lesson description – mitch taylor - acls 4...
TRANSCRIPT

Lesson Description –Mitch Taylor
• Respiratory Failure/
Mechanical Ventilation
• The lesson will enable the student to describe the manifestations of respiratory failure and Adult or Acute Respiratory Distress Syndrome (ARDS).
• The student will be able to describe the assessment, nursing diagnosis, and interventions for the treatment of respiratory failure and ARDS.
• This includes discussion of management of patients receiving mechanical ventilation.


Ventilation is the structural movement of air in and out of the lungs – O2 in
and CO2 out from the lungs.
A. Compliance involves the expansion and recoil of the lungs.• Volume – residual volume is what is left after a full
exhalation.
• Pressure – Diffusion of O2 from the Alveoli (inhaled air) to the blood stream and cells and diffusion of CO2 from the blood to the Alveoli (for exhalation). • Stiffness - low compliance
• Elastic - high compliance, but may have less recoil
B. Surface Tension – surfactant production in the Alveoli produces a liquid that acts as a lubricant
C. Muscular Effort – Contraction of the diaphragm and intercostal muscles move the rib cage and allow for expansion of the lungs.

Respiratory Anatomy and Physiology
Dead Space – that
part of ventilation that
does not take part in
gas exchange
Perfusion – circulatory
side of oxygen exchange
– carries high amounts of
CO2 to be given to the alveoli

RESPIRATORY SYSTEMOxygenated blood
to the left side of the heart
from the pulmonary veins
Deoxygenated blood
from the right side of the heartfrom the pulmonary arteries
Alveoli -site of gas exchange
Bronchioles
The pulmonary arteriesturn into the pulmonarycapillaries and then turninto pulmonary veins to goback to the left side of theheart with oxygenated blood.
It is at the capillary level is wherethe sacs of the alveoli exchangewith the blood stream.

The Oxyhemoglobin Dissociation Curve –what this tells us is the higher the arterial oxygen on the bottom (horizontal axis) the higher the attachment to the red blood cell showing up in higher O2 sats (vertical axis). With changes in pH that connection is disrupted.
We can turn up the oxygen a great deal, but if the pH is not corrected, then our O2 sats will not improve.
The hemoglobin cannot carry as much oxygen to the tissues if the pH is not corrected.

What is Acute Respiratory Failure?
Remember 50/50 rule?
PaO2 < 50 mm Hg and
PaCO2 > 50 mmHg and pH < 7.35 (Some might say pH closer to 7.25 or 7.20)
PaCO2 5 mmHg > than baseline in already elevate PaCO2

What type is it?
• Is it the Ventilation or Perfusion side of things?
• We will focus on the Ventilatory side.
• Is it the O2 or the CO2?
–Hypoxemic Failure – too low O2
–Hypercapnic (Ventilatory) Failure – too high CO2
• What is the normal respiratory drive?

Hypoxemic Resp. Failure
• Pulmonary Edema – fluid in the alveolar sacs in the spaces around the alveoli
• Third spacing, the fluid leaks out of the vessels into the spaces around the alveoli

Sponge
• The lungs take on the extra fluid because the lymphatic vessels cannot remove the fluid quickly enough in certain conditions:
• Heart failure, sepsis, head injuries, and other systemic inflammatory responses.
• This will produce the coarse crackles heard in the bases of the lung fields.

Respiratory Failure
• Brain Stem, specifically the lowest part, the Medulla Oblongata controls the respiratory center
• And centers for cough, gag, swallow, and vomit.

Respiratory Failure
• Causes could be related to the central nervous system (trauma to the head or brain tumor)
• Causes could be related to the lungs such as in restrictive lung diseases (C.O.P.D.) such as bronchitis, emphysema, and asthma.
• Trauma to the chest such as pneumothorax or even pulmonary contusions.

Assessment
• Determine patient’s level of consciousness
– Can the patient maintain his/her own airway?
– Have they been sedated? Can it be reversed?
– Has the patient has a stroke or head injury?
– Can the patient swallow or have a gag reflex?

