lethal osteosclerotic skeletal dysplasia with intracellular inclusion bodies
TRANSCRIPT

Lethal Osteosclerotic Skeletal Dysplasia WithIntracellular Inclusion Bodies
Steven G. Brodie,1 Ralph S. Lachman,1,2 Margaret M. McGovern,3 Pertchoui B. Mekikian,1 andWilliam R. Wilcox1,4*1Ahmanson Department of Pediatrics, Steven Spielberg Pediatrics Research Center, Cedars-Sinai Burns and AllenResearch Institute, Los Angeles, California
2Department of Radiology, UCLA School of Medicine, Los Angeles, California3Division of Genetics, State University of New York, Stony Brook, New York4Department of Pediatrics, UCLA School of Medicine, Los Angeles, California
We report an apparently previously unde-scribed form of lethal osteosclerotic skeletaldysplasia in a 30-week male fetus with mi-cromelic shortness of the limbs. Radio-graphic findings at necropsy included in-creased density in all bones, most marked inthe skull, mandible, and pubis. The ribswere very short, abnormally modeled, andwide anteriorly. The vertebrae were poste-riorly hypoplastic and wedged, particularlyin the cervical and lumbar regions. Thefemora and tibiae were short with wide dis-tal metaphyses, undermodeled diaphyses,and coxa vara. The humeri, radii, and ulnaewere also short and undermodeled withproximal and distal flare. Chondro-osseousmorphology showed short chondrocyte col-umns, extension of hypertrophic cells intothe metaphysis, and overgrowth of peri-chondral bone. In the resting cartilage therewere large chondrocytes containing a ho-mogeneous material staining pink with vonKossa trichrome, gray with toluidine blue,and black with silver methenamine. Thecortical bone was lacking and the trabecu-lar bone was hypercellular, thick, andcoarse. Ultrastructurally, the resting zonechondrocytes were large and round withcondensed chromatin and dilated loops ofrough endoplasmic reticulum. The radio-graphic and histopathologic findings in thiscase are unique and differ from those seenin other reported lethal osteosclerotic skel-
etal dysplasias. Am. J. Med. Genet. 83:372–377, 1999. © 1999 Wiley-Liss, Inc.
KEY WORDS: osteosclerosis; inclusion bod-ies; lethal skeletal dysplasia
INTRODUCTION
Increased bone density is an important finding inseveral skeletal dysplasias including forms of osteope-trosis, hyperostosis, and osteosclerosis. These disor-ders are thought to be caused by abnormal modelingand/or remodeling of the bone [Whyte, 1997]. Radio-graphically, osteopetrosis has a generalized increase inbone density with bony encroachment into the medul-lary cavities. Increased thickness of the cortex istermed hyperostosis, while increased width of trabecu-lar bone is called osteosclerosis. The lethal osteoscle-rotic chondrodysplasias are a heterogeneous group ofdisorders that present in the perinatal period with in-creased density of trabecular bone and dwarfism[Spranger and Maroteaux, 1990; Taybi and Lachman,1996]. The biochemical defects in one form of osteope-trosis, pycnodysostosis, and Blomstrand dysplasiahave been identified but the defects in other disorderswith bone overmineralization have yet to be deter-mined [Sly and Hu, 1995; Gelb et al., 1996; Hart et al.,1997; Johnson et al., 1997; Van Hul et al., 1997, 1998;Whyte, 1997; Jobert et al., 1998].
We report on the clinical, radiographic, and morpho-logic findings in a previously undescribed form of lethalosteosclerotic skeletal dysplasia.
CLINICAL REPORT
The propositus [Registry no. 93-67] was a 30-week-gestation female fetus with micromelia. The family his-tories of both the Italian–Puerto Rican 23-year-old G1mother and a 27-year-old nonconsanguineous Italian-Polish father were unremarkable. Physical examina-tion also showed microcrania, midface hypoplasia, anda prognathic mandible (Fig. 1).
Contract grant sponsor: National Institutes of Health; Contractgrant number: HD 22657.
