lesson learnt from imi-protect - globe network · lesson learnt from imi-protect benefit-risk...
TRANSCRIPT
Lesson learnt from IMI-PROTECTBenefit-risk assessment of medications,
and adaptation to vaccines
Perspective on Benefit-Risk Decision-Making in Vaccinology Conference24th June 2014Fondation Merieux, Annecy, France
Shahrul Mt-Isa
School of Public Health
Follow us
Disclaimers
“The processes described and conclusions drawn from the work presented herein relate solely to the testing of methodologies and representations for the evaluation of benefit and risk of medicines.
This report neither replaces nor is intended to replace or comment on any regulatory decisions made by national regulatory agencies, nor the European Medicines Agency.”
2
PROTECT is receiving funding from the European Community’s Seventh Framework Programme
(F7/2007-2013) for the Innovative Medicine Initiative (www.imi.europa.eu)

3
IMI-PROTECT Work Package 5Benefit-risk integration and representation

The licensing challenge in medical decision-making
• The task of regulators (e.g. EMA, FDA) is to make a good and defensible decision on which medicines should receive a license for which indications, based on the available evidence of risks and benefits.
• It is increasingly important to be able to justify and explain these decisions to patients and other stakeholders.
• Whose value preferences take priority?
• Can more formal approaches of decision-making, and especially more modern methods of graphical display help regulators do these better?
• Which quantitative approach(es) to use?
4
Methodologies available
5
Non –quantitative
All B-R assessment approaches
Benefit-risk assessment framework
Metric indices for B-R assessment
NNTNNH
AE-NNTRV-NNH
Impact numbersMCE
RV-MCEMARNEAR
Estimation techniques
QALYDALYHALE
Q-TWiST
UT-NNTINHBBRRGBR
Principle of 3TURBO
Beckmann
BLRANCB
Decision treeMDP
MCDASMAASBRAM
CUIDI
Trade-off indices
