left bundle branch block-type ventricular tachycardia originating from the left ventricular septum...
TRANSCRIPT
CASE REPORT
Left bundle branch block-type ventricular tachycardia originatingfrom the left ventricular septum in a patientwith cardiac sarcoidosis
Yasuo Okumura & Ichiro Watanabe & Toshiko Nakai &Kimie Ohkubo & Tatsuya Kofune & Sonoko Ashino &
Masayoshi Kofune & Atsushi Hirayama
Received: 4 May 2009 /Accepted: 25 May 2009 /Published online: 21 July 2009# Springer Science + Business Media, LLC 2009
Abstract This case report describes a left bundle branchblock (LBBB)-type ventricular tachycardia (VT) with aunique reentrant circuit in a patient with cardiac sarcoido-sis. The VT morphology and pace mapping supported anexit site of the VT from the basal posterior right ventricle(RV) septum. Nonetheless, concealed entrainment wasestablished by pacing from a septal left ventricular (LV)site recording a diastolic potential, opposite site to the RVsite. A point ablation at that LV site could successfullyterminate the VT, suggesting that a critical isthmus waslocated on the LV side of the interventricular septumdespite the demonstration of an LBBB-type VT.
Keywords Cardiac sarcoidosis . Ventricular tachycardia .
Catheter ablation
1 Case presentation
A 59-year-old man was diagnosed as having sarcoidosis8 years prior because of bilateral hilar lymphadenopathy onthe chest X-ray and a transbronchinal biopsy showingnumerous noncaseating granulomas. He was previouslyimplanted with an implantable cardioverter defibrillator(ICD) for a drug-refractory ventricular tachycardia (VT).Over the past 2 years, he had been free from any symptomson an oral administration of amiodarone, but again
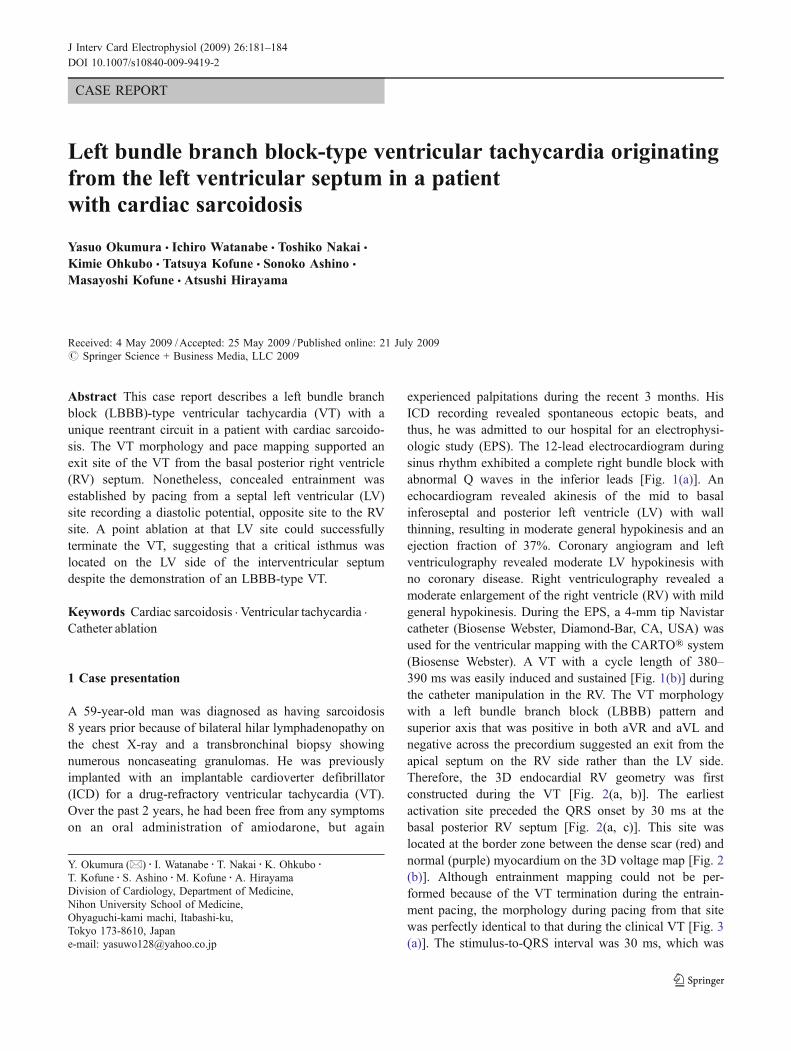
