lecture 20 physiopathology of the female reproductive system. hipotalamo-pituitary-ovarian axis....
TRANSCRIPT

Lecture 20Lecture 20
PHYSIOPATHOLOGY OF THE PHYSIOPATHOLOGY OF THE FEMALE REPRODUCTIVE SYSTEM. FEMALE REPRODUCTIVE SYSTEM.
HIPOTALAMO-PITUITARY-OVARIAN HIPOTALAMO-PITUITARY-OVARIAN AXIS. AXIS.
ENDOMETRIAL CYCLE AND ENDOMETRIAL CYCLE AND MENSTRUATIONMENSTRUATION
Prof. Vlad TICA, MD, PhDProf. Vlad TICA, MD, PhD

OVARIAN CYCLEAs graafian follicle develops, primary
oocyte completes meiosis I
One daughter cell (secondary oocyte) receives cytoplasm
Other daughter, now a small polar body degenerates
Secondary oocyte arrests at metaphase II
Only fertilized ova complete meiosis II

OVARIAN CYCLESecondary oocyte is part of the graafian follicle
Granulosa cells form a layer around outside of follicle
Oocyte sits on a mound of this layer the cumulus oophorus
Corona radiata – ring of granulosa cells enclosing the secondary oocyte
Zona pellucida – gelatinous layer between oocyte and radiata forms barrier to sperm penetration

OVULATION10-14 days after start of
menstruation
Only 1 follicle survives
Others become atretic follicles (degenerate)
Surviving graafian follicle forms bulge on surface of ovary
Secretes increasing levels of estrogen
Graffian follicle releases secondary oocyte
Into uterine tube at ovulation

OVULATION FROM A HUMAN OVARY

FERTILIZATION
If a sperm passes through the corona radiata and zona pellucida and enters the cytoplasm of the occyte
now the oocyte completes meiosis II
with formation of another polar body
If not fertilized within 2 days, secondary oocyte degenerates

OVARIAN CYCLEFollowing ovulation empty follicle under the influence
of LH becomes a corpus luteumwhich secretes progesterone and estradiolNon-fertile cycle, becomes corpus albicans (non-
functional remnant)

PITUITARY-OVARIAN AXISHormonal interactions between anterior pituitary and
ovaries
Anterior pituitary secretes luteinizing hormone (LH) and follicle-stimulating hormone (FSH)Both promote cyclic changes in the ovaries
Both are controlled by GnRH from hypothalamusFSH secretion slightly greater during early phase
of menstrual cycleLH secretion greatly exceeds FSH secretion prior
to ovulationNot clearly understood but believed to result from
negative feedback effects

HYPOTHALAMIC- PITUITARY-OVARIAN AXIS

MENSTRUAL (MONTHLY) CYCLEApproximately month-long cycle of ovarian activity
humans, apes, old world monkeys
Menstruation – characterized by shedding of endometrial lining accompanied by bleeding
And sexual receptivity anytime throughout the cycle
Nonprimate female mammals have estrous cycles
no shedding of endometrium and receptivity is limited
estrous animals that bleed (dogs and cats) is due to high estrogen that accompanies receptive period

MENSTRUAL CYCLEIn humans is about 28 days
Day 1 is taken to be the first day of menstruation
Days 1 thru ovulation constitutes the follicular phase
Time from ovulation to menstruation is luteal phase
Endometrial changes are called: menstrual, proliferative and secretory phases

FOLLICULAR PHASELasts from day 1 to ~13
Dominated by growth and death of a cohort of primary follicles into secondary follicleswith one survivor becoming
a graafian follicle
which will undergo ovulation
As follicles grow granulosa cells secrete increasing amounts of estradiolReaching peak about day 12

FOLLICULAR PHASEFollicular growth and
estradiol secretion dependent on FSH
FSH and estradiol induce
formation of FSH receptors in granulosa cells
Follicles increasingly sensitive to the same level of FSH
At same time – FSH and estradiol recruit LH receptors in graafian follicle

