linehan.pdf · studies the dynamics of a medical condition in ... european brain council, ......
TRANSCRIPT
Epidemiology (1)
• "The study of the distribution and determinants of health-related states or events in specified populations and the application of this study to control health problems."
• “Epidemiology is the medical discipline which studies the dynamics of a medical condition in the general population. It is concerned about the numbers of people with the condition who are at risk and what is the outcome of the condition. It allows for the rational planning of health delivery”.
SEIN (WHO Collaborating Centre for Research, Training and Treatment in Epilepsy), WHO Headquarters, and the ILAE/IBE/WHO Global Campaign Against Epilepsy. (2010). Epilepsy in the WHO European region: Fostering epilepsy care in Europe
Epidemiology (2)
• “Recently, psychosocial and economic indicators such as quality of life and standards of care, have been incorporated into epidemiological research, as their relationship to morbidity becomes evident”.
Epidemiology (3)
Epidemiology (2003) Epilepsia, 44 (Suppl 6) 17-18.

What’s epidemiology ever done for epilepsy?
• 1st epidemiological study examining population-based data from Rochester.
• Studies “are not necessarily representative of a population from which the patients are drawn”.
• Challenged the prevailing view of epilepsy as a rare and unremitting condition.
What Epidemiology tells us about Prognosis
• Rochester study (1935-1984) reported the probability of being in remission 5 years at 20 years after diagnosis was 75%.
• National General Practice Study of Epilepsy (UK) 68% in 5 year remission at 7 years after diagnosis.
• Outcome of (treated) epilepsy strongly reflects syndromic classification and underlying aetiology.

Current Applications of Epidemiology
• Frequency counts are useful to highlight healthcare needs, identify co-morbidities, determine impact, plan services and justify expenditure.
• Epidemiological research can identify risk factors, outline prognosis, and assess treatment options.
• Studies examining aetiology can contribute to a range of endeavours from public health initiatives
to genetic investigations.

Epidemiological Research
• Descriptive – the ‘vital statistics’ of a condition that is usually based on observation.
• Analytical – establishes associations and determinants of condition usually by case control studies.
• Experimental – relevant factors are controlled by the investigator (underdeveloped in epilepsy).
Sander, J.W., (2003) The epidemiology of epilepsy revisited. Current Opinion in Neurology, 16, 165-170.
Defining Epilepsy
• The widely accepted operational definition of epilepsy requires that an individual have at least two unprovoked seizures on separate days, generally 24 hours apart.
• Typically exclude single unprovoked seizure or two or more unprovoked seizures within a 24-hour period from epidemiological studies.

Defining Epilepsy
• Epilepsy is a disorder of the brain characterised by an enduring predisposition to generate epileptic seizures and by the neurobiologic, cognitive, psychological and social consequences of this condition. The definition of epilepsy requires the presence of at least one epileptic seizure.
“Epidemiologists require operational case definitions... We advise that epilepsy be defined in
practice as two or more unprovoked seizures occuring at least 24 hours apart”.