experienced palpitations during the recent 3 months. HisICD recording revealed spontaneous ectopic beats, andthus, he was admitted to our hospital for an electrophysi-ologic study (EPS). The 12-lead electrocardiogram duringsinus rhythm exhibited a complete right bundle block withabnormal Q waves in the inferior leads [Fig. 1(a)]. Anechocardiogram revealed akinesis of the mid to basalinferoseptal and posterior left ventricle (LV) with wallthinning, resulting in moderate general hypokinesis and anejection fraction of 37%. Coronary angiogram and leftventriculography revealed moderate LV hypokinesis withno coronary disease. Right ventriculography revealed amoderate enlargement of the right ventricle (RV) with mildgeneral hypokinesis. During the EPS, a 4-mm tip Navistarcatheter (Biosense Webster, Diamond-Bar, CA, USA) wasused for the ventricular mapping with the CARTO® system(Biosense Webster). A VT with a cycle length of 380–390 ms was easily induced and sustained [Fig. 1(b)] duringthe catheter manipulation in the RV. The VT morphologywith a left bundle branch block (LBBB) pattern andsuperior axis that was positive in both aVR and aVL andnegative across the precordium suggested an exit from theapical septum on the RV side rather than the LV side.Therefore, the 3D endocardial RV geometry was firstconstructed during the VT [Fig. 2(a, b)]. The earliestactivation site preceded the QRS onset by 30 ms at thebasal posterior RV septum [Fig. 2(a, c)]. This site waslocated at the border zone between the dense scar (red) andnormal (purple) myocardium on the 3D voltage map [Fig. 2(b)]. Although entrainment mapping could not be per-formed because of the VT termination during the entrain-ment pacing, the morphology during pacing from that sitewas perfectly identical to that during the clinical VT [Fig. 3(a)]. The stimulus-to-QRS interval was 30 ms, which was
J Interv Card Electrophysiol (2009) 26:181–184DOI 10.1007/s10840-009-9419-2
Y. Okumura (*) : I. Watanabe : T. Nakai :K. Ohkubo :T. Kofune : S. Ashino :M. Kofune :A. HirayamaDivision of Cardiology, Department of Medicine,Nihon University School of Medicine,Ohyaguchi-kami machi, Itabashi-ku,Tokyo 173-8610, Japane-mail: [email protected]