PROACT-URLASF
BRATFDA BRF
CMR-CASSCOBRASABRE
UMBRAOMERACT 3x3
Descriptive framework
Quantitative framework
Threshold indices Health indices
SPMCVCA
DCE
DAGsPSMCPMITC
MTCCDS
Approaches excluded and not appraised
Utility survey techniques
Mt-Isa et al. Balancing benefit and risk of medicines: a systematic review andclassification of available methodologies. Pharmacoepidemiology and Drug Safety 2014. DOI: 10.1002/pds.3636.

Recommendation Roadmap
6
Planning
Evidence gathering and data preparation Analysis
Exploration
Conclusion and dissemination
• critical issues
• think & discuss purpose and context
• documentation
• foundations for future analyses and updates
• relevant evidence
• data collection
• data aggregation
• missing/incomplete data
• Evaluate data
• Quantify benefits and risks
• Weigh or integrate
• robustness
• sensitivity
• assumptions and uncertainties
• other consequences
• impact or added value to the RMPs
• communicate results/consensus
• any influence on future actions
• transparent audit trail
• ensures "big picture" is not lost
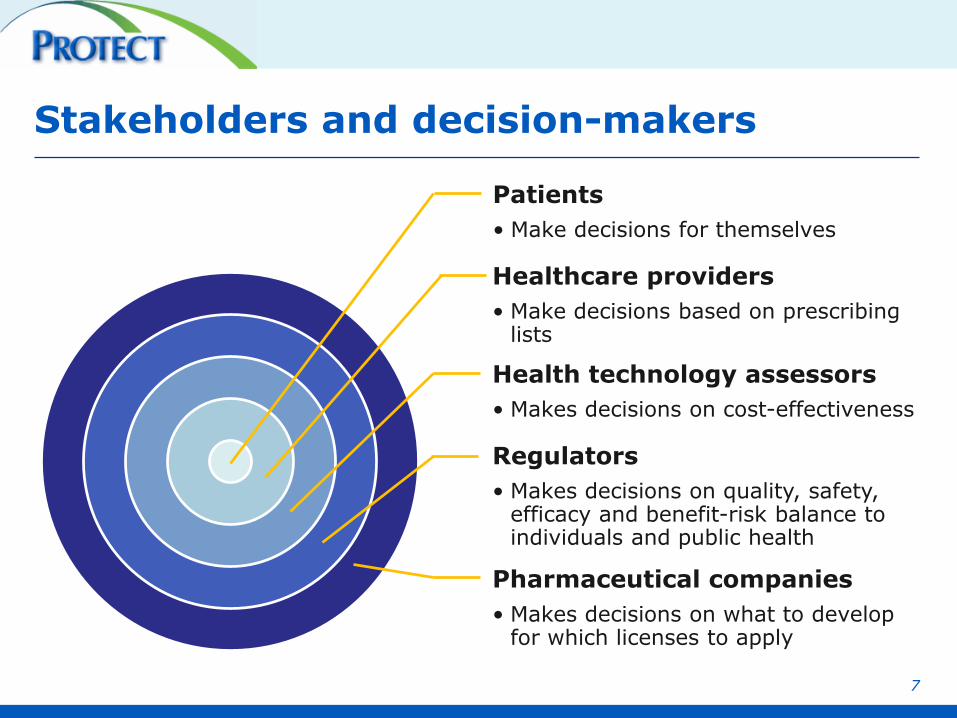
Stakeholders and decision-makers
Patients
• Make decisions for themselves
Healthcare providers
• Make decisions based on prescribing lists
Health technology assessors
• Makes decisions on cost-effectiveness
Regulators
• Makes decisions on quality, safety, efficacy and benefit-risk balance to individuals and public health
Pharmaceutical companies
• Makes decisions on what to develop for which licenses to apply
7

Perspectives
• Individual vs public health
• Stakeholders:
– who the decision maker is (the first party),
– who the decision is to be made for (the first or the second party), and
– any other stakeholders involved (the third party) in the decision making.
• Highlight relevant benefits and risks
• Affects different population differently
8
Rimonabant case study
Drug of interest Rimonabant
