lgbt aging: hiv prevention and primary care for lgbt older ... · lgbt aging: hiv prevention and...
TRANSCRIPT
LGBT Aging: HIV Prevention and Primary Care for LGBT Older Adults
Jonathan S. Appelbaum, MD, FACP, AAHIVS Associate Professor and Education Director, Internal Medicine
Florida State University College of Medicine Harvey Makadon, MD
Director, National LGBT Health Education Center This publication was produced by the National LGBT Health Education Center, The Fenway Institute, Fenway Health with funding under cooperative agreement# U30CS22742 from the U.S. Department of Health and Human Services, Health Resources and Services Administration, Bureau of Primary Health Care. The contents of this publication are solely the responsibility of the authors and do not necessarily represent the official views of HHS or HRSA.
Continuing Medical Education Disclosures Program Faculty: Jonathan S. Appelbaum, MD Current Position: Associate Professor and Education Director, Internal
Medicine Florida State University College of Medicine, Tallahassee, FL Disclosure: Speaker’s Bureau: Florida AETC and Clinical Care
Options/HealthHIV Program Faculty: Harvey J Makadon, MD Current Position: Director, the National LGBT Health Education Center,
Assistant Professor of Medicine, Harvard Medical School Disclosure: No significant financial relationships to disclose It is the policy of The National LGBT Health Education Center, Fenway Health that all CME planning committee/faculty/authors/editors/staff disclose relationships with commercial entities upon nomination/invitation of participation. Disclosure documents are reviewed for potential conflicts of interest and, if identified, they are resolved prior to confirmation of participation. Only participants who have no conflict of interest or who agree to an identified resolution process prior to their participation were involved in this CME activity.
Learning Objectives
At the end of this webinar, participants will be able to: Describe current HIV/AIDS epidemiology and
risk factors among older adults Identify treatment and prevention issues in older
HIV patients Access and understand screening and treatment
guidelines for HIV and co-morbidities found in older HIV patients

When We Talk about the Elderly What Comes to Mind?
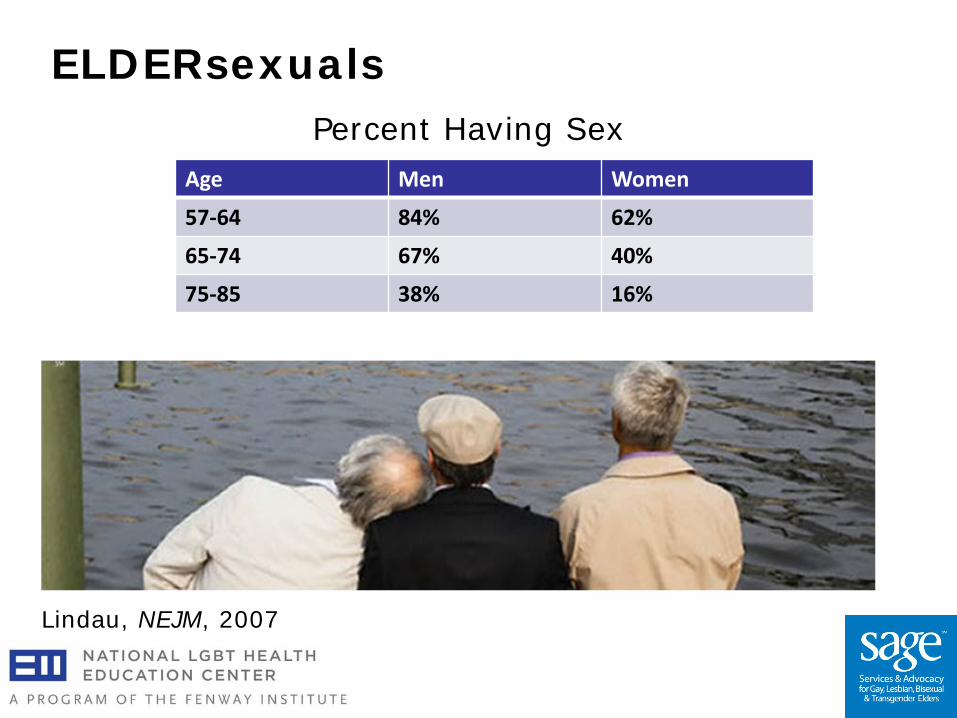
Lindau, NEJM, 2007
Percent Having Sex
ELDERsexuals
Age Men Women
57-64 84% 62%
65-74 67% 40%
75-85 38% 16%
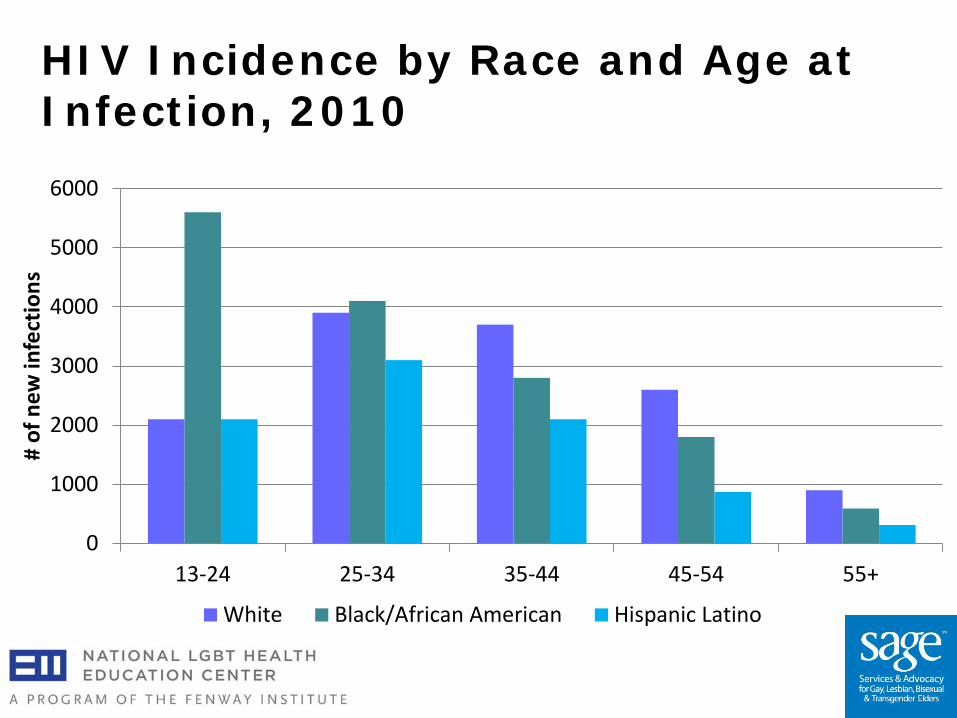
HIV Incidence by Race and Age at Infection, 2010
0
1000
2000
3000
4000
5000
6000
13-24 25-34 35-44 45-54 55+
# of
new
infe
ctio
ns
White Black/African American Hispanic Latino
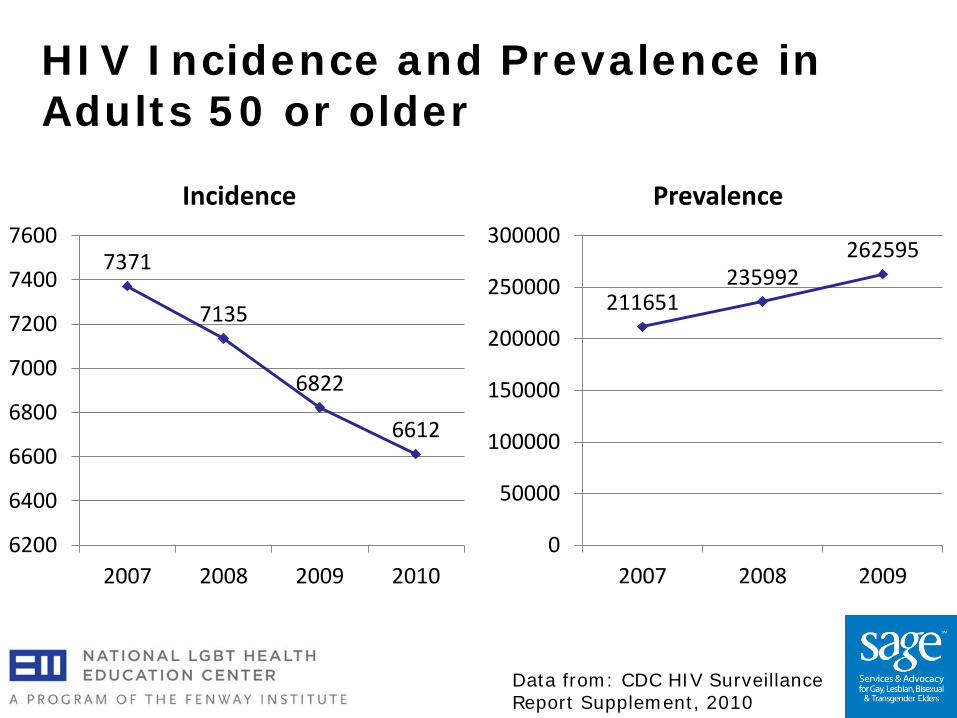
HIV Incidence and Prevalence in Adults 50 or older
7371
7135
6822
6612
6200
6400
6600
6800
7000
7200
7400
7600
2007 2008 2009 2010
Incidence
