linda r.greene,rn,mps,cic manager of infection prevention highland hospital rochester, ny affiliate...
TRANSCRIPT
Linda R.Greene,RN,MPS,CICManager of Infection PreventionHighland Hospital Rochester, NY
Affiliate of University of Rochester Medical [email protected]
Clinical Uses and Ramifications of VAE Data
ObjectivesDiscuss the ramifications of VAE
Describe methods to evaluate VAE
Identify ways to use data to drive improvement

Why Collect VAE Data ?
Infection Prevention efforts may fail due to silo mentality
Need to view interventions under the larger context of patient safety
Connect the dots to harm
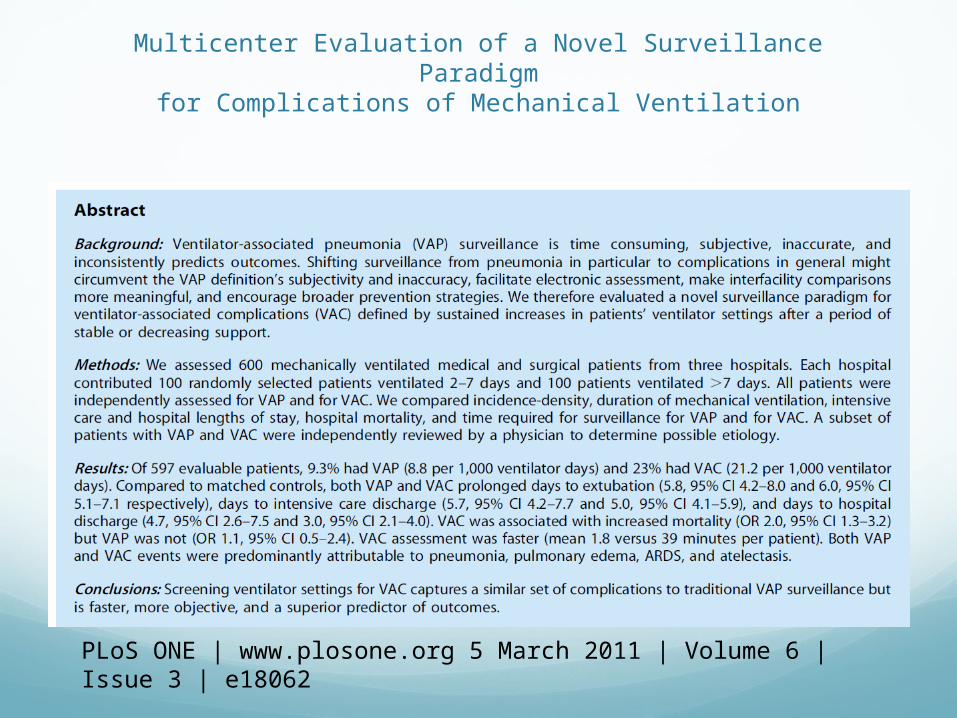
Multicenter Evaluation of a Novel Surveillance Paradigmfor Complications of Mechanical Ventilation
PLoS ONE | www.plosone.org 5 March 2011 | Volume 6 | Issue 3 | e18062
