longterm antibacterial effect of chx glass ionomers
TRANSCRIPT

29
*Associate professor, Department of Restorative Dentistry and Endodontics, Ege University, School of Dentistry, Izmir, Turkey
†Professor, Department of Restorative Dentistry and Endodontics, Ege University, School of Dentistry, Izmir, Turkey
‡Associate professor, Department of Pedodontics, Ege University, School of Dentistry, Izmir, Turkey§Associate professor, Department of Basic and Industrial Microbiology, Ege University,
Faculty of Science, Izmir, Turkey¶Chemist, Dentsply DeTrey, Konstanz, Germany
Long-Term Antibacterial Effects and Physical Properties of a Chlorhexidine-Containing Glass Ionomer Cement
L. SEBNEM TÜRKÜN, DDS, PHD*
MURAT TÜRKÜN, DDS, PHD†
FAHINUR ERTUGRUL, DDS, PHD‡
MUSTAFA ATES, PHD§
STEFAN BRUGGER, PHD¶
ABSTRACTStatement of the Problem: Many regions in the world do not have electricity, water, or access todental facilities that allows the treatment of caries with dental handpieces and rotary burs. Forrestorative techniques used in these regions, an antibacterial self-adherent glass ionomer materialwould contribute considerably.
Purpose: This study aimed to test if chlorhexidine diacetate (Fluka BioChemika, Buchs, Switzerland)- or chlorhexidine digluconate (Sigma-Aldrich, Steinheim, Germany)-added ChemFilSuperior glass ionomer cement (Dentsply DeTrey, Konstanz, Germany) had any long-termantibacterial effect against certain oral bacteria and to test the new formulation’s physical properties.
Materials and Methods: ChemFil Superior was used as a control. Chlorhexidine diacetate (pow-der) was added to the powder and chlorhexidine digluconate (liquid) was mixed with the powderin order to obtain 0.5, 1.25, and 2.5% concentrations of the respective groups. Setting time,compressive strength, and acid erosion were tested according to ISO 9917-1. Working time,hardness, diametral tensile strength, and biaxial flexural strength were also determined. Long-term antimicrobial activity against S. mutans, L. acidophilus, and C. albicans were tested withthe agar diffusion method. Analysis of variance (ANOVA) was used for comparison (p < 0.05).
Results: Regarding the immediate antibacterial effect for S. mutans, all the tested groups showedinhibitions of the strain compared with the control group (p < 0.05), with larger zones for thehigher concentration groups and all the diacetates. For L. acidophilus, all the groups were effec-tive compared with the control, but the greatest antibacterial effect was observed with the 2.5%diacetate group. The 2.5% group of chlorhexidine diacetate showed antibacterial activity up to90 days against S. mutans and up to 60 days against L. acidophilus. The working and settingtime, acid erosion test, diametral tensile strength, and biaxial flexural strength of the tested
© 2 0 0 8 , C O P Y R I G H T T H E A U T H O R SJ O U R N A L C O M P I L A T I O N © 2 0 0 8 , B L A C K W E L L P U B L I S H I N GDOI 10.1111/j.1708-8240.2008.00146.x V O L U M E 2 0 , N U M B E R 1 , 2 0 0 8

30
A N T I B A C T E R I A L E F F E C T S O F A C H L O R H E X I D I N E - C O N T A I N I N G G I C
© 2 0 0 8 , C O P Y R I G H T T H E A U T H O R SJ O U R N A L C O M P I L A T I O N © 2 0 0 8 , B L A C K W E L L P U B L I S H I N G
I N T R O D U C T I O N
Caries disease still remains amajor public health problem
despite the widespread use of fluo-ride and the decline in caries preva-lence observed in the majority ofhighly industrialized countries.1
Caries epidemiology will stillremain an indispensable part ofdental public health because chil-dren of low socioeconomic statusgenerally have higher disease levels,leading to an increase in cariesprevalence as well. Furthermore,many regions in the world do nothave electricity, water, or access todental facilities that allows thetreatment of caries with dentalhandpieces and rotary burs. Forfield treatment in these regions, anew technique based on manualinstrumentation, atraumaticrestorative treatment (ART), was developed.2
The ART is a minimal-interventionapproach where demineralizedtooth tissues are removed usinghand instruments and the cavity,