Indication Weight loss in obese and overweight patients with co-morbidities in adults (>18y)
Severe side effect
Increased risk of psychiatric disorders
Regulatoryhistory
2006 Approved in June2009 Voluntary withdrawal in January bythe MAH
Comparators Placebo, orlistat, sibutramine9
It is an interesting case study because: Despite some benefits in
patients, risk of psychiatric disorders emerged post-marketing, resulting
first in label changes and then voluntary withdrawal in the EU.
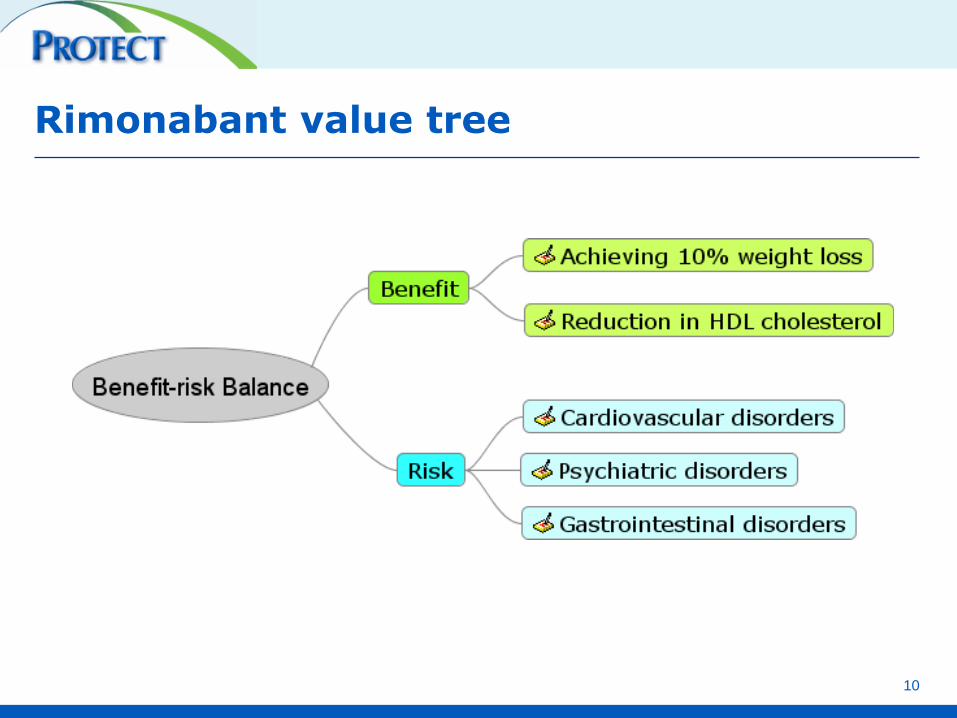
Rimonabant value tree
10

Median [Range] absolute valuesIndirect treatment comparison
Criteria Placebo Orlistat Sibutramine Rimonabant
Achieving 10% Weight loss (proportion)
0.11 [0.10,0.14] 0.24 [0.15,0.34] 0.47 [0.16,0.80] 0.40 [0.22,0.62]
Reduction in HDL Cholesterol (mg/dL)
1.02 [0.95,1.10] 1.92 [1.12,2.75] 2.63 [1.19,4.11] 2.12 [0.26,3.93]
Cardiovascular disorders (proportion)
0.02 [0.01,0.02] 0.11 [0.00,1.00] 0.04 [0.00,1.00] 0.03 [0.00,0.99]
Psychiatric disorders (proportion)
0.01 [0.01,0.01] 0.00 [0.00,0.03] 0.02 [0.00,0.11] 0.02 [0.00,0.06]
Gastrointestinal disorders(proportion)
0.05 [0.05,0.06] 0.19 [0.06,0.50] 0.09 [0.02,0.35] 0.07 [0.04,0.15]
11

• AKA Impact Numbers
• England and Wales 2006 >20y
• Assumptions: target popn similar to placebo arm, ~62% overweight+, ~70% eligible Rx, target 10% coverage
Attributable Population assessment Performance assessment Impact estimation
Population Impact Measures (PIM)
Median (95% CI) Achieved a 10% weight loss in one year Any psychiatric disorders
PAR 0.54 (0.47, 0.60) 0.55 (-0.06, 0.87)
PIN-ER-t 1338016 (1052444, 1663270) 27190 (-2633, 98730)
EIN 6 (5, 9) 253 (-1911, 8.5e+8)
NEPP (target 10%) 291781 (207657, 402174) 6140 (-247, 53674)
12Verma et al. Population Impact Analysis: a framework for assessing the population impact of a risk or intervention. J Public Health (Oxf). 2012 Mar; 34(1):83-9. doi: 10.1093/pubmed/fdr026.