FOLLICULAR PHASERapidly rising estradiol
secretion:
Hypothalamus increases pulses of GnRH
Anterior pituitary sensitivity to GnRH increases:
results in greater LH secretion
Positive feedback between estrogen and anterior pituitary
results in LH surge, peaks 16 hrs before ovulation and causes ovulation
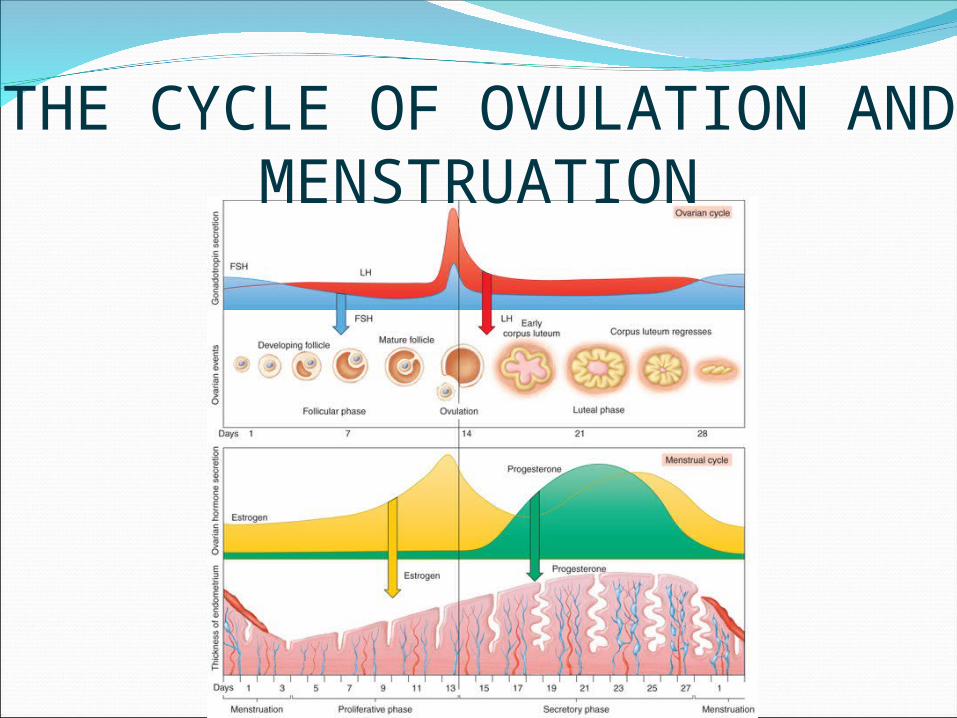
THE CYCLE OF OVULATION AND MENSTRUATION

THE LUTEAL PHASEAfter ovulation – LH causes empty follicle to become
corpus luteum
which secretes Estrogen and Progesterone
Progesterone levels rise and peak about a week after ovulation
Development of new follicles and another ovulation inhibited by:
high progesterone and estrogen exert strong negative feedback on LH and FSH
inhibin from corpus luteum further suppresses FSH

THE LUTEAL PHASENo fertilization →
corpus luteum regresses
Estrogen and
Progesterone levels decline
with menstruation and new cycle of follicle development