*Correspondence to: William R. Wilcox, M.D., Ph.D., MedicalGenetics, Cedars-Sinai Medical Center, 8700 Beverly Blvd., SSB-3, Los Angeles, CA 90048. E-mail: [email protected]
Received 25 June 1998; Accepted 12 October 1998
American Journal of Medical Genetics 83:372–377 (1999)
© 1999 Wiley-Liss, Inc.

METHODS
Formalin-fixed chondro-osseous tissue was pro-cessed undecalcified in glycol and methyl methacry-late. Sections were stained with von Kossa trichrome,toluidine blue, alcian blue, silver methenamine, andGoldner’s reagent. For electron microscopy and immu-nohistochemistry, cartilage from the resting zone wasexamined as described previously [Chitayat et al.,1993; Brodie et al., 1998].
RADIOGRAPHIC FINDINGS
Postmortem radiographs (Fig. 2) showed increaseddensity in all bones. There was increased density of thebase and supraorbital regions of the skull with less inthe convexity of the skull. The mandible was dense,proximally widened, and the mandibular angle was ab-sent. There was calcification of the hyoid and cricoidcartilages. The ribs were very short, abnormally mod-eled, and widened anteriorly. The vertebrae were hy-poplastic posteriorly and wedged, especially in the cer-vical and lumbar regions. There was no coronal or sag-ittal clefting. The iliac wings were dense and flaredwith irregularity of the iliac crest, the greater sciaticnotches were very narrow, and the acetabular roofs
were flattened. The ischia were dense and verticallywidened. The pubic bones were dense but normallyformed. The femora were short with widened diaphysesand metaphyses, and coxa vara. The tibiae had a simi-lar configuration to the femora. The fibulae were nor-mally formed but short with distal overgrowth. Thehumeri, radii, and ulnae were dense and markedlyshort with proximal and distal flaring. The hands werenot well seen radiographically.
CHONDRO-OSSEOUS MORPHOLOGY
Histological studies were performed on chondro-osseous specimens from the costochondral junction andfemur. In the resting cartilage, the chondrocytes werelarge and round. They contained a homogeneouslystaining material staining pink with von Kossa tri-chrome, gray with toluidine blue, and positive with sil-ver methenamine. The chondrocyte columns wereshort, hypertrophic cells extended into the metaphysis,and there was overgrowth of perichondral bone with anincrease in calcifying cartilage. The growth plate wasnarrow and irregular, and there was marked mesen-chymal ingrowth from the perichondrium/periostium(Fig. 3). The marrow spaces were fibrotic and the cal-cospherites were not coalescing. There was a lack of
Fig. 1. Supine (A) and lateral (B) photographs of the proband. Note the micromelia, midface hypoplasia, and small chest.
Lethal Osteosclerotic Skeletal Dysplasia 373

Fig. 2. Postmortem anteroposterior (A,B) and lateral (C,D) radiographs showing disproportionate shortness of the limbs. Note the generalizedincreased density especially of the cranial bones, spine, and pelvis.
