leveraging the ehr to your advantage: make the electronic
TRANSCRIPT

Leveraging the EHR to Your Advantage: Make the electronic beast work for you!
Manoj K. Mehta, MD, FACG Endoscopy Center of the North Shore, Wilmette, IL
Richard L. Nemec, MD, FACG Winchester Gastroenterology Associates, Winchester, VA Aside from the COVID-19 pandemic, there is probably no single more difficult hurdle within the last generation of medicine than the implementation of electronic health records (EHR) as mandated by the 2009 HITECH Act1. Scanning and destruction of paper records, steep learning curves, IT issues, multiple platforms, difficult to navigate patient encounters, cost, and delayed integration have plagued nearly every practice. Physicians identify their obligations to the EHR as a major source of stress, and therefore physician burnout2,3. Many more physicians report taking work home with them to complete after hours than during the paper-chart era3. The EHR is a template-driven system, and the more complex efforts to perform “data entry” become a major impediment to delivery of care.
That is not to say there have not been major benefits, and in the early days of any process, it is easy to focus on the negative. The EHR has clearly helped us with governmental compliance, legibility, record permanency, pre-populating notes, and potentially shorter encounters. This article will explore ways to leverage as much good out of your EHR as possible. By grooming your electronic health record, you might start to see the positives outweigh the negatives.
The EHR is a tool. The key to making any tool work appropriately for you is to learn how to use it. Computers have the advantage of being programmable, and therefore malleable to the needs of a number of different users. Unlike most tools, which have only one right way to use them, your EHR can be made to work to your style. The good news is, you don’t need to be a programmer to set up an EHR to work in your favor.
Epic and Cerner, combined, comprise over 50% of the HIT market. Bigger healthcare systems appear to
Epic 30.9%
Cerner 25.1%
MEDITECH 14.7%
Evident 8.1%
Allscripts 5.7%
Top 5 EHR’s in the US by Market Share4
favor Epic and ambulatory centers appear to favor Cerner5. One of the biggest advantages of being aligned with a larger healthcare system is a strong information systems support staff. Classes, trainers,