Global Impact: Prevalence
• Oft cited prevalence estimate of 50 million people with epilepsy worldwide.
• National experts from 160 countries (97.5%).
• “The key persons were among the most knowledgeable persons in their countries, but the possibility remains of the data being incomplete and in certain areas even inaccurate.”
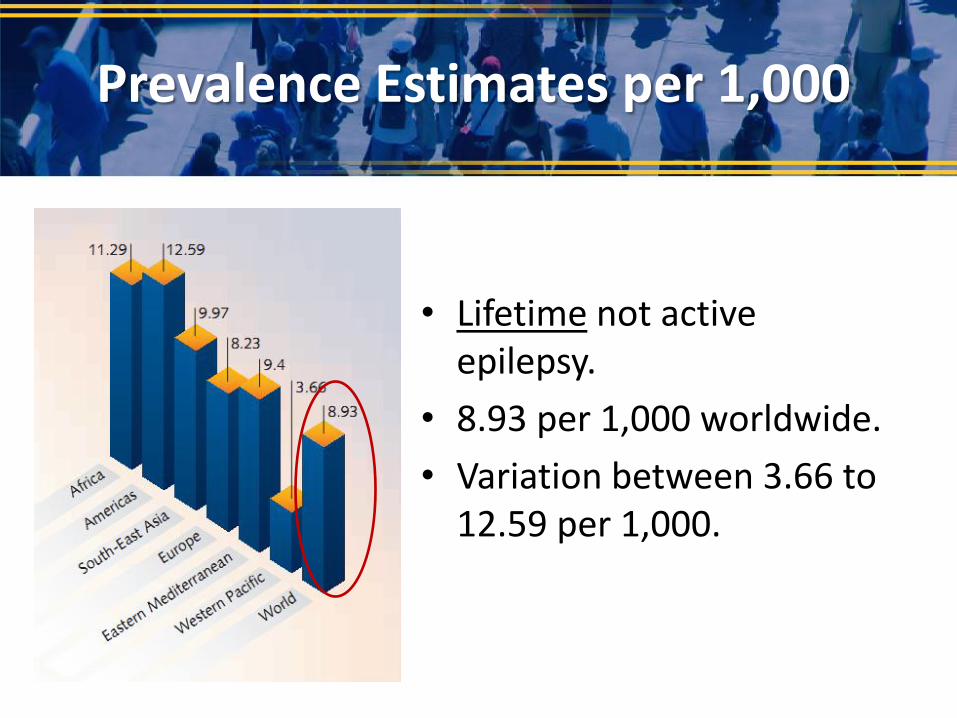
• Lifetime not active epilepsy.
• 8.93 per 1,000 worldwide.
• Variation between 3.66 to 12.59 per 1,000.
Prevalence Estimates per 1,000
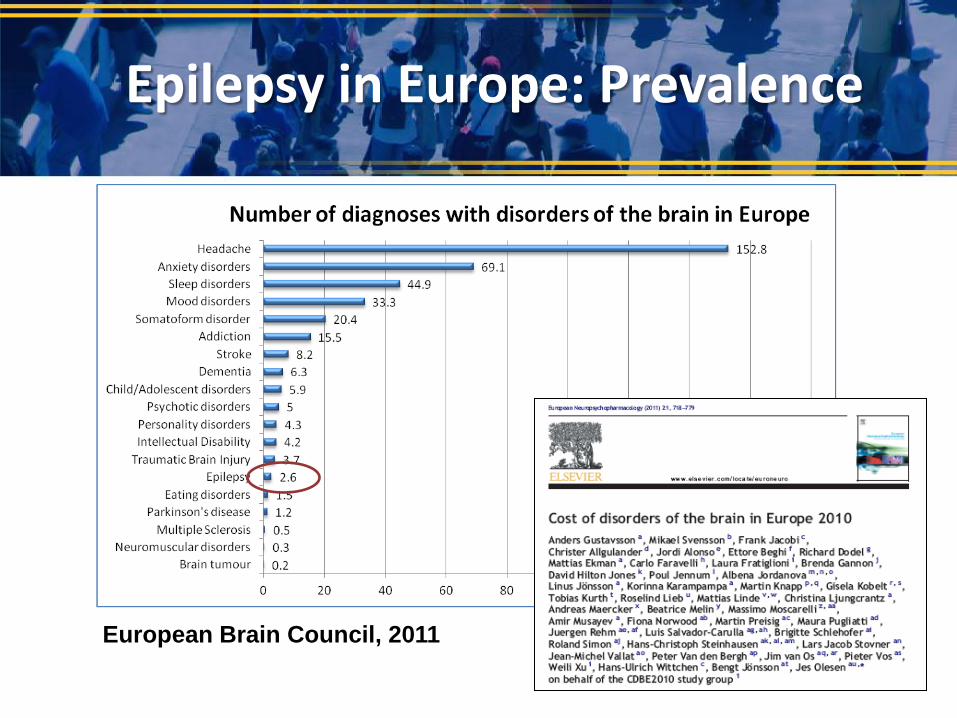
Epilepsy in Europe: Prevalence
European Brain Council, 2011