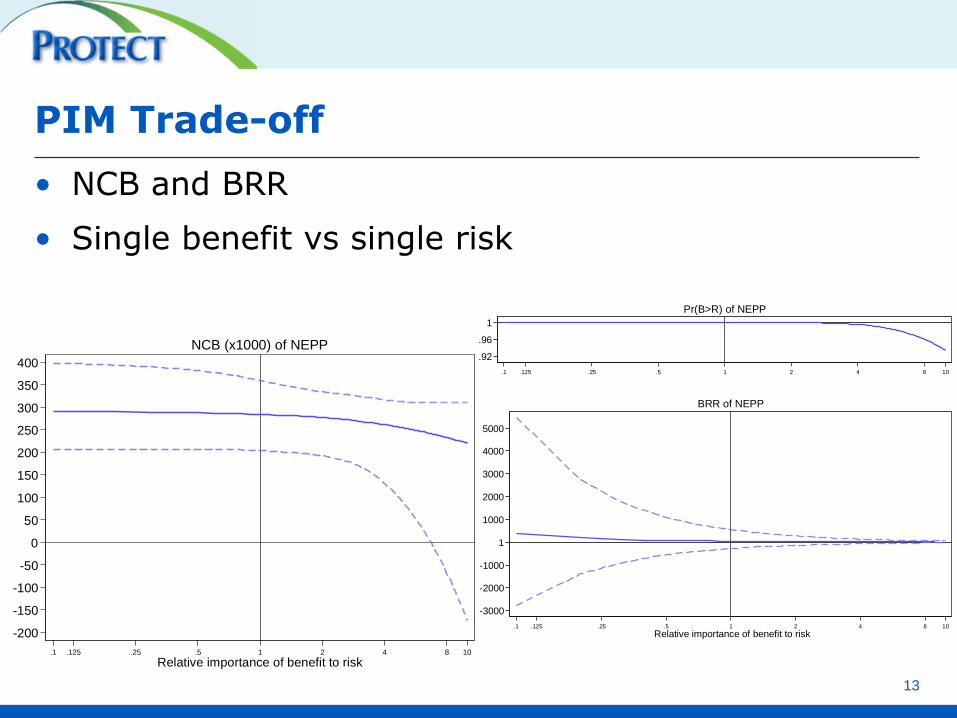
PIM Trade-off
13
• NCB and BRR
• Single benefit vs single risk
-200
-150
-100
-50
0
50
100
150
200
250
300
350
400
.1 .125 .25 .5 1 2 4 8 10
Relative importance of benefit to risk
NCB (x1000) of NEPP.92
.96
1
.1 .125 .25 .5 1 2 4 8 10
Pr(B>R) of NEPP
-3000
-2000
-1000
1
1000
2000
3000
4000
5000
.1 .125 .25 .5 1 2 4 8 10
Relative importance of benefit to risk
BRR of NEPP
Multi-criteria methodology requirements
• Most multiple criteria methods for benefit-risk assessment require:
– Favourable (benefit) and unfavourable (risk) effects data
From clinical trials, post-marketing surveillance, epidemiological studies
– Preference data (weights, value functions)
14
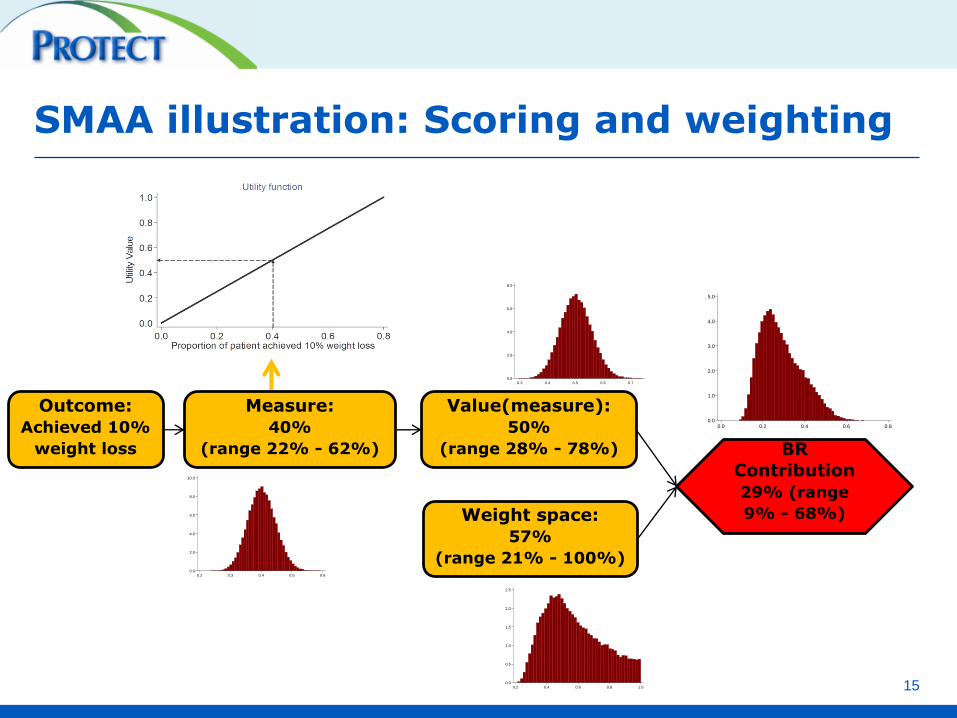
SMAA illustration: Scoring and weighting
15
Outcome:
Achieved 10%
weight loss
Measure:
40%
(range 22% - 62%)
Value(measure):
50%
(range 28% - 78%)
0.0
2.0
4.0
6.0
8.0
10.0
Den
sity
0.2 0.3 0.4 0.5 0.6
0.0
2.0
4.0
6.0
8.0
Den
sity
0.3 0.4 0.5 0.6 0.7
Weight space:
57%
(range 21% - 100%)
0.0
0.5
1.0
1.5
2.0
2.5
Den
sity
0.2 0.4 0.6 0.8 1.0
0.0