and after-hours support can be invaluable. Trainers may have learned tricks and tips, and more trainers equals more means to achieve the same ends. However, one of the biggest drawbacks of a larger system is bureaucracy. One author here was surprised to get a call back for a help ticket request submitted a year prior!
What can this guide to for you?
This guide can get you started, provide ideas of what can be accomplished, open your eyes to what can be improved, and point you to resources to achieve what you need. It cannot give you specific, step-by-step instructions. There are simply too many EHR’s, and even a single EHR can have multiple versions. You will have to do some research, sit down in front of the computer, and perhaps consult your trainer for advanced tips and setup. However, spending a few hours up front could save you untold amounts of time in the future.
What can your EHR do for you?
1. Help you type?
Yes, actually. Many EHR’s have autocorrect functions. If you commonly misspell something, enter it into the autocorrect dictionary. Amytriptiline becomes “amitriptyline” without a second thought. You can also use this as a shortcut. Enter an abbreviation for any string in autocorrect, and every time you enter the shorter string, the entire phrase will be entered. Nonstandard abbreviations can be normalized. For example, “hf” becomes “hepatic flexure,” “ih” becomes “internal hemorrhoids” and so on. Even standard abbreviations can be made more readable, as things you find common might be foreign to people in other specialties. For example, “WON” can be automatically changed to “walled off necrosis.” This can speed up your workflow, achieve better communication, and make you look more professional.
Any EHR will require typing. If you never learned to type, it might be worth a typing class. The investment in time and energy will pay off in the long run; if nothing else it will keep the EHR from being a major source of stress. If typing is not an option, there are possibilities like voice recognition/transcription. For example, Dragon Medical can be used in conjunction with your EMR, boasts a 99% accuracy for speech recognition and is encrypted for HIPPA compliance. Traditional transcription services, and medical scribes can also be used to populate the EMR but can increase expenses.
2. Achieve more meaningful communication with patients
The 21st Century Cures Act was signed into law in 20166. One of the mandates is increased transparency for patient access to your notes and tests you have ordered. This means that not only patients may get results before you see them, but they will also be able to read many of your notes just as written. Notwithstanding the lack of medical education in the general public leading to much confusion and perhaps concern, the medical language we use will raise a myriad of questions. Save yourself from the inbox messages and phone calls by cleaning up dialogue. With autocorrect, you can type SOB and have the EHR correctly write out “shortness of breath,” PO to “by mouth,” and BRBPR to “bright red blood
per rectum.” These shorthand notations were developed when writing was done by hand, but we are not tied to that now.
Patient portals, or your “inbox,” are another common consumer of overall computer time. Answering questions this way has the advantage of permanency in the record, but is also a source of after-hours computer time and potentially overall frustration. As with anything, there will be respectful users of your time, and perhaps patients who abuse this system. Use the system at a balance, benefiting you and your patients. If that balance is lopsided, don’t be afraid to ask the patient to make an appointment to address their questions and advise them the portal is not a good place for urgent or detailed dialogue.
3. Reduce your workload
For more control, create a smart phrase. In Epic, these are preceded by a dot, so “.PREP” could print out the entire bowel prep regimen step-by-step. Like autocorrect, you need to set these up. That is a little time consuming, but will pay dividends in the long run. Please note, you can usually look at others’ smart phrases in Epic, and these are not proprietary to the user, so they can be copied and pasted into your own smart phrases. The EHR gGastro has MACROs that operate similarly.
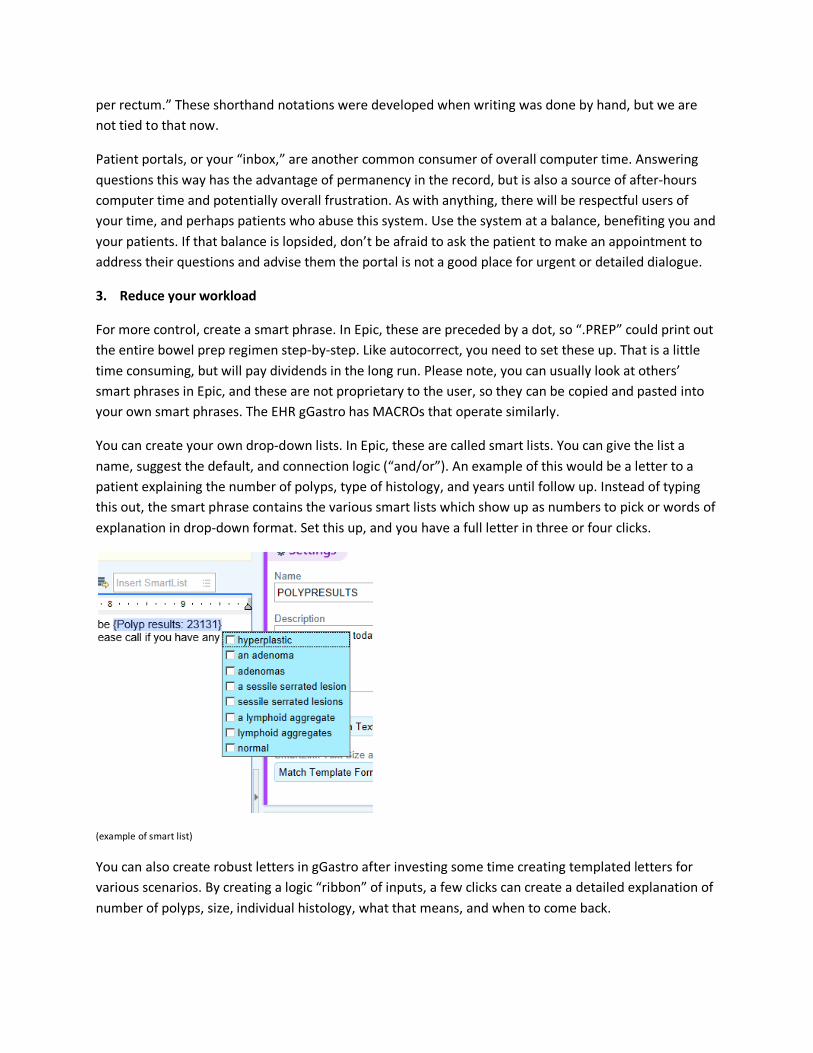
You can create your own drop-down lists. In Epic, these are called smart lists. You can give the list a name, suggest the default, and connection logic (“and/or”). An example of this would be a letter to a patient explaining the number of polyps, type of histology, and years until follow up. Instead of typing this out, the smart phrase contains the various smart lists which show up as numbers to pick or words of explanation in drop-down format. Set this up, and you have a full letter in three or four clicks.
(example of smart list)
You can also create robust letters in gGastro after investing some time creating templated letters for various scenarios. By creating a logic “ribbon” of inputs, a few clicks can create a detailed explanation of number of polyps, size, individual histology, what that means, and when to come back.