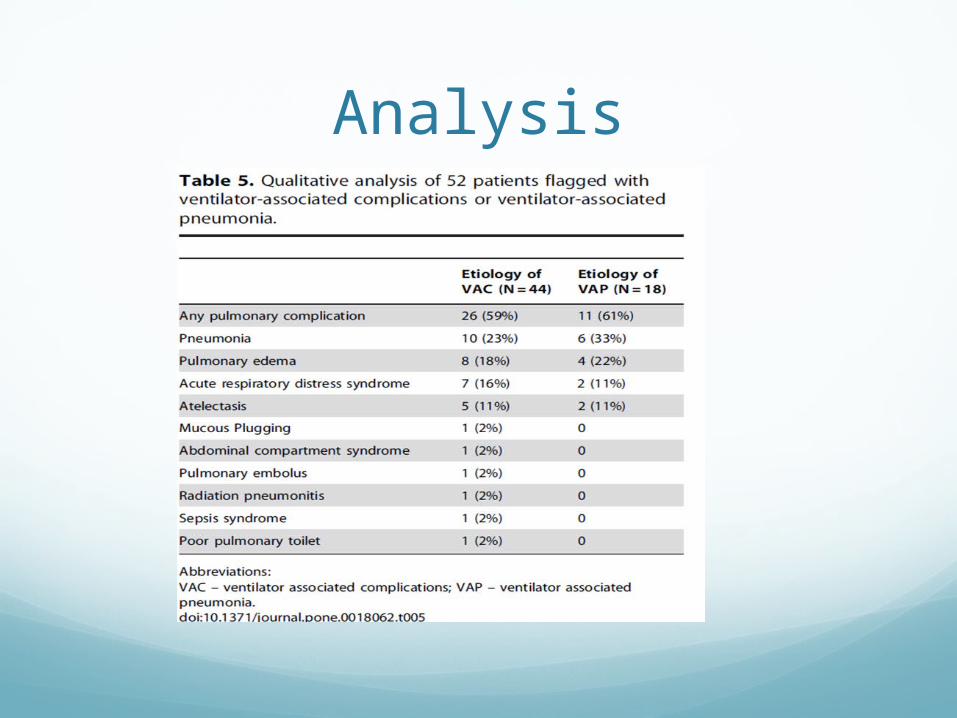
Analysis

Outcomes of VAE
Conclusions: Objective surveillance definitions that include quantitative evidence of respiratory deterioration after a period of stability strongly predict increased length of stay and hospital mortality
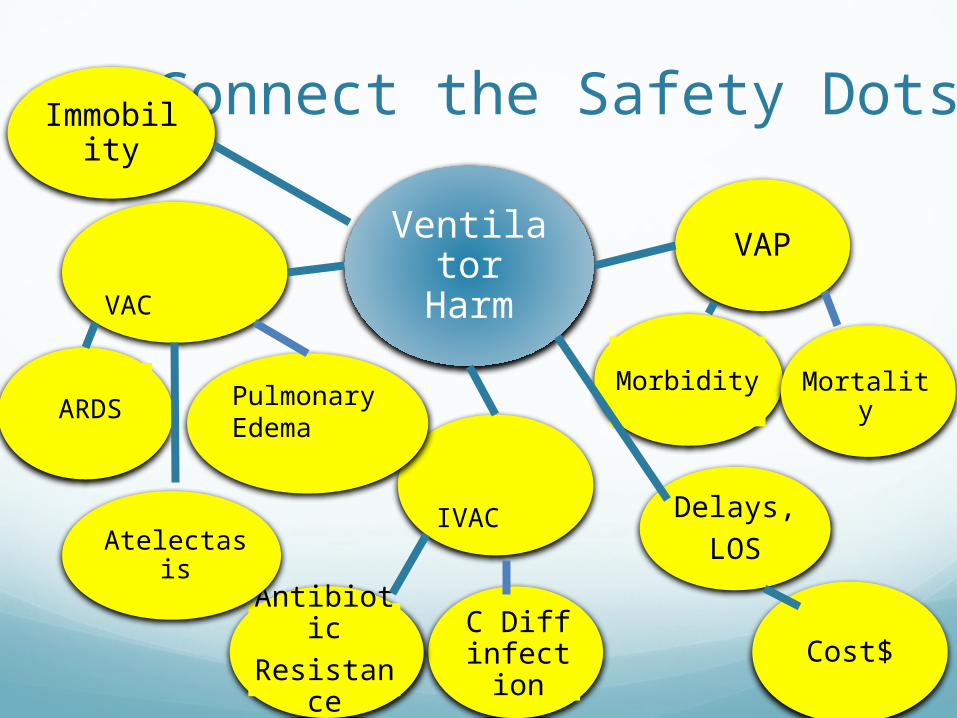
Connect the Safety Dots
ARDS
AntibioticResistance
Atelectasis
C Diff infection
Ventilator Harm
IVAC
VAC
Pulmonary Edema
VAP
Morbidity Mortality
Delays,LOS
Cost$
Immobility

Broadening the Surveillance
Intentional
Associated Conditions: • ARDS• Pulmonary Edema• Thromboembolic disease• Sepsis
Respiratory deterioration in previously stable patients is a
risk factor for increased morbidity and mortality
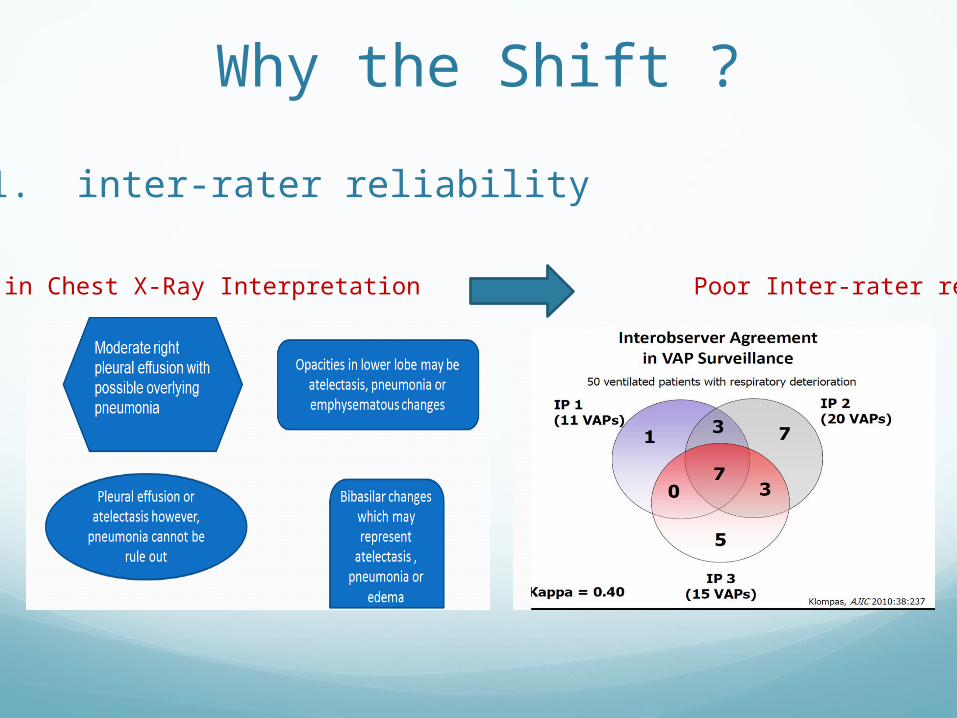
Why the Shift ?