Median Lifetime Epilepsy
(5th–95th percentile range)
Median Active Epilepsy
(5th–95th percentile range)
Developing rural
areas
15.4 per 1,000
(4.8–49.6)
45 million (14–145) 12.7 per 1,000
(3.5–45.4)
17 million (5-61)
Developing urban
areas
10.3 per 1,000
(2.8–37.7)
17 million (10-133) 5.9 per 1,000 (3.4–
10.2)
10 million (5-17)
Developed 5.8 per 1,000 (2.7–
12.4)
6.8 million (3.2–14.7) 4.9 per 1,000 (2.3–
10.3)
5.7 million (2.7–12.2)
69 million 33 million
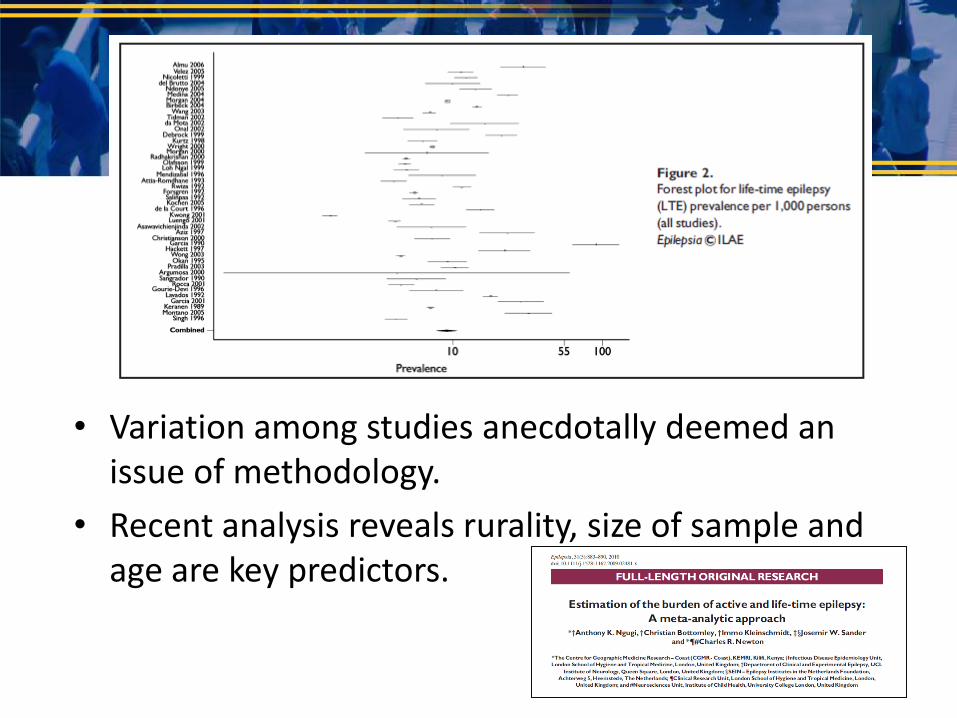
• Variation among studies anecdotally deemed an issue of methodology.
• Recent analysis reveals rurality, size of sample and age are key predictors.

The Treatment Gap
• The proportion of people with epilepsy who have active epilepsy but who are not taking AEDs or are inadequately treated.
• Ranges 25%-100% in low income countries compared with 10% in high.
• Inadequate skilled manpower, cost of treatment, unavailability of drugs, cultural beliefs, use of
traditional medicine, distance from healthcare.
Aetiology in Developing Countries
• Head injury – (traffic, work related injury)
• Brain tumour
• Cerebrovascular disease
• Febrile seizures (malaria)
• Viral infection (measles and HIV)
• Bacterial meningitis
• Fungal disease
• Parasites (neurocysticercosis)
Prevalence vs Incidence
“Since mortality is high in the early course of epilepsy and spontaneous remission may occur, prevalence figures may significantly underestimate the burden of epilepsy”

