long-term care wound assessment and documentation: …
TRANSCRIPT

Long-Term Care Wound Assessment and Documentation:
Meeting the Regulatory and Clinical Guidelines for Best Practice
-PART 2-
Ryan P. Dirks MS, PA-C
There is more changing this fall than the weather!Patient Driven Payment Model (PDPM)
replaces RUG-IV (October 1, 2018) PART A
1.SNF Value Based Purchasing Model (SNF VBP)
2.SNF Quality Reporting System (SNF QRS)
PART B- Final Rule Releasing in November 2018, so far it exceeds 660 pages

1. SNF Value Based Purchasing Program (VBP)
• Part A
• EVERY SNF looses 2% off the top of their Federal per diem rate
• Some, all or NONE of this can be earned back based on quality reporting
• There is only 1 measure (for now) to focus on…
• SNF 30-day Readmission Measure (SNFRM-NQF #2510• #2 DRG for readmission is cellulitis

2. SNF Quality Reporting (SNF QRP)
• IMPACT Act 2014
• 3 measures started in 10/1/18
NFQ Measure ID Measure Title
NFQ #0674 Application of percent of residents experiencing one or more falls with major injury (Long Term)
NFQ #0678 Percent of residents with pressure ulcers that are new or worsened
NFQ #2631 LTAC- Function

Also…
• SNF QRP Claims Based Measures
Measure Data Source
Discharge to community Medicare FFS Claims
Potentially preventable 30-days post discharge readmission
Medicare FFS Claims
Medicare spending per beneficiary Medicare FFS Claims

And…
• 6 New Measures (data collection 10/1/18 impacting payment 10/1/19
Measure MDS
Drug Regimen Review Section N
Change in Skin, Pressure Ulcer/Injury Section M
Change in Self Care Section GG
Change in Mobility Section GG
Discharge Self Care Score Section GG
Discharge Mobility Score Section GG

Pressure It takes a Team!
• Success with new payment models requires accurate assessment of non-pressure vs. pressure injuries/ulcers
• DON’T MISTAKENLY CALL THINGS PRESSURE THAT ARE NOT PRESSURE!
AND
• Aggressive prevention and treatment of wound related conditions in order to avoid re-hospitalizations

Road to of success Detailed Wound Assessment/Risk
Assessment
Individualized Care Planning
Evidence-Based Treatment
Documentation
Documentation
External Support

Road of Wound Care Success Includes…
1) Committed People- Wound Champion or Navigator • Education, Education, Education
• Cross Training (Nursing, CNA/NAC, dietary, therapy)
• Expertise
2) Outcomes driven process- results are key• Admission to discharge, heavily focused on individualized care and
documentation

Road to of success starts with assessment
Detailed Wound Assessment/Risk
Assessment
Individualized Care Planning
Evidence-Based Treatment
Documentation
Documentation
External Support

Wound Assessment Must Combine
Visual
Tactile
Olfactory
Expertise

What is a Chronic Wound and What Causes It?
12Copyright © 2018 - AMT Education
Division

Chronic Wound Definition
Copyright © 2018 - AMT Education Division 13
• “have failed to proceed through an orderly and timely process to produce anatomic and functional integrity, or proceeded through the repair process without establishing a sustained anatomic and functional result”
• For reimbursement CMS considers chronic wounds to be one that has not improved within 30 days with usual and customary wound care interventions
Nustoe TA, O’Shaughnessy K, Kloeters O. Chronic wound pathogenesis and current treatment
strategies: a unifying hypothesis. J Plast Reconstr Surg. 2006;117:35-41.