211651 235992
262595
0
50000
100000
150000
200000
250000
300000
2007 2008 2009
Prevalence
Data from: CDC HIV Surveillance Report Supplement, 2010
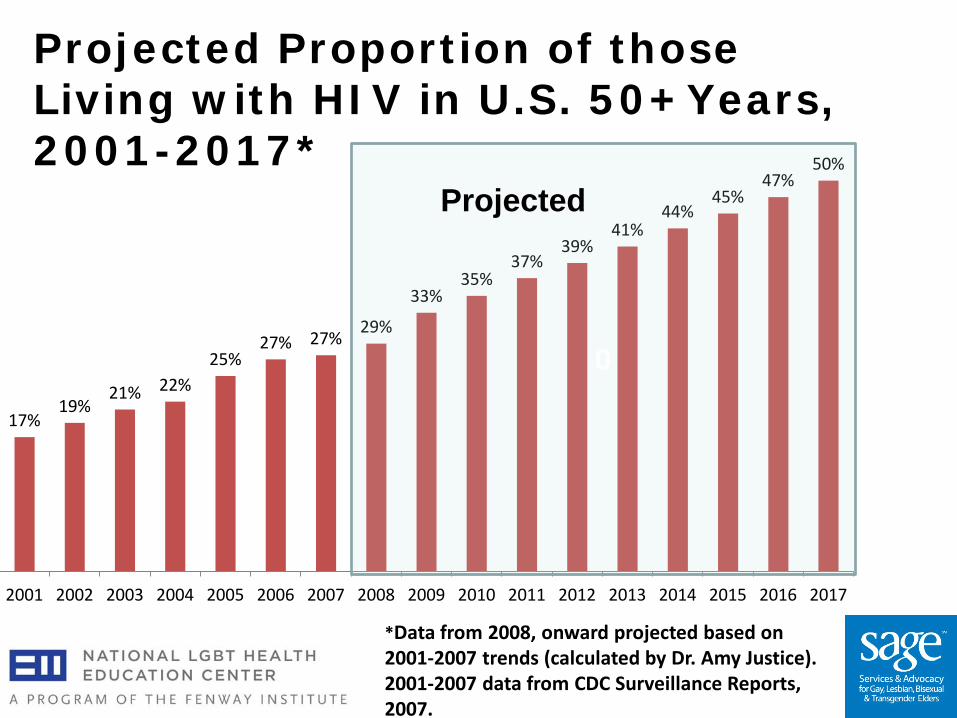
17% 19%
21% 22% 25%
27% 27% 29%
33% 35%
37% 39%
41% 44%
45% 47%
50%
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
*Data from 2008, onward projected based on 2001-2007 trends (calculated by Dr. Amy Justice). 2001-2007 data from CDC Surveillance Reports, 2007.
0
Projected
Projected Proportion of those Living with HIV in U.S. 50+Years, 2001-2017*
Challenges to Prevention and Care
Prevention fatigue Knowing treatment is possible Avoidance of discussion by clinicians Isolation makes prevention and care
more complex Discrimination in housing and long-
term care
Overcoming Barriers
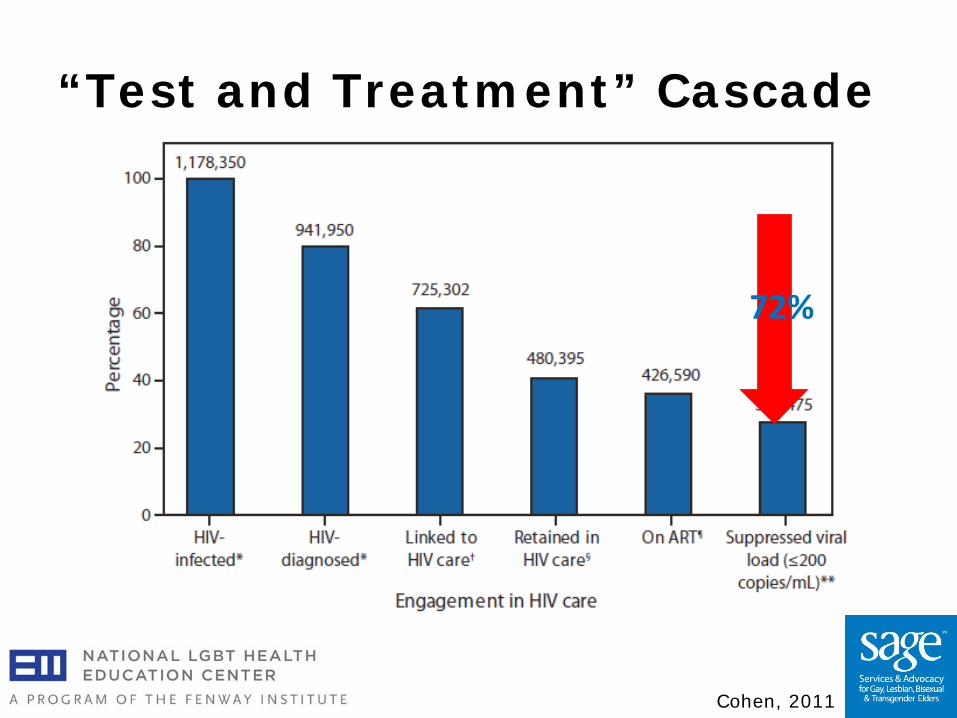
“Test and Treatment” Cascade
Cohen, 2011
72%

Barriers to Linkage to Care
Counseling and Testing Care and Treatment
Focused Prevention With Older Adults
Barriers to Routine HIV Testing
50% of EDs are aware of CDC’s guidelines, and only 56% offer HIV testing (Haukoos, 2011).
Only 61% of general internists offer HIV testing regardless of risk (Korthuis, 2011).
Accessing Antiretroviral Therapy
Newly diagnosed patients should be linked to HIV care as soon as possible.
HIV counseling and testing
should be integrated with HIV care.
Socio-economic and cultural factors impeding HIV care must be addressed.