Variations in Chest X-Ray Interpretation Poor Inter-rater reliability
1. inter-rater reliability
Why the Shift?
2. Broaden the Focus
Shifting the focus of surveillance from pneumonia alone to complications in general emphasizes the importance of preventing all complications of mechanical ventilation, not just pneumonia.
When definitions are objective, care givers can focus on what went wrong rather than debate the definition.
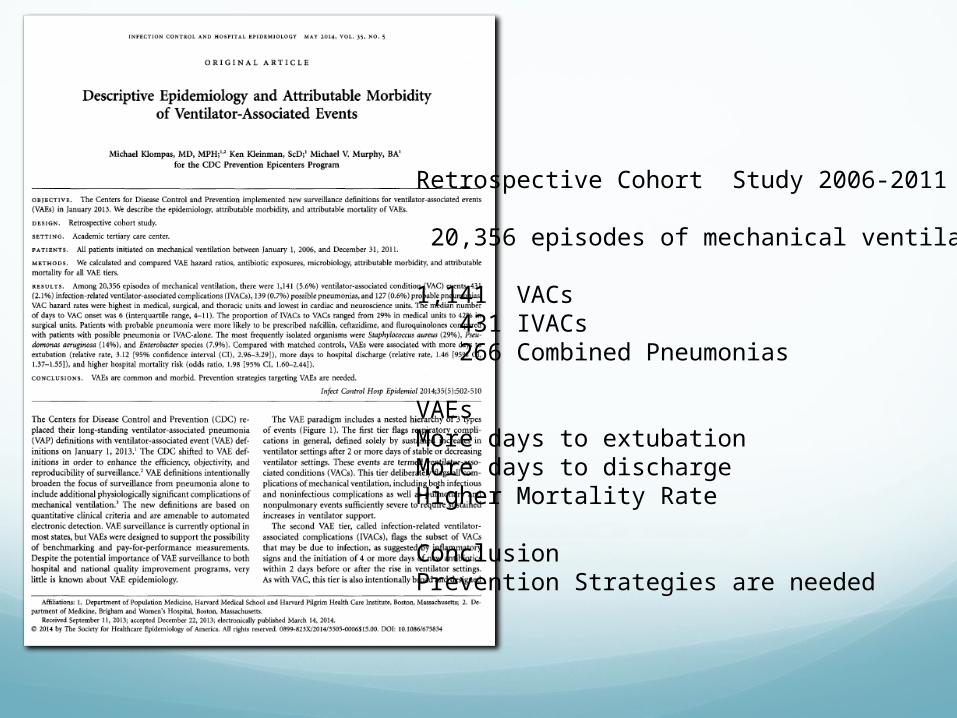
Retrospective Cohort Study 2006-2011
20,356 episodes of mechanical ventilation
1,141 VACs 431 IVACs 266 Combined Pneumonias
VAEsMore days to extubationMore days to dischargeHigher Mortality Rate
ConclusionPrevention Strategies are needed
.
Magill et.al 2014 ID Week : approximately 79% of VAEs were in patients who were either on MV for ≥5 days or in the hospital for ≥5 days at the time of VAE onset.
Conclusion: Characteristics of patients with VAEs in 2013 differ from those with tVAP in 2012. Time to onset data suggest that the majority of VAEs are likely hospital-associated.
Is VAC Preventable ?

What Else do we Know About VAE Prevention?
.
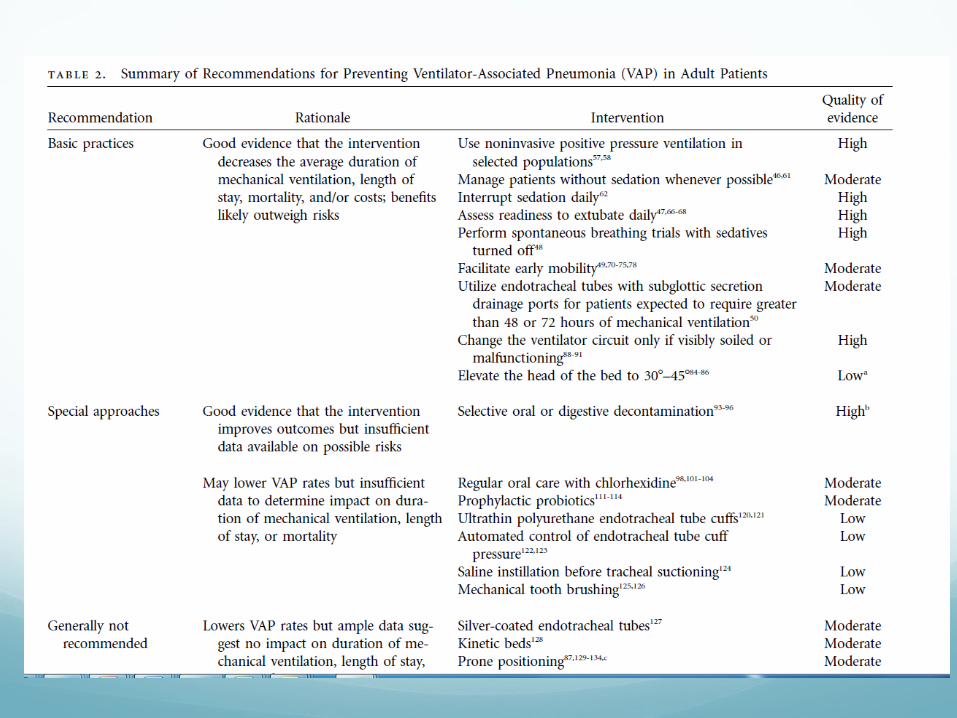
The existing VAP prevention literature is the best available guide to improving outcomes for ventilated patients.