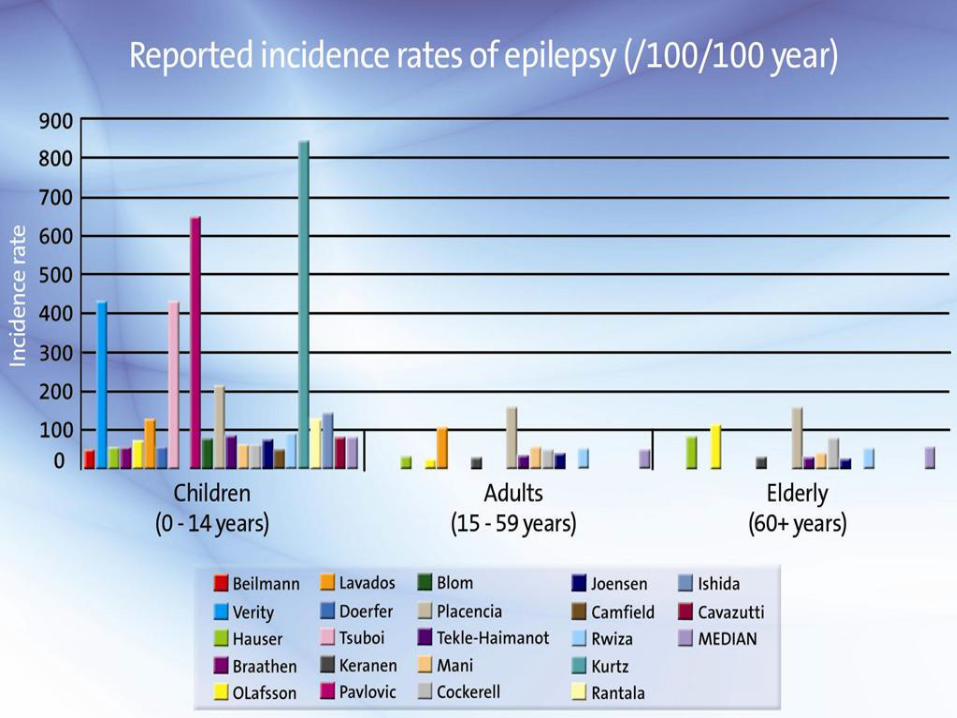
Global Impact: Incidence
• Incidence – the number of new cases in a standard size population per unit of time – e.g. Number of cases per 100,000 population per year.
• Typically 40-70 and 63-158 per 100,000 in developed and developing countries.
• Studies are very expensive, recommended that they are prospective.
Sander, J.W., (2003). The epidemiology of epilepsy revisited. Current Opinion in Neurology. 16, 165-170
Sander, JW & Shorvon, SD, (1996) Epidemiology of the epilepsies. Journal Neurol Neurosurg Psychiatry, 61:433-43
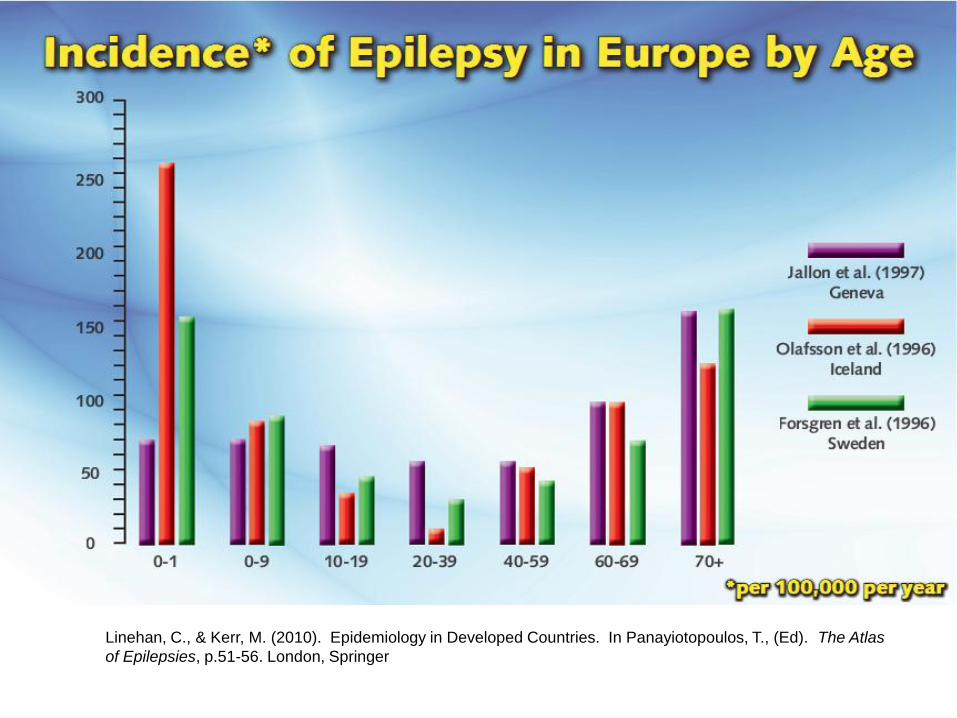
Linehan, C., & Kerr, M. (2010). Epidemiology in Developed Countries. In Panayiotopoulos, T., (Ed). The Atlas
of Epilepsies, p.51-56. London, Springer