including adjacent pits and fissures,are restored with adhesive restora-tive materials.3 Today, ART doesnot seem to be confined to placeswhere electricity is absent. It is alsoaccepted by patients with dentalanxiety and by children in modernclinical settings, as the sound andpressure caused by rotary instru-ments is omitted and local anesthe-sia is not needed.4 At the beginning,conventional hand-mixed glassionomer cements (GICs) were usedwith ART; later on, condensed glassionomers with improved physicalstrength were produced especiallyfor ART.2–4 Early studies applied in the field revealed the success of ART.4
However, dental hand instrumentsalone do not remove carious dentinas effectively as rotary burs,5 andcariogenic bacteria can surviveincarceration under GIC restora-tions for up to 2 years.6,7 Conse-quently, cavities treated by ARTmay have residual infected dentin,and if a GIC is unable to arrest the
carious process, the restorationcould fail.8 For that purpose, theimprovement of filling materials toovercome the problems caused byincomplete removal of infecteddentin will be beneficial for increasing the success rate of ART further.
The chemistry of the setting reac-tion of all versions of glassionomers is essentially an acid/basereaction, and the two major advan-tages of the material are an ionexchange adhesion and a continu-ing fluoride release. Recently, sev-eral hand-mixed conventional GICshave been manufactured specificallyfor the ART approach.9 Reportshave shown that the newer, moreviscous GICs release substantiallyless cumulative fluoride ions thanless-viscous esthetic restorativeGICs and resin-modified GICs.10–13
The effect of the lower fluoride ionsrelease on the ability of the viscousGICs to inhibit dental caries inadjacent tooth tissues is not known.Moreover, the use of GIC as a
groups were not different from the control ChemFil group. However, the 1.25 and 2.5% groupsof chlorhexidine diacetate had significantly lower compressive strengths than the control group. Lower hardness values were obtained with the 0.5 and 2.5% chlorhexidine digluconategroups in comparison with the control group.
CLINICAL SIGNIFICANCEThe results of this in vitro investigation demonstrated that chlorhexidine diacetate or digluconateadded to the ChemFil Superior glass ionomer material can exhibit long-term antibacterial effects against S. mutans and L. acidophilus without compromising the physical properties of the material.
(J Esthet Restor Dent 20:29–45, 2008)

T Ü R K Ü N E T A L
V O L U M E 2 0 , N U M B E R 1 , 2 0 0 8 31
restorative material for the sealing-in of caries is also questionedbecause of the possible microleak-age and limitations associated withtheir physical properties.8
Therapeutic benefit may thereforebe gained by combining antibacterial agents with glassionomer materials.
Recently, researchers modified fill-ing materials such as compositeresins, acrylic resins, and GICs by adding chlorhexidine (CHX)and quaternary ammonium compounds.14 Moreover, antisepticagents have the potential to be usedin combination with GICs to obtainan antibacterial restorative mater-ial. From the dental literature, itappears that CHX has been incor-porated frequently into GIC materi-als, and all of the studies haveshown an increased antibacterialeffect in vitro.15–17 However, theincorporation of antibacterialagents in restorative materials fre-quently results in changes in thephysical properties,14,15,18,19 and itis critical that the type of restora-tive material show strong enoughphysical properties to resist occlusalload. Therefore, antibacterial GICsfor use in the ART approachrequire an optimum amount ofantibacterial agents, which shouldnot jeopardize the basic propertiesof the parent materials.15–22 It wasshown that the incorporation ofCHX dihydrochloride and CHXdiacetate into GICs can increase the
antimicrobial effect without seriously compromising the physical properties of the original material.15,16
This study aimed to: (1) test ifCHX diacetate- or CHX diglu-conate-added ChemFil SuperiorGIC had any long-term antibacter-ial effect, (2) test if these new for-mulations had similar physicalproperties compared with the par-ent material, and (3) determine theoptimal concentration of CHXincorporation for obtainingantibacterial GICs for use with theART approach.
