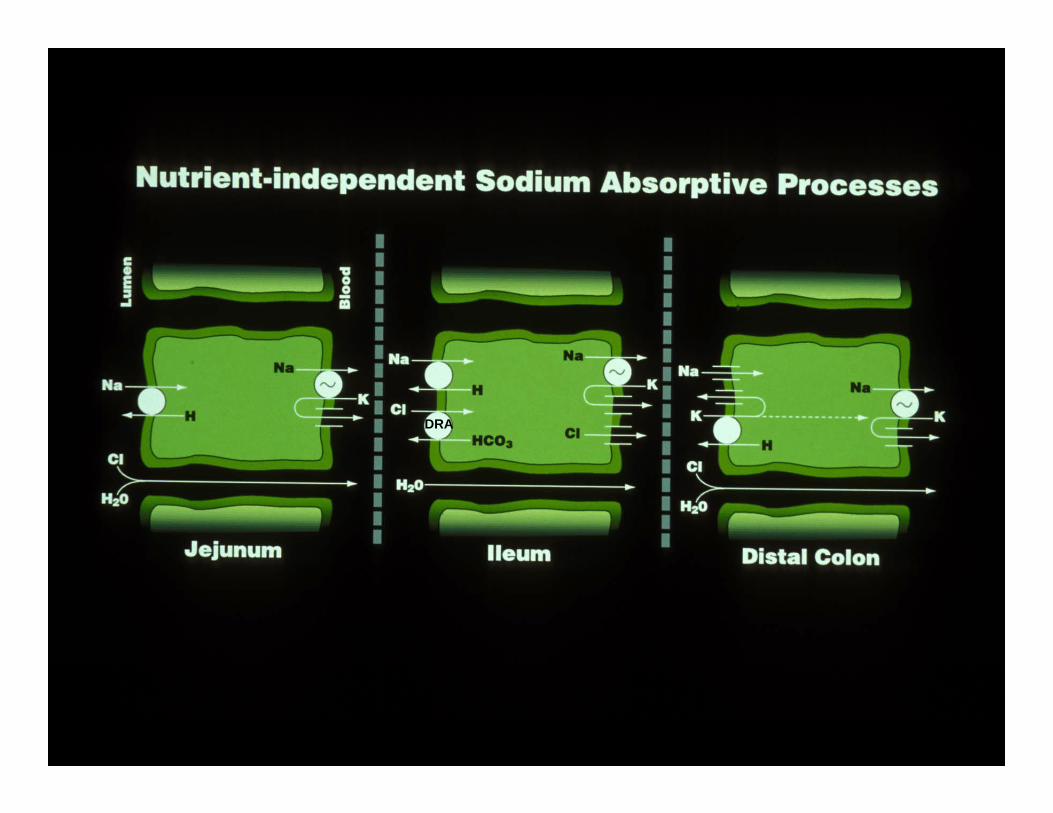
DRA
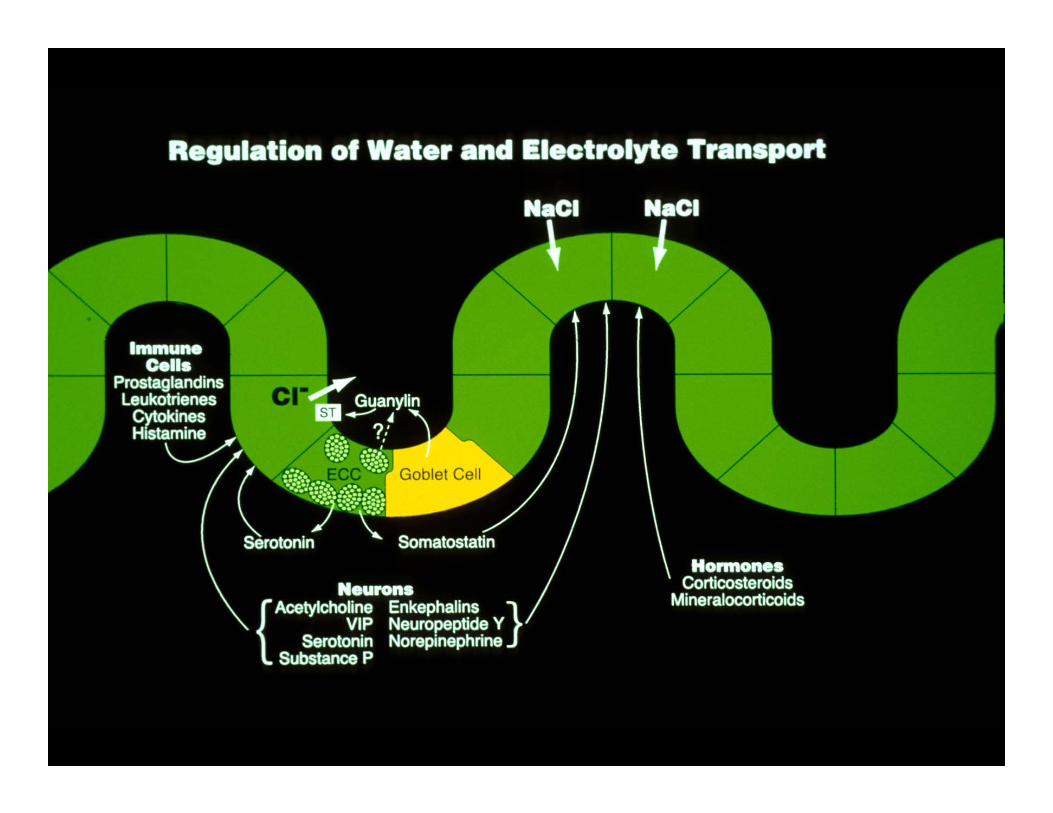
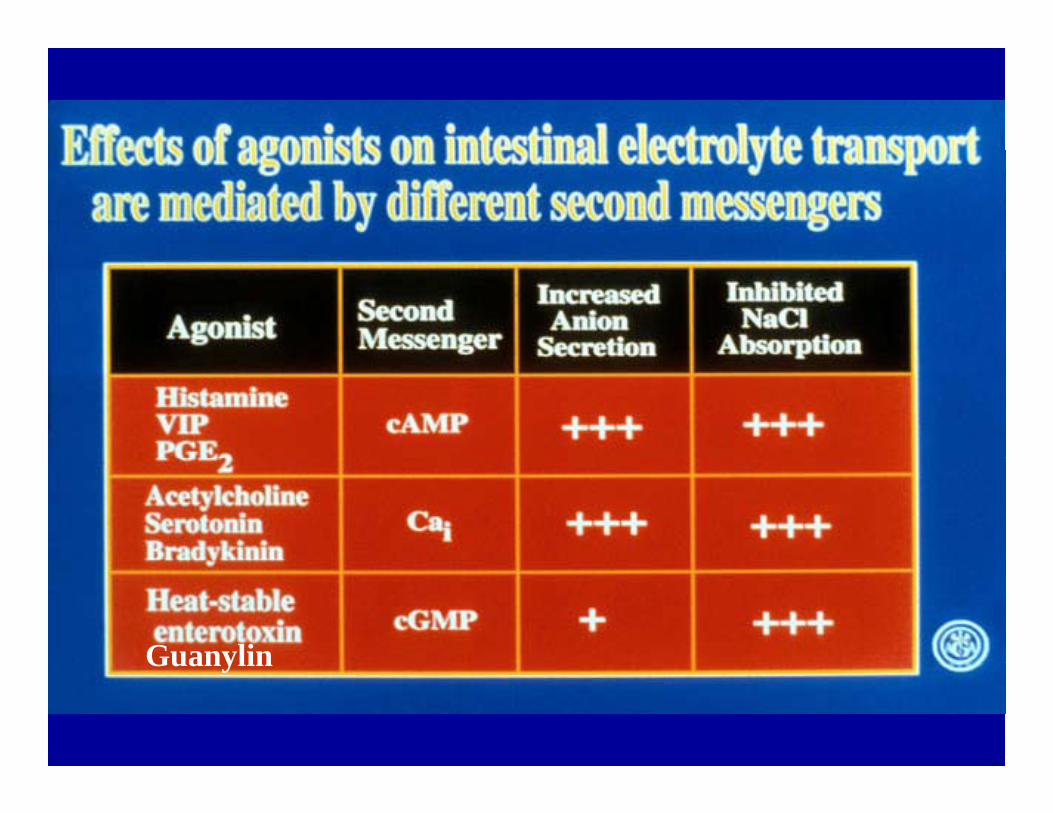
GuanylinGuanylin
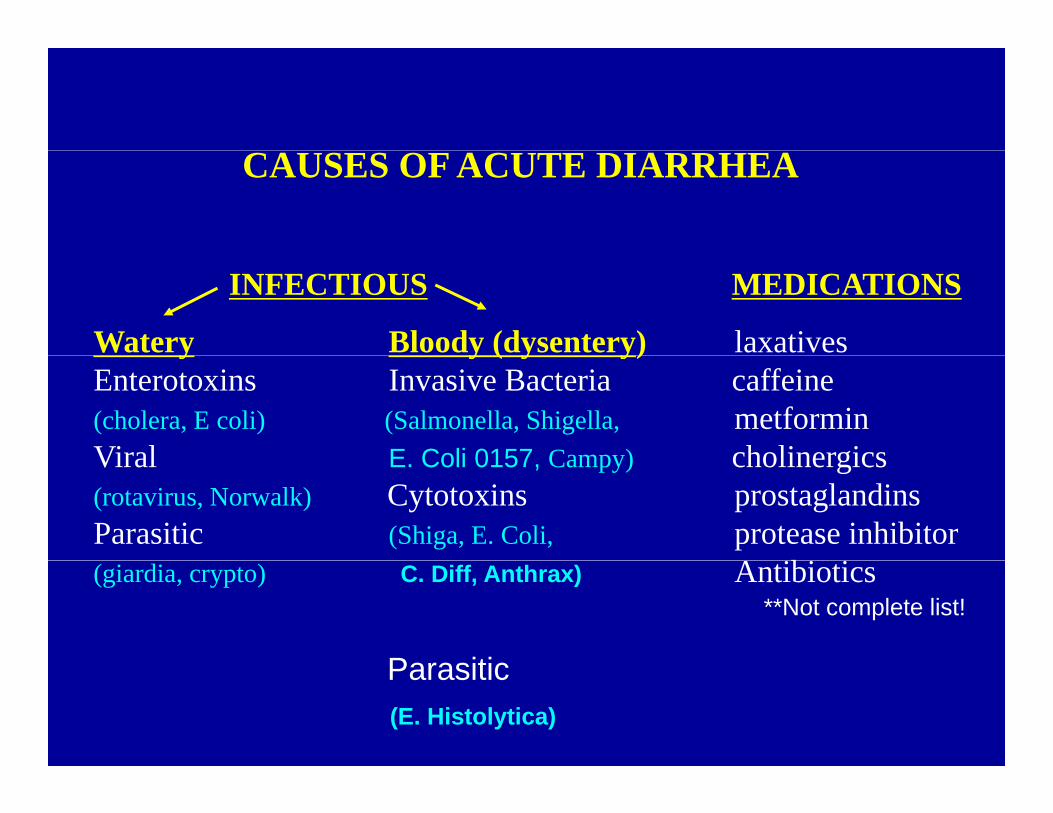
CAUSES OF ACUTE DIARRHEA
INFECTIOUS MEDICATIONS
Watery Bloody (dysentery) laxatives y y ( y y)Enterotoxins Invasive Bacteria caffeine(cholera, E coli) (Salmonella, Shigella, metforminViral E Coli 