(example of gGastro template ribbon)
4. Document E/M coding (with a warning)
Many EHR’s support disease-specific templates. You can create a template for a patient with, say, abnormal liver enzymes, which covers all the historical points that you typically ask, as well as the orders that you would write. Not only will this help you and your patient, but oftentimes the more specific documentation leads to more accurate coding for billing!
ACG has spent considerable effort in developing guidelines in the evaluation and management (E/M) of most significant GI conditions. By building a smart phrase (or similar process in other EHR systems), you can incorporate the latest guideline into your note with one smart phrase or ribbon. For example, the following ribbon in gGastro can be set up to select Celiac, subtype refractory, and subsequently fill in the entire 2013 ACG management guidelines into your note.
(example of gGastro guideline selection)
However, you must be careful with templates. You are probably all aware that you can generate almost an entire note with all the past medical history, vitals, and usual note requirements. Do not get too caught up in this. Notes that claim a gastroenterologist examined the optic fundus will be suspicious. Cutting and pasting from your prior note, in part, is fine. Just keep in mind when you are writing it that it is a rolling history and that you will be building on it. You’ve all seen notes that say “awaiting x” even though it’s been done for days. Do not be that person. Copying and pasting others’ notes is not a good

idea, as errors get perpetuated. Also know that there is an element of “note fatigue.” A longer note filled with pre-populated information tends to not get read. Change the font for your impression and plan, bold it, or even put it at the top above the computer-generated information. Still, a properly set-up note template is instrumental in making you efficient. In 2021, a “Patients over Paperwork” initiative refocuses E/M coding on complexity of patient care rather than overall face-to-face time spent. You can qualify your billing via either total time spent or complexity of medical decision making. The American Medical Association (AMA)7 and ACG both have guidelines you can use to assess what level E/M code is appropriate. 5. Make you look good
Do you find yourself making the same teaching points? Make a smart phrase that encompasses the nature of Ranson’s criteria, the differential diagnosis for post-op hyperbilirubinemia, or a hyperlink to a reference article. One author here uses a smart phrase .STRATE when trying to stop the habitual restriction of nuts in patients with diverticulosis. This phrase inserts “see LL Strate, et al, Nut, corn, and popcorn consumption and the incidence of diverticular disease. JAMA. 300(8):907-14, 2008 Aug 27.” By using these short cuts you can provide increased diagnostic accuracy, precision in the care you deliver for your patient, and thoroughness of documentation.
Epic is soon to roll out a tool called Synopsis, which allows chronological tracking of interventions and recorded outcomes. For example, in IBD, you would record the patient's past history of interventions and status updates with semi-quantitative scores (e.g., HBI, CDAI, Mayo scores) via your template. Synopsis can generate a report that contains a rolling history of the patient's previous symptoms, treatments, and (most importantly) responses. At a glance, you could see the Mayo score and how it correlated with different biologics, calprotectin, or even seasonality. Think about the power of this tool when evaluating DILI. Every drug used when overlying a graph of LFT’s! 6. Order efficiently
Admitting diagnoses can be set up to generate order sets (e.g., orders relevant to abnormal liver enzymes, variceal bleeding, or colonoscopy preparation). By creating an order set/smart phrase/macro (depending on your EHR), you can quickly and rapidly order all necessary tests in the evaluation and management of your patient's condition. Not only does this increase the efficiency of your orders, but it increases the consistency of your orders and the quality of your patient care. Finally, it helps you to "remember" all the necessary orders for this condition. Did you “remember” that celiac disease can cause abnormal LFT’s? It may or may not be relevant to your case, but there is the order to remind you to consider it. Below is an example of what part of an order set looks like in Epic for abnormal liver enzymes.