M A T E R I A L S A N D M E T H O D S
CHX diacetate monohydrate (Lot37/4204/1 24999, Fluka Bio-Chemika, Buchs, Switzerland),which is commercially available asa solid substance, was added to aconventional glass ionomer powder,ChemFil Superior LY (Lot0507001008, Dentsply DeTrey,Konstanz, Germany) in order toobtain three groups of 0.5, 1.25,and 2.5% concentrations (= content) of CHX in the GIC formulation. The same procedurewas used with the CHX diglu-conate solution (Lot 084K0536,Sigma-Aldrich, Steinheim, Ger-many), which is available as anaqueous solution. The original ratioof powder/liquid for ChemFil Supe-rior was 7.4g :1g and was used asa reference. For the CHX diacetategroup, 29.829g of ChemFil powder
was mixed with 0.171g of CHXdiacetate to obtain a 0.5% formula-tion. For the 2.5% diacetate formu-lation, 29.148g of ChemFil powderwas mixed with 0.852g of CHXdiacetate, and the half dose wasused in order to obtain the 1.25%group. Three different GIC liquids,containing different amounts ofCHX digluconate, were prepared.The ChemFil powder was thenmixed with the undiluted CHXdigluconate solution to obtain the2.5% digluconate formulation. Thissolution was diluted 50% with dis-tilled water to obtain the 1.25%formulation. For the last group,4.190g of CHX digluconate wasadded to 95.810g of water toobtain the 0.5% CHX digluconateformulation. The groups tested arepresented in Table 1.
Agar-Diffusion TestThe antibacterial activity was eval-uated against S. mutans CCUG6519 (Culture Collection, Univer-sity of Göteborg, Sweden), L. acidophilus LA-CH-5DVS(CHR.HANS, Copenhagen, Denmark), and C. albicans ATCC10231 (American Type CultureCollection, Rockville, MD, USA)using the agar-diffusion test. Thesemicroorganisms were chosenbecause S. mutans is the main bac-teria responsible for caries forma-tion, L. acidophilus is the principlebacteria related to caries progres-sion, and C. albicans was recentlyisolated in 58 to 70% of the caries
32
A N T I B A C T E R I A L E F F E C T S O F A C H L O R H E X I D I N E - C O N T A I N I N G G I C
© 2 0 0 8 , C O P Y R I G H T T H E A U T H O R SJ O U R N A L C O M P I L A T I O N © 2 0 0 8 , B L A C K W E L L P U B L I S H I N G
in children23,24 and in root cariouslesions in middle-aged and olderadults.25
All procedures were carried outunder aseptic conditions in a lami-nar airflow cabinet. Seventy speci-mens were prepared for the sixantibacterial material-added groupsand the control (N = 10) for the initial antibacterial effect, and 70more for testing the 24-hourantibacterial effect. For the long-lasting procedure, only fivespecimens were used for the tested groups.
All bacteria and yeast were culti-vated overnight in specific culturemediums: tryptic soy broth for S.mutans, Lactobacilli MRS broth forL. acidophilus, and Sabouraud dextrose broth for C. albicans(800.675.0908, Difco Laboratories,Detroit, MI, USA) at 37°C. Theincubation for S. mutans and L.acidophilus had a 5% CO2 addi-tion, whereas the one used for C.albicans had no additions. The
broth culture was diluted andgrown to a density of 107 colonyforming units (cfu)/mL, confirmedby viable cell count.