0157 Campy) cholinergicsViral E. Coli 0157, Campy) cholinergics (rotavirus, Norwalk) Cytotoxins prostaglandinsParasitic (Shiga, E. Coli, protease inhibitor
A ibi i(giardia, crypto) C. Diff, Anthrax) Antibiotics**Not complete list!
ParasiticParasitic(E. Histolytica)
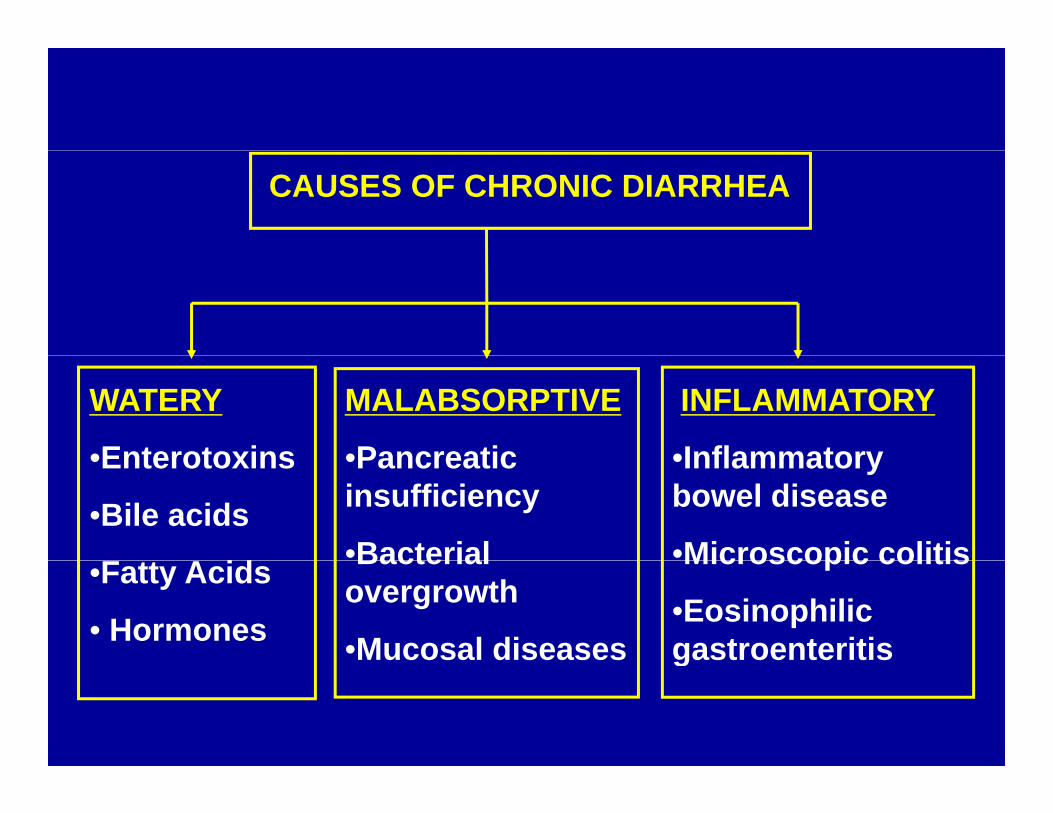
CAUSES OF CHRONIC DIARRHEA
WATERY
•Enterotoxins
INFLAMMATORY
•Inflammatory
MALABSORPTIVE
•Pancreatic•Enterotoxins
•Bile acids
F A id
•Inflammatory bowel disease
•Microscopic colitis
•Pancreatic insufficiency
•Bacterial•Fatty Acids
• Hormones
Microscopic colitis
•Eosinophilic gastroenteritis
Bacterial overgrowth
•Mucosal diseases g

Mechanisms of DiarrheaMechanisms of Diarrhea
• Osmotic (malabsorptive)Osmotic (malabsorptive)
S t ( t )• Secretory (watery)