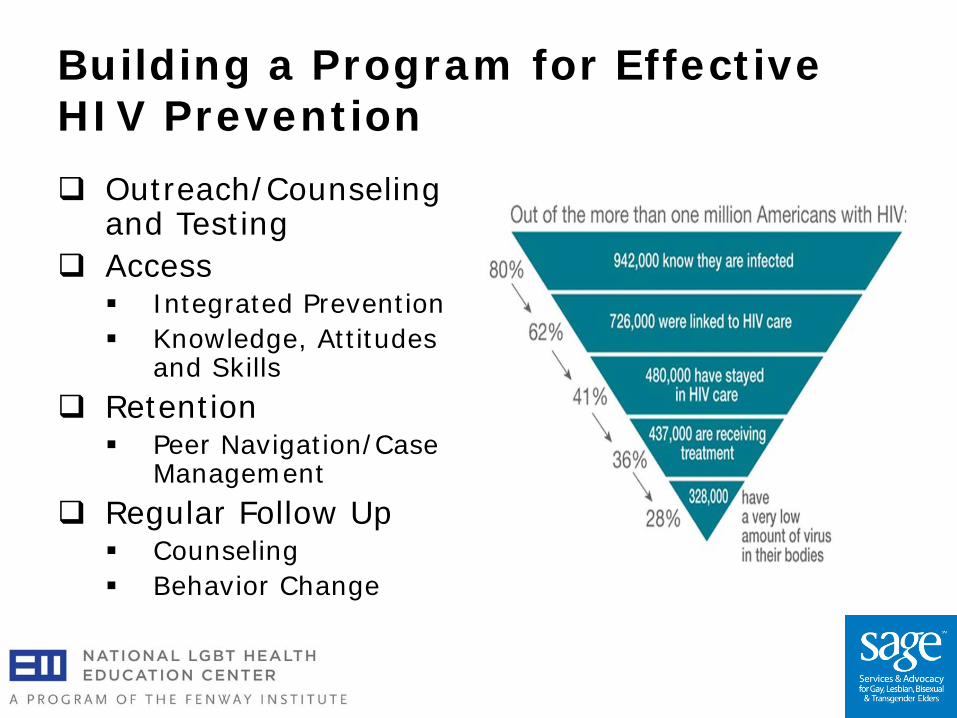
Building a Program for Effective HIV Prevention Outreach/Counseling
and Testing Access
Integrated Prevention Knowledge, Attitudes
and Skills Retention
Peer Navigation/Case Management
Regular Follow Up Counseling Behavior Change

Cultural, Clinical Competence: Quality Senior Care

Cases: HIV Treatment Issues
Kenji
Kenji 63 yo MSM HIV+ 10 yrs, CD4 420, VL <50 copies PMH: HTN, depression, DM, hyperlipidemia Meds: emtricitabine/tenofovir/efavirenz, HCTZ,
citalopram, glargine insulin, lisinopril, EcASA, pravastatin
SH: lives alone, no tobacco, IDU, has boyfriend and uses condoms intermittently
Difficulty with adherence to non-ART medicines HbA1C >10, SBP >160
Normal Aging Process
Loss of bone and muscle mass
Weight loss Decrease in kidney function Memory loss Immunosenescence
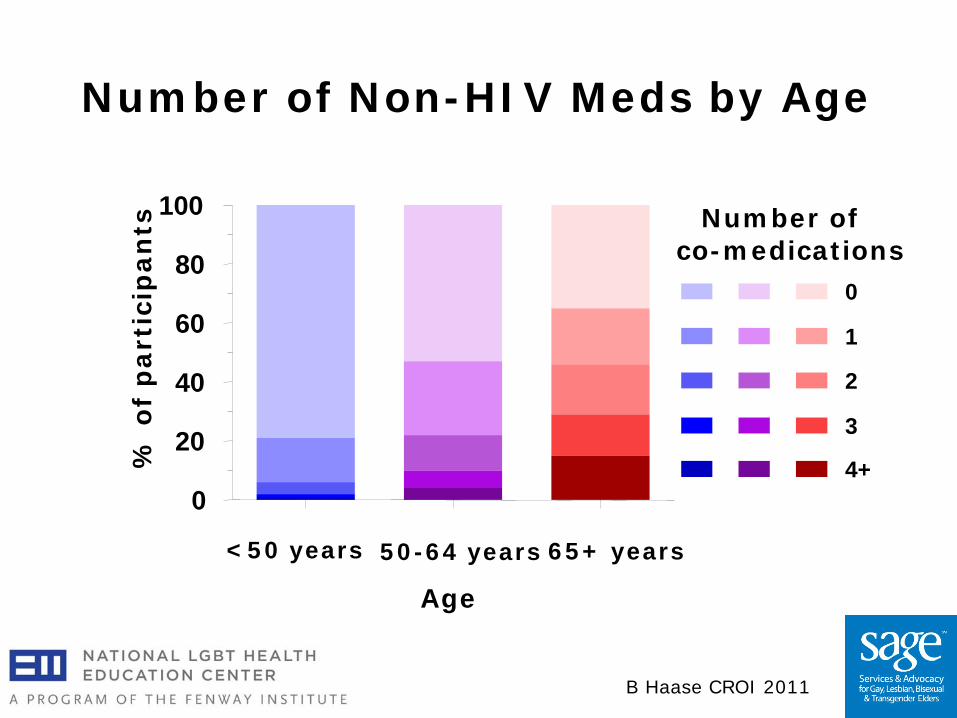
Number of Non-HIV Meds by Age
B Haase CROI 2011
0
20
40
60
80
100
% o
f p
arti
cip
ants
<50 years 50-64 years 65+ years