(example of order set for LFT’s in Epic)
Here is an example of part of the potential order set for a patient admitted with abnormal liver enzymes in gGastro.
(example of order set for LFT’s in gGastro)
7. Remind yourself of something important
Use the power of the computer to your advantage: it remembers everything you tell it to. Do you find yourself repeatedly looking up, say, the management of pancreatic cysts? Or perhaps the ascites characteristics of nephrotic syndrome? Create a smart phrase encompassing what you need to know, and you can pull it up in a note and then delete it after you’ve refreshed your thinking on this subject. This will save you from going back and forth to Google.
Let the computer remind you (or your staff) of the need for future care for a specific patient. If there is an imaging study that needs a follow-up study in six months, the computer can remind you when that is

due. You or your support staff can use the reminder function to warn you when the IBD patient is due for routine labs, levels, vaccines, or if they have a TB evaluation due. Your EHR can be constructed to create appropriate recalls and reminders whether for labs, imaging, endoscopic procedures, vaccinations, etc. It only takes a little time to set this up in your EHR and your patients will benefit from your efforts. Epic has reminders available for you, for staff, and in the Inbox areas separately Here is an example you can send yourself after a patient visit.
(example of self-reminder in encounter)
Similarly, for your staff.
(example of Epic reminder for staff)
The reminder tab in Epic will let you send yourself an inbox message.
(example of Epic in basket reminder)
8. Separate the wheat from the chaff
You can generally modify the EHR start page to show your schedule, notes, patient list, and any number of other factors. Each of these, in turn, can be modified to suit you. Choose the best formats that works for your needs. Are you on rounds in the hospital? Start with your patient list. Endoscopy day? Start with your schedule.

The gGastro example shown below allows you to enter a brief note for rapid review of the case directly on the schedule. Epic has similar Sticky Notes you can leave yourself, and even Specialty Notes all other GI’s can see. The latter is a great way to communicate about your specialties “frequent flyers.”
(example of gGastro schedule)
You can change the search function defaults, for example, to display notes from you, your partners, or your specialty first. This lets you hone in on what is probably most relevant to you as a consultant, and bypass those infamous notes from music therapy.
(example of chart review limited to GI notes)
You can also set up templates or short cuts to review specific labs (e.g., "bleeding labs,” "liver labs,” "ERCP labs") that allow you to quickly access only the labs that you need. The same thing can be done with imaging studies by creating a template or shortcut for "GI imaging only.”
9. Use available metrics

You are all probably familiar with the reports you get from your endoscopy report writing system, showing your ADR, how you compare to peers and the national standards, how many sessile serrated lesions you find, and perhaps your time efficiency in the GI Lab. Did you know there are similar, and even much more robust, resources available to assess how efficiently you use your EHR time? Epic is constantly tracking everything you do. What times are you logged on, how much time you spend in your basket answering messages, how much time writing orders, and how much time in chart review. It tracks how much time you spend writing notes, how many characters are in your average note, and even how much of that note is cut and paste vs original writing. This data is presented in a pathway called Signals. It is overwhelmingly thorough. Be aware the information is not blinded like your ADR data might be. You can see every person’s details in your section, in your hospital, and even across institutions. All centers using Epic are included. At a minimum executives, project directors, and managers qualify for access, so someone at your organization can get this information. Here are some examples of what that data looks like.
The above institution’s data shows that group spends more time than most organizations in notes, placing it at the bottom 25% of efficiency. The medical specialties spend the longest time in notes, several minutes per day longer than the national average. Neurology and Psychiatry write long notes as well, but less than the national Epic average.