VAP interventions that have been shown to improve objective outcomes, such as duration of mechanical ventilation, intensive care or hospital length of stay, mortality, and/or costs in randomized controlled trials.
Getting Started
Where to Start ?
1. Look at both process and outcome measures
2. Do we see improvements?
3. Important to track you own performance over
time
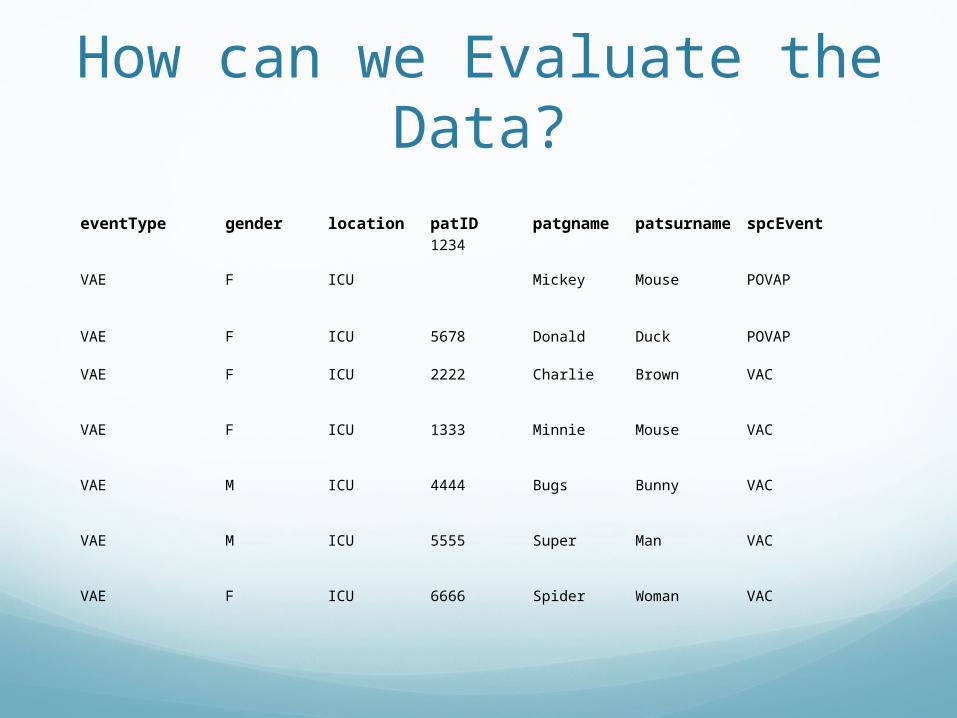
How can we Evaluate the Data?