Age
4+
3
2
1
0
Number of co-medications
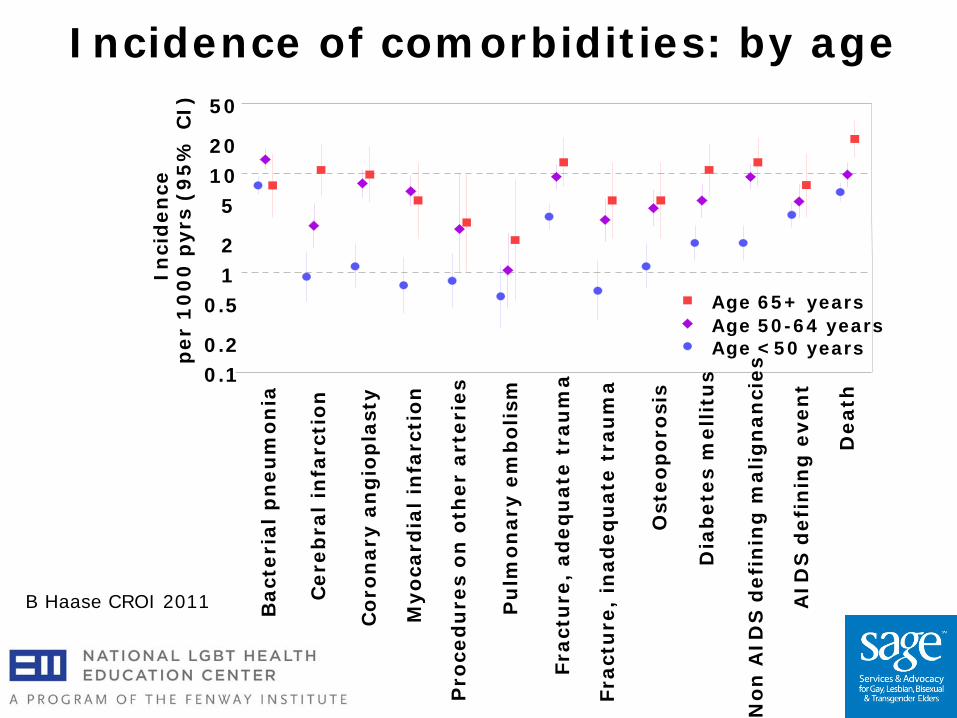
Incidence of comorbidities: by age
B Haase CROI 2011 Bac
teri
al p
neu
mo
nia
Cer
ebra
l in
farc
tio
n
Co
ron
ary
ang
iop
last
y
Myo
card
ial
infa
rcti
on
Pro
ced
ure
s o
n o
ther
art
erie
s
Pu
lmo
nar
y em
bo
lism
Frac
ture
, ad
equ
ate
trau
ma
Frac
ture
, in
adeq
uat
e tr
aum
a
Ost
eop
oro
sis
Dia
bet
es m
elli
tus
No
n A
IDS
def
inin
g m
alig
nan
cies
AID
S d
efin
ing
eve
nt
Dea
th
1 2
5 10 20
0.1 0.2
0.5 Age 50-64 years Age <50 years
Age 65+ years
50
Inci
den
ce
per
10
00
pyr
s (9
5%
CI)
Potential Comorbidities among Older Patients with HIV
Cardiovascular disease Metabolic disorders
Diabetes Dyslipidemias
Neurocognitive abnormalities Liver and renal problems Bone disorders
Osteopenia Osteoporosis
Malignancies
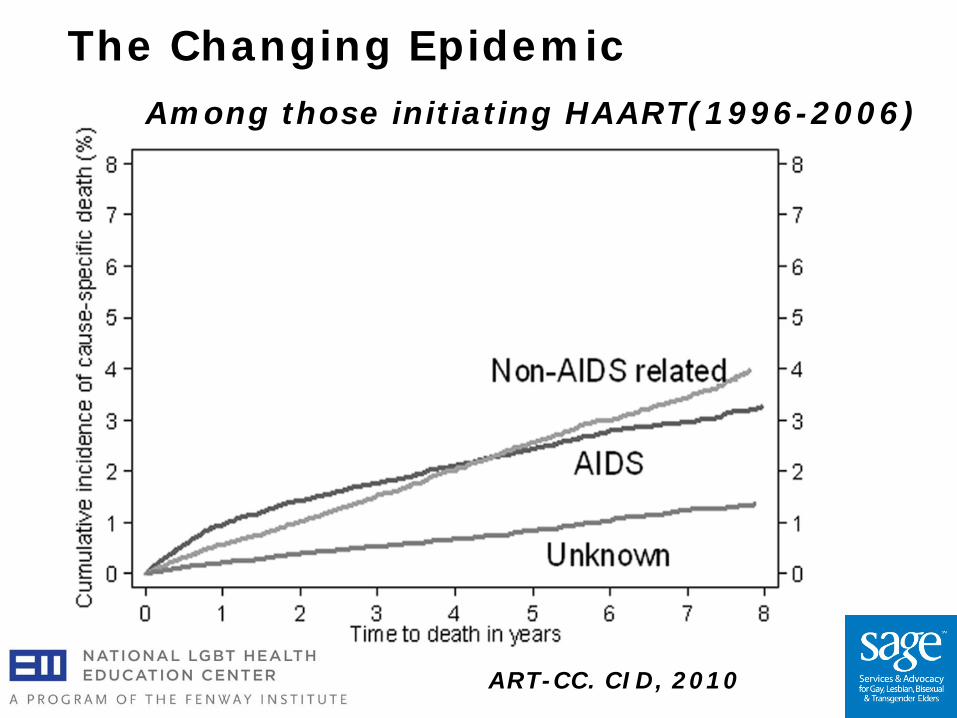
The Changing Epidemic
ART-CC. CID, 2010
Among those initiating HAART(1996-2006)
Polling Question: Would you recommend ART for this patient?
