liver disease brenda beckett, pa-c. liver large, 4 lobes highly vascularized –nutrient-rich blood...
TRANSCRIPT
Liver Disease
Brenda Beckett, PA-C
Liver
Large, 4 lobes Highly vascularized
– Nutrient-rich blood from GI tract with products of digestion via portal vein
– Oxygen-rich blood via hepatic artery Metabolism, detoxification, storage,
excretion Ability to regenerate
Mechanisms of disease
Hepatocyte damage Biliary tract obstruction Metabolic disorders Metallic deposition Fibrotic changes Neoplasms
Symptoms of Liver Disease
May be asymptomatic until advanced– RUQ abdominal pain– Pruritis – bile salts deposited below skin– Fatigue– Weakness– Decreased libido– Nausea– Bleeding
Signs of Liver Disease
Gynecomastia
Diabetes
Testicular atrophy
Ataxia / Asterixis
Xanthomas, xanthelasmas
Jaundice (icterus)
Spider angiomata
Palmar erythema
Hepatosplenomegaly
Ascities / anasarca
Encephalopathy
Fetor hepaticus
Caput medusa
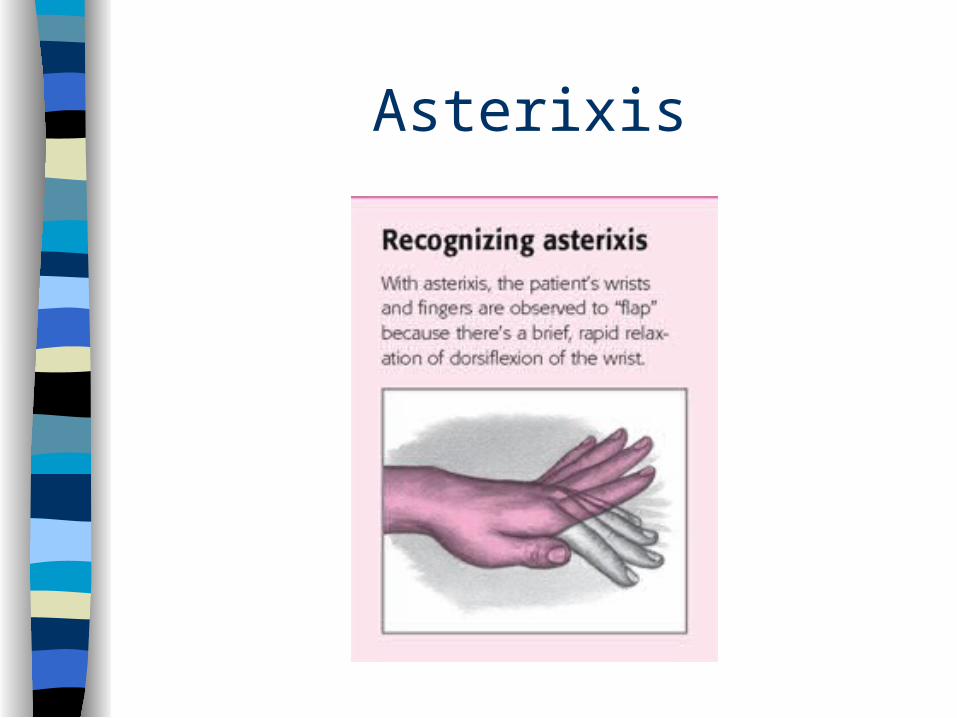
Asterixis
Assessing for Liver Disease
Typical patterns in lab tests Many patients with abnormal labs are
asymptomatic (need for screening)– Tests for hepatocellular damage– Tests for liver function
Hepatocellular Damage
Aminotransferases – AST, ALT– Present in hepatocytes. AST also in
cardiac muscle. Released with necrosis Alkaline phosphatase
– Isoenzymes in liver, bone, gut GGT
– Enzyme present in multiple tissues– Nonspecific. Will help to locate liver source
Tests for Liver Function
Prothrombin time - measures synthesis of factors II and VII
Albumin – plasma protein. Maintains oncotic pressure
Cholesterol – Not specific, many variables. May be decreased in end-stage disease
Bilirubin
Hemoglobin heme biliverdin unconjugated bilirubin.