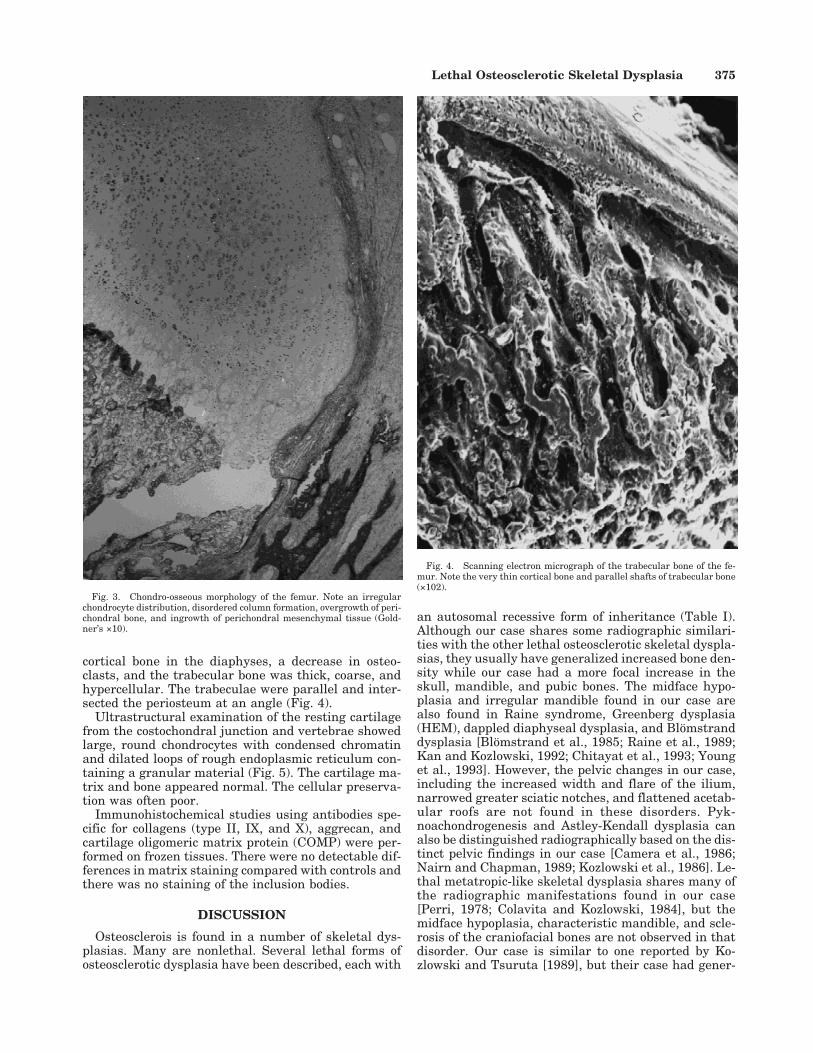
cortical bone in the diaphyses, a decrease in osteo-clasts, and the trabecular bone was thick, coarse, andhypercellular. The trabeculae were parallel and inter-sected the periosteum at an angle (Fig. 4).
Ultrastructural examination of the resting cartilagefrom the costochondral junction and vertebrae showedlarge, round chondrocytes with condensed chromatinand dilated loops of rough endoplasmic reticulum con-taining a granular material (Fig. 5). The cartilage ma-trix and bone appeared normal. The cellular preserva-tion was often poor.
Immunohistochemical studies using antibodies spe-cific for collagens (type II, IX, and X), aggrecan, andcartilage oligomeric matrix protein (COMP) were per-formed on frozen tissues. There were no detectable dif-ferences in matrix staining compared with controls andthere was no staining of the inclusion bodies.
DISCUSSION
Osteosclerois is found in a number of skeletal dys-plasias. Many are nonlethal. Several lethal forms ofosteosclerotic dysplasia have been described, each with
an autosomal recessive form of inheritance (Table I).Although our case shares some radiographic similari-ties with the other lethal osteosclerotic skeletal dyspla-sias, they usually have generalized increased bone den-sity while our case had a more focal increase in theskull, mandible, and pubic bones. The midface hypo-plasia and irregular mandible found in our case arealso found in Raine syndrome, Greenberg dysplasia(HEM), dappled diaphyseal dysplasia, and Blomstranddysplasia [Blomstrand et al., 1985; Raine et al., 1989;Kan and Kozlowski, 1992; Chitayat et al., 1993; Younget al., 1993]. However, the pelvic changes in our case,including the increased width and flare of the ilium,narrowed greater sciatic notches, and flattened acetab-ular roofs are not found in these disorders. Pyk-noachondrogenesis and Astley-Kendall dysplasia canalso be distinguished radiographically based on the dis-tinct pelvic findings in our case [Camera et al., 1986;Nairn and Chapman, 1989; Kozlowski et al., 1986]. Le-thal metatropic-like skeletal dysplasia shares many ofthe radiographic manifestations found in our case[Perri, 1978; Colavita and Kozlowski, 1984], but themidface hypoplasia, characteristic mandible, and scle-rosis of the craniofacial bones are not observed in thatdisorder. Our case is similar to one reported by Ko-zlowski and Tsuruta [1989], but their case had gener-
Fig. 3. Chondro-osseous morphology of the femur. Note an irregularchondrocyte distribution, disordered column formation, overgrowth of peri-chondral bone, and ingrowth of perichondral mesenchymal tissue (Gold-ner’s ×10).