eventType gender location patID patgname patsurname spcEvent
VAE F ICU
1234
Mickey Mouse POVAP
VAE F ICU 5678 Donald Duck POVAP
VAE F ICU 2222 Charlie Brown VAC
VAE F ICU 1333 Minnie Mouse VAC
VAE M ICU 4444 Bugs Bunny VAC
VAE M ICU 5555 Super Man VAC
VAE F ICU 6666 Spider Woman VAC
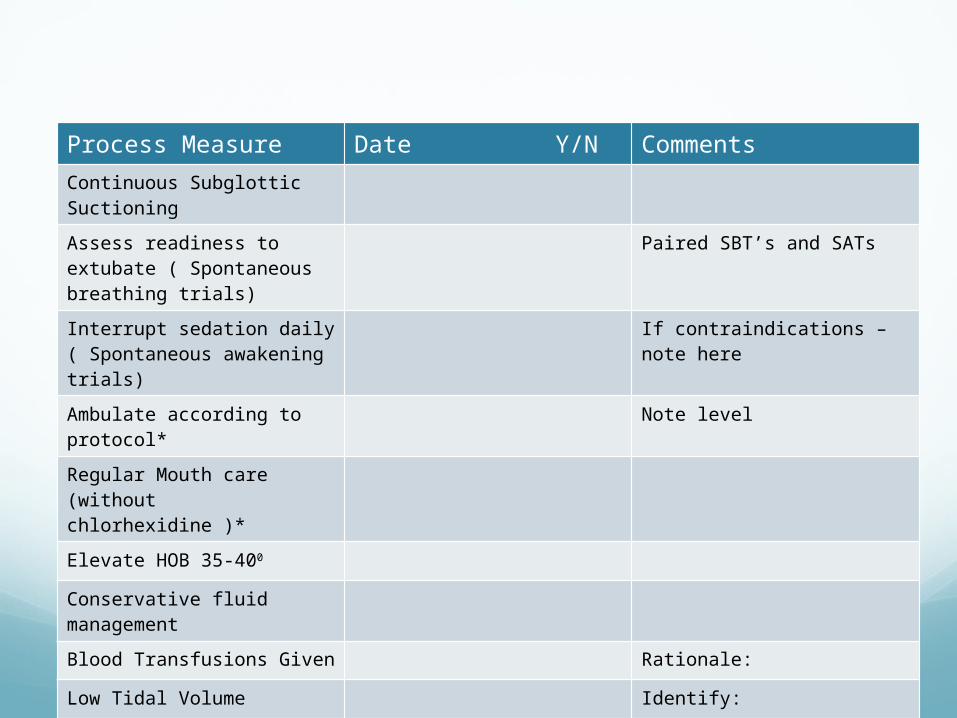
Bundle Process Measure Date Y/N CommentsContinuous Subglottic Suctioning
Assess readiness to extubate ( Spontaneous breathing trials)
Paired SBT’s and SATs
Interrupt sedation daily( Spontaneous awakening trials)
If contraindications – note here
Ambulate according to protocol*
Note level
Regular Mouth care (without chlorhexidine )*
Elevate HOB 35-400
Conservative fluid management
Blood Transfusions Given Rationale:
Low Tidal Volume Identify:
What about Oral Care?
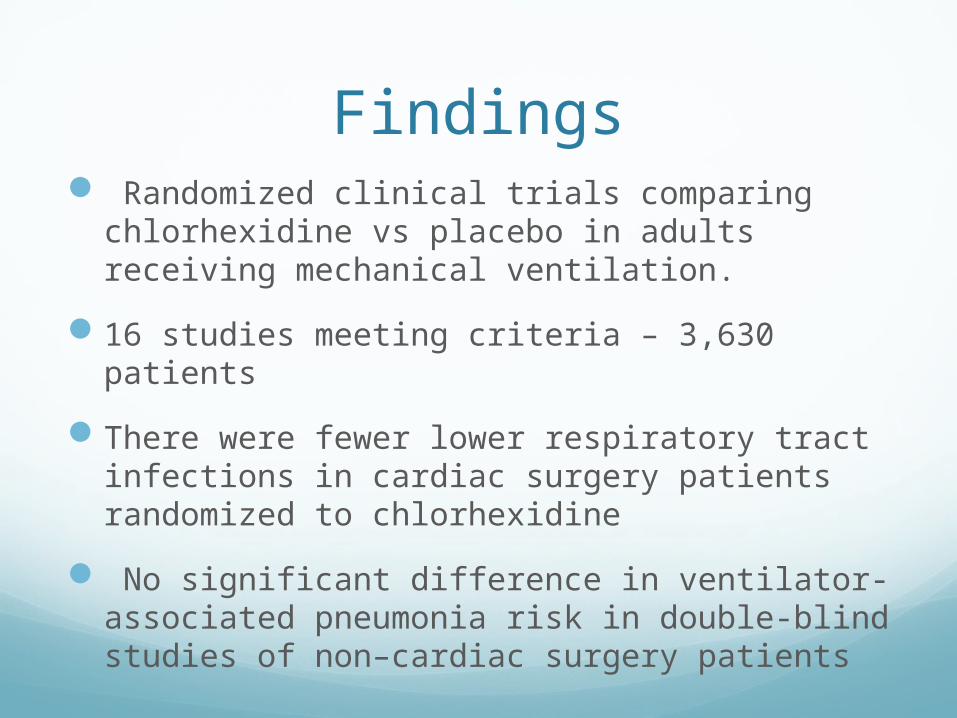
Findings Randomized clinical trials comparing
chlorhexidine vs placebo in adults receiving mechanical ventilation.