Twenty-five milliliters of the respec-tive culture mediums with agar(tryptic soy agar for S. mutans, Lactobacilli MRS agar for L. acidophilus, and Sabouraud dex-trose agar for C. albicans) wereevenly distributed over the surfaceof 15-cm-diameter petri dishes to athickness of 5mm. For each petridish, seven standardized wells witha diameter of 4mm were punchedinto the agar with the blunt end ofa sterile Pasteur pipette. Bacterialinoculation was made by a bentglass rod over the agar surfaceswith 0.5mL of the microorganism’ssuspension (107 cfu/mL).
The powder-liquid materials weremixed for 30 seconds with sterilemetal spatulas to the given ratiosand inserted in the wells within 1 minute with sterile dental instruments. For monitoring the
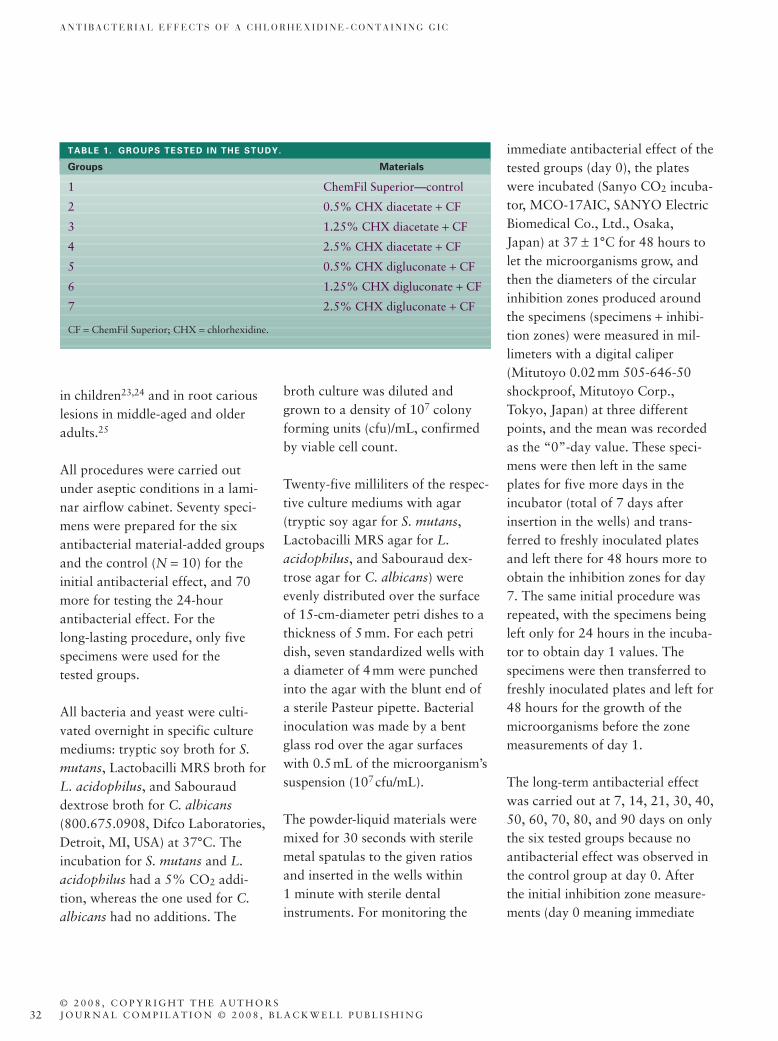
TABLE 1. GROUPS TESTED IN THE STUDY.