Fig. 4. Scanning electron micrograph of the trabecular bone of the fe-mur. Note the very thin cortical bone and parallel shafts of trabecular bone(×102).
Lethal Osteosclerotic Skeletal Dysplasia 375

alized osteosclerosis with thickened cortical bone andcoronal clefts of the vertebrae. Muller et al. [1992] re-ported a case with osteosclerosis of the skull, facialbones, and spine, but poor ossification of the limbs andthin ribs. The case reported by Al Gazali et al. [1996]had generalized osteosclerosis but wormian bones inthe skull and absent ossification of the pubic rami.Seller et al. [1996] reported a fetus with mixed bonedensity consisting of metphyseal sclerosis and lysis ofthe diaphyses, similar to that seen in Pacman dyspla-sia [Wilcox et al., 1998].
The chondro-osseous morphology of our case is un-usual. There were hypertrophic cells extending into themetaphysis, overgrowth of perichondral bone, abnor-mal cytoplasmic staining of chondrocytes, and a lack ofcortical bone. Extention of hypertrophic cells into themetaphysis are also found in spondylometaphysealdysplasia Sedaghatian and hypophosphatasia, but theother histologic changes of this case are distinct andthere is no osteosclerosis in those disorders [Sedagha-tian, 1980; Peeden et al., 1992]. The bony overgrowthin this case is nonspecific and frequently seen in lethalskeletal dysplasias such as thanatophoric dysplasia,short-rib polydactyly I/III, and platyspondylic lethalskeletal dysplasias, but the columns are shorter inthese disorders [Horton et al., 1979; Martınez-Frıas et
TA
BL
EI.
Su
mm
ary
ofF
indi
ngs
inL
eth
alO
steo
scle
roti
cS
kele
tal
Dys
plas
ias
Pre
sen
tca
seR
ain
esy
ndr
ome
Let
hal
met
atro
pic-
like
dysp
lasi
aP
ykn
oach
on-
drog
enes
isG
reen
berg
dysp
lasi
a
Dap
pled
diap
hys
eal
dysp
lasi
a
Ast
ley-
Ken
dall
dysp
lasi
aB
löm
stra
nd
dysp
lasi
a
Koz
low
ski
and
Tsu
ruta
,[1
989]
Mü
ller
etal
.,[1
992]
Al
Gaz
ali
etal
.,[1
996]
Sel
ler
etal
.,[1
996]
Cli
nic
alF
indi
ngs
Mid
face
hyp
opla
sia
++
−−
++
−+
++
+−
Hyp
opla
stic
man
dibl
ean
d/or
max
illa
++
−−
++
−+
++
−−
Sm
all
ches
t+
++
++
++
++
++
+L
imb
shor
tnes
s+
−+
++
++
++
++
+R
adio
grap
hic
fin
din
gsO
steo
scle
rosi
sS
kull
base
/man
dibl
e+
−−
−−
−−
−?
++
−P
elvi
s+
−+
−−
−−
−+
−+
+L
imbs
+−
++
++
++
+−
++
Hyp
opla
stic
vert
ebra
e+
−+
−+
++
++
−+
+S
hor
tri
bsw
ith
wid
een
ds+
−+
+−
−−
+−
−−
−F
latt
ened
acet
abu
lar
roof
s+
−+
−−
−−
−+
++
+M
orph
olog
yA
ccu
mu
lati
onof
mu
coid
mat
eria
lin
chon
droc
ytes
++
−?
−−
−−
?−
??
Dis
orga
niz
edgr
owth
plat
e+
−+
?+
++
+?
+?
?H
yper
trop
hic
cell
sex
ten
din
tom
etap
hys
is+
−−
?−
−−
−?
+?
?
Per
ich
ondr
albo
ne
over
grow
th+
−−
?−
−−
−?
−?