16 studies meeting criteria – 3,630 patients
There were fewer lower respiratory tract infections in cardiac surgery patients randomized to chlorhexidine
No significant difference in ventilator-associated pneumonia risk in double-blind studies of non–cardiac surgery patients
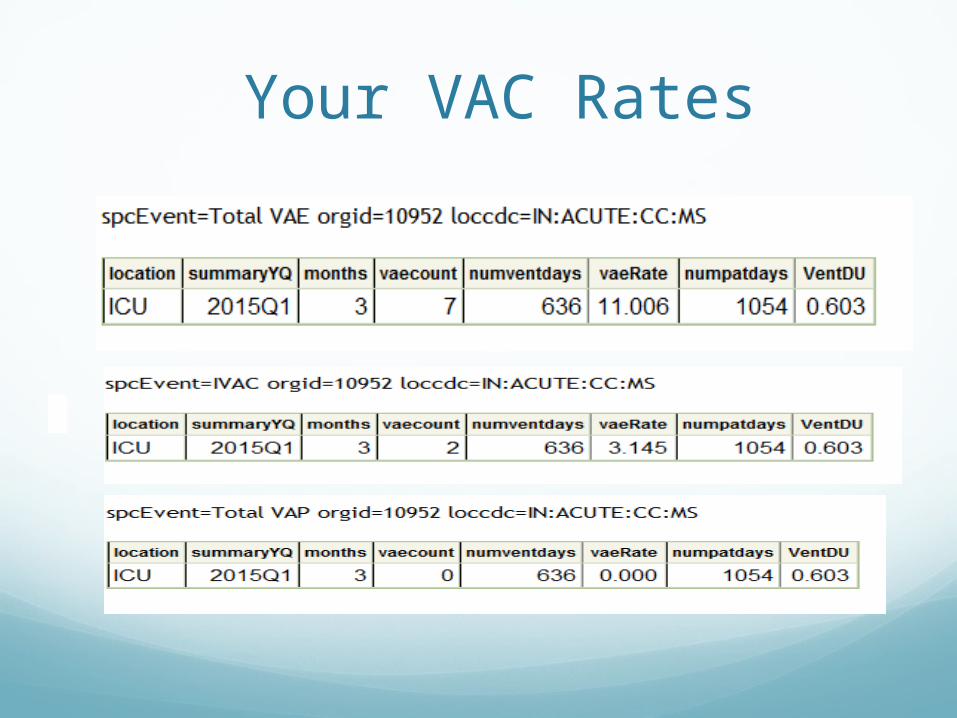
Your VAC Rates
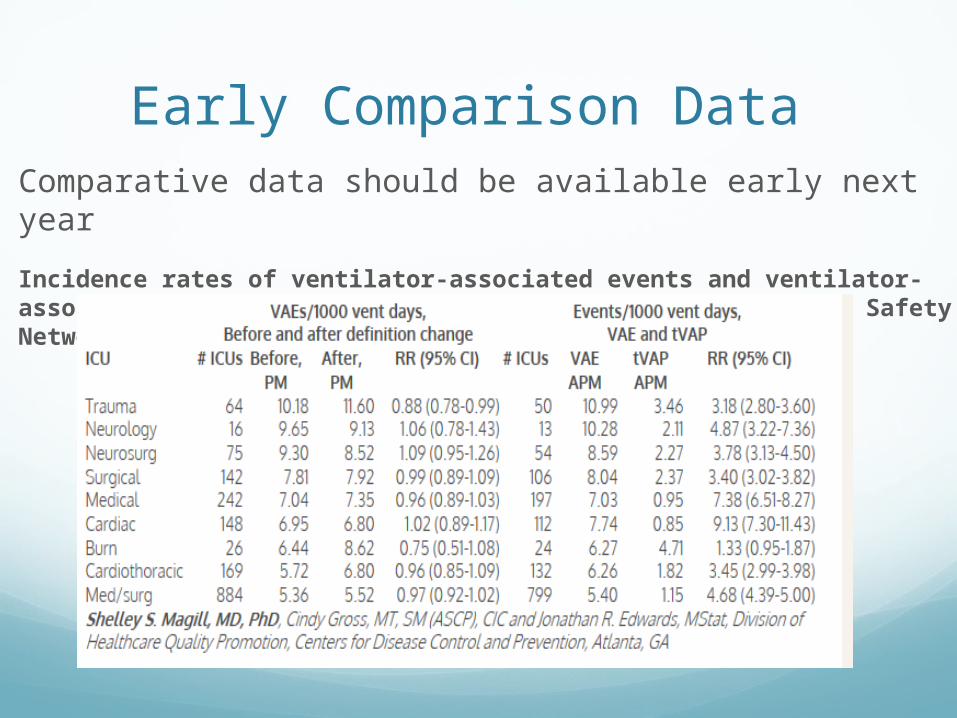
Early Comparison DataComparative data should be available early next year
Incidence rates of ventilator-associated events and ventilator-associated pneumonia in the National Healthcare Safety Network, 2012-2013
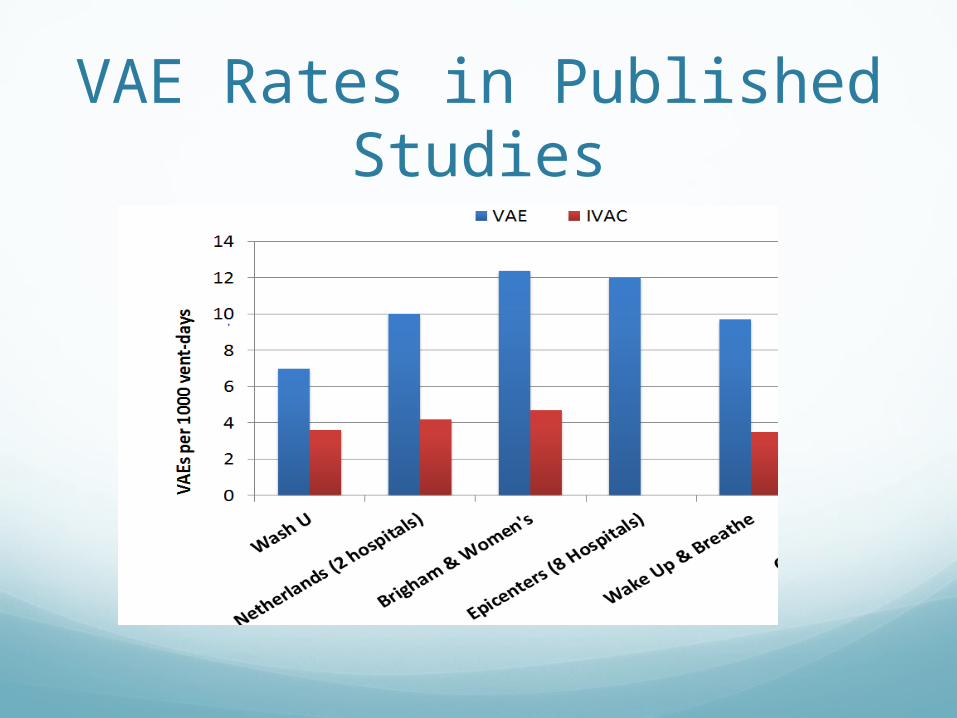
VAE Rates in Published Studies
How will I use my data to drive improvement?