1.0
2.0
3.0
4.0
5.0
Den
sity
0.0 0.2 0.4 0.6 0.8
BR
Contribution
29% (range
9% - 68%)
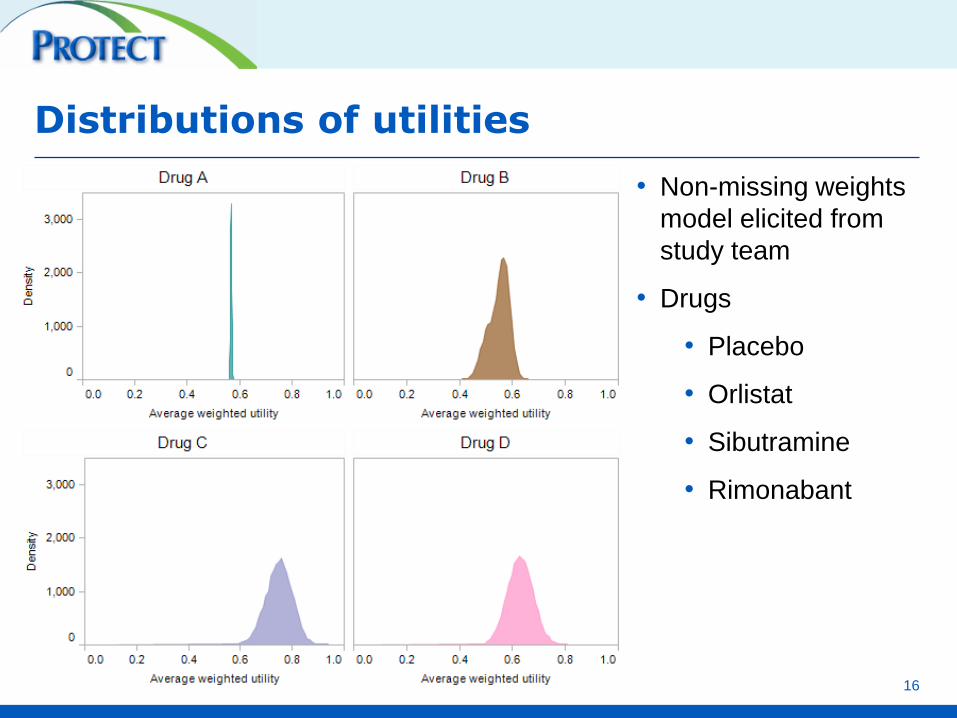
Distributions of utilities
16
• Non-missing weights
model elicited from
study team
• Drugs
• Placebo
• Orlistat
• Sibutramine
• Rimonabant
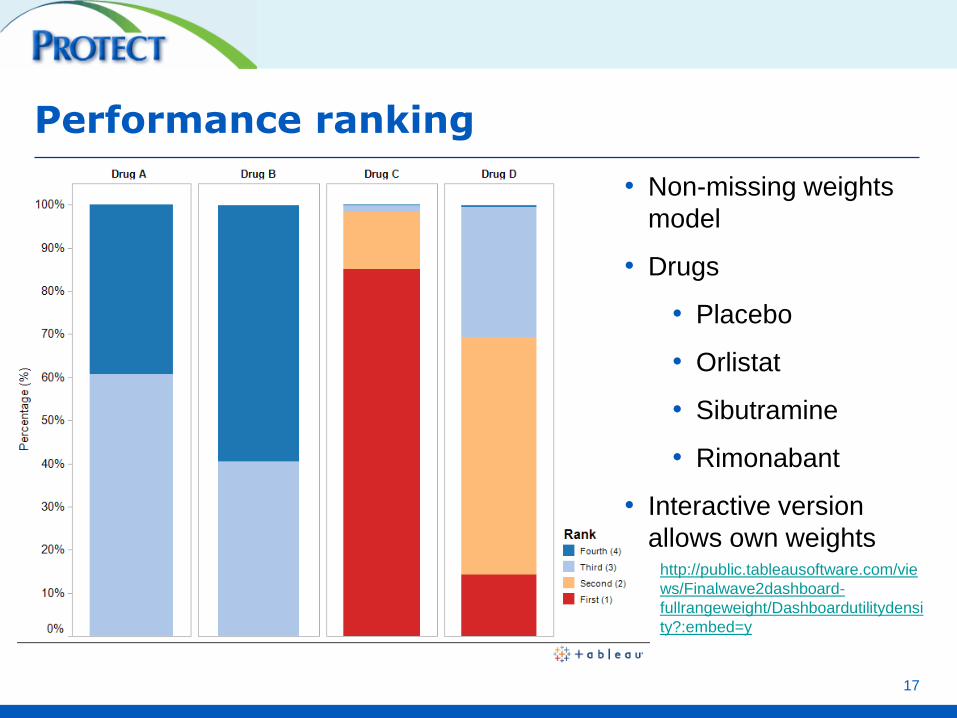
Performance ranking
17
• Non-missing weights
model
• Drugs
• Placebo
• Orlistat
• Sibutramine
• Rimonabant
• Interactive version
allows own weightshttp://public.tableausoftware.com/vie
ws/Finalwave2dashboard-
fullrangeweight/Dashboardutilitydensi
ty?:embed=y

Direct preference elicitation
• Simple
• Unstructured
• May result in inconsistency
• Lack transparency
18
Structured elicitation methods
available – not covered
Remarks
• Formally structured benefit-risk assessment can aid with transparency and communication of benefits and risks
• These methodologies do not make decisions themselves. They support decision-making and are not intended to replace medical expertise.
• Stakeholders such as patients and public involvement may add value and would lead to more clinically relevant decisions.
19
Final thoughts…
1. Estimate PIMS
2. Use within multi-criteria analysis method e.g. MCDA or SMAA
20
RESOURCES
21
Follow us

Acknowledgements
• The research leading to these results was conducted as part of the PROTECT consortium (Pharmacoepidemiological Research on Outcomes of Therapeutics by a European ConsorTium, www.imi-protect.eu) which is a public-private partnership coordinated by the European Medicines Agency.
• The PROTECT project has received support from the Innovative Medicine Initiative Joint Undertaking (www.imi.europa.eu) under Grant Agreement n° 115004, resources of which are composed of financial contribution from the European Union's Seventh Framework Programme (FP7/2007-2013) and EFPIA companies’ in kind contribution.
22

Work Package 5 of IMI-PROTECT
23
Public Private
Imperial College (co-leader) Merck KGaA (co-leader)
EMA AMGEN
DHMA AstraZeneca
MHRA Bayer
Mario Negri Institute GSK (deputy co-leader)
GPRD Lilly
La-SER Novartis
IAPO Novo Nordisk
Pfizer
Roche
Sanofi-Aventis
Takeda

24
Click or scan me!
http://www.imi-protect.eu/results.shtml#