Assessment
• Determine patient’s airway clearance
–Can patient clear their own secretions?
–Does the patient have rhonchi or gurgles when auscultating lung sounds
–Does the patient have dyspnea?

Assessment
• Determine patient’s ABG results
–Fifty/Fifty rule of hypoxemia and hypercapnia, PaO2 < 50 and PaCO2 > 50
–Persons with a chronic PaCO2 > 50, then check baseline, if > 5mmHg rise on the PaCO2 = acute respiratory failure

Assessment
• Determine if patient has impaired gas exchange–Does the patient have coarse crackles
when auscultating lung sounds
–Does the patient have decreased lung sounds
–Assess patient’s fluid status and weight gain
–Assess patient’s blood pressure
–Assess patient’s anxiety, shortness of air, accessory muscles when breathing

Nursing Diagnosis• Activity Intolerance
• Ineffective Airway Clearance
• Ineffective Breathing Pattern
• Impaired Gas Exchange
• Excess fluid volume to the lungs
• Anxiety

Prioritize
• Ineffective Airway Clearance –secretions or bronchospasms, if pt cannot maintain their airway, this will always be the first priority
• Ineffective Breathing Pattern – seen clinically in respirations and O2 sats and visual inspection of accessory muscles
• Impaired Gas Exchange – seen in ABG values

Nursing Diagnosis cont.
• Excess fluid volume to the lungs –careful with this.
• Fluid volume overload talks about fluid from the perspective of the vascular space and heart.
• A patient could be drowning in their lungs, but have low volume in their vessels.

Nursing Diagnosis cont.
• If that is the case, the pt might have fluid volume deficit, but still have pulmonary edema because they are third spacing their fluid into their lungs.
• The treatment might be fluids, but be mindful of the fluid overload in the lungs. A balancing act may be required for BP and Lungs.

Cont.
• Anxiety – this may be an early indicator of hypoxemia, get an order to check a blood gas at the same time you are reassuring and talking to your patient.
• Activity Intolerance – if pt is requiring frequent rest periods be mindful to check O2 sats before and after activity.

Outcomes
• The patient will have improved activity tolerance back to baseline within 24-48 hours.
• The patient will maintain airway patency within 1-5 minutes.
• The RR will return to 10-20 within 30 minutes of treatment.

Outcomes
• The ABGs will show a resolution of the hypoxemia and respiratory acidosis by either returning to baseline or
• pH 7.35-7.45, PaCO2 < 50, PaO2 > 50, or O2 sats > 90% within 1-30 minutes of treatment.
• The patient will have improved lung sounds, improved urine output, and/or weight loss within 24-48 hours.
• The patient will have less anxiety and show less use of accessory muscles to breathe.

Planning• The plan is to maintain patency
of the airway– Facilitate coughing and deep
breathing
– Reverse sedation as ordered
– Remove secretions with oral and nasal-tracheal suctioning as ordered
• Improve ventilation– Coughing and Deep Breathing
– Incentive Spirometry
– Breathing Treatments if wheezing heard upon auscultation
– Positive pressure breathing

Improve oxygenationas ordered
• Oxygen per Nasal Cannula• Recommended flow rate is 0.5 to 6 Liters. • Precise FiO2 is not determined. Anything > 2
or 3 LPM will need humidification.• FiO2 will vary with respiratory rate, tidal
volume, anatomic reserve, and inspiration. • FiO2 estimation rule: 1 Liter per minute (LPM)
about 4% increase.• Room Air = 21% FiO2 (Fraction of inspired
oxygen)• 1 LPM = 24% FiO2• 2 LPM = 28% FiO2• 3 LPM = 32% FiO2• 4 LPM = 36% FiO2• 5 LPM = 40% FiO2• 6 LPM = 44% FiO2• Oximyzer cannula is a high flow cannula that
can be increased above 6 LPM.