Yes No Not sure
Key Updates in 2012 DHHS Guidelines
Timing of ART initiation in treatment-naive patients Treatment as prevention Guidance on new regimens Considerations for older patients Considerations for HIV-infected women of
childbearing age Coadministration of antiretrovirals and HCV
protease inhibitors Timing of ART initiation in pt with TB
Key Considerations for Older HIV+ Patients
ART recommended in patients >50 years of age, regardless of CD4 cell count (BIII)
Why? The risk of non-AIDS related complications may increase and the immunologic response to ART may be reduced in older HIV+ patients
But, ART-associated adverse events may occur more frequently in older adults
Therefore, the bone, kidney, metabolic, cardiovascular, and liver health of older HIV-infected adults should be monitored closely
Key Considerations for Older HIV+ Patients The increased risk of drug-drug interactions
between ART and other medications commonly used in older HIV-infected patients should be assessed regularly, especially when starting or switching medications
HIV experts and primary care providers should work together to optimize the medical care of older HIV-infected patients with complex comorbidities
Counseling to prevent secondary transmission of HIV remains an important aspect of the care of the older HIV-infected patient
HIV Outcomes with ART: What We Know Already
HIV-1 viral load suppression
Older > Younger, doesn’t vary by class
CD4 cell response Younger > Older Mortality Older > Younger,
usually due to non-HIV causes
James
James
64 yo MSM, HIV+ 22 years, no OIs Smokes 1 ppd x 40 yrs Multiple ART, now on boosted darunavir,
etravirine, raltegravir CD4 321, VL<48 copies Facial lipoatrophy, truncal lipohypertrophy Other meds: metformin, lisinopril, ASA Reports decreased libido and ED
To evaluate this patient’s concerns, he should have:
CBC/LFT’s/thyroid function tests PSA Free testosterone Total testosterone All of the above
Endocrine Testosterone Deficiency: 54% had
testosterone <300 ng/dL Low androgen levels were associated with
increasing age, HIV+ IDU, HCV+ and use of psychotropic medications
Menopause: Occurs at younger age in HIV infection 46 (IQR 39-49)
Associated with increased symptoms of estrogen withdrawal
Klein CID 2005; Schoenbaum E CID 2005
Polling Question: Which of the following should be your first counseling priority?
Diet? Smoking? Exercise? Blood pressure control? Diabetes Mellitus management? Not sure
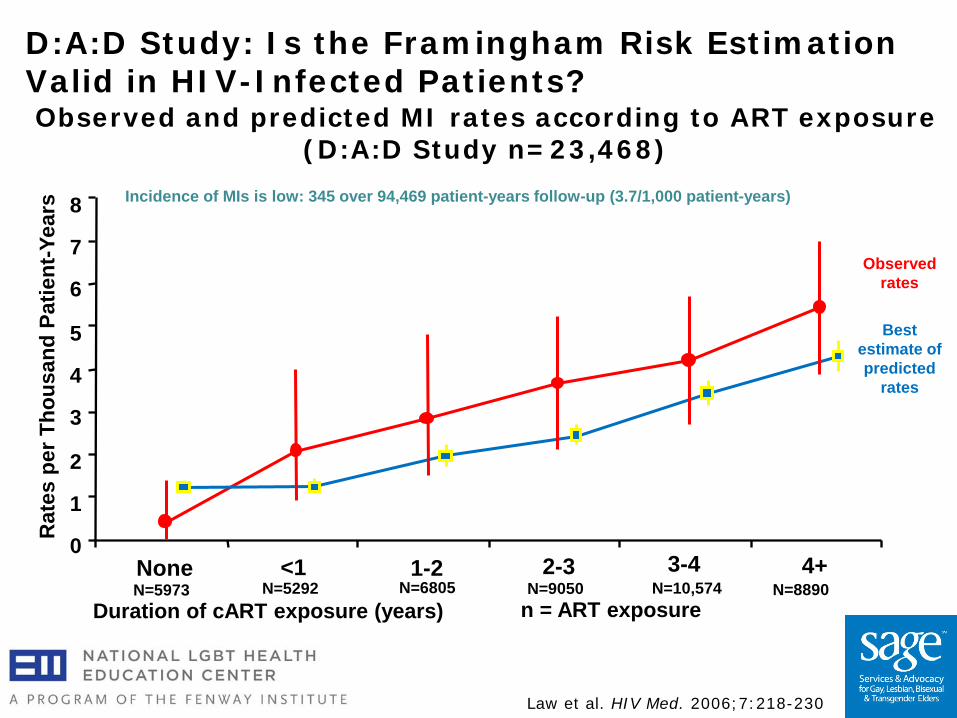
Law et al. HIV Med. 2006;7:218-230
0
1
2
3
4
5
6
7
8
Duration of cART exposure (years)
Rat
es p
er T
hous
and
Patie
nt-Y
ears
<1 1-2 2-3 3-4 4+
Observed rates
Best estimate of predicted
rates
None
Observed and predicted MI rates according to ART exposure (D:A:D Study n=23,468)
N=5292 N=6805 N=9050 N=10,574 N=8890 N=5973
Incidence of MIs is low: 345 over 94,469 patient-years follow-up (3.7/1,000 patient-years)
D:A:D Study: Is the Framingham Risk Estimation Valid in HIV-Infected Patients?