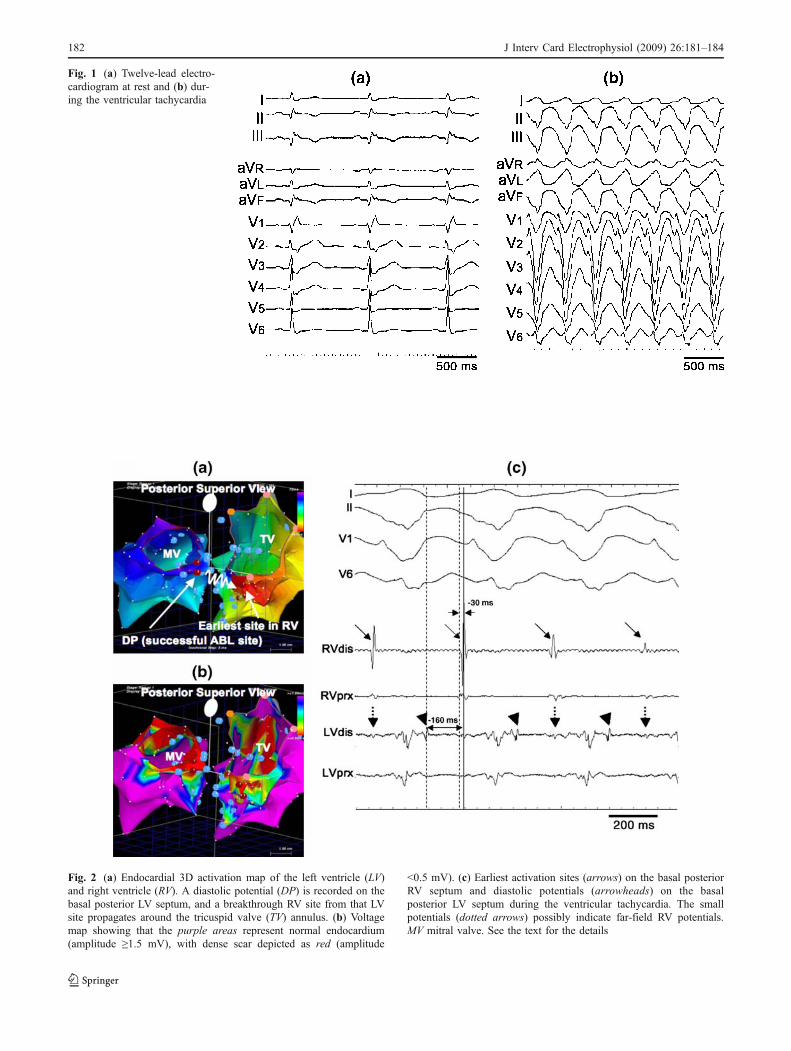
Fig. 1 (a) Twelve-lead electro-cardiogram at rest and (b) dur-ing the ventricular tachycardia
Fig. 2 (a) Endocardial 3D activation map of the left ventricle (LV)and right ventricle (RV). A diastolic potential (DP) is recorded on thebasal posterior LV septum, and a breakthrough RV site from that LVsite propagates around the tricuspid valve (TV) annulus. (b) Voltagemap showing that the purple areas represent normal endocardium(amplitude ≥1.5 mV), with dense scar depicted as red (amplitude
<0.5 mV). (c) Earliest activation sites (arrows) on the basal posteriorRV septum and diastolic potentials (arrowheads) on the basalposterior LV septum during the ventricular tachycardia. The smallpotentials (dotted arrows) possibly indicate far-field RV potentials.MV mitral valve. See the text for the details
182 J Interv Card Electrophysiol (2009) 26:181–184

also consistent with the earliest bipolar signal-to-QRSinterval during the VT. Several applications of radiofre-quency energy (50 W, 60°C, 60 s) at that site could notterminate the VT, and there was no change in VT cyclelength or morphology. Three-dimensional endocardialelectroanatomic LV mapping was then performed via aretrograde transaortic approach. A spiky diastolic potentialpreceded the QRS onset by 160 ms at the basal posteriorLV septum [Fig. 2(a, c)], opposite the site of the earliest RVactivation [Fig. 2(a)]. This was located at the dense scar(red) on the 3D voltage map [Fig. 2(b)]. Pacing at that siteat a cycle length of 360 ms entrained the VTwith concealedfusion and the stimulus-to-QRS interval was 160 ms, whichwas identical to the diastolic potential-to-QRS intervalduring the VT. The postpacing interval of 390 ms approx-imated the VT cycle length [Fig. 3(b)]. Ablation at that siteterminated the VT within 14 s and rendered it no longerinducible with double/triple RV extrastimuli. He has beenfree from any symptoms for 12 months.
