lipoprotein(a) as a cause of cardioborbobbvascular disease · lp(a) atherosclerotic stenosis...
TRANSCRIPT
Børge G Nordestgaard
Professor, Chief Physician, MD, DMSc
University of Copenhagen & Copenhagen University Hospital
Conflict of Interest Disclosure
Consultancies or talks sponsored by AstraZeneca, Merck, Omthera, Sanofi, Regeneron,
IONIS, Aegerion, Dezima, Fresenius, B Braun, Kaneka, Amgen, Denka Seiken, Kowa
Lipoprotein(a) as a Cause of
Cardioborbobbvascular Disease

HDL
LDL
Rem
nant
Lp(a)
HDL
LDL
Rem-
nant
”GOOD”
BAD
UGLY
Genetic Lp(a)
=innocent
TGs

Lipid Lipoprotein
HDL
Remnants
LDL
Lipoprotein
HDL cholesterol
Remnant cholesterol
LDL cholesterol
Triglycerides
Lipid
Lp(a)
Lp(a) total mass

Lp(a)
Atherosclerotic
stenosis
Myocardial
infarction
Aortic valve
stenosis
Clinical familial
hypercholesterolemia
25%
Lp(a)↑
KIV-2↓

Lp(a) developed twice in evolution

0 50 100 150 200Lp(a), mg/dL
0 50 100 150 200Lp(a), mg/dL
F
raction o
f P
opula
tion
Men Women
20% 20%
Low number of
Kringle IV-2
repeats
High number of
Kringle IV-2
repeats
Nordestgaard et al. EAS Consensus Panel. Eur Heart J 2010;31:2844-2853
80-90%
genetically
determined
Copenhagen General Population Study

Whites
Chinese
Japanese
Hispanics
Blacks
5 10 20 40
Uterman G 2001 &
Matthews KA et al. Am
Heart J 2005
Lipoprotein(a), mg/dL
Median (interquartile range)

Whom to screen for Lp(a)
• Premature CVD
• Familial hypercholesterolemia
• Family history premature CVD or Lp(a)
• Recurrent CVD despite statins
• ≥3% 10-year risk of fatal CVD
• ≥10% 10-year risk of fatal/nonfatal CHD
• Aortic valve calcification or stenosis?
Nordestgard et al. EAS Consensus Panel. Eur Heart J 2010;31:2844-2853 - updated
0 50 100 150 200Lp(a), mg/dL
0 50 100 150 200Lp(a), mg/dL
Fra
ctio
n of
Pop
ulat
ion
Men Women
20% 20%
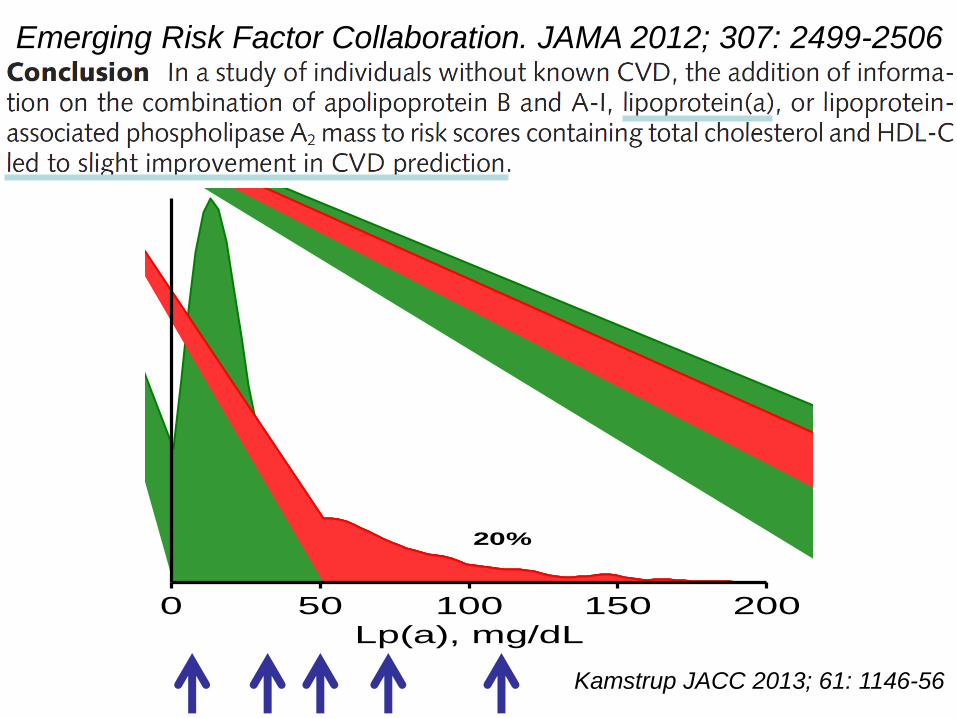
Kamstrup JACC 2013; 61: 1146-56
Emerging Risk Factor Collaboration. JAMA 2012; 307: 2499-2506