?D
ilat
edrE
R+
−−
?+
?−
−?
??
?
Fig. 5. Transmission electron micrograph of vertebral resting cartilage.Note the loops of dilated rough endoplasmic reticulum within the chondro-cyte (×13,500). The nuclear crystals are an artifact of fixation.
376 Brodie et al.

al., 1993; Taybi and Lachman, 1996]. The homoge-neous staining cytoplasmic material within restingzone chondrocytes is distinct from the amophous stain-ing material found within the calcospherites of Rainedysplasia [Raine et al., 1989]. The lack of cortical bonehas not been reported in other cases of lethal osteoscle-rotic skeletal dysplasias.
The presence of rER inclusion bodies within chondro-cytes are found consistently in a number of chondro-dysplasias. The rER inclusion bodies in our case sug-gests it may also be due to a defect in an extracellularmatrix protein or another protein trafficked throughthe rER. Immunohistochemical studies excluded colla-gens (type II, IX, and X), aggrecan, and cartilage oligo-meric matrix protein (COMP). No inclusion bodieswere found in the nonhematopoietic cells of bone,which suggests an underlying defect in chondrocytesmay lead to secondary osteosclerotic findings in bone.
ACKNOWLEDGMENTS
This work was supported by an NIH program projectgrant (HD 22657). We thank Christine Kim and LoydaNolasco for technical assistance, Maryann Priore andRoberta Bonacquisti for administering the Interna-tional Skeletal Dysplasia Registry, and David L.Rimoin for reviewing the manuscript.
REFERENCESAl Gazali LI, Devadas K, Hall CM. 1996. A new lethal neonatal short limb
dwarfism. Clin Dysmorphol 5:159–164.
Al Mane KA, Coates RK, McDonald P. 1996. Intracranial calcification inRaine syndrome. Pediatr Radiol 26:55–58.
Blomstrand I, Claesson I, Save-Soderbergh J. 1985. A case of lethal con-genital dwarfism with accelerated skeletal maturation. Pediatr Radiol15:141–143.
Brodie SG, Lachman RS, Crandall BF, Fox MA, Rimoin DL, Cohn DH,Wilcox WR. 1998. Radiographic and morphologic findings in a previ-ously undescribed type of mesomelic dysplasia resembling atelosteo-genesis type II. Am J Med Genet 80:247–251.
Camera G, Giordano F, Mastroiacovo P. 1986. Pyknoachondrogenesis: Anassociation of skeletal defects resembling achondrogenesis with gener-alized bone sclerosis. A new condition? Clin Genet 30:335–337.
Chitayat D, Gruber H, Mullen BJ, Pauzner D, Costa T, Lachman R, RimoinDL. 1993. Hydrops-ectopic calcification-moth-eaten skeletal dysplasia(Greenberg dysplasia): prenatal diagnosis and further delineation of arare genetic disorder. Am J Med Genet 47:272–277.
Colavita N, Kozlowski K. 1984. Neonatal death dwarfism—a new form.Pediatr Radiol 14:451–452.
Gelb BD, Shi GP, Chapman HA, Desnick RJ. 1996. Pycnodysostosis, alysosomal disease caused by cathepsin K deficiency. Science 273:1236–1238.
Hart TC, Bowden DW, Bolyard J, Kula K, Hall K, Wright JT. 1997. Geneticlinkage of the tricho-dento-osseous syndrome to chromosome 17q21.Hum Mol Genet 13:2279–2284.
Horton WA, Rimoin DL, Hollister DW, Lachman RS. 1979. Further het-
erogeneity within lethal neonatal short-limbed dwarfism: the platy-spondylic types. J Pediatr 94:736–742.
Jobert A-S, Zhang P, Couvineau A, Bonaventure J, Roume J, Le Merrer M.1998. Absence of functional receptors for parathyroid hormone andparathyroid hormone-related peptide in Blomstrand chondrodysplasia.J Clin Invest 102:34–40.
Johnson ML, Goudong G, Kimberling W, Recker SM, Kimmel DB, ReckerRR. 1997. Linkage of a gene causing high bone mass to human chro-mosome 11 (11q12-13). Am J Hum Genet 60:1326–1332.