Most Common Chronic Wound Etiologies
Pressure Ulcer/
Injuries
PeripheralArterialDisease
VenousInsufficiency
Diabetic Neuropathic
Foot Ulcers
Lymphedema

Other Frequently Encountered Wounds
Copyright © 2018 Gordian Medical, Inc. dba American Medical Technologies. www.amtwoundcare.com
Moisture Associated
Skin Damage
Deep Tissue Pressure
Injury
Kennedy Terminal
Ulcer
(KTU)
AKA
Skin Failure
Medical Adhesive
Related Skin Injury
(MARSI)
Medical Device Related Pressure Injury
Must be staged and reported on
the MDS
15

Other Frequently Encountered Wounds
Copyright © 2018 Gordian Medical, Inc. dba American Medical Technologies. www.amtwoundcare.com
Surgical Dehiscence
Infection
Poor closing technique
Too much strain on incision by
patient
Skin Tears
Can be partial or full-
thickness injuries
Considered traumatic
wound
Atypical Wounds
Host of different etiologies often associated with
autoimmune diseases
Cancer Wounds
Fungating wound
depicted here
16

Autoimmune/Atypical Wounds
Copyright © 2018 Gordian Medical, Inc. dba American Medical Technologies. www.amtwoundcare.com
Pyoderma Gangrenosum
Beware of Pathergy
Effect
Vasculitis
Inflammation and
destruction of blood vessels
Pemphigus Vulgaris
Auto-antibodies
against some part of
epidermis
Oral lesions seen 1st
Bullous Pemphigoid
Most common
auto-immune
dermatosis
(Allergy to one’s own
skin)
Bullous Diabeticorum
Spontaneous non-
inflammatory blistering unique to
patients with diabetes17
Attrib
utio
n:
Derm
atolo
gy Info
rmatio
n
Cen
ter

Factors that Contribute to Wound Chronicity
• Increased bacterial load• Excessive proteases
• Degraded• Growth factors• Matrix proteins• Cell surface receptors
• Prolonged inflammation• Cellular senescence• Inadequate / inappropriate treatment
• Diseases or conditions• Competing for oxygen or
metabolic resources• Medications
• Steroids• Immunosuppressive agents• Chemotherapy
• Patient adherence• Diet/blood glucose• Smoking• Off-loading
18
Time Driven Patient Driven
Complicating Factors-About 60 Listed on FormOver 100 Complicating Factors
• Age
• Chronicity of wound
• Cognitive status
• Incontinence – Braden
• Location
• Medications – Steroids
• Mobility Impairment – Braden
• Activity - Braden
• Sensory deficits – Braden
• Nutrition/hydration - Braden
• Pain – Braden
• Psychosocial/Behavioral Issues
• Skin-Integrity Impairment
• Vascular/Cardiovascular Impairments
• Wound decline/complications
19
Copyright © 2018 - AMT Education Division

Pressure Injury/Ulcer

What is NOT a Pressure Injury/Ulcer?

Moisture Associated Skin Damage
• NOT a pressure injury
• Top Down Mechanism vs. Bottom UP
• Documentation of the history is key

Moisture Associated Skin Damage
• Risk Factors• Prolonged exposure to moisture +
chemical irritant• Urine
• Stool
• Wound Exudate
• Perspiration
• Mucous
• Saliva
• TOP DOWN MECHANISM
• Characteristics • Inflammation with or without
erosion
• History indicating exposure to moisture and chemical irritant
• Incontinence (incontinence associated dermatitis)
• C-Diff
• “the mystery is in the history”

Moisture Associated Skin Damage
• Assessment• Visual assessment
• “The mystery is in the history”
• location
• Treatment • Reduce irritant exposure
• Consistent regimen of skin barrier
• Identify and treat fungal infections quickly

Diabetic Ulcers

Diabetic Ulcer

Diabetic Foot Ulcer

Microvascular Disease

Diabetic Foot Ulcer
• Risk Factors• Diabetes
• Metabolic Syndrome
• Insulin Resistance
• A continuum not everyone who is diabetic KNOWS they are.
• Characteristics • Round
• Deep
• Painless
• Foot deformity
• Callous

Diabetic foot deformity

Diabetic Foot Ulcer
• Assessment• Fasting Glucose
• Hemoglobin A1C (HgA1C)
• Neuropathy exam
• ABI/PAD assessment
• Treatment • Strict glycemic control
• Target is <140
• Wound healing stops at >180
• Wound bed preparation
• Moist warm wound healing
• Callus management
• Off-loading is KEY
• Don’t forget foot checks and footwear

Wound Bed Preparation

To Debride or Not to Debride… there is noquestion!