Where it really gets interesting is looking at your department by itself, and looking at yourself vs various colleagues. The Signals system can give you an overall user proficiency score. Here is a detail shot of what one efficient users profile looks like:
This doctor, like all of us, has a few overnight calls. But they start their use of the EHR at 9AM every day and are done by 6PM. Almost no work is being done after hours. This is efficiency—and suggests a good work/life balance. This has implications about quality of life and overall satisfaction. Contrast that graph with the following:
This doctor has 12AM to 7AM off every day, but otherwise is working as much between 8PM and midnight as they are during the day! Before jumping to conclusions about work volume, Signals gives you that as well. Both these doctors saw the same number of patients per day on average for the time period reported. Signals has the capability to drill down on where you are efficient or not. Without data on where you are, it is hard to know where to make changes. The graphs above show that the time physicians spend in the chart are exactly the areas covered in this article. If you can make your smart phrases and smart lists efficient, you can shrink your time in the in basket. If your orders and notes can be groomed to happen

quickly and efficiently, that time shrinks as well. If you use Synopsis and chart review via the tips shown here, you can reduce your clinical review time as well.
Conclusions
Getting the most out of your EHR involves a little bit of setup time. But in the end it saves you time, makes you look good, and shortens your workload instead of expanding it. This doesn’t just help you; it helps your patients. The EHR is here to stay. You might as well use the power of the computer to remember and organize things for you, help you find information, and help you communicate effectively. As you free up time spent struggling with notes and orders, you can get back to doing what you do best—taking care of patients.
Practical steps to implement these ideas:
1) Ask and answer the question: What makes my EHR so painful? (Pick your top three)
2) Ask and answer the question: What do I need to change in my EHR to make it more helpful to me? Use the data from Signals (if you are an Epic user), or just pick your top three.
3) Review some of the specific ideas attached to this article. Do you like any that you see?
4) Decide how much time you want to invest in the process. Do you want someone to set it up, show you how to use it, and just use it in a static fashion moving forward? Or do you want to do a “deep dive” on learning how to create and modify the EHR on the go? The more you invest, the greater the return, but we all know we have limits.
5) Take your preferred ideas from #1 through #3 above to your local EHR expert--those people really do exist! Take an active role in building the structure that addresses YOUR wants: whether it be through templates, smart phrases, short cuts, or different views.
6) Preview with partners and list “shortcuts” or EHR efficiencies that they have found or developed for various tasks or documentation, list them, and disperse to others to improve group efficiency. This can also be done on a staff level and revisit biannually to update ideas. We all have different skill sets and can empower others in the group.
6) As you learn how to make your EHR work for you, you can identify other areas for improvement and efficiency.
7) Show others how you have improved the generic EHR at your hospital or practice. This will not only help your colleagues, but as you instruct others, you will become a local expert.
References
1. Boonstra, A., Versluis, A., & Vos, J. F. (2014). Implementing electronic health records in hospitals: a systematic literature review. BMC health services research, 14, 370. https://doi.org/10.1186/1472-6963-14-370
2. Medscape National Physician Burnout, Depression & Suicide Report 2019 https://www.medscape.com/slideshow/2019-lifestyle-burnout-depression-6011056
3. Rebekah L Gardner, Emily Cooper, Jacqueline Haskell, Daniel A Harris, Sara Poplau, Philip J Kroth, Mark Linzer, Physician stress and burnout: the impact of health information technology, Journal of the American Medical Informatics Association, Volume 26, Issue 2, February 2019, Pages 106–114, https://doi.org/10.1093/jamia/ocy145
4. Alanna Moriarty. The 10 Most Common Inpatient EHR Systems by 2019 Market Share. The Definitive Blog, Definitive Healthcare. https://blog.definitivehc.com/most-common-inpatient-ehr-systems
5. Forrest Brown. Cerner vs. Epic: Comparing the Biggest EHR Vendors. Technology Advice. https://technologyadvice.com/blog/healthcare/cerner-vs-epic/
6. 21st Century Cures Act https://www.congress.gov/114/plaws/publ255/PLAW-114publ255.pdf 7. AMA CPT E/M Office Revisions Level of Medical Decision Making (MDM). https://www.ama-
assn.org/system/files/2019-06/cpt-revised-mdm-grid.pdf