lodwar clinic, turkana, kenya · lodwar clinic, turkana, kenya ... derrick lowoto and jonathan...
TRANSCRIPT

1
Lodwar Clinic, Turkana, Kenya
Date: October 30, 2014 Prepared by: Derrick Lowoto and Jonathan White I. Demographic Information 1. City & Province: Lodwar, Turkana , Kenya 2. Organization: Real Medicine Foundation Kenya (www.realmedicinefoundation.org) Medical Mission International (www.mminternational.org.uk) Share International Inc. (www.shareint.net) 3. Project Title: Healthcare Programs – Turkana Drought Region, Northern Kenya 4. Reporting Period: July 1 – September 30, 2014 5. Project Location (region & city/town/village): Lodwar Town, Turkana, Kenya 6. Target Population:
1. Nabuin Village – 3,100 2. Chokchok Village – 3,561 3. Nadapal Village – 2,723 4. Nayanae Village – 1,060 5. Elelea Village – 2,830 6. Kaitese Village – 3,491 7. Nayuu Village - 2,654 8. Nakabaran Village – 2,926 9. Kanamkemer Village – 6,120 10. Nawoitorong Village – 6,450 11. Lodwar Town - 48,316 12. Lomopus Village – 3,780 13. Nakoriongora – 3,670 14. Kangikukus – 3,820 15. Napetet – 5,410 16. Nakwamekwi – 6,210 17. Kerio Region – 24,500 (includes: Lokori, Kalokol, Lokichar, Katilu, Kerio, Kalokutanyang, Kimabur, Lochwaa, Nakepokan, Nakoret, Kaikir, Kapua, Lolupe, Lokichogio, Lomuriae, Lorengelup) Target Population = 106,121 approximately II. Project Information 7. Project Goal: To improve the delivery of Primary Health Care Services within the Turkana Drought Region in Northern Kenya, its capital Lodwar and the people living in the remote villages of Turkana, Kenya. 8. Project Objectives:
• Provide Medicines and Medical supplies to meet the needs of the targeted population • Increase Mobile/Outreach Clinics in the remote villages • Provide Medical Services at the Health Facility in Lodwar Town:
• Supporting the physical/medical needs of the targeted population • Home visitations • Referrals of patients needing advanced care to secondary and tertiary care hospitals, and HIV and
TB government clinics

2
• Teaching about and providing nutritious food. • Provide nutrition to babies and young children.
9. Summary of RMF/MMI-sponsored activities carried out during the reporting period under each project objective
(note any changes from original plans): - A total of 3,859 patients were treated in the medical outreach clinics and 2,800 patients treated at the Lodwar Clinic location. - A total of 40 outreach clinics were conducted in the rural villages in the third quarter. - Twelve home visits were made in the rural villages and within and around Lodwar Town to patients not able to come to the Lodwar Clinic. - We made ten referrals mostly collecting patients who were very sick from rural villages and transporting to our clinic in Lodwar and to Lodwar District Hospital. - Continued public health education done at the beginning of every clinic session. - Purchased medicines. - The program met the cost of medical fees for some patients whom we referred for treatment to other secondary and tertiary health facilities. - The staff maintained the medicine inventory. 10. Results and/or accomplishments achieved during this reporting period: - This quarter we treated a total of 6,659 patients both in the Lodwar Clinic and villages. - During this quarter, 1,687 laboratory tests were conducted with 1,035 tests showing positive results. Many patients tested had malaria. - The program conducted 40 outreaches in the rural villages where health facilities are far from reach. - We made twelve home visits mostly in villages on the outskirts of Lodwar Town. - We provided transportation for ten referrals mostly from rural villages to health facilities in Lodwar. - Public health teaching was done at the beginning of every clinic day for the patients who arrive early and individual teaching on specific cases in the course of treatment. - Purchased medicines from pharmaceutical company in Nairobi, Kenya. - The program paid salaries for the staff. 11. Impact this project has on the community (who is benefiting and how) Having adequate medical personnel and medicine stores has enabled us to treat more patients and combat a wider range of diseases on a regular basis, especially in the remote villages of Turkana. Our target population of this project is at 106,121, and rising. The villages we serve do not have access to other regular medical care. We are able to provide predictable clinic coverage monthly as well as follow up if patients can travel to the Lodwar Clinic. The nomadic nature of the Turkana tribe causes the population of these villages to migrate about every 4 months and to be a new group of villagers about every 4 months; therefore we are providing service to more than the estimated population of persons living in each village at one time. The improved quality and regularity of medication purchase from MEDS in Nairobi through RMF/MMI funding has allowed the clinics to be conducted and improved the quality of the service. Previous to RMF/MMI involvement, medication was scarce and depended on availability of specific donations each month. The clinic staff serves all villagers who come for treatment, but we see an especially high number of children and pregnant women. Prior to the funding provided through RMF/MMI, there were an average of one to two mobile clinics per month, based on variable funding availability through private donors; now there is an average of 30 mobile clinics each month. Previously, there was often not enough medicine in stock to treat all patients; now the proper medication is always available. 12. Number served/number of direct project beneficiaries (for example, average number treated per day or month and if possible, per health condition). A total of 6,659 patients were treated during this quarter, up significantly from Q2 at 4,799; 2,599 patients were male and 4,060 were female. We treated 8,955 cases during this quarter. See Appendix A