453 367 176 121 70 38 N
2% 3% 11% 16% 16% 23% NRI
Pia Kamstrup.
JACC 2013;
61: 1146-56
Myocardial infarction

0
50
100
150
Lip
opro
tein
(a)
CO
BA
S,
nm
ol/
L
0 20 40 60 80Lipoprotein(a) COBAS, mg/dL
R2 = 0.99. Lp(a), nmol/L = 2.14 * lp(a), mg/dL – 3.15
104 nmol/L
50 mg/dL
Nordestgaard,
Kamstrup &
Langsted 2016
Lp(a) nmol/L vs. Lp(a) mg/dL
Denka Seiken assay on Roche COBAS
Lp(a) ≤70 mg/dL N=2157

apolipo-
protein(a)
LDL-like
particle
Koschinsky et al. Cur Opin Lipidol 2004;15:167-174
Kringle IV-2
copy
number
variant:
2 to >40
repeats
Danish
kringle
Lipoprotein(a)

Randomization methods
Placebo Drug: lipoprotein
levels or
Cardiovascular disease or
Confounders
evenly distributed
Random distribution of alleles
Confounders
evenly distributed
Cardiovascular disease or
Normal
allele
Allele: lipoprotein
levels or
Reverse causationNordestgaard 2015
Randomized trial vs. Mendelian randomization

Lipoprotein Cardiovascular
Disease Risk
Genotype
established but causal?
effect size?
pleiotropic effects?statistical power?
1
2 3
Causality: Instrumental Variable Analysis
Mendelian randomization hypotheses

Lp(a)Lp(a)↑
Atherosclerotic
stenosis
Myocardial
infarction
Aortic
stenosis
KIV-2↓
LDL
Apo(a)
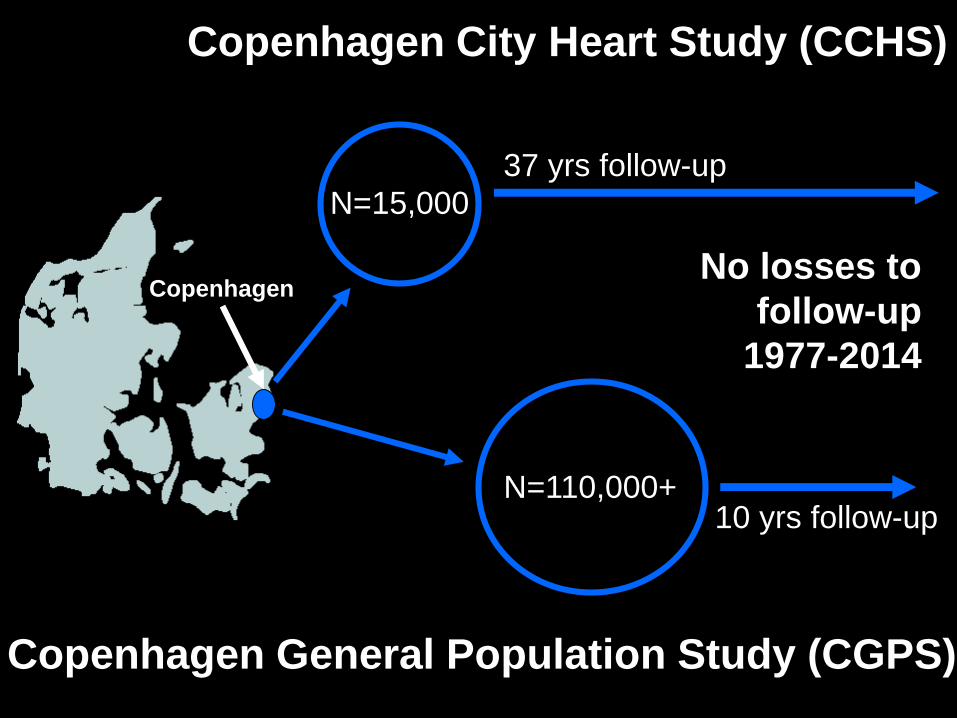
Copenhagen General Population Study (CGPS)
N=15,000
N=110,000+
37 yrs follow-up
10 yrs follow-up
No losses to
follow-up
1977-2014
Copenhagen
Copenhagen City Heart Study (CCHS)