Review both individual cases and system level issues
Do we have policies and procedures in place ?
Do we follow evidence based guidelines?
Are we consistent with our practices?
Reviewing Cases
Patient who develops a VAC
Chronic vent
Ambulation protocols not implemented
Dehydrated
Sputum not documented
Nursing and respiratory not communicating
Opportunities
• Hardwire ambulation protocols
• Ensure documentation of secretions
• Work collaboratively with respiratory therapy to identify subtle changes
• Daily huddle
28
Another Case Mrs. X is a 76 y.o. woman admitted to the ICU with septic shock requiring large volume fluid resuscitation.
She is intubated and placed on the ventilator
She is stable on the ventilator until day 6 when she has
progressing oxygenation demands
She has developed a VAC
Case evaluationNo fever
No increased white count
No new antibiotics
Diagnosis: Pulmonary Edema
Opportunities for improvement ?

Another oneIn another ICU, a large proportion of VAC’s are possible or probable pneumonia
Evaluation:
HOB monitoring?
Suctioning frequency?
SATs?
ET tubes with Subglottic suctioning?

Analysis of Data
The team analyzes their data
During the first quarter they had 20 VAC’s
16 of these meet criteria for IVAC
They recognize that the usual ratio for ICU’s is 1/3 to 1/2
IVAC Analysis Not PVAPS
Most are other HAIs
Considerations?
Prevention Thoughts
Prevention of Pneumonia- HOB
Pulmonary- fluid conservation
Atelectasis – manage sedation
Acute lung injury-low tidal volume
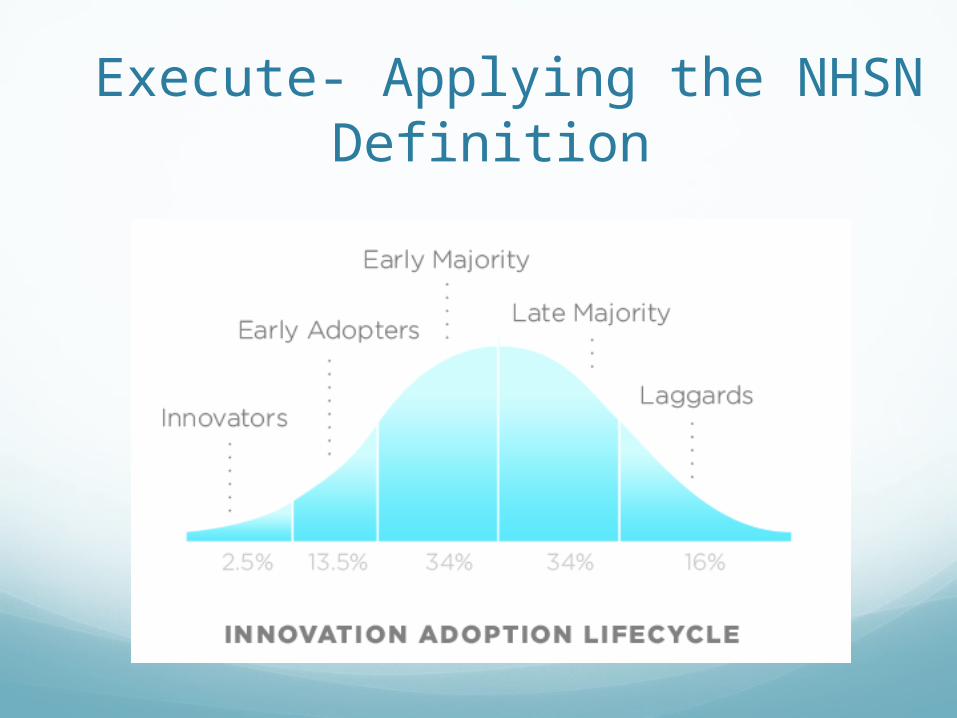
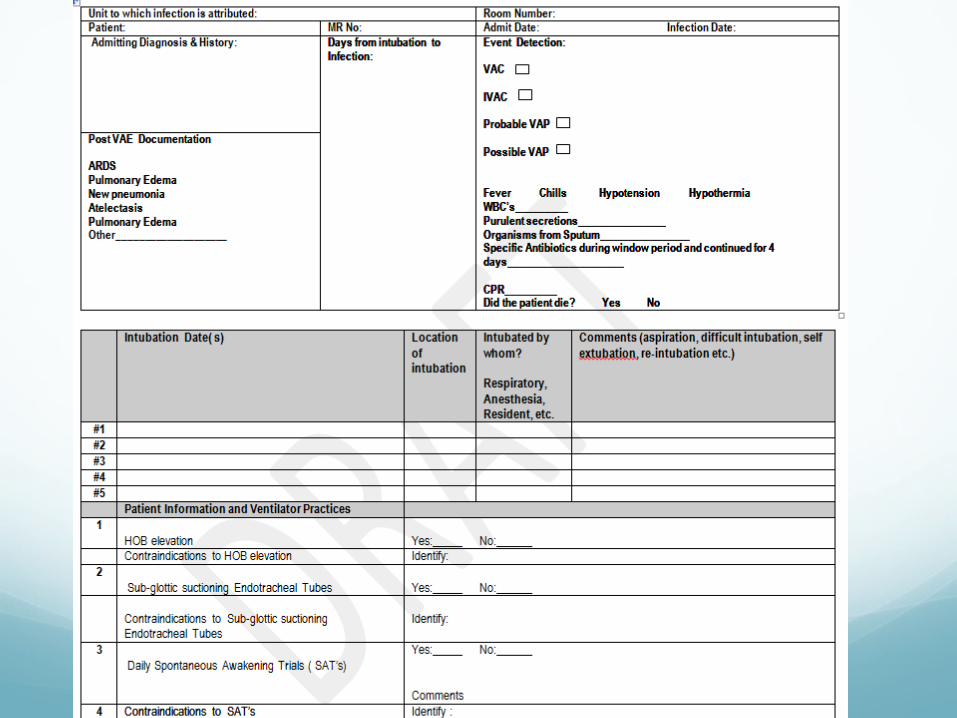
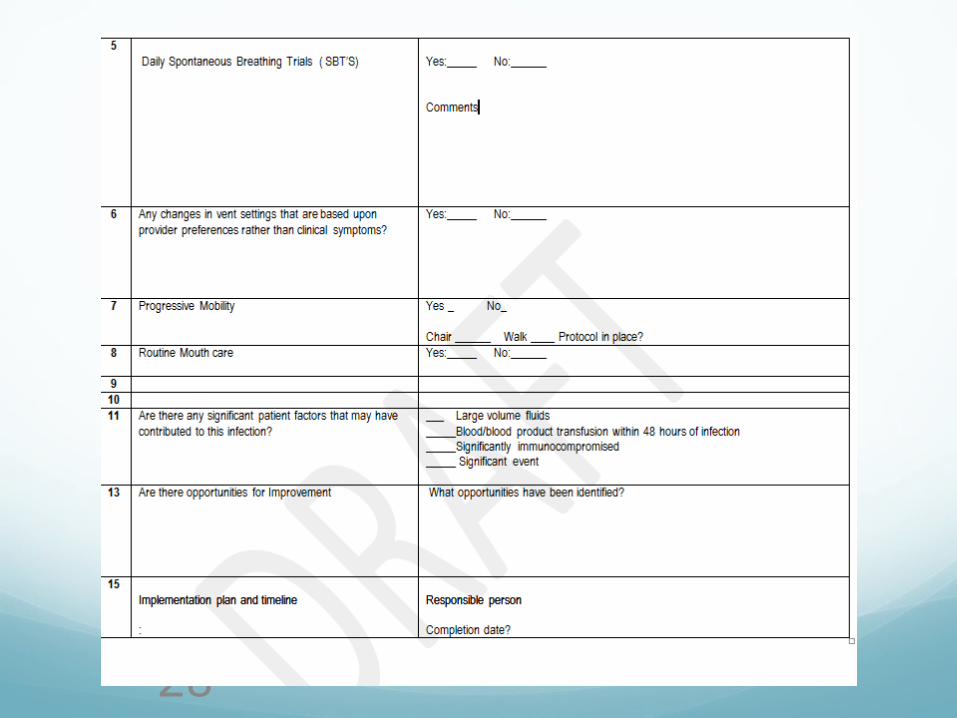
Execute- Applying the NHSN Definition
“If we could change ourselves, the tendencies in the world would also change. As a man changes his own nature, so does the attitude of the world change towards him. … We
need not wait to see what others do”
-Gandhi
36
Know your Data
Surveillance is a critical component of every quality improvement effort; you cannot prevent it if you cannot measure it.

The Bottom Line
VAE associated with mortality and LOS (my experience supports this)
Continue to monitor processes of care and outcomes
Give feedback to providers and assess potential for preventable events