Simple Mask• Recommended minimum flow
rate is greater than 5 LPM• Lower flow rates may cause
rebreathing of the patient’s CO2• Precise FiO2 is not determined
~ 50% FiO2, used for short term use
• A Venturi Mask is similar except there are attachments that regulate the FiO2 to give a specific flow (24, 26, 28, 31, 35, 40, and 50% FiO2). Not seen used much any more.

Non-Rebreathing Mask (NRB-non rebreather)
• This has a mask and a reservoir bag, rubber valves on the 2 exhalation ports and a valve between the mask and bag.
• Removing the rubber valve on the exhalation opening will reduce the FiO2 ~ 80%, both off will reduce to ~ 60% FiO2.
• Provides high FiO2 between 90-100%
• Bag will remain inflated
• Prevents rebreathing of pt’s exhaled CO2
• Flow rate should be at least 10-15 LPM• Does not need humidifier (bubbler)

High Flow O2 Nebulizer• Will provide O2 with heated
or cooled aerosol mist
• Devices:– Aerosol Mask
– Trach. Shield
– T-piece blow by
• Delivers 28-90% FiO2 that can be dialed in
• Flow rate needs to be at least 10-15 LPM.
• Requires Humidification

CPAP/BiPAP• Continuous Positive
Airway Pressure –delivers pressure support to the patient all the time – i.e. 20 cm H20, max on most home CPAPs
• Bilevel Positive Airway Pressure – delivers PS and PEEP – two settings - i.e. 18/5 cm H20
• Pros: Non-invasive, prevent intubation and complications of intubation
• Cons: Breathe against forced air, dry mouth, skin breakdown to bridge of nose, feeling of claustrophobia

Planning• Provide CPAP/BiPAP or mechanical ventilation if
patient’s ventilation does not improve
• Prevent secondary complications if patient is on mechanical ventilation
• Ventilator Associated Pneumonia – VAP– HOB – elevated 30 degrees or greater if condition
tolerates
– Oral care
• Prevent risk of aspiration by placing oral gastric tube into the stomach as ordered
• Prevent gastric complications and DVTs (Deep Vein Thrombosis) by collaboration with provider

Airways
• Oropharyngeal airway – useful when the tongue falls back against the pharynx – May cause gagging in the semi-conscious patient
• Nasopharyngeal airway or Nasal trumpet – this is preferred in conscious patients because it will not gag the patient –contraindicate in basilar skull fractures – many times kept in place for suctioning

Laryngeal Mask Airway (LMA)
• The LMA provides an indirect way to intubate the patient.
• It is an alternative when endotracheal intubation cannot be performed.
• It is contraindicated in the semi-conscious patient due to gagging.
• Because the LMA sits above the vocal chords, the airway is technically not protected.
• The patient is at risk for aspiration.
• It is an indirect form of intubation and ventilation.
http://www.merck.com/media/mmpe/figures/figure1sec6ch64_eps.gif

Esophageal Obturator Airway (EOA)
• Can be placed blindly, meaning the vocal chords do not have to be visualized.
• Place in the esophagus
• Inflate the balloon