Combines with albumin to liver. Conjugated and excreted as bile to
intestines Elevated in liver disease and hemolysis
Jaundice
Prehepatic - excess production Hepatic - impaired function (uptake
or conjugation) Posthepatic - obstruction
Jaundice
Unconjugated - (pre and hepatic) Excess production
– Hemolytic anemia, hemolysis Hepatic
– Causes• Hepatocellular disease, Gilbert’s,
neonatal jaundice
Jaundice
Conjugated (posthepatic) Causes
– Obstruction
– Hepatocellular disease
– Drugs
– Sepsis
– Post surgical
Jaundice Evaluation
History– Drugs – prescribed, otc, vit., herbs, etc– Transfusions, IVs, tattoos, IV rec drugs,
sexual activity– Recent travel, exposure to jaundiced,
alcohol intake– Duration, constitutional symptoms, fever,
weight loss, RUQ pain
Jaundice Evaluation
Physical– Nutrition, signs of chronic liver disease– JV distention, liver and spleen
enlargement,– Ascites, tender RUQ
Labs– Bilirubin, Conj and Unconj. Liver
enzymes
Other diagnostic tools
17
Ultrasound
Obstruction:– Biliary tract stones– Intrahepatic biliary dilation
Texture of liver (fatty vs. cirrhosis) Cystic/solid tumors
18
CT Scan
Characterize/quantify lesions Enhancement with contrast Smallest detectable lesion is 1cm
Obstruction
19
MRI
Best for:– Cystic lesions– Hemangiomas– Iron overload
20
PET Scan
Positron emission tomography FDG (Fluorodeoxyglucose) taken up by
active tissue and cancer cells Whole body scan Especially to rule out extrahepatic
disease in colon cancer patients
21
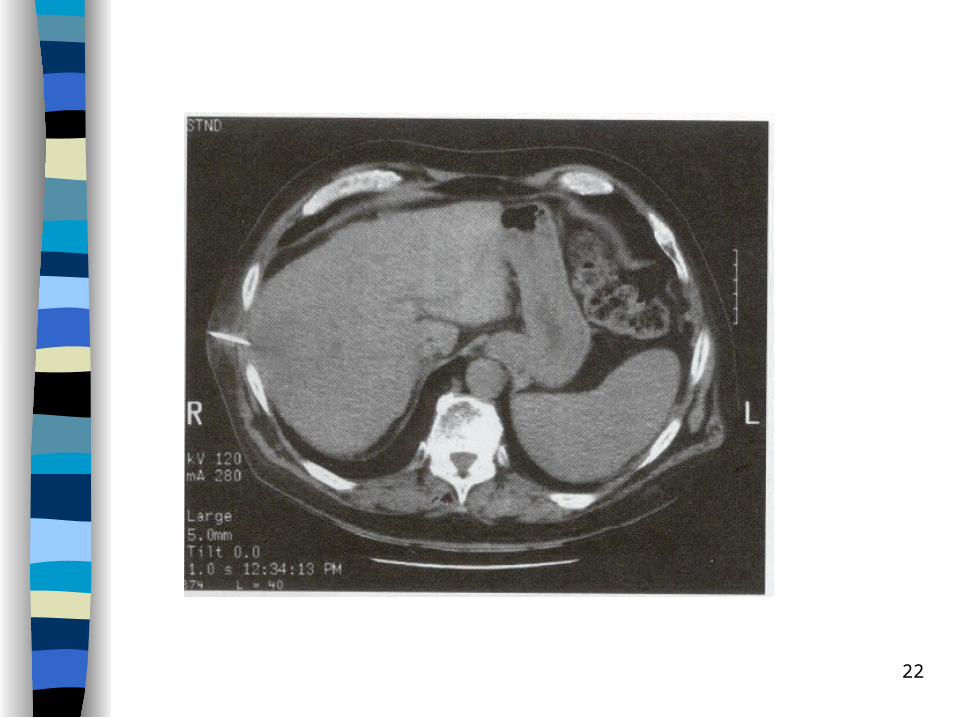
Percutaneous Biopsy
Can be safely done Use US or CT guidance Allows tissue diagnosis
22
Alcohol Related Liver Disease
Chronic alcohol intake can lead to fatty liver, hepatitis and finally, cirrhosis
Fatty liver and hepatitis (inflammation) are reversible, but are precursors to cirrhosis
Exact mechanism unknown, but partially due to toxicity and partially due to nutritional deficits
Alcohol Related Liver Disease
Mechanism not well understood mechanisms
– Direct toxicity to hepatocytes– Malnutrition– Immune reactivity after cell damage
– Inc risk of Hepatocellular Carcinoma (HCC)
Alcohol Induced Hepatotoxicity
Alcohol Dehydrogenase primary metabolic pathway– Present in gastric mucosa and liver– Women with less in stomach so more reaches liver
Fatty acid & triglyceride deposition 1st response • Fatty Liver or Steatohepatitis in 80%+ EtOH abusers• Usually reversible - may be due to obesity
EtOH metabolism products toxic to hepatocytes– Pathologic changes cause hepatitis
• Infiltrative PMNs• Inflammatory product cell changes• Fibrotic changes and cirrhosis• Partially reversible
Alcohol Related Liver Disease
Risk for EtOH disease fxn of quantity and duration of abuse– No correlation to type of beverage– Women develop ARLD with less intake
EtOH– 1 beer, 4 oz wine, 1 ounce whiskey has
about 12 g of EtOH• Inc risk with intake of >60-80 g EtOH daily for
10 years by men, >20-40 g daily by women
Alcohol Abuse
Patient may not admit to over-consumption
First clue may be liver failure/disease Use transaminase levels for clue, then