n = ART exposure
Effect of Smoking on HIV
HIV infected smokers lose more life-years to smoking than to HIV
35 year-old HIV-positive smoker has ~16 less life-years than non-smoker
Risk of smoking doubles in HIV-positive smokers compared with HIV-positive non-smokers
Helleberg M et.al. CID 2013
James: Follow Up
Free/total testosterone decreased PSA, CBC, LFTs normal Started on testosterone replacement Appropriate lab follow up done, no
improvement in symptoms Sildenafil added (dose-adjusted) with
improvement
Recommendations: Lipids
There is insufficient evidence to alter current recommendations for management of dyslipidemia or CVD/cerebrovascular disease screening by specific age criteria
Use Framingham Risk Score to guide decision
Polling Question: Should this patient be screened for osteoporosis?
Yes No Don’t Know
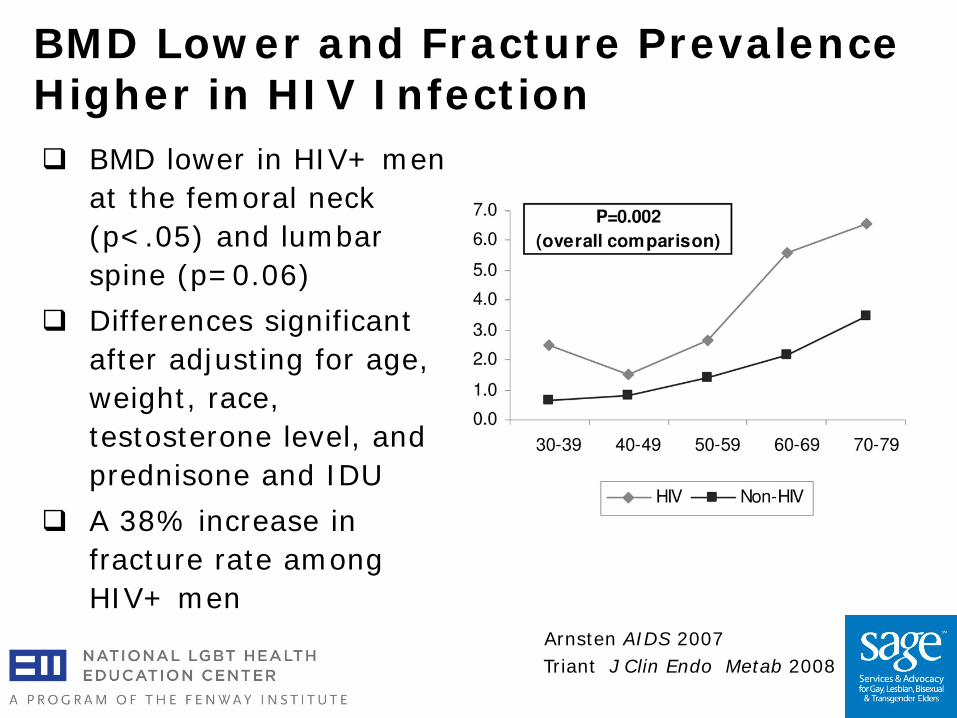
BMD Lower and Fracture Prevalence Higher in HIV Infection BMD lower in HIV+ men
at the femoral neck (p<.05) and lumbar spine (p=0.06)
Differences significant after adjusting for age, weight, race, testosterone level, and prednisone and IDU
A 38% increase in fracture rate among HIV+ men
Triant J Clin Endo Metab 2008 Arnsten AIDS 2007
Since older patients have bone loss due to
osteoporosis, and since many HIV-infected patients on ART have accelerated bone loss, screening for (and aggressive treatment of) osteoporosis should be done
Since vitamin D deficiency is prevalent in older HIV-infected persons, screening for vitamin D deficiency is warranted
Recommendations: Osteoporosis Screening
Frailty
Frailty phenotype: 3 of 5 (weight loss, exhaustion, weakness, slowness, and low physical activity). earlier occurrence in HIV-infected patients
Functional status – may be better indicator
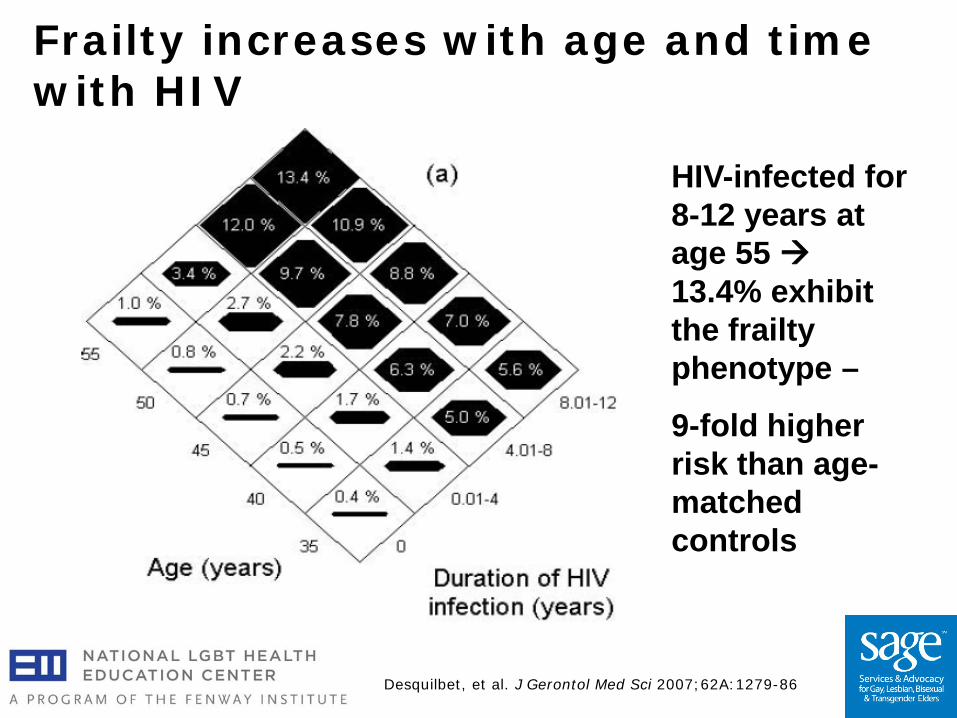
Frailty increases with age and time with HIV
Desquilbet, et al. J Gerontol Med Sci 2007;62A:1279-86
HIV-infected for 8-12 years at age 55 13.4% exhibit the frailty phenotype –
9-fold higher risk than age-matched controls
Samantha
Samantha
57 yo MTF TG, HIV x 15 years, CD4 500, VL <50 copies
PMH: HTN, stable CAD, depression, Meds: tenofovir/emtricitabine/efavirenz,
carvedilol, HCTZ, citalopram, pravastatin, conjugated estrogen, spironolactone
SH: lives with partner, no tobacco, ETOH, IDU

What health maintenance issues should you discuss?
Mammogram? Prostate screening? Colon cancer screening? Heart disease? Osteoporosis? Advance directives? All of the above?
Recommendations: Cancer Screening As part of general health maintenance practices,