Combitube• Combination tube
• EOA/ET tube
• Can be placed blindly, like an OG tube
• If it winds up in the esophagus, ok.
• If it winds up in the trachea, ok.
• Two balloons
– one distal – goes with the blue port – if in trachea – just blow this one up
– One proximal – goes with white port – if in the esophagus, then blow both up
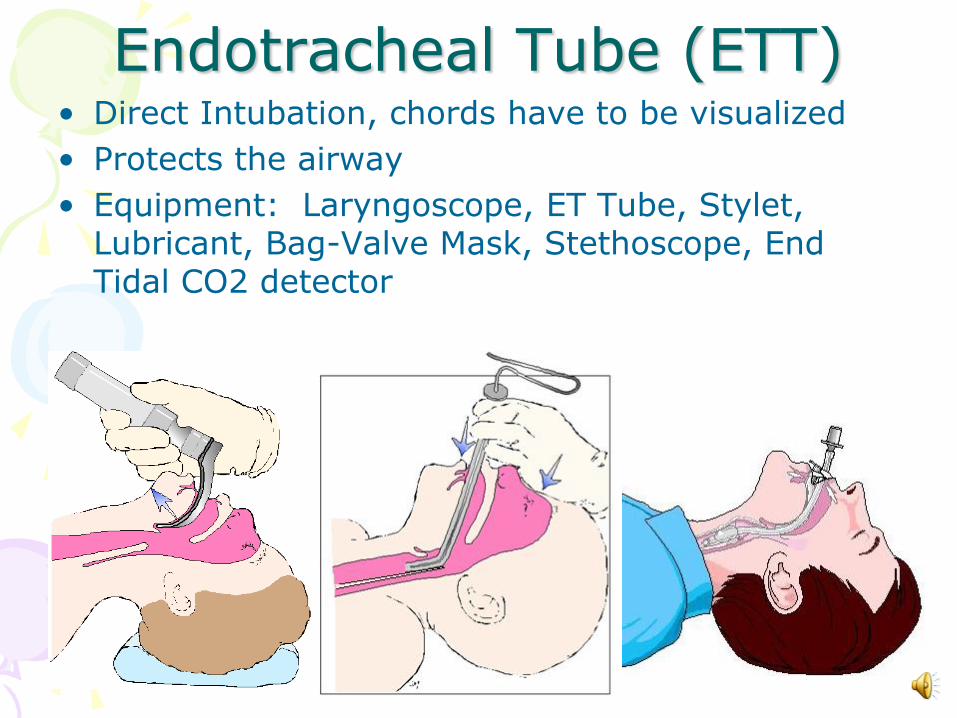
Endotracheal Tube (ETT)• Direct Intubation, chords have to be visualized
• Protects the airway
• Equipment: Laryngoscope, ET Tube, Stylet, Lubricant, Bag-Valve Mask, Stethoscope, End Tidal CO2 detector

After Intubation• Confirm Placement by auscultating lung sounds
right upper airway, left upper airway, right lower airway, left lower airway, and epigastric area
• If you hear over the epigastric area, it is in the stomach. Should be removed and reintubated.
• If you hear on the right side, could be a right main stem bronchial intubation, then the cuff should be deflated and pulled back 1 cm at a time until bil. lung sounds are heard.
• A 2ndary confirmation is done with an End Tidal CO2 detector. It will start out purple – and turn yellow if CO2 is present. We want it to turn yellow. Ventilate with the bag.
• A chest X-ray will need to be ordered.

Mechanical Ventilation
• Like the CPAP/BiPAP, the provides positive pressure ventilations
• Unlike the CPAP/BiPAP, this is invasive

Ventilator Settings• Tidal Volume (VT) – for Volume Controlled Ventilations
– Volume of gas delivered during each ventilator breath– Usually 6-8 mL/kg (older way was 10 mL/kg – still seen at times)
OR• Inspiratory Pressure (IP) – for Pressure Controlled Ventilations
– Maximum amount of pressure the ventilator can use to deliver breath– 10-20 cm H2O above peak inspiratory pressure; maximum is 35 cm H2O------------------------------------------------------------------------------------
• Respiratory Rate (RR)– Number of breaths delivered by the ventilator per minute– Usually 4-20 breaths per minute
• Fractional Inspired Oxygen (FIO2)– Amount of oxygen delivered by ventilator to patient– 21% to 100%; usually set to keep PaO2 > 60 mmHg or SaO2 > 90%
• PEEP (Positive End Expiratory Pressure)– PEEP is positive pressure that is applied by the ventilator at the end of
expiration. – Much like a balloon the hardest part of getting your lungs (alveoli) to open is the
first breath. This allows some pressure to be left in the alveoli so the lung does not have to overcome the resistance with every breath.
– 5-10 cmH20 to as much as 35 cmH20 with conditions such as ARDS– The higher the number, the greater the intrathoracic pressure – may lower BP.
• Pressure Support (PS) – this can be set to overcome the resistance of the ET tube usually set, only used in SIMV mode