biopsy to definitively diagnose R/O other causes and comorbidities
– HBV, HCV, etc.
Cirrhosis Inflammation activates lipocytes
– Lose Vit A and form collagen Fibrotic bands form and replace normal
cellular architecture Lose compliance firm liver Results in liver function and Portal
Hypertension Treatment possible early in process
– Treat cause: EtOH, metals, infection, etc.
Causes of Cirrhosis Alcohol Viral hepatitis Biliary obstruction Veno-occlusive disease Hemochromatosis Wilson disease Autoimmune Drugs and toxins Metabolic diseases Idiopathic
Cirrhosis
Manifestations - determined by pathology
Scarring and disruption of architecture distorts vascular bed
Inadequate blood flow and ongoing damage disturbs hepatocyte function
Initially: fatty infiltration
Alcohol Related Liver Disease
Signs and symptoms:– Often asymptomatic until late.– Hepatomegaly– Anorexia, nausea– Jaundice– Abdominal pain, RUQ tenderness,
splenomegaly, ascites, fever, encephalopathy
Dx: ARLD Typical blood abnormalities: Incr GGT,
AST, ALT (AST>ALT), ALP, Bilirubin. Decr Albumin. Anemia. Prolonged PT
Liver biopsy to confirm– Large fatty droplets in fatty liver– Inflammatory changes in hepatitis– Fibrosis with nodular formation, Mallory
bodies, destruction of liver architecture in cirrhosis
DDX: ARLD
US and other imaging to r/o obstruction Hepatitis screening
NAFLD can be diagnosed AST/ALT ratio, BMI, MCV and gender
Trt: ARLD
Abstain from alcohol! Maintain adequate coloric intake Thiamine and folate supplements Cirrhosis: often hospitalization
– Low protein diet, monitor lytes, remove ascites, give clotting factors, lactulose to decrease nitrogen absorption from gut
Complications of Cirrhosis
Chronic Liver Failure Portal hypertension. Causes:
– Esophageal varices– Ascites– Encephalopathy
Hepatorenal syndrome Hepatopulmonary syndrome
Ascites - fluid in abdomen Total body water and sodium excess Cause unknown but 3 theories:
– Portal HTN causes sequestration fluid in splanchnic bed dec circulating blood volume
– Primary renal process causing retention H2O, Na+– Portal HTN causes release NO arterial
vasodilatation All cause RAA system activation, worsening
problem Dec albumin levels dec oncotic pressure to
hold fluid in vascular space
Ascites Anasarca less common form of same
pathophys Inc abdominal girth, weight Dyspnea as fluid restricts diaphragmatic
excursion Shifting dullness and US to confirm diagnosis Treat the root cause: fix the liver
– Na+ restrict 1500 mg/d– Spironolactone initially, add furosemide prn– Paracentesis (up to 4-6L)– Beware of spontaneous bacterial peritonitis
Other Complications
Hepatorenal syndrome: cause unknown– Azotemia, hypernatremia, oliguria in presence of
histologically normal kidneys• No urinary sediment indicating nephritis
– Dx by failure to resolve with hydration– No known treatment
Hepatopulmonary syndrome causes hypoxemia– Pulmonary hypertension and R-to-L intrapulmonary
shunts– Confused with co-morbid COPD
Hepatic Encephalopathy