Groups Materials
1 ChemFil Superior—control
2 0.5% CHX diacetate + CF
3 1.25% CHX diacetate + CF
4 2.5% CHX diacetate + CF
5 0.5% CHX digluconate + CF
6 1.25% CHX digluconate + CF
7 2.5% CHX digluconate + CF
CF = ChemFil Superior; CHX = chlorhexidine.
immediate antibacterial effect of thetested groups (day 0), the plateswere incubated (Sanyo CO2 incuba-tor, MCO-17AIC, SANYO ElectricBiomedical Co., Ltd., Osaka,Japan) at 37 ± 1°C for 48 hours tolet the microorganisms grow, andthen the diameters of the circularinhibition zones produced aroundthe specimens (specimens + inhibi-tion zones) were measured in mil-limeters with a digital caliper(Mitutoyo 0.02mm 505-646-50shockproof, Mitutoyo Corp.,Tokyo, Japan) at three differentpoints, and the mean was recordedas the “0”-day value. These speci-mens were then left in the sameplates for five more days in theincubator (total of 7 days afterinsertion in the wells) and trans-ferred to freshly inoculated platesand left there for 48 hours more toobtain the inhibition zones for day7. The same initial procedure wasrepeated, with the specimens beingleft only for 24 hours in the incuba-tor to obtain day 1 values. Thespecimens were then transferred tofreshly inoculated plates and left for48 hours for the growth of themicroorganisms before the zonemeasurements of day 1.
The long-term antibacterial effectwas carried out at 7, 14, 21, 30, 40,50, 60, 70, 80, and 90 days on onlythe six tested groups because noantibacterial effect was observed inthe control group at day 0. Afterthe initial inhibition zone measure-ments (day 0 meaning immediate

T Ü R K Ü N E T A L
V O L U M E 2 0 , N U M B E R 1 , 2 0 0 8 33
effect), all the samples were incubated at 37 ± 1°C in their initialpetri dishes until day 7. On that day,the respective culture mediums withfresh agar for the microorganismswere placed in new petri dishes, sixstandardized wells were punchedinto the agar, and new bacterialinoculation was made over the agarsurfaces with 0.5mL of the bacterialsuspension (107 cfu/mL). The glassionomer specimens were taken outof their previous petri dishes andplaced in the new wells. The plateswere then incubated with activemicroorganisms at 37 ± 1°C for 24hours, and the diameters of the inhi-bition zones around the specimenswere measured in millimeters with adigital caliper the day after. Thisprocedure was repeated with freshagar plates inoculated with freshmicroorganisms on all the control days.
For all seven groups, the settingtime, compressive strength, andacid erosion were tested accordingto ISO 9917-1 standards.26 Allspecimens were mixed at a temper-ature of 23 ± 1°C and a relativehumidity of 50 ± 10%. A fresh mixwas prepared for each specimen.
Net Setting TimeThe net setting time is the period oftime measured from the end of mix-ing until the material has set. Thetest was undertaken in a climaticcabinet capable of being maintainedat a temperature of 37 ± 1°C and arelative humidity of 95 ± 5% using
an indentor (Gilmore needle) with amass of 400 ± 5g, a needle having aflat end that is plane and perpendic-ular to the long axis of the needle.Five specimens per group were pre-pared in stainless-steel blocks of 8mm ¥ 75mm ¥ 100mm positionedon aluminum foils and filled to alevel surface with the mixed GICs.Sixty seconds after the end of mix-ing, the assembly, comprising mold,foil, and cement, was placed in thecabinet. Ninety seconds after theend of mixing, the indentor wascarefully lowered vertically onto thesurface of the cement and remainedthere for 5 seconds. The processwas repeated, starting the indenta-tion at 30 seconds before theapproximate setting time was determined, making indentations at 10-second intervals. The net setting time was recorded as thetime elapsed between the end of mixing and the time when the needle failed to make a complete circular indentation in the cement.