1
1.5
2
2.5
Haz
ard r
atio
(95%
CIs
)
0 50 100 150
Copenhagen General Population Study and
Copenhagen City Heart Study
N=58,340
1897 myocardial infarction (MI)
Emerging Risk Factor Collaboration
N=126,634
9336 MI + coronary death
1
1.5
2
2.5
Haz
ard
rat
io (
95
% C
Is)
0 50 100 150
Lipoprotein(a), mg/dL Lipoprotein(a), mg/dL
Nordestgaard & Langsted 2016
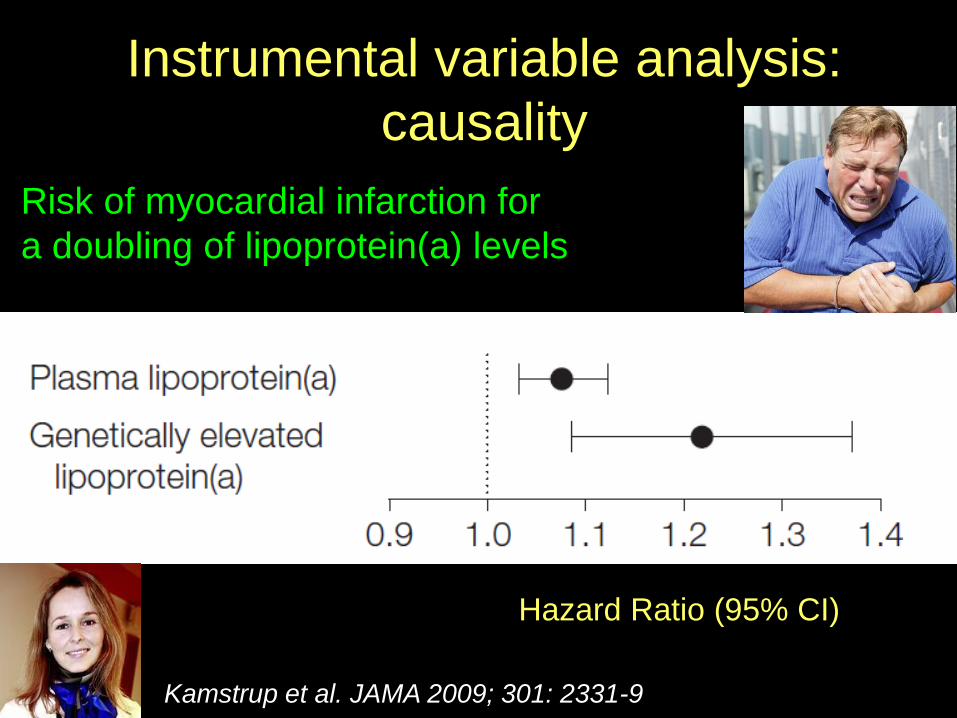
Instrumental variable analysis:
causality
Risk of myocardial infarction for
a doubling of lipoprotein(a) levels
Hazard Ratio (95% CI)
Kamstrup et al. JAMA 2009; 301: 2331-9

Lipoprotein(a) Myocardial
Infarction
KIV-2 genotype
1
2 3
Causal association
large effect size,
pleiotropic effects
unlikely
adequate statistical
power
GWAS
SNPs
Kamstrup et al. JAMA 2009; 301: 2331-9
Hypotheses

Consistency with custom-made
chip/GWAStudies
Schunkert et al. 2011
•confirmed association of LPA locus
with CAD in CAD case-control study
of 56 000 individuals
Clarke et al. 2009
Trégouët et al. 2009
•LPA locus strongest association with CAD
of 48 000 tested SNPs
•2 LPA SNPs explained 36% of p-lp(a)
variation and associated ↑ risk of CAD

Atherosclerosis
through ”LDL”
depositionAtherosclerotic
stenosis through
wound healing
Thrombosis
through
fibrinolysis
inhibition
Nordestgaard 2015