• Inflammatory
• Motility
***Overlap exists! Diseases can involve more than one mechanism.

Stool electrolytesStool electrolytes
• 290 mOsm/kg- 2(stool K +Na)290 mOsm/kg- 2(stool K +Na)
• <50mOsm/kg SECRETORY50mOsm/kg SECRETORY– Diarrhea due to other ions present (not-measured)
• >100mOsm/kg OSMOTIC – Diarrhea due to poorly absorbed substance, electrolytes
account for only a small portion of osmotic activityy p y
• <290 mOsm/kg Contaminated by adding water to sample

OSMOTIC DIARRHEAOS O C
CAUSESI ti f l b b bl l t• Ingestion of poorly absorbable solute
Mg++ and PO4--- containing laxatives, antacids
Sorbitol in sugar free candies, gumg , gFructose containing fruits, sodaLactulose
• Acquired lactase deficiency• Acquired lactase deficiency
• Malabsorptive diseasesMalabsorptive diseasesmucosal (e.g. celiac disease, tropical sprue)maldigestion (e.g. bacterial overgrowth)

Atrophy- celiac disease

Partial atrophyPartial atrophy


Characteristics of OsmoticCharacteristics of Osmotic Diarrhea
• Low volumes (< 1 liter)• Resolves with fastingResolves with fasting• Excess stool osmotic gap > 100 mOsm/kg
L t l H ( b h d t l b ti )• Low stool pH (carbohydrate malabsorption)

Causes of Secretory DiarrheaCauses of Secretory Diarrhea
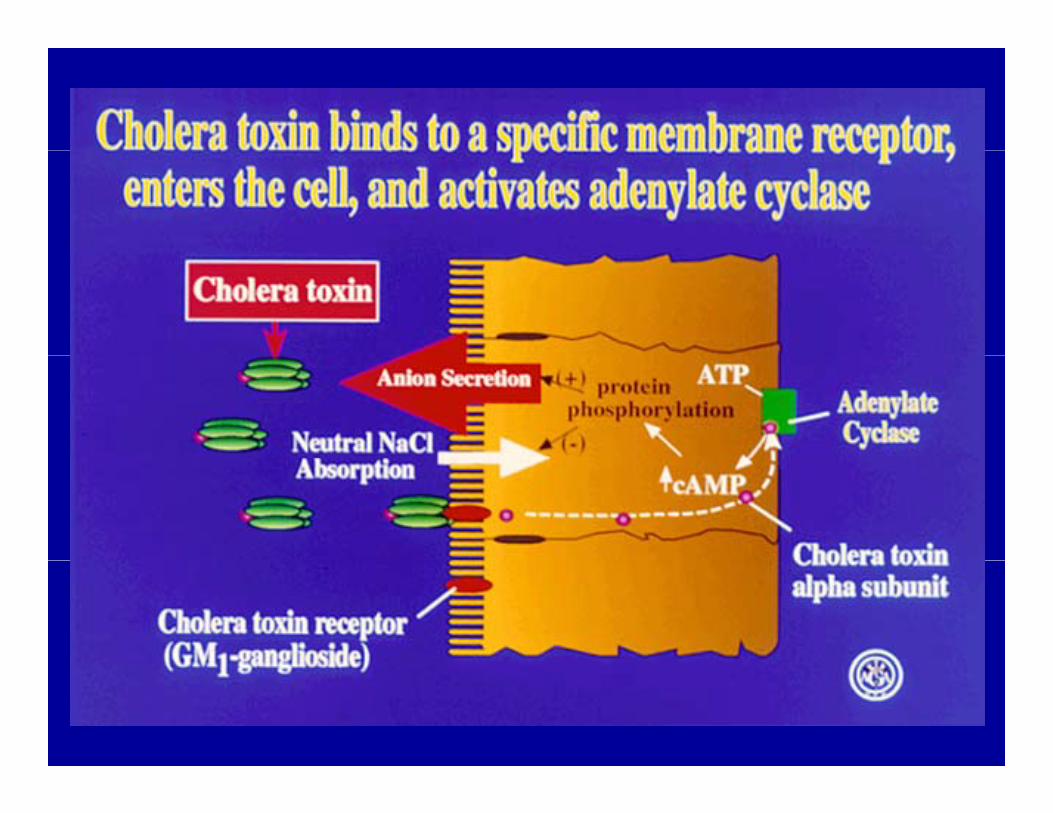
• Bacterial EnterotoxinsBacterial Enterotoxins(cholera, E. Coli LT,ST)
• Hormones and NeurotransmittersHormones and Neurotransmitters(VIP, 5-HT, Substance P, calcitonin, acetylcholine)y )
• Inflammation(prostaglandins, leukotrienes, (p gcytokines, histamine)
• Bile acids and hydroxylated fatty acidsy y y
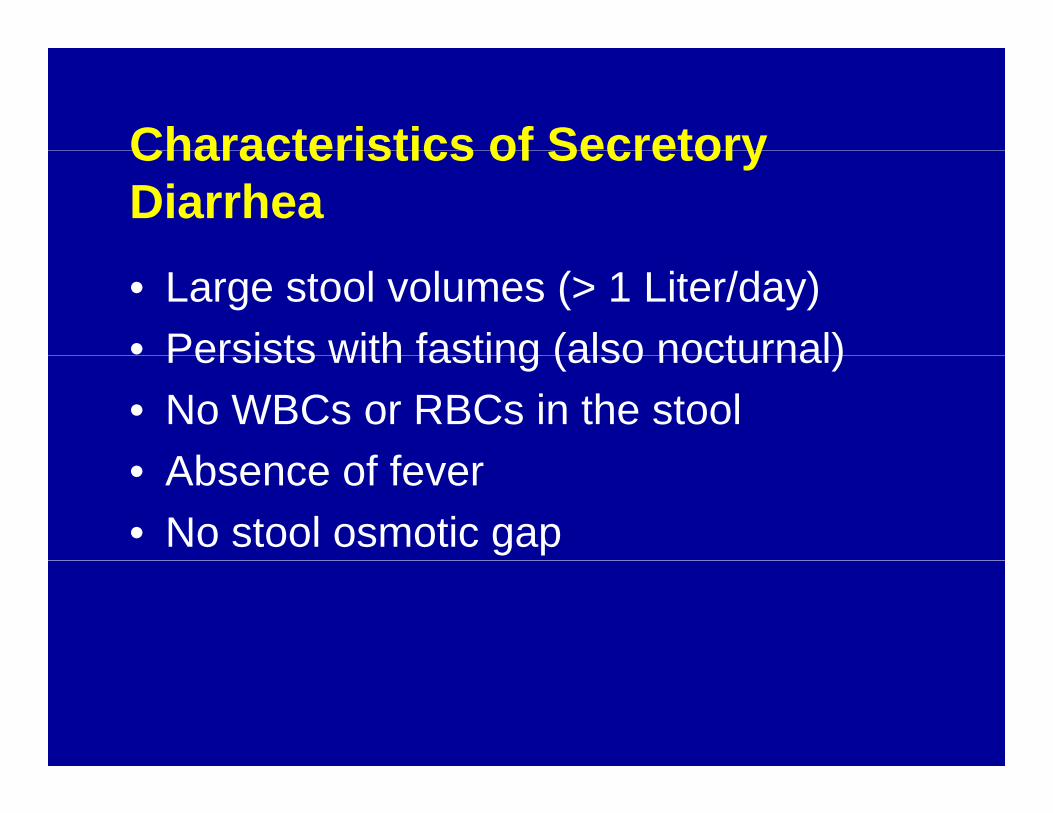
Characteristics of SecretoryCharacteristics of Secretory Diarrhea
