loneliness and later life: prevalence and consequences christina victor, school of health sciences...
TRANSCRIPT

Loneliness and later life: prevalence and consequences
Christina Victor,School of Health Sciences &
Social Care,Brunel University, UK

Presentation overview
• What is loneliness-definition & measurements
• Prevalence of loneliness
• Consequences of loneliness

What gives quality to life? • Personal social capital (social
activities, contacts and support, loneliness) a key dimension of quality of life
• Social relationships one of the ‘good things’ that give ‘quality’ to life.
Bowling and Gabriel (2004) (Bowling et al. 2002).

What is loneliness?
“Language... has created the word "loneliness" to express the pain of being alone. And it has created the word "solitude" to express the glory of being alone.” - Paul Tillich

What is loneliness?
Cognitive discrepancy theory
Loneliness results from the difference between desired and actual social relations (Perlman & Pelau, 1981)-either in quantity or quality of relationships (or both)
Theoretical or conceptual understandings of loneliness are both complex and contested (Peplau and Perlman, 1982).
Three main approaches:-
Self rating questionSingle dimension scale-UCLAMulti-dimensional scale-de Jong-Gierveld measure which distinguishes social and emotional loneliness

Loneliness and old ageIn 2010 a survey reported community breakdown as the major contemporary ‘social ills- it was felt that neighbours no longer know or look out for one another, which left people feeling isolated, lonely and fearful – particularly the elderly
‘’Loneliness is an inner, gnawing pain born of circumstance and inertia, verging on despair. There is a higher risk the older you get, and no one talks about it’’
Joan Bakewell-The Times 31/12/09

Loneliness and old age
‘’A distressing feature of old age is loneliness. All who have done welfare work among the old have found it the most common, if at the same time the most imponderable, of the ills from which the aged suffer, and its frequency was amply confirmed by our study’’
(Rowntree, 1947,52)

Prevalence of loneliness
• Peer group (comparison with other older people)
• Generation contrasted (comparison with younger people)
• Age-related (comparison with younger selves)• Preceding cohort (comparison with previous
cohorts of older people)

Are older people the loneliest?
Source: Victor & Yang, 2012

Has loneliness in old age increased?
SHELDON 1948
TOWNSEND1954
VICTOR 2005
Always/often 8 9 9
Sometimes 13 25 32
Never 79 66 61
Source: Victor et al, 2009
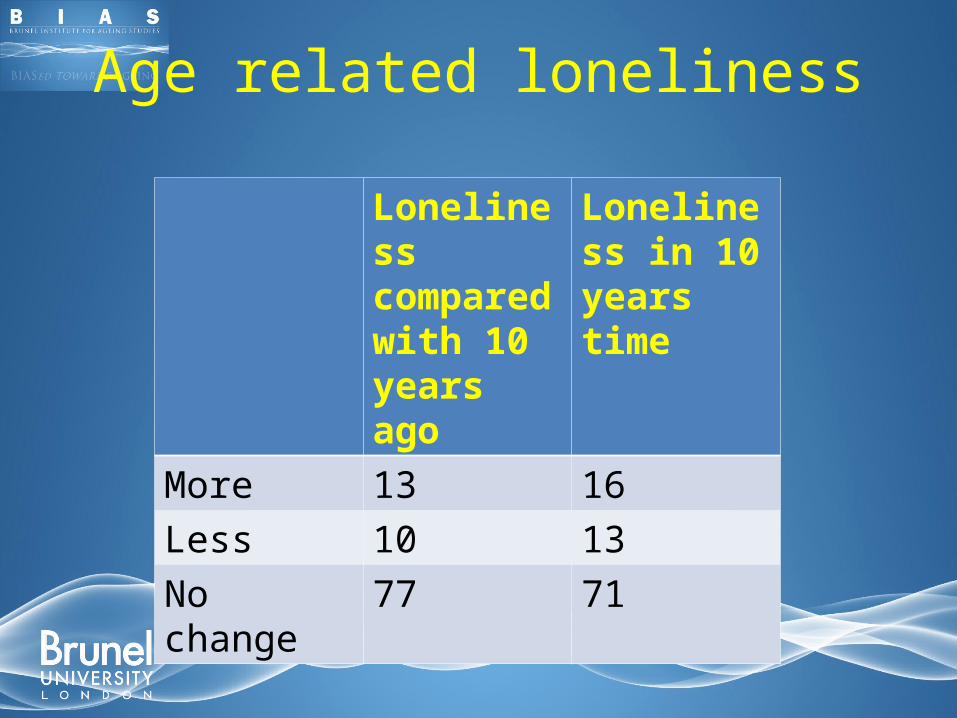
Age related loneliness
Loneliness compared with 10 years ago
Loneliness in 10 years time
More 13 16Less 10 13No change 77 71