3
13. Number of indirect project beneficiaries (geographic coverage): Our services are available to all residents of central and western Turkana, approximately 900,000 persons. 14. If applicable, please list the medical services provided: - Outpatient diagnosis and treatment - Medication available with pharmacy counseling - Public health education with each clinic session - Minor surgery - Wound care - Referral to secondary and tertiary care centers for advanced care - Nutrition supplementation to the elderly, malnourished children and terminally ill during mobile outreach clinics and home visitations - Care of patients with advanced and/or special needs: arranging transport and accompaniment by staff if needed to referral centers for special consultations, procedures, etc. 15. Please list the five most common health problems observed within your region. - Malaria - Respiratory tract infections - Eye infections - Skin diseases - Gastroenteritis 16. Notable project challenges and obstacles: The present maternal and child health clinic does not have adequate space to cater to the population requiring its services. Two additional rooms in the clinic are required to build upon the small and congested building, which currently lacks a friendly environment for women presenting for prenatal care and for children visiting the clinic for immunizations. Maternal and child health services are currently not sufficient to provide for all the patients in rural villages needing these services, where, i.e. children are not immunized against childhood immunizable diseases. The major problem is a shortage of staff that can offer these services to mothers and children. Three additional staff members are required to run these programs to ensure adequate provision of maternal and child healthcare to the population we are serving. 17. If applicable, plans for next reporting: - Thirty-six mobile clinics in the next quarter. - Make emergency trips to villages and offer transport to Lodwar Hospital if needed; especially for complicated deliveries and other medical conditions. - Twelve hospice services (home visits) in the next quarter. - Consider how to best meet the needs of the special cases, which require funds not in the budget. - Pay salaries for the staff. - Purchase medicine from pharmaceutical company in Nairobi, Kenya, at least on monthly basis. - Continue supporting education for staff members, including additional training for the nurse in charge. - Continue looking for additional means of support; in August we received a consignment of medicines from the County Government of Turkana through the Ministry of Health. 18. If applicable, summary of RMF/MMI-sponsored medical supply distribution and use: Please reference Appendix B

4
20. Successful story(s) highlighting project impact. By Derrick Lowoto
1. It was on a hot afternoon while conducting a medical outreach clinic in Nakoriongora Village that a middle-aged man arrived, sweating profusely after a long run. He spoke to the health team and explained that his wife was severely sick and needed help immediately. He had run ten kilometres to the site where we had the medical outreach clinic. Without hesitation we took the necessary medication and part of the team went to rescue the patient. We found the patient (Mrs. Aleper) aged 25 years old and her baby lying down in the hot sun. Her husband had left her under the sun with the baby after struggling to take her under the shade but unable since he was also sick with malaria. It was a very emotional experience for the health team, one member of the team narrated how she found herself tearful after seeing the situation of the patient under the hot sun with her baby. The patient was moved to the shade and given medication and water with difficulty. After the initial medication, the patient was taken to Lodwar Hospital for further treatment where she was diagnosed with severe malaria and amoebiasis. She was treated immediately and discharged four days later in much better condition.
Mrs. Aleper found by the health team under the sun with her baby
Our health team member was very emotional due to the difficult situation people in the rural villages are facing as a result of lack of health facilities within their reach.