A note of caution: Misdiagnosis & Case Ascertainment


Economic Impact
• Relatively recent area of study– 1993
– 20th International Epilepsy Congress in Oslo
• Four phases of research areas have evolved:
– Cost of epilepsy (direct, indirect, intangible costs)
– Cost benefit (cost effectiveness of alternative treatments)
– Cost effectiveness of structural programmes (e.g. decentralise outpatient clinics?)
– Comparing health care systems (ILAE Commission on Health Care Policy)

Economic Impact
• ‘Societal perspective’ approach most typical in epilepsy which examines all costs, irrespective of who incurs cost.
• Examine costs in the following areas:
– Direct healthcare costs (e.g. diagnosis, treatment)
– Direct non-medical (e.g. other related goods, accommodations, may include informal care)
– Indirect costs (value of lost output – employment)
– Intangible (pain, etc. Valued as DALYS or lost QALYs)

Economic Impact
• Top down
– national level costs for disorders are divided up by disorder.
• Bottom up
– Cost data gathered per patient extrapolated to national level using prevalence data.
– Prevalence data typically over 12 months.
Total cost of epilepsy
= cost per patient X number of patients

Economic Impact in Europe
(1) >20 billion euro/year (2) 15.5 billion euro/year (3) 13.8 billion euro/year

Cost per person Cost per disorder
Economic Impact in Europe

Economic Impact in Europe
• Breakdown of €13.8 billion per annum:
–€5,644 bn = Indirect costs (lost productivity)
– €1,653 bn = Direct non-medical costs
– €6,503 bn = Direct healthcare costs
• Average cost per person per annum:
• €5,221 (€1,291 Bulgaria - €10,246 Germany)
Cost of Care in Developing Countries
• Average cost to provide care to person with epilepsy in a developing country:
= <$25 per person, per year.
Mortality
• Mortality data -142,000 people die annually of epilepsy.
• Equates to 0.2% of all deaths worldwide.

Cause of Death Both Sexes Males Females
Populations (millions) 000 % total 000 % total 000 % total
TOTAL DEATHS 58,772 100% 31,082 100% 27,690 100
Neuropsychiatric Disorders: 1,263 2.1% 647 2.1% 616 2.2%
Alzheimers, other dementias 492 0.8% 181 0.6% 312 1.1%
Epilepsy 142 0.2% 82 0.3% 60 0.2%
Parkinson’s disease 110 0.2% 58 0.2% 52 0.2%
Drug use disorders 91 0.2% 75 0.2% 16 0.1%
Alcohol use disorders 88 0.1% 75 0.2% 13 0.0%
Schizophrenia 30 0.1% 15 0.0% 14 0.1%
Unipolar depressive disorders 15 0.0% 7 0.0% 8 0.0%
Bipolar affective disorder 1 0.0% 0 0.0% 1 0.0%