Biofilm

Offloading

Arterial Ulcer


Arterial Ulcer

Arterial Ulcer
• Risk Factors• Diabetes• Metabolic Syndrome• Insulin Resistance• Hyperlipidemia • Hypertension• Known artherosclerosis
• Coronary Artery Disease (History of Angina or MI)
• Carotid Stenosis• *can be in upper extremities also
• Characteristics • Round “punched out”• Deep• Painful• Scant drainage• Site of trauma• Periwound edema

Arterial Ulcer
• Assessment• Physical Exam (no cost)
• ABI/PAD assessment (low cost)
• May need arterial duplex doppler (high cost) *cheaper than a lawsuit for Part A stay resident
• HgA1C
• Treatment • Vascular surgery consultation
• “time is tissue”
• Wound bed preparation
• Moist warm wound healing
• Pain management
• Dry stable eschar should always be left intact



Venous Ulcer

Venous Ulcer

Venous Ulcer

Venous Ulcer
• Risk Factors• Obesity
• Known venous hypertension
• Prior venous wound
• Vericose Veins
• DVT
• Impaired calf pump
• Characteristics • Large
• Deep
• Painful
• Copious drainage
• Site of trauma
• Hemosiderin staining
• Venoustasis dermatitis
• Limb edema


Venous Ulcer
• Assessment• Physical Exam (no cost)
• Venous duplex doppler (complete exam, not “rule out DVT exam”
• ABI
• Treatment • Compression, compression,
compression
• Wound bed preparation
• Moist warm wound healing
• Pain management

Compression

CMS Guidelines/Mandates for Assessing Non-Pressure Ulcer Wounds
Copyright © 2018 - AMT Education Division 50
• At the time of the assessment and diagnosis of a skin ulcer/wound, the clinician is expected to document:
• underlying condition contributing to the ulcerationDATA IS KEY (LABS, IMAGING, EXPERT CONSULTATION)
• ulcer edges
• wound bed
• location
• condition of surrounding tissues
• especially if the ulcer has characteristics consistent with a pressure ulcer, but is determined not to be one.

Definition of Pressure Injury• Localized damage to the skin and/or underlying soft tissue usually
over a bony prominence or related to a medical or other device. The injury can present as intact skin or an open ulcer and may be painful. The injury occurs as a result of intense and/or prolonged pressure or pressure in combination with shear. The tolerance of soft tissue for pressure and shear may also be affected by microclimate, nutrition, perfusion, co-morbidities and condition of the soft tissue.
(NPUAP, 2016)

Pathogenesis of Pressure Injury
• “Stuck between a rock and a hard place”
• Capillary closing pressure generally considered to be 32 mmHg• Venous/lymphatic outflow ceases• Increased hydrostatic pressure reduces arterial
inflow
(Bryant, R.A. & Nix, D.P.,2007)

Pathogenesis of Pressure Injury
• Within 2-9 hours of sustained pressure tissue ischemia can occur.
(Bryant, R.A. & Nix, D.P.,2007)

Sites for Pressure Injury Development

WHY DO WE NEED TO STAGE?

Layers of Skin
• Epidermis
• Dermis
• Subcutaneous

Stage 1 Pressure Injury

Stage 1 pressure Injury
• Intact skin with a localized area of non-blanchable erythema, which may appear differently in darkly pigmented skin. Presence of blanchable erythema or changes in sensation, temperature, or firmness may precede visual changes.
• Color changes do not include purple or maroon discoloration; these may indicate deep tissue pressure injury.
(NPUAP2016)

Stage 2 Pressure Injury

STAGE 2
Stage 2 Pressure Injury
Partial Thickness Skin loss with exposed dermis Wound bed is viable, pink or red, moist, and may also present as an intact
or ruptured serum-filled blister.
Adipose (fat) is not visible and deeper tissues are not visible. Granulation tissue, slough and eschar are not present.
These injuries commonly result from adverse microclimate and shear in the skin over the pelvis and shear in the heel. This stage should not be used to describe moisture associated skin damage (MASD) including incontinence associated dermatitis (IAD), intertriginous dermatitis (ITD), medical adhesive related skin injury (MARSI), or traumatic wounds (skin tears, burns, abrasions).
(NPUAP2016)