5
Mrs. Aleper receives first line treatment of malaria before referral.
Mrs. Aleper supported to take medicine and drink water by health team member and her husband. 2. During the month of August, a female child aged 5 years old was brought by her father to our Lodwar Clinic. After taking her history and a physical examination, the child was found to have a complication that needed proper investigation to ascertain the actual problem. Her parents have been in Lodwar District Hospital several times but with no benefit over her condition. From her previous records and our clinical assessment she is likely to have cardiac-related problems or blood vessels obstructing in the brain.
Somebody donated part of the money to facilitate her referral to a tertiary hospital though more money may be needed. The parents of the girl are poor and are not in a position to meet the cost. Her father told us that they had had twenty goats but the drought that is currently being experienced in Turkanaland has killed them all. We will be keeping an eye on the situation and update as we hear more.

6
The sick girl being held by her father 3. Medical outreaches in August encountered some sad moments. There was a lot of migration of families in rural villages from one area to another in search of water and grass. The famine and drought is so intense that many families had to relocate to a new area where they can get water and some grass for their animals.
Our medical outreach team was very keen to monitor their movement so that this essential service is taken where they have settled. At such times of drought and famine, monitoring of migration of people living in rural villages is essential as this will help us to know where they have settled and where they are planning to re-settle. Sadly sometimes they have to migrate very far away where the medical clinic is unable to reach them.
Prayer session before medical clinic begins in Kaikir Village

7
Medical clinic in a rural village
Immunization being given in a rural village
III. Financial Information 21. Detailed summary of expenditures within each budget category as presented in your funded proposal (file
attachment is fine). Please note any changes from plans. Please see Appendix emailed separately from accountant.

8
APPENDIX A Total patients treated – 6,659 Total cases seen – 8,955 a) Morbidity by disease type
b) Morbidity by village
Disease type Male Female Total Respiratory tract infections 1105 1544 2649 Malaria 1119 1380 2499 Skin diseases 147 279 426 Urinary tract infections 139 244 383 Myalgia 141 340 481 Allergy 59 92 151 Gastroenteritis 276 321 597 Accidents 31 43 74 Gastritis 29 73 102 Epilepsy 6 5 11 Typhoid 58 93 151 Gynecology and Obstetrics 0 93 93 Sexually transmitted diseases 19 26 45 Oral thrush 26 51 77 Peptic ulcer disease 14 20 34 Ear 96 155 251 Eye 183 258 441 Dysentery 10 13 23 Arthritis 52 77 129 Worms infestation 9 16 25 Anemia 14 39 53 Malnutrition 74 114 188 Brucellosis 27 45 72 TOTAL 3634 5321 8955
Village Male Female Total Nawoitorong 600 718 1318 Kanamkemer 574 618 1192 Lodwar town center 25 37 62 Nayuu 78 129 207 Nakabaran 37 86 123 Nakwamekwi 23 30 53 Elelea 134 222 356 Turkwel 0 1 1 Nabuin 170 351 521 Lokichar 8 10 18 Kangikukus 76 161 237 Lodos 100 181 281 Nakoriongora 118 221 339 Lomopus 96 147 243 Kalokutanyang 58 122 180 Kaikir 57 131 188 Nakudet 96 197 293 Chokchok 72 176 248 Nadapal 52 104 156 Monti 112 219 331