Kan AE, Kozlowski K. 1992. New distinct lethal osteosclerotic bone dys-plasia (Raine syndrome). Am J Med Genet 43:860–864.
Kozlowski K, Tsuruta T. 1989. Dysplastic cortical hyperostosis: a new formof lethal neonatal dwarfism. Br J Radiol 62:376–378.
Kozlowski K, Tsuruta T, Taki N, Tsunoda I, Ozawa H, Hasegawa T, Sil-lence D. 1986. A new type of achondrogenesis. Pediatr Radiol 16:430–432.
Martınez-Frıas ML, Bermejo E, Urioste M, Huertas H, Arroyo I. 1993.Lethal short rib-polydactyly syndromes: further evidence for their over-lapping in a continuous spectrum. J Med Genet 30:937–941.
Muller D, Kozlowski K, Sillence D. 1992. Lethal micromelic facial bonessclerosis dysplasia. Br J Radiol 65:1137–1139.
Nairn ER, Chapman S. 1989. A new type of lethal short-limbed dwarfism.Pediatr Radiol 19:253–257.
Peeden JN, Rimoin DL, Lachman RS, Dyer ML, Gerard D, Gruber HE.1992. Spondylometaphyseal dysplasia, Sedaghatian type. Am J MedGenet 44:651–656.
Perri G. 1978. A severe form of metatropic dwarfism. Pediatr Radiol 7:183–185.
Raine J, Winter RM, Davey A, Tucker SM. 1989. Unknown syndrome:Microcephaly, hypoplastic nose, exophthalmos, gum hyperplasia, cleftpalate, low set ears, and osteosclerosis. J Med Genet 26:786–788.
Sedaghatian MR. 1980. Congenital lethal metaphyseal chondrodysplasia:A newly recognized complex autosomal recessive disorder. Am J MedGenet 6:269–274.
Seller MJ, Berry AC, Maxwell D, McLennan A, Hall CM. 1996. A newlethal chondrodysplasia with platyspondyly, long bone angulation andmixed bone density. Clin Dysmorphol 5:213–215.
Sly WS, Hu PY. 1995. The carbonic anhydrase II deficiency syndrome:Osteopetrosis with renal tubular acidosis and cerebral calcification. In:Scriver CR, Beaudet AL, Sly WS, Valle D, editors. The metabolic andmolecular bases of inherited disease. 7th ed. New York: McGraw-Hill.p 4113–4124.
Spranger J, Maroteaux P. 1990. The lethal osteochondrodysplasias. AdvHum Genet 19:1–45.
Taybi H, Lachman RS. 1996. Radiology of syndromes, metabolic disorders,and skeletal dysplasias. 4th ed. St. Louis: Mosby-Year Book, Inc.
Van Hul W, Bollerslev J, Gram J, Van Hul E, Wuyts W, Benichou O,Vanhoenacker F, Willems PJ. 1997. Localization of a gene for autoso-mal dominant osteopetrosis (Albers-Schonberg disease) to chromosome1p21. Am J Hum Genet 61:363–369.
Van Hul W, Balemans W, Van Hul E, Dikkers FG, Obee H, Stokroos RJ,Hildering P, Vanhoenacker F, Van Camp G, Willems PJ. 1998. VanBuchem disease (hyperostosis corticalis generalisata) maps to chromo-some 17q12-q21. Am J Hum Genet 62:391–399.
Whyte MP. 1997. Searching for gene defects that cause high bone mass.Am J Hum Genet 60:1309–1311.
Wilcox WR, Lucas BC, Loebel B, Bachman RP, Lachman RS, Rimoin DL.1998. Pacman dysplasia: report of two affected sibs. Am J Med Genet77:272–276.
Young ID, Zuccollo JM, Broderick NJ. 1993. A lethal skeletal dysplasiawith generalised sclerosis and advanced skeletal maturation: Blom-strand chondrodysplasia? J Med Genet 30:155–157.
Lethal Osteosclerotic Skeletal Dysplasia 377