• Large stool volumes (> 1 Liter/day)• Persists with fasting (also nocturnal)Persists with fasting (also nocturnal)• No WBCs or RBCs in the stool
Ab f f• Absence of fever• No stool osmotic gap


Vibrio Cholerae
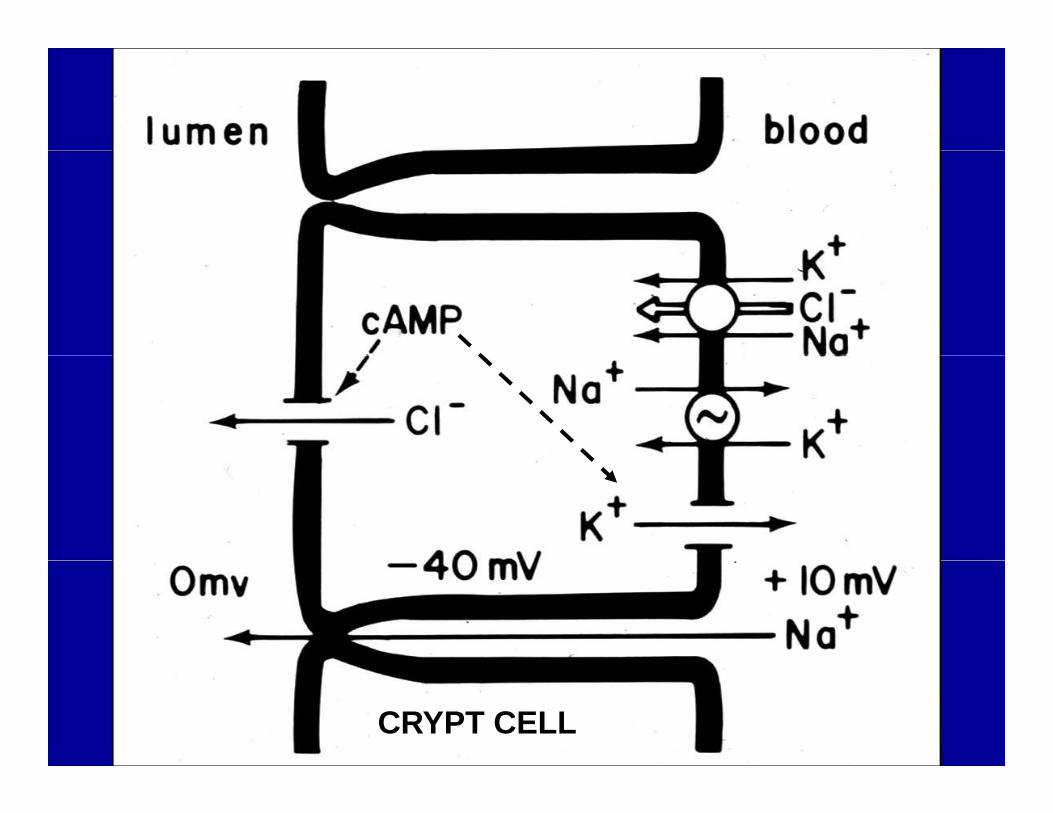
CRYPT CELL
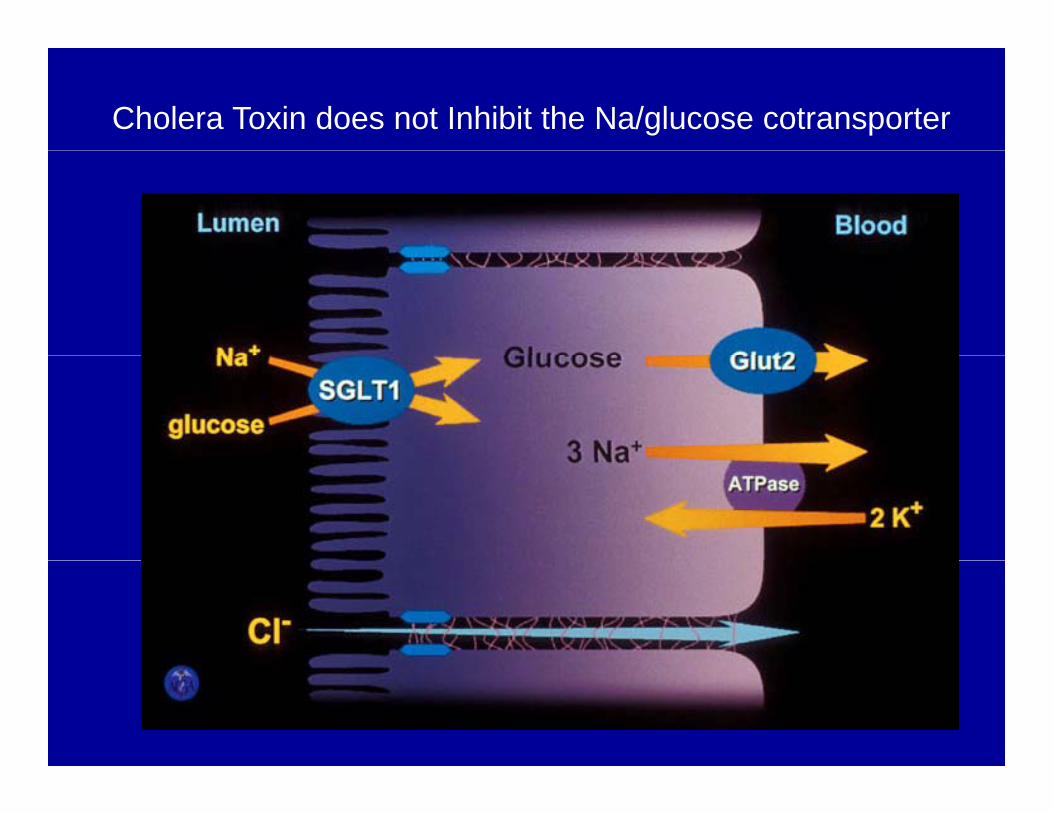
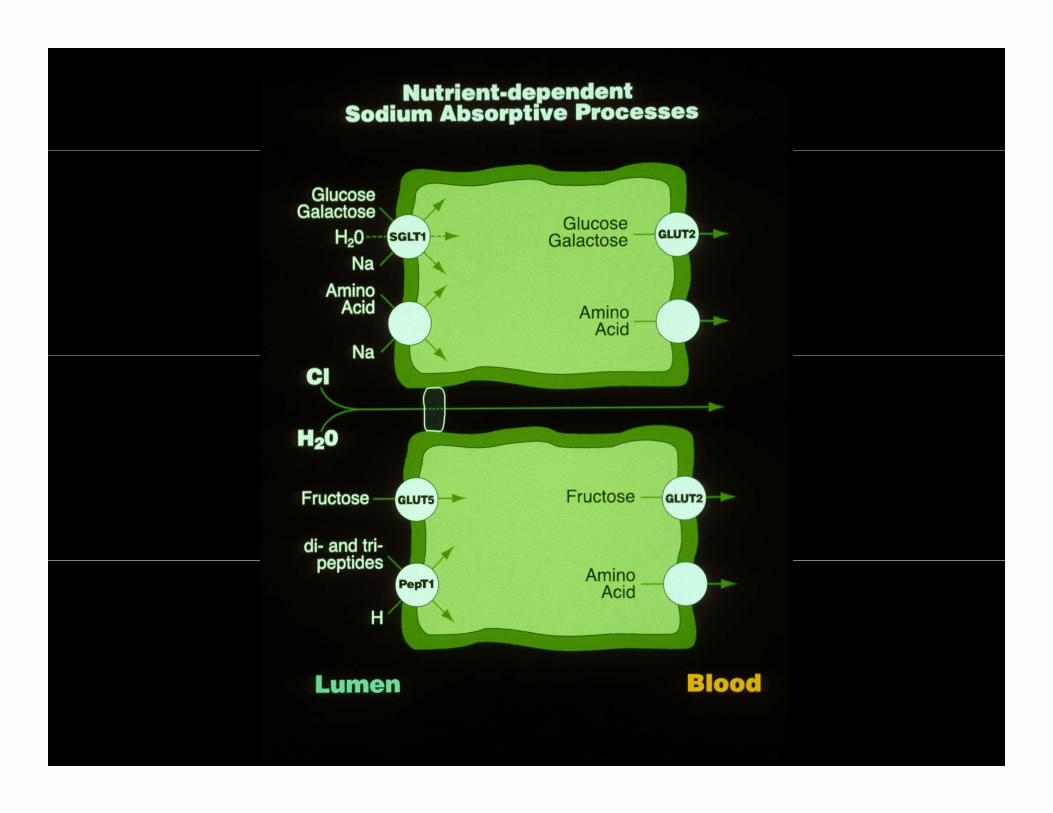
Cholera Toxin does not Inhibit the Na/glucose cotransporter

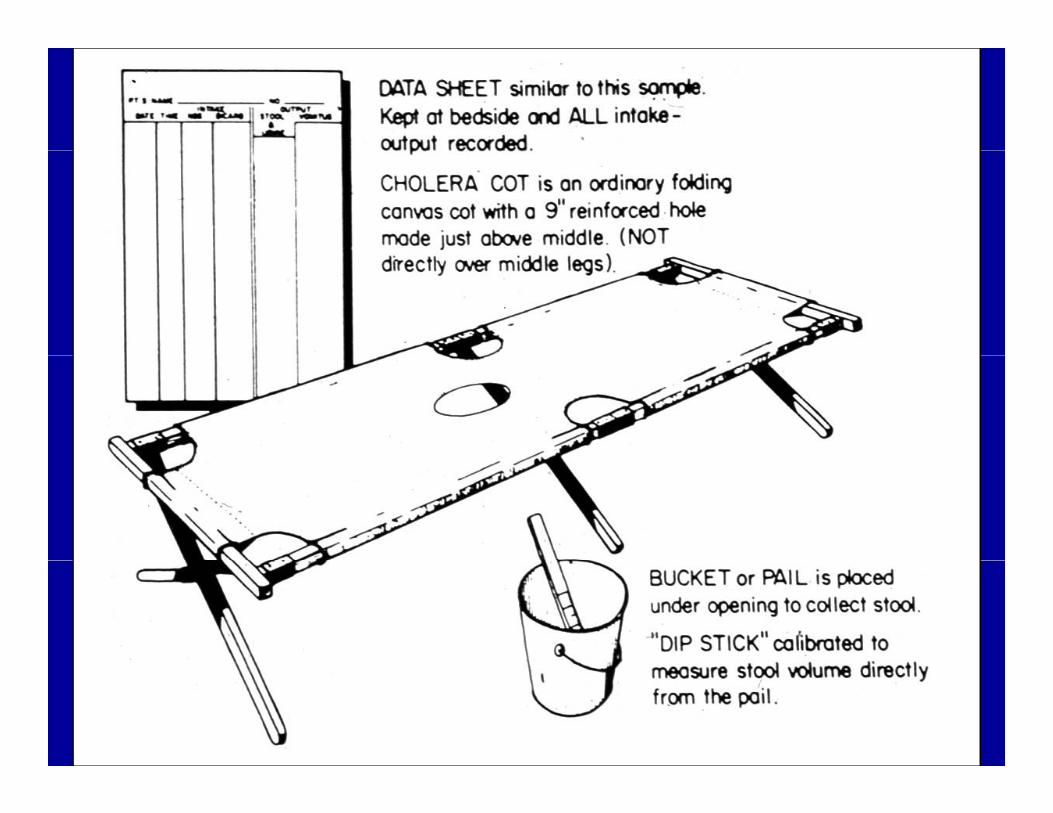
TREATMENT OF DIARRHEATREATMENT OF DIARRHEAORAL REHYDRATION SOLUTIONS
• Utilize Na/glucose co-transporters• Requires intact villus epitheliumRequires intact villus epithelium• Solution must contain Na and glucose
S l ti t b i l l ti• Solution must be near isosmolar relative to plasma



Hormone-secreting Tumors (rare)
Agent Source Cell mediator Mechanism