Lp(a) SNP
rs10455872
Thanassoulis NEJM 2013; 369: 503-512

Kamstrup, Tybjærg-Hansen, Nordestgaard JACC 2015; 63; 470-477
Copenhagen General Population Study
& Copenhagen City Heart Study
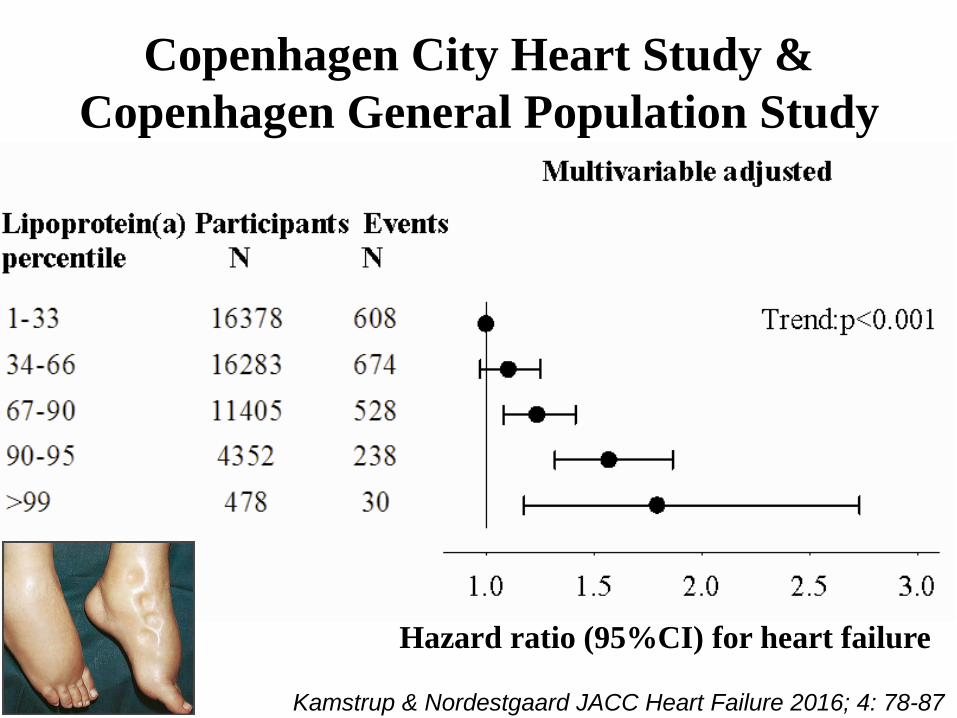
Kamstrup & Nordestgaard JACC Heart Failure 2016; 4: 78-87
Hazard ratio (95%CI) for heart failure
Copenhagen City Heart Study &
Copenhagen General Population Study