Compressive StrengthFive specimens per group were pre-pared using a split stainless-steelmold with inner dimensions of 6 ± 0.1-mm height and 4 ± 0.1-mmdiameter. The molds were treatedwith a 5% solution of beeswax involatile petroleum ether. The petro-leum ether was given a few secondsto evaporate, and the residualbeeswax gave a very thin layer tocoat the surface of the mold. Within60 seconds after the end of mixing,
the GICs were packed into the splitmolds and covered with the plates.One hour later, the specimens wereground with wet 500-grit siliconcarbide paper and stored at 37 ± 1°C in water for 24 hours.Prior to testing, the diameter ofeach specimen was determinedusing a micrometer gauge, and thespecimens were placed with the flatends up between the plates of theuniversal testing machine (Zwickmachine, Z010, Zwick GmbH &Co., Ulm, Germany). A compres-sive load along the long axis wasapplied at a crosshead speed of 1mm/min. The maximum forceapplied when the specimens frac-tured was recorded, and the com-pressive strength was calculated inN/mm2 (MPa) according to theequation CS = 4F/ppd2, where F isthe failure load and d the diameterof the specimen.
Acid ErosionFive specimens per group were pre-pared in conditioned 5mm ¥ 30-mm-diameter polymethylmethacrylate (PMMA) disks with ahole (5 ± 0.5mm in diameter ¥ 2 ±0.5-mm deep) in the center. ThePMMA disks were filled with themixed cements and covered withseparating sheets, pressed firmlytogether, and clamped. At 180 sec-onds after the end of mixing, thewhole assembly was transferred tothe cabinet maintained at 37 ± 1°Cand a relative humidity of 95 ± 5%.After 24 hours, the clamps and theseparating sheets were removed,

34
A N T I B A C T E R I A L E F F E C T S O F A C H L O R H E X I D I N E - C O N T A I N I N G G I C
© 2 0 0 8 , C O P Y R I G H T T H E A U T H O R SJ O U R N A L C O M P I L A T I O N © 2 0 0 8 , B L A C K W E L L P U B L I S H I N G
and the specimens were flattenedwet with 1,200-grit abrasive paper.For each specimen, the initial depthat the center of the specimen wasmeasured at five points using theedge of the specimen holder as afixed reference plane. The height atthe center of the specimen was sub-tracted from the average height ofthe specimen holder to obtain theDo value. The specimens wereimmersed horizontally into individ-ual bottles containing 30mL of theeroding solution (0.1mol/L lacticacid/sodium lactate buffer solutionadjusted to pH 2.74 ± 0.02) for 24hours at 37°C. After the immersionperiod, the specimens wereremoved and rinsed with water. Foreach specimen, the depth at the cen-ter was measured again to obtainthe depth of the GICs after erosion(Dt). The eroded depth, D (in mm),at the center of each specimen was calculated using the following equation:
Hardness27
A stainless-steel mold with innerdimensions of 6 ± 0.1-mm heightand 3 ± 0.1-mm diameter was usedfor preparing the six samples pergroup. Within 60 seconds after theend of mixing, the GICs werepacked into the conditioned moldsslightly in excess and covered withstrips. One hour after the end ofmixing, the specimens wereremoved from their molds and
D Dt Do= −
stored at 37 ± 1°C in water prior totesting. After the storage time of 24hours and 10 days, the Vickershardness HV3 was measured byapplying a load of 29.42N on thesamples for 30 seconds. Five indentation measurements werecarried out and averaged for each specimen.
Diametral Tensile Strength28
Six cylindrical specimens (3mm ¥ 6mm) per group were prepared usingsplit metal molds. Within 60 sec-onds after the end of mixing, theGICs were packed into the condi-tioned split molds slightly in excessand covered with strips. All theassembly was then transferred intothe climatic cabinet at 37 ± 1°C and95 ± 5% relative humidity for 1 hour. After that period, the speci-mens were ground with wet 500-grit silicon carbide paper to flattenthe surfaces, removed from theirmolds, and stored at 37 ± 1°C inwater for 24 hours. Prior to testing,the diameter and thickness of eachspecimen was determined using amicrometer gauge. The specimenswere placed on the universal testingmachine (Zwick machine, Z010) sothat the diameter of the specimencoincided with the direction of thecompressive force. The specimenswere then loaded in compression tofail at a crosshead speed of 1mm/min. The maximum forceapplied when the specimens frac-tured was recorded, and the diametral tensile strength was
calculated in N/mm2 (MPa) accord-ing to the equation DTS = 2F/pdt,where F is the failure load, d thediameter, and t the thickness of the specimen.