2 Discussion
Sarcoidosis is a systemic granulomatous disease thatinvolves practically every organ of the body [1–3].Myocardial involvement has been shown in up to 10% ofpatients with systemic sarcoidosis [1, 2]. Clinical manifes-tation of cardiac sarcoidosis is dependent on the locationand extent of the granulomas and subsequent scarring [4–6]. Involvement of the basilar septum causes bundle branchblock or AV block. Multiple or localized cardiac involve-ment can be an arrhythmogenic substrate for VT, of whichthe mechanism is reentry [4–6]. The majority of patientswith sarcoid-related VT have been reported to havemultiple morphologies of inducible VT, and the origin
includes the RV and LV endocardium or epicardium [4–6].In two recent reports, the RV was predominantly involved,and the VT reentrant origin was commonly located at thetricuspid annulus, RV free wall, or septum [5, 6].Fortunately, our case had an inducible monomorphic VTdemonstrating a LBBB pattern. The VT morphology andperfect pace map from the earliest RV bipolar signal at thebasal septum suggested an exit from the RV septum, aspreviously reported [5, 6]. Nonetheless, the ablation at thatRV site did not terminate the VT. Eventually, the VT wassuccessfully cured by a point ablation at the basal posteriorLV septal region. These findings could be explained by amechanism involving an exit deep in the septum, andablation on both sides of the septum was needed toeliminate the VT. Nevertheless, the ablation on the RV sidedid not cause any change in the cycle length or morphologyof the VT. In addition, pacing from the site recording adiastolic potential on the LV side demonstrated entrainmentwith concealed fusion. This would rather support amechanism involving the LV side of the interventricularseptum serving as a critical isthmus of the reentrant circuit,and the earliest RV activation site was a breakout regionfrom the left-sided circuit. To the best of the authors'knowledge, this is the first report to clearly describe areentrant mechanism of LBBB-type VT originating fromthe left ventricular septum with an exit site on the RVseptum associated with cardiac sarcoidosis.
References
1. Chapelon-Abric, C., de Zuttere, D., Duhaut, P., Veyssier, P.,Wechsler, B., Huong, D. L., et al. (2004). Cardiac sarcoidosis: Aretrospective study of 41cases. Medicine, 83, 315–334.
Fig. 3 (a) Pacing at the earliestactivation right ventricular (RV)site perfectly (left panel)matches the ventricular tachy-cardia morphology (right panel).(b) Concealed entrainment pac-ing at the left ventricular (LV)site recording a diastolic poten-tial. PCL pacing cycle length,PPI postpacing interval, VCLVT cycle length. See the text forthe details
J Interv Card Electrophysiol (2009) 26:181–184 183

2. Silverman, K. J., Hutchins, G. M., & Bulkley, B. H. (1978).Cardiac sarcoid: A clinicopathologic study of 84 unselectedpatients with systemic sarcoidosis. Circulation, 58, 1204–1211.
3. Roberts, W. C., McAllister, H. A., Jr., & Ferrans, V. J. (1977).Sarcoidosis of the heart. A clinicopathologic study of 35 necropsypatients (group 1) and review of 78 previously described necropsypatients (group 11). The American Journal of Medicine, 63, 86–108.
4. Winters, S. L., Cohen, M., Greenberg, S., Stein, B., Curwin, J., Pe,E., et al. (1991). Sustained ventricular tachycardia associated withsarcoidosis: Assessment of the underlying cardiac anatomy and the
prospective utility of programmed ventricular stimulation, drugtherapy and an implantable antitachycardia device. Journal of theAmerican College of Cardiology, 18, 937–943.
5. Koplan, B. A., Soejima, K., Baughman, K., Epstein, L. M., &Stevenson, W. G. (2006). Refractory ventricular tachycardiasecondary to cardiac sarcoid: Electrophysiologic characteristics,mapping, and ablation. Heart Rhythm, 3, 924–929.
6. Jefic, D., Joel, B., Good, E., Morady, F., Rosman, H., Knight, B., etal. (2009). Role of radiofrequency catheter ablation of ventriculartachycardia in cardiac sarcoidosis: Report from a multicenterregistry. Heart Rhythm, 6, 189–195.
184 J Interv Card Electrophysiol (2009) 26:181–184