9
c) Morbidity by age
d) Laboratory report
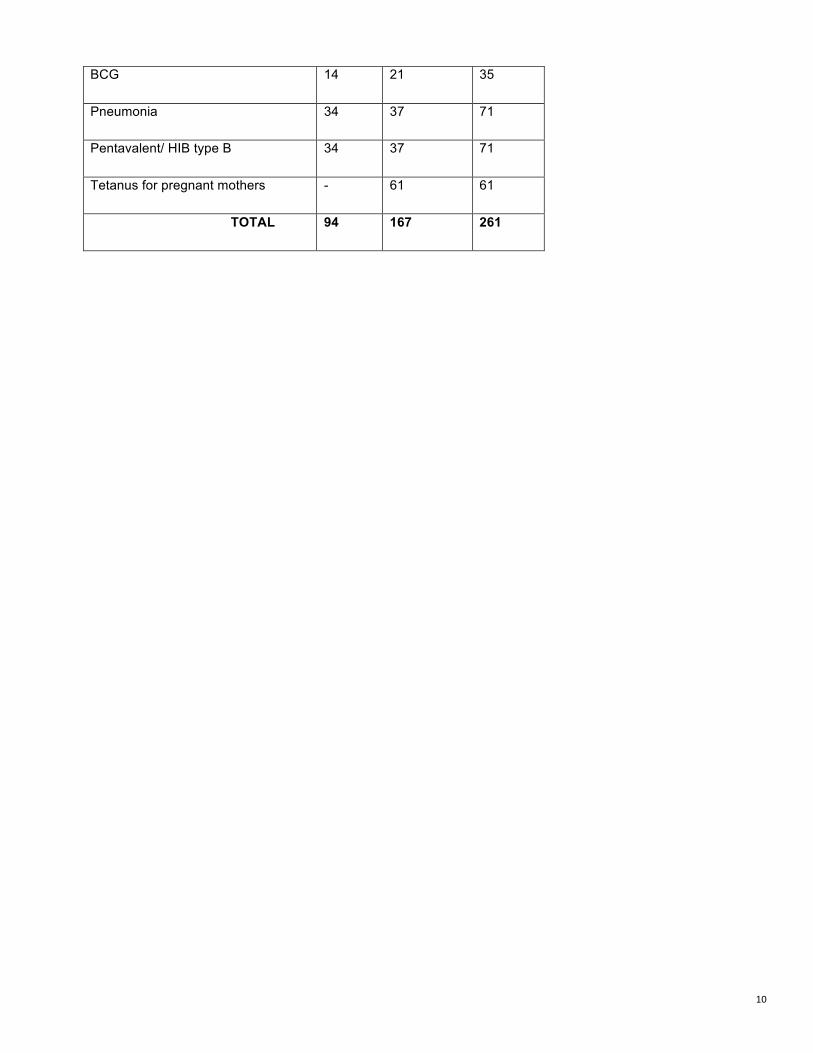
e) Immunization
VACCINE MALE FEMALE TOTAL
Measles 12 11 23
Napetet 15 20 35 Sopel 1 0 1 Kalokol 2 4 6 Nayanae 5 7 12 Locheremoit 3 5 8 Kimabur 4 6 10 Kerio 14 15 29 Nariamao 69 142 211 TOTAL 2,599 4,060 6,659
Age Male Female Total
0-5 945 1043 1988
6-15 535 787 1322
16-24 451 722 1173
25-49 461 1115 1576
50 + 207 394 601
TOTAL 2,599 4,060 6,659
Category No. of tests done No. of positive tests done
Male Female Male Female Malaria - Blood smear 497 488 350 369 Typhoid - Widal test 100 119 40 59 Brucellosis - Brucella 48 55 25 31 Urine - Urinalysis 37 53 16 26 Pregnancy – Urine test - 54 - 54 Syphilis - Blood for VDRL 9 6 3 1
Stool - for Amoebiasis 18 19 5 6 Gonorrhea 4 3 3 2 Blood for HIV 34 38 3 3 Hemoglobin level 36 46 16 22 Blood grouping 9 14 9 14 TOTAL 792 895 470 587
10
BCG 14 21 35
Pneumonia 34 37 71
Pentavalent/ HIB type B 34 37 71
Tetanus for pregnant mothers - 61 61
TOTAL 94 167 261