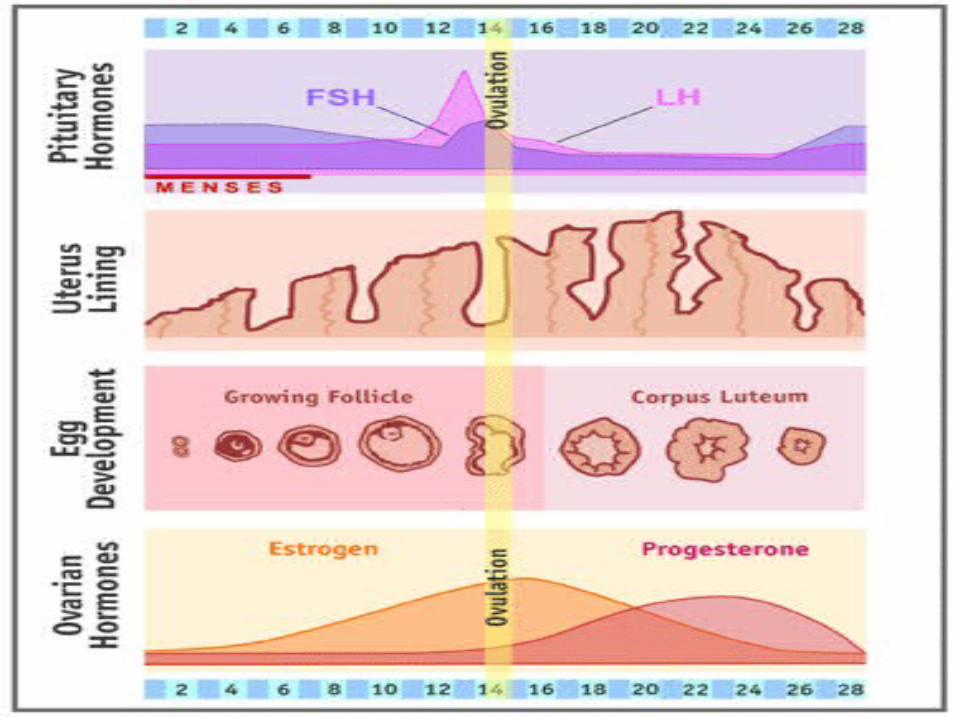
CYCLIC CHANGES IN THE ENDOMETRIUM
Driven by cyclic changes in estrogen and progesterone levels
Proliferative phase (menstration cycle) occurs during follicular phase - ↑ levels of estrogen
stimulates growth of endometrial lining and development of spiral arteries
causes cervical mucus to become thin and watery to allow sperm penetration

CYCLIC CHANGES IN THE ENDOMETRIUM
Secretory phase occurs during luteal phase – endometrium becomes ready for implantation
Progesterone stimulates development of uterine glands
Progesterone and Estrogen cause endometrium to become thick, vascular, and spongy
Progesterone causes cervical mucus to thicken and become sticky

CYCLIC CHANGES IN THE ENDOMETRIUM
Menstrual phase results from drop in Progesterone and Estrogen following corpus luteum degeneration
Low progesterone: constriction of spiral arteries
Blood flow stops followed by necrosis and sloughing of endometrium

ENDOCRINE CONTROL OF
THE OVARIAN CYCLE

FACTORS AFFECTING MENSTRUAL CYCLE
Release of GnRH is regulated not only by hormonal feedback but also by input from higher brain centers
Olfactory system can send activity to hypothalamus in response to pheromones
Can cause the “dormitory effect” in which cycles of roommates become synchronized

FACTORS AFFECTING MENSTRUAL CYCLE
Limbic system input to the hypothalamus:
In times of stress can cause functional amenorrhea (cessation of menstruation)
Also occurs in very thin or athletic females with low body weight
may be related to reduced leptin secretion by small adipocytes

CONTRACEPTIVE METHODS
Oral contraceptive pills – synthetic estrogen and progesterone
Taken daily for 3 weeks after menstrual period
Mimic corpus luteum, so that negative feedback inhibits ovulation
Placebo pills taken in 4th wk to permit menstruation

RHYTHM METHODInvolves daily measurement of oral basal body
temperature (BT) upon awakening because:
ovarian steroids cause BT changes
declining Estrogen on day of LH surge causes a slight drop in BT
rising Progesterone on day after LH peak causes elevated BT

MENOPAUSECessation of ovarian activity and menstruation
roughly ~50 years
Ovaries depleted of follicles produce no estrogen
LH and FSH are high because of no negative feedback
Lack of Estrogen from ovaries most responsible for:
Hot flashes, osteoporosis, and increased risk of atherosclerosis

THANKS !