Stage 3 Pressure injury

Stage 3 Pressure Injury
Full Thickness Skin Loss
Granulation tissue and adipose tissue often visible
Slough and/or eschar may be visible
Depth of the tissue damage varies depending on anatomical location (no stage 3 on nose and ear)
Undermining and tunneling may occur
Fascia, Muscle and tendon ligaments, cartilage , and bone are not exposed
If slough or eschar obscures the extent of the tissue loss the wound be considered Unstageable.
(NPUAP2016)

STAGE 3

Stage 4 Pressure Injury

Stage 4 Pressure Injury
Full Thickness and Tissue Loss exposed WITH directly palpable fascia, muscle, tendon, ligament, cartilage or bone in the ulcer
Slough and/or eschar may be visible
undermining and/or tunneling often occur
Depth varies by anatomical location
If slough or eschar obscures----STILL A STAGE 4!
(NPUAP2016)

Unstageable Pressure Injury Full thickness skin and tissue loss in which the extent of the tissue
damage within the ulcer cannot be confirmed because it is obscured by slough or eschar.
If slough or eschar is removed, a Stage 3 or Stage 4 pressure injury will be revealed.
Stable eschar (i.e. dry, adherent, intact without erythema or fluctuance) on an ischemic limb or the heel(s) should not be removed.
(NPUAP2016)

Unstagable Pressure Injury

Deep Tissue Pressure Injury

Deep Tissue Injury Persistent non-blanchable deep red, maroon or purple discoloration
Intact or non-intact skin or blood filled blister
Pain and temperature change often can precede a skin color change
Discoloration may appear differently in darkly pigmented skin
DTPI results from intense and/or prolonged pressure and shear forces at the bone-muscle interfaces
Can evolve rapidly to reveal the actual extent of tissue injury, or may resolve without tissue loss. If necrotic tissue, subcutaneous tissue, granulation tissue, fascia, muscle or other underlying structures are visible, this indicates a full thickness pressure injury (Unstageable, Stage 3 or Stage 4)
(NPUAP2016)

DEEP TISSUE PRESSURE INJURY

KENNEDY ULCER

MEDICAL DEVICE PRESSURE INJURY

MEDICAL DEVICE PRESSURE INJURY

INCREASED RISK WITH:
• Impaired sensation
• Moisture under the device
• Poor perfusion
• Altered tissue tolerance
• Poor nutritional status
• Edema

Common devices
• Nasogastric tubes • Feeding tubes • Endotracheal tubes • Tracheostomy tubes/collars/straps • Oxygen delivery – Mask • – Nasal cannula
• IV/PICC line/Central lines • Anti-Embolic stockings • bedpans

I have some very bad news!