Mortality
• Population-based incidence cohort studies with 7-29 years follow up reveal three fold increase in mortality compared to general population.
• Highest mortality risk among those with epilepsy since birth (intellectual disability, cerebral palsy) – underlying aetiology.
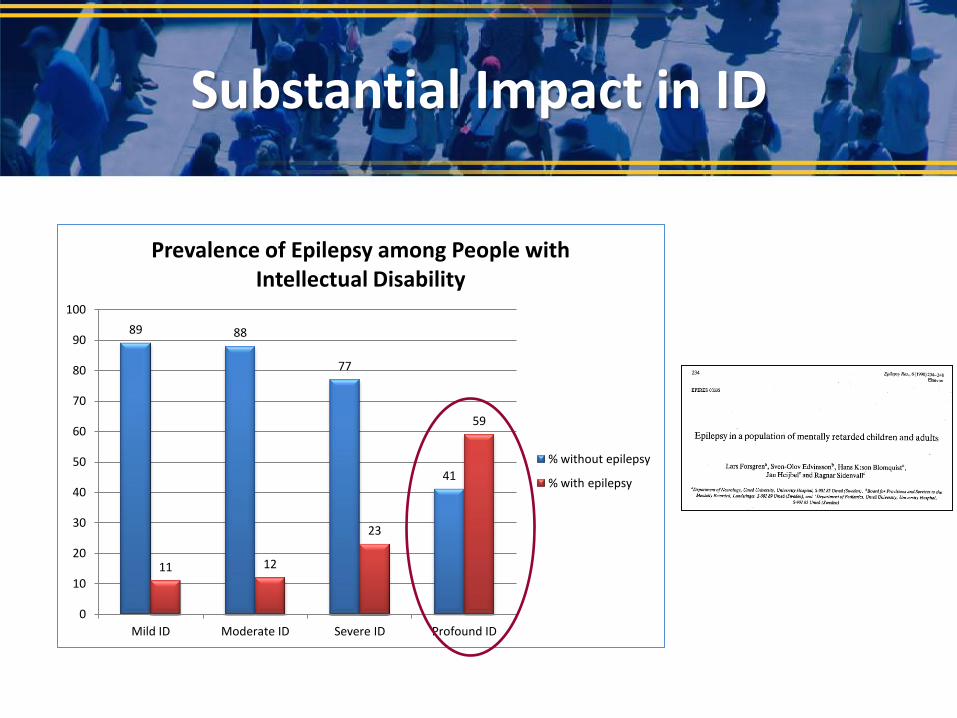
Substantial Impact in ID
89 88
77
41
11 12
23
59
0
10
20
30
40
50
60
70
80
90
100
Mild ID Moderate ID Severe ID Profound ID
Prevalence of Epilepsy among People with Intellectual Disability
% without epilepsy
% with epilepsy

Mortality: SUDEP
• SUDEP is the most common form of mortality directly related to epilepsy.
• Most common form of mortality among 20-40 yrs is SUDEP – 24 times higher than expected rate of sudden death in general population.
• Risk of SUDEP almost 40 times higher among those with poorly controlled seizures than those seizure free.

Disability Adjusted Life Years
• Mortality figures ‘mask the burden of epilepsy’.
• In 1990 GBD introduced a new metric of burden of disease, injuries & risk factors:
DALY (disability adjusted life year)
• One DALY = one year of healthy life lost due to disability or poor health.
• Epilepsy contributes 7,854,000 DALYS (0.5%) to the global burden of disease.
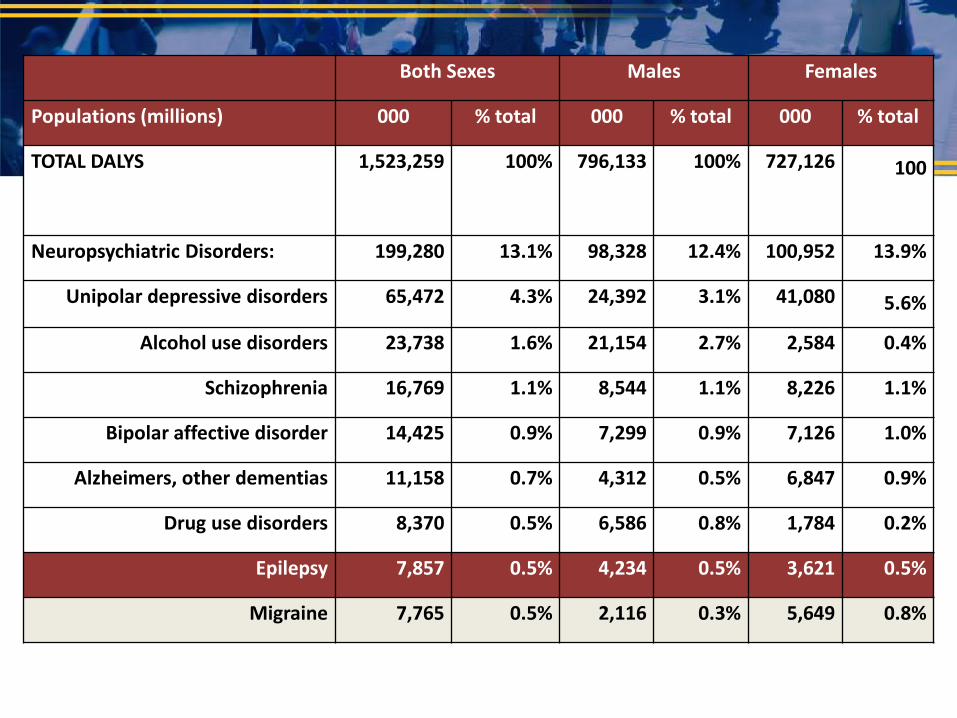
Both Sexes Males Females
Populations (millions) 000 % total 000 % total 000 % total
TOTAL DALYS 1,523,259 100% 796,133 100% 727,126 100
Neuropsychiatric Disorders: 199,280 13.1% 98,328 12.4% 100,952 13.9%
Unipolar depressive disorders 65,472 4.3% 24,392 3.1% 41,080 5.6%
Alcohol use disorders 23,738 1.6% 21,154 2.7% 2,584 0.4%
Schizophrenia 16,769 1.1% 8,544 1.1% 8,226 1.1%
Bipolar affective disorder 14,425 0.9% 7,299 0.9% 7,126 1.0%
Alzheimers, other dementias 11,158 0.7% 4,312 0.5% 6,847 0.9%
Drug use disorders 8,370 0.5% 6,586 0.8% 1,784 0.2%
Epilepsy 7,857 0.5% 4,234 0.5% 3,621 0.5%
Migraine 7,765 0.5% 2,116 0.3% 5,649 0.8%