Change in mental status in presence of liver disease– Spectrum from subtle personality changes to
confusion to coma
EEG changes noted Can cause coma and death Usually follows precipitating event:
– GI bleed, sepsis, electrolyte disturbance, shock, sudden inc dietary protein intake
Hepatic Encephalopathy
Pathophysiology unknown Theory: hepatocellular damage and cirrhosis
cause extrahepatic shunting of venous portal blood– Toxic substances not removed from blood
Increased serum ammonia level Treat with lactulose up to qid to cause
diarrhea (decr nitrogen absorption)
41
Portal Hypertension
Classified as:1) Sinusoidal: Alcoholic cirrhosis2) Presinusoidal: Splenic/portalvein
thrombosis, hepatitis, hepatic fibrosis3) Postsinusoidal: Vascular outflow
problem- Budd-Chiari syndrome:
Thrombosis of hepatic veins
Portal Hypertension
Signs: – Ascites– Caput medusa– Splenomegaly– Variceal bleeding– Encephalopathy
43
Management of Portal HTN
1) Medical: Ascities, encephalopathy, coagulopathy
2) Surgical: TIPS (Transjugular Intrahepatic Portosystemic Shunt), other shunting procedures
44
Acute Liver Failure
Acute massive loss of hepatocyte function
No pre-existing liver disease or portal HTN
Acetaminophen overdose, viral hepatitis, drug toxicity, herbal and dietary supplements
Acute Liver Failure
Extremely elevated transaminases Bilirubin may be normal Coagulopathies Increased ammonia
Acetaminophen overdose: treat with acetylcysteine
46
Acute Liver Failure
Can progress to fulminant hepatic failure with encephalopathy – Sepsis– Cerebral edema
High mortality rate– May need transplantation
No long term sequelae in survivors Uncommon
47
Benign Solid Liver Tumors
Hepatic Adenoma
- Reproductive age females on OCPs
- Sheets of hepatocytes with no parenchymal cells
- Risk of rupture and malignant transformation
48
Hepatic Adenoma
DX: Difficult to distinguish from FNH (Focal Nodular Hyperplasia)
- CT/MRI: to differentiate
Can rupture and bleed
49
Hepatic Adenoma
Management:
<4cm: cessation of OCPs, can regress
>4cm, no regression; resection
50
Malignant Tumors of Liver
Hepatocellular Carcinoma (HCC)
- Associated with cirrhosis, hepB, C
- Weight loss, weakness, abdominal pain, hepatomegaly, mass
DX: CT scan, perc. biopsy
- Will have elevated Alk Phos, AFP
51
HCC
Tx: surgical resection - difficult
Prognosis: Poor – depends on stage
4-6 months
5 year survival 25%
- Death due to cachexia, hepatic failure, mets, bleeding
52
Metastatic Lesions to Liver
- Most common neoplasm of liver- Reach liver by portal venous circulation, hepatic artery, direct extension or lymphatic spread- Colon, breast, lung, pancreas, stomach, others
53
Metastatic Lesions
DX: CT, labs, PET scan
TX: Resection of mets, segments, lobe
- Hepatic arterial infusion chemotherapeutic agents
- New: Portal vein embolization, radiofrequency ablation
54
Hepatic Resection
- Can remove up to 80%
- Albumin, synthetic capability by 3rd week
- Regeneration by hypertrophy of remaining tissues
Wilson Disease