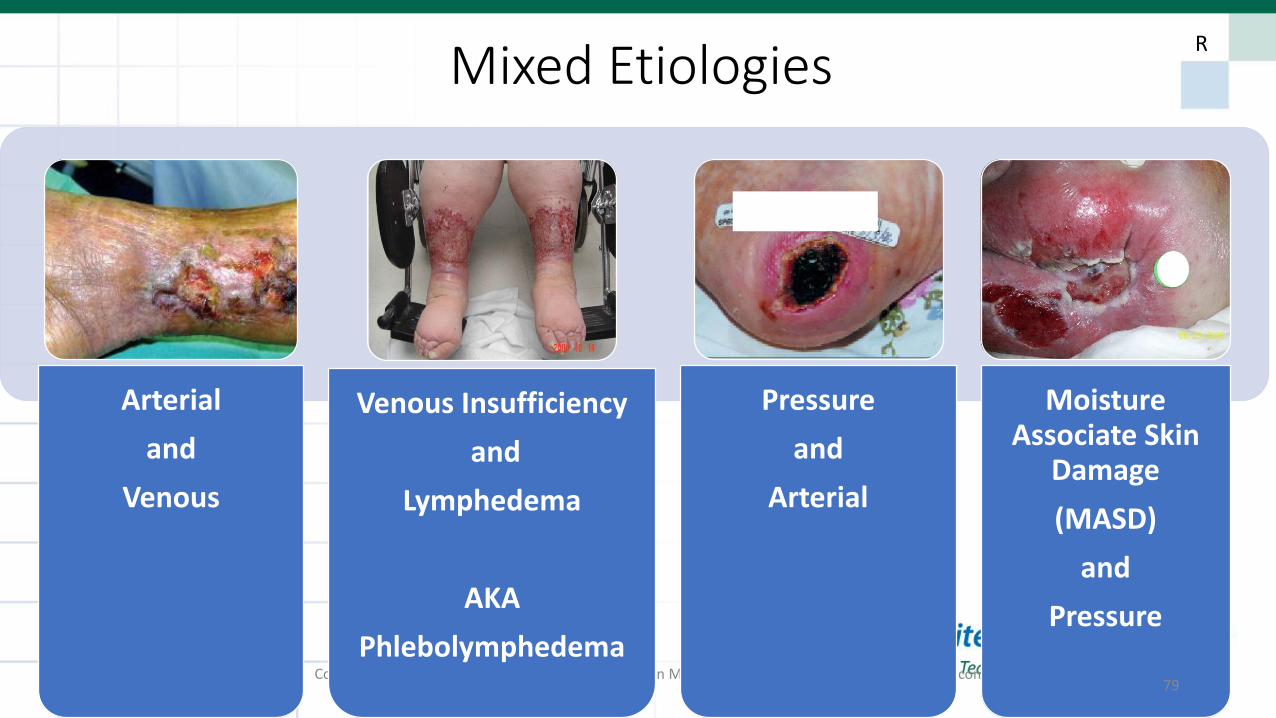
Mixed Etiologies
Copyright © 2018 Gordian Medical, Inc. dba American Medical Technologies. www.amtwoundcare.com
Arterial
and
Venous
Venous Insufficiency
and
Lymphedema
AKA
Phlebolymphedema
Pressure
and
Arterial
Moisture Associate Skin
Damage
(MASD)
and
Pressure
79
xx xx xX XX
Xx
xx xx
R

The Wound Care Practitioner
• MD, DO, ARNP, PA-C, PT
• Benefits • Assessment and documentation of the comorbidities impacting
• wound healing… as well as not • Wound regression or stalling• risk for new/more wounds
• Bedside procedures including surgical/excisional debridement • Advanced differential diagnosis and work up• Education and encouragement• Coordination and networking with other specialists • Documentation, documentation, documentation

Excisional Debridement
• Initial encounter • 5 min later

And…

Treat the whole patient not just the hole in the patient!• Protein, Albumin, Pre albumin
• Fasting Glucose, A1C
• ABI
• Osteomyelitis Work Up (exposed bone in a diabetic is osteo until proven otherwise)
• Imaging (XR, CT, MRI, Bone Scan)
• Tissue Biopsy, wound culture
• Dermatopathology (cancer)

Team-Centered Wound Care

What Makes a Winning Team?
– Focusing on patient care
– Willing to discuss ideas and challenge each other in a positive way while always moving to a solution.
– Understanding that together we are better than if we worked independently:• Bringing different treatment ideas together to find the best treatment
• Serving each other to provide care that would be extremely difficult for one person (one person treats, one positions, one charts)
• Daily care combined with weekly consulting with an expert can produce faster/more complete healing.
Winning Components of Weekly Wound Rounds• Consistent Team members
• Organized Approach
• Accurate Wound Assessments
• Evidence-Based Treatments
• Infection Prevention
• Consistent Documentation
• Routine

Wound Rounds Flow
Huddle
Position
AssessWound
Bed Prep
Dressing
IDT Team Members Present• DNS/ADON
• Dietary Manager/RD
• Therapist
• SDC
• CNA/NAC (new regs)
• Unit Manager/RCM’s
• MDS nurse
IDT Skin Review
Thank you!