Co-morbidities: Psychiatric
Prevalence ratios of comorbid disorders in all individuals, irrespective of age and gender
All individuals Rate ratio
Mental health disorders
Dementia 6.34
Organic Psychosis 6.05
Alcohol Dependence 5.70
Schizophrenia 4.13
Other Psychosis 3.98
Hysteria 3.92
Obsessive-compulsive disorder 2.57
Anxiety 1.99
Depression 1.98
Neurosis 1.90


Co-morbidities: Somatic
Prevalence ratios of comorbid disorders in all individuals, irrespective of age and gender
All individuals Rate ratio
Somatic disorders
Brain neoplasm 55.05
Meningiomas 31.44
Alzheimer's Disease 8.05
Cerebrovascular accident 6.96
Transient ischemic attack 4.94
Parkinson's Disease 3.19
Pneumonias 3.19
Fractures 2.17
Bi-directional Relationship
• Epidemiological research now examining if some co-morbidities may have a bi-directional relationship.
• Early onset developmental epilepsies carry a high risk of ASD.
• Speculation of an underlying mechanism linking the two conditions.
• Most, if not all of the association may be due to intellectual disability.

• Does the area represented by the question mark occur at a greater frequency than would be expected on the basis of ASD alone or epilepsy alone in the general population?
Bi-directional Relationship

• Bi-directional relationship between epilepsy and psychiatric disorder
• Increased risk of epilepsy in people with psychiatric disorders and increased risk of psychiatric disorders in people with epilepsy.
• Adelow et al., (2012) population-based study reported those who went on to develop epilepsy had higher rates of psychiatric admission prior to developing epilepsy.
Bi-directional Relationship
Berg, AT (2013). Epilepsy – clinical implications of recent advances. Lancet Neurology, 12, 1, 8-10.

Social Impact: Lifestyle Factors
• US Population-based self report surveys.
• National Health Interview Survey – N=30,445 adults over 18 years – 1.4% ‘had seizures’.
• Those with seizures vs no seizures reported:
– Lower levels of education
– Higher levels of unemployment
– Insufficient physical activity
– More physical co-morbidities

Social Impact: Life Satisfaction
• Theoretical concept – Goffman described as ‘deeply discrediting’ of individuals.
• ‘Felt’ and ‘enacted’ stigma – shame and discrimination.
• It's not just the seizures; it's living with epilepsy.
Social Impact: Stigma

Quality of Life and Seizure Control
• Growing body of literature suggesting those with infrequent or no seizures do not report diminished quality of life (Jacoby, 1992; Leidy et al., 1999; Stavem et al., 2000; Sander, 2005; Jacoby & Baker, 2008).


• 69 million people worldwide have epilepsy, 89% in developing countries.
•Treatment gap is substantial.
• Costs range 5,000 euro vs $25 per person.
•142,000 people die annual; epilepsy contributes 0.5% of DALYs to global burden.
•Co-morbidities common – bi-directional?
• Social impact and stigma are considerable.
Conclusions

“Better data from surveillance and research could improve epilepsy care and prevention”
“The stigma associated with epilepsy has to be eliminated”
To the future…
Thank you!