Genetic disorder of copper metabolism Impaired biliary excretion of Cu Age 14-30, unless caught in screening Neuro Sx: tremor, ataxia, anxiety, MS Liver: cirrhosis, hepatitis Renal, cardiac involvement
Wilson Disease Dx
Inc transaminases Dec ceruloplasmin <20 mg/dl Inc urinary copper excretion >100
g/24h Inc liver copper deposition >250 g/g Kayser Fleischer rings

Kayser Fleischer rings
Wilson Disease Tx
Usually lifetime of chelating agents Penicillamine, trientine, zinc Liver transplant for fulminant liver failure Important to catch early
Hereditary Hemochromatosis Excess Fe absorption and deposition Caucasians, us. Northern European Early: fatigue, arthralgias, abd pain,
impotence Later: diabetes, hepatitis, cirrhosis,
cardiomyopathy– Usually age 40-60 depending on co-
morbidities Screening iron studies
HHC Dx
Sl. elevated transaminases Incr iron, Transferrin saturation >50% Serum ferritin elev but less specific Genotyping for C282Y and H63D
mutations Liver biopsy gold standard but not
necessary
HHC Tx is Phlebotomy To prevent irreversible end organ
damage Phlebotomy 500 cc weekly until mild
anemia and ferritin <50 ng/ml May take 2 years initially Maintenance: phlebotomy quarterly Can improve quality of life in patients
with liver disease May need transplant
Vascular Diseases
Acute ischemic injury due to shock, CHF Injury due to chronic congestion from right-
sided heart failure– Retrograde elevated venous pressure dilates
sinusoids– Poor perfusion results in ischemic injury, loss of
metabolic function– Centrilobar fibrosis and cirrhosis– Firm, large liver, other signs liver failure
Vascular Diseases
Budd-Chiari Syndrome– Occlusion of hepatic veins– Venous thrombosis
• Polycythemia Vera, hypercoagulable states, myeloproliferative diseases (cause hypercoagulable state)
– Mass or tumor– US or MRI to diagnose– Anticoagulate or TIPS
Granulomatous Liver Disease
Granuloma: Nodular inflammatory lesion
Usually asymptomatic Multiple causes
Granulomatous Liver Disease
Causes:– Drugs: Allopurinol, quinidine, quinine, etc– Infections: Bacterial, fungal, parasitic, viral– Cirrhosis– Systemic: Hodgkin’s, polymyalgia
rheumatica, connective tissue disorders, sarcoidosis
Granulomatous Liver Disease
DX:– Labs: elevated ALP, GGT– Imaging: US, CT, MRI show calcifications– Biopsy
– Often found during imaging for other reasons
Granulomatous Liver Disease
Treatment:– Treat the cause (stop meds, treat infection,
etc)
Pyogenic Hepatic Abscess
Multiple routes of entry of bacteria– Common bile duct (ascending cholangitis)– Portal vein – Hepatic artery– Direct extension from infection– Trauma
Pyogenic Hepatic Abscess
Most common bacteria– E. coli– K. Pneumoniae– P. vulgaris– Enterobacter– Multiple anaerobes
Pyogenic Hepatic Abscess
Signs/Symptoms:– Fever almost always present– RUQ pain– Jaundice
Pyogenic Hepatic Abscess
Labs:– Leukocytosis, shift to the left– Liver tests nonspecific– Positive blood culture
Imaging– CXR: elevated diaphragm on R– US, CT, MRI
Pyogenic Hepatic Abscess
Treat:– IV antibiotics (3rd gen cephalosporin plus
metronidazole. 3-6 weeks– Possible abscess drainage– Treat underlying source