Heart
failure
63%
21%
47%Lp(a)↑
Myocardial
infarction
Aortic
stenosis
Both
Kamstrup & Nordestgaard JACC Heart Failure 2016; 4: 78-87
KIV-2↓
Mediation analysis (n=50,000)
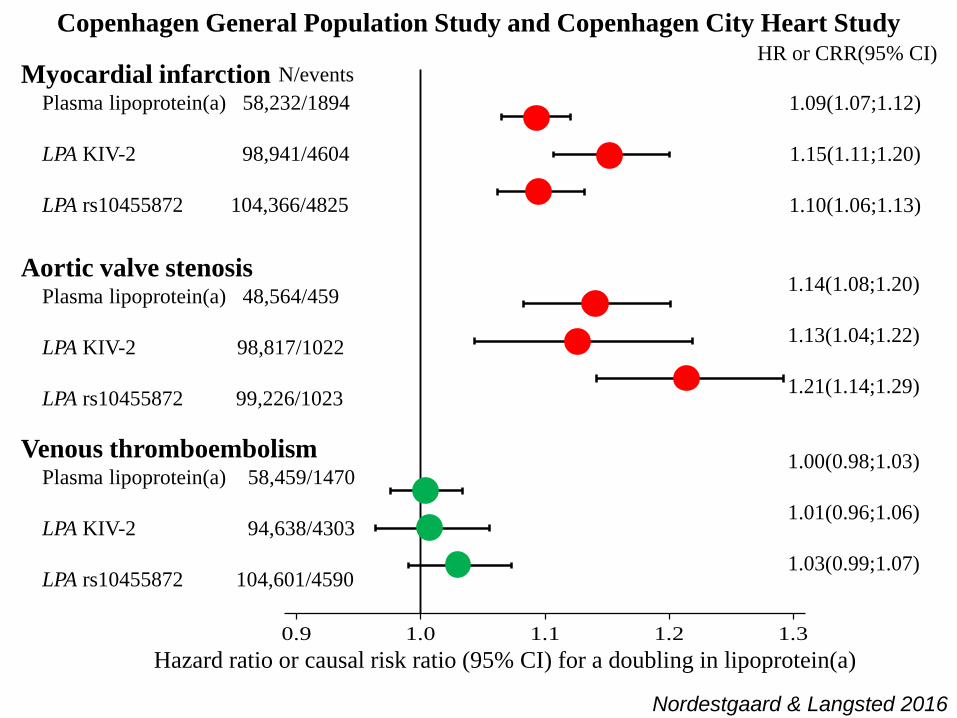
0.9 1.0 1.1 1.2 1.3
Hazard ratio or causal risk ratio (95% CI) for a doubling in lipoprotein(a)
Myocardial infarctionPlasma lipoprotein(a) 58,232/1894
LPA KIV-2 98,941/4604
LPA rs10455872 104,366/4825
Aortic valve stenosisPlasma lipoprotein(a) 48,564/459
LPA KIV-2 98,817/1022
LPA rs10455872 99,226/1023
Venous thromboembolismPlasma lipoprotein(a) 58,459/1470
LPA KIV-2 94,638/4303
LPA rs10455872 104,601/4590
HR or CRR(95% CI)
1.09(1.07;1.12)
1.15(1.11;1.20)
1.10(1.06;1.13)
1.14(1.08;1.20)
1.13(1.04;1.22)
1.21(1.14;1.29)
1.00(0.98;1.03)
1.01(0.96;1.06)
1.03(0.99;1.07)
N/events
Nordestgaard & Langsted 2016
Copenhagen General Population Study and Copenhagen City Heart Study

Lp(a)
Lp(a)↑
Aortic valve
stenosis
KIV-2↓
Atherosclerosis
through ”LDL”
deposition
Stenosis
through wound
healing
Thrombosis
through
fibrinolysis
inhibition
Atherosclerotic
stenosis
Myocardial
infarction

HDL
LDL
Rem-
nant
BAD
UGLY
Genetic Lp(a)
=innocent
TGs
FH
”GOOD”

Atherosclerosis
Myocardial
infarction
Angina
pectoris
Elevated LDL cholesterol
Mutations in LDL receptor,
apolipoproteinB or PCSK9
Liver with only 50%
functional LDL receptors
Coronary heart disease
Nordestgaard et al. Eur Heart J 2013; 34: 3478-3490
Heterozygous familial
hypercholesterolaemia

High lipoprotein(a) as a possible cause of clinical familial hypercholesterolaemia: a prospective cohort study
Langsted et al. 2016; Lancet DE; online May 12.
Raul D. Santos. 2016; Lancet DE; online May 12.

Langsted et al. 2016; Lancet DE; online May 12.

Langsted et al. 2016; Lancet DE; online May 12.
Copenhagen General Population Study by clinical FH

Langsted et al. 2016;
Lancet DE; online May 12.

0
0.2
0.4
0.6
0.8
Cu
mu
lati
ve i
nci
den
ce o
f m
yo
card
ial
infa
rcti
on
20 40 60 80 100
Age, years
Clinical Lp(a)
FH mg/dL
Yes >50
Yes ≥50
No ≥50
No <50
Clinical Familial Hypercholesterolemia:
DLCN, Simon Broome and/or MEDPED
Langsted et al. 2016; Lancet DE; in press.
Copenhagen General Population Study

Langsted et al. 2016; Lancet DE; online May 12.
Copenhagen General Population Study by clinical FH, n=46,200

Copenhagen
General
Population
Study
N=46,200
FH
1:200
Ranked causes
of clinical FH
1. LDLR
2. Lp(a) (25%)
3. APOB
4. PCSK9
Langsted, Kamstrup, Benn, Tybjærg-Hansen, Nordestgaard 2016; Lancet DE; online May 12.
High lipoprotein(a) as a possible
cause of clinical familial
hypercholesterolemia (FH)

Conc
lusio
n
Atherosclerotic
stenosis
Myocardial
infarction
Aortic valve
stenosis
Clinical familial
hypercholesterolemia
25%
Lp(a)↑
KIV-2↓