cancer screening in clinically stable HIV-infected patients 50 years and older should be in accordance to current guidelines for the general population.
For cervical cancer, anal cancer, and liver cancer where HIV-specific recommendations exist, these guidelines should be adhered to instead.
For all patients, providers should take into consideration functional status and life expectancy in applying these recommendations.
When to Stop Screening
When life expectancy less than natural history of disease: for example, colorectal cancer
Patient desires/expectations Current guidelines—for example, PSA and
colon cancer screening after age 75
Impact of Hormones on HIV and Aging
MTF: Current estrogen use: 3x increase risk in CVD
mortality Total mortality 51% higher, but due to other
causes (suicide, HIV, CVD, drug abuse) FTM: No difference in mortality
Asscheman H. European Journal of Endocrinology 2011
General Routine Health Maintenance
Review ALL medications every visit Tobacco/ETOH/drug use Nutrition Injury Prevention: Burns/Falls/Driving Bowel Habits/Incontinence Psychosocial issues- $, end-of-life,
social support Please see the first two webinars in this series for more information
Other Important Issues: Holistic Care for the Older Patient
Sexuality Mobility Cognitive Impairment Depression Dealing with “triple” stigma: HIV, age, being gay Sensory Deprivation: Hearing/Vision Activities of daily living Housing stability
Conclusions
HIV infection is increasing in the older population
Older patients present later=>need to improve testing and linkage to care
Compared to younger patients, older HIV patients have: Better virologic response, less immunologic
boost, shortened survival Psychosocial issues and advanced directives
are important
Recommendations Start older patients with ART earlier for
improved CD4 counts and reducing comorbidities Watch closely for side effects/toxicities
Screen for comorbid disease (but stop screening when appropriate!) DeXA for osteoporosis Cancer screening STI’s
Recommendations Avoiding comorbid disease (good primary
care!) Vaccinations (Flu, S. pneumoniae? HZV) Smoking cessation, exercise, diet
Treat comorbid disease Treat lipids, hypertension, diabetes Substance abuse and mental health HCV
Address psychosocial issues and advanced directives

Treatment Recommendations
www.aahivm.org/hivandagingforum
Other Resources AOA: Know the Risks,
Get the Facts: Older Adults and HIV Toolkit
Hivoverfifty.org SAGEusa.org National Resource
Center on LGBT Aging: www.lgbtagingcenter.org
LGBT Aging Project