Loneliness varies over time• 50% reported loneliness worse at night &
two thirds at weekend (Victor et al, 2005)
• ‘’I'm lonely of a night. ‘’(Man 16)
• ‘’Of a night you're lonely’’. (Woman 12)
• ‘’Such a lonely life … Saturdays and Sundays are a bit dead for me…’’
• ‘’So long [Sunday] and so lonely.’’
Source: Bennett & Victor, 2012

How does loneliness vary over time?
• If we follow people aged 65+ over 5 years we find that:-– 25% become more lonely– 12% become less lonely– 22% were always lonely– 44% never lonely
• So we can see different types of loneliness which might have different causes and require different types of interventions
Source: Victor & Bowling, 2012

Understanding loneliness‘’Loneliness and social isolation are subjective lived experiences that exist in the form of multiple realities constructed and reconstructed by individual older people within the context of their different lives and life histories’’ (Victor et al., 2009).
Source: Sullivan & Victor, 2012
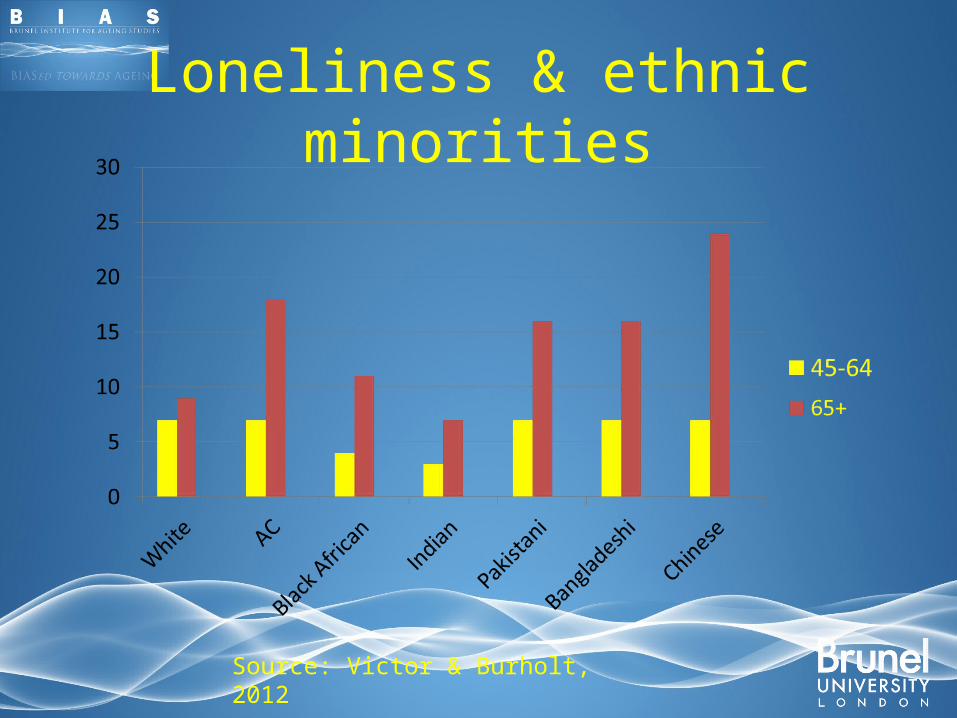
Loneliness & ethnic minorities
Source: Victor & Burholt, 2012

Why does loneliness matter?
• Reduced or low quality of life
• Negative health behaviours (e.g. smoking, alcohol)
• Negative health outcomes - Early studies by Durkheim link loneliness to mortality-50% higher for those lonely/isolated (independent of health status!)
• Excessive use of health services-hospital admission, A&E contact,GP consultations