VIP pancreatic tumor cAMP secretionVIP pancreatic tumor cAMP secretionganglioneuroma
5HT carcinoid tumor calcium secretion (serotonin) (intestine, lung) motility
Gastrin gastrinoma calcium acid secretion
Calcitonin medullary CA calcium secretion thyroid


Viral diarrhea• Rotavirus (infants)( )
Norwalk agent (cruise-ship diarrhea)• Invades the intestinal epithelium with select
ill ll dvillus cell damage• Mechanism of diarrhea
1) absorption due to villus damage1) absorption due to villus damage2) secretion due to
activation of the enteric nervous systemNSP4 rota-toxin
• Treatment with ORS effective
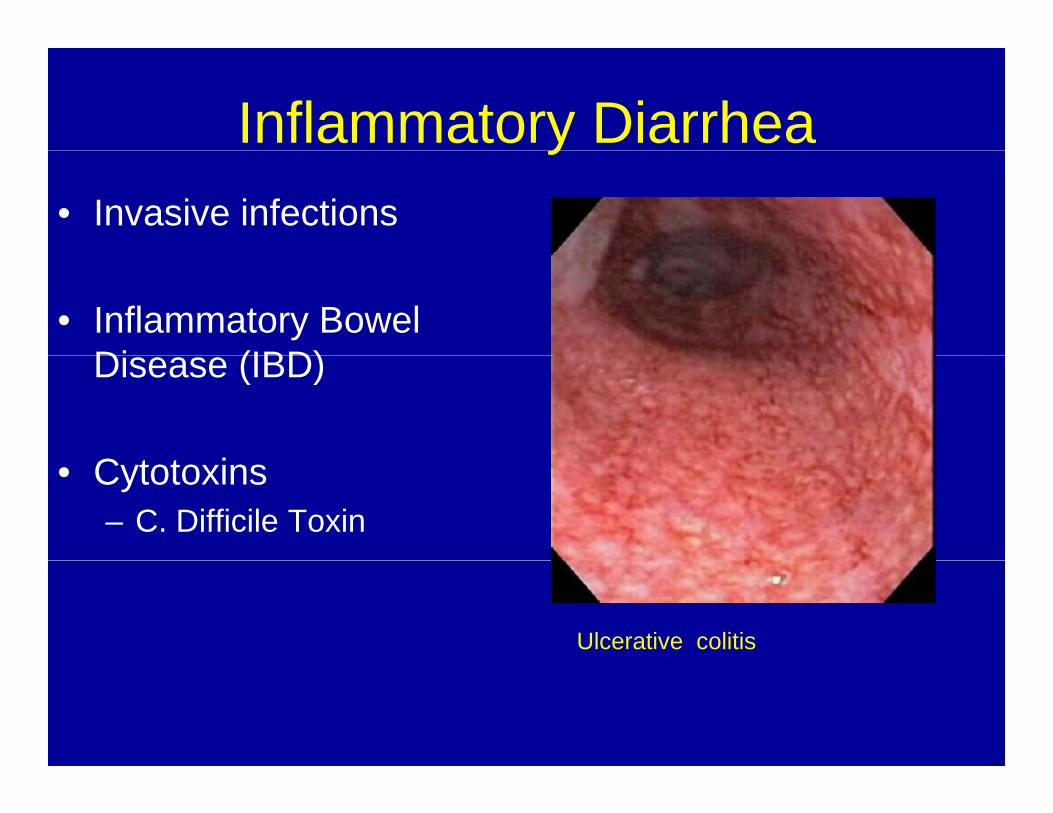
Inflammatory Diarrheay• Invasive infections
• Inflammatory Bowel Di (IBD)Disease (IBD)
C i• Cytotoxins – C. Difficile Toxin
Ulcerative colitis

Colectomy specimen following fulminant Clostridium difficile
Intestinal Inflammation
• Acute inflammationProstaglandins, leukotrienes, free g , ,radicals, PAF, histamine and others stimulate active secretion
• Chronic inflammationCytokines (e g IFN-γ TNF-α) suppressCytokines (e.g. IFN γ, TNF α) suppress both absorption and secretion

Characteristics of inflammatoryCharacteristics of inflammatory diarrhea:
• Damage of intestinal epithelium• Exudation of protein blood and pus intoExudation of protein, blood and pus into
intestinal lumen• Urgency frequency tenesmus with• Urgency, frequency, tenesmus with
recto-sigmoid disease Bl d t t l• Bloody or watery stools
• Low serum protein and albumin levels
TreatmentTreatment• Oral rehydration• Oral rehydration• Clinical evaluation• Stool tests as needed• Antimicrobial therapy if indicatedpy• Anti-diarrheal medication if indicated• Treat underlying disease• Treat underlying disease