Modes of Ventilation
• Two most common types:
• Assist Control (A/C) – not a weaning mode– Delivers either a certain Volume or Pressure with every
breath
– Set at 10, if the patient is breathing 13, then 13 breaths will be given that breath at the IP setting or TV set.
– All deep breaths – could be uncomfortable
• Synchronized Intermittent Mandatory Ventilation (SIMV) – weaning mode– Delivers either Volume or Pressure on the set number of
times the RR is set.
– The rest of the breaths can be at whatever the patient wants to breathe.
– Only deep breaths are set, rest can be smaller or larger

Alarms
• High Pressure Alarms – ie. High Peak airway pressures, think obstructions from tubing kinked to secretions
• Low Pressure Alarms – think disconnections – check cuff/tubings, check Tidal Volumes (if lower than what they are set at, then may be a leak)

ARDS
• Definition – Acute (Adult) Respiratory Distress Syndrome is a progressive form of respiratory failure as seen by severe dyspnea, hypoxemia, and bilateral infiltrates on a chest X-Ray (usually seen as a whitening throughout the lung fields – normally the lung fields would be black)
• Basically an advanced form of third spacing to the lung –pulmonary edema

ARDS - Causes
• Pneumonias – including ventilator associated pneumonia (VAP)
• Lung contusions
• Aspiration
• Smoke inhalation
• Sepsis
• Shock
• Increased ICP

ARDS
• Phase 1 – exudate leaks into the spaces around the alveoli due to the damage – 24 hours
• Phase 2 – alveoli collapse resulting in atelectasis – impairing gas exchange 7-10 days
• Phase 3 – damaged lung tissue is replaced with fibrotic tissue, producing stiff lungs and worsening hypoxemia.

Pharmacologic Therapy
• High levels of Oxygen to maintain sats > 90% or PaO2 > 60mm Hg
• Diuretics – for true fluid overload
• Reversal agents for narcotics and/or sedatives to prevent failure
• Sedatives after failure for intubation and mechanical ventilation
• Paralytics for intubation and/or mechanical ventilation
• Rotation of patient 45 degrees – bed rotation
• Maintain hemodynamic stability if needed with inotropic agents such as dopamine or dobutamine

50/50 Rule
• PaO2 < 50 mm Hg – hypoxemia or
• PaCO2 > 50 mmHg – hypercapnia and pH < 7.35 (Some might say pH closer to 7.25 or 7.20) or
• PaCO2 5 mmHg > than baseline in already elevate PaCO2

Case Study
• Pt. is in the ICU for 3 days post – op heart surgery. Refuses to get up out of bed or use his incentive spirometer or to use his 6L/NC.
• Patient becomes anxious and agitated about his care, RR 38.
• The RN gets an ABG on the patient.
• What would you expect the ABG to show?

ABG
• pH 7.52
• PaCO2 28
• PaO2 48
• HCO3 24
• Patient becomes more agitated until he pulls out the IV and gets up to go to the bathroom alone.
• Patient falls to one knee.
• You assist the patient back to bed.

What is happening?
• Hypoxemia as evidenced by PaO2 < 50 and agitation/confusion
• Respiratory Alkalosis because of hyperventilation
• What should we do?
• Get patient back on oxygen
• Assess pt - Get an O2 sat – reads 86% and check for cyanosis

Begin Collaboration
• Call charge nurse or neighbor for help
• Increase the O2 – 100% non-rebreather
• Notify RT of respiratory distress
• Notify physician of patient’s resp. distress, RR decreases to 8 per min.
• Physician orders another ABG

ABG• pH 7.18
• PaCO2 72
• PaO2 44
• HCO3 24
• Patient becomes unresponsive.
• Call a code-blue
• Begin ventilating the patient w/bag-valve-mask
• Notify Anesthesiologist on call or Respiratory Therapist on call for a stat intubation
• Physician intubates the patient and provides these vent settings: SIMV, TV 800 FiO2 100% RR 18 Peep 5 PS 8, ask for orders for sedation
• Get an ABG in 30 mins and call results