Biaxial Flexural Strength29
Six shell-like specimens per group(20mm ¥ 1mm) were prepared inTeflon molds. Within 60 secondsafter the end of mixing, the GICswere packed into the ring moldsslightly in excess, covered withstrips, and clamped. All the assem-bly was then transferred into theclimatic cabinet at 37 ± 1°C and 95± 5% relative humidity. After 1hour, the specimens were groundwith wet 500-grit silicon carbidepaper to flatten the surfaces,removed from their molds, andstored at 37 ± 1°C in water for 24hours. Prior to testing, the thicknesswas determined for each specimen,which was then placed horizontallyon the universal testing machine(Zwick machine, Z010). The speci-mens were then loaded with 2N/min at a crosshead speed of 1.5mm/min. The maximum forceapplied when the specimens frac-tured was recorded, and the biaxialflexural strength was calculated inN/mm2 (MPa) according to theequation below:
BiaxFSF
t
dd
d d
d
s
l
s l
= +( ) ⎡⎣⎢
⎤⎦⎥
+⎡⎣⎢
−( ) +⎡
⎣⎢⎢
⎤
⎦⎥⎥
⎤
⎦⎥⎥
3
21
12
2
2 2
2
pn
n
ln

T Ü R K Ü N E T A L
V O L U M E 2 0 , N U M B E R 1 , 2 0 0 8 35
where F is the failure load, ds thesupport ring diameter, t the speci-men’s thickness, dl the loading ringdiameter, d the specimen’s diameter,and n the Poisson’s ratio.
Working Time30
The working time, which is under-stood as the time at which it is pos-sible to manipulate a dental materialwithout an adverse effect on itsproperties, was measured by deter-mining the viscosity over the timeusing a cycloviscosimeter (Cyclo-Viscos-E, Brabender, Duisburg, Ger-many). The material was mixed for30 seconds and then transferred onthe probe head, which was adjustedto 23°C. Exactly 60 seconds fromthe beginning of mixing, the mea-surement was started and the viscos-ity was recorded. Five mixtures pergroup were tested.
Statistical analysis was carried outby one-way analysis of variance(ANOVA) and Dunnet-C test for theimmediate inhibition zones of theagar-diffusion test (day 0). One-wayANOVA, Dunnet-C, and Tukeyposthoc test were carried out for allthe physical properties except hardness. The two-way ANOVAwith Tukey or Dunnet-C test wasused for hardness, and t-test wasused for comparing the differentperiods (p < 0.05).
R E S U L T S
Agar-Diffusion TestFor this test, only the immediateinhibition zones (day 0) against the
strains of the different groups were compared statistically witheach other. The zones were thenchecked for long-term antibacterialactivity at 1, 7, 14, 21, 30, 40, 50, 60, 70, 80, and 90 days (Tables 2 and 3).
“Day 0” results showed no antibac-terial effect of the conventionalChemFil Superior against all thetested strains. For S. mutans, thedifference between all the groupsand the control was significant (p < 0.05). The greatest inhibition
TABLE 2. LONG-TERM INHIBITION ZONES ( IN MILLIMETERS) OF THE TESTED GROUPS AGAINST S. MUTANS (N = 5) .
DaysS. mutans 0 1 7 14 21 30 40 50 60 70 80 90
0.5% diacetate 23 16 14 13 13 13 12 11 10 8 0 025 16 14 14 14 13 12 12 10 8 0 027 17 16 16 15 15 14 12 10 9 0 024 17 16 15 15 14 13 12 10 8 0 026 16 15 14 14 13 12 11 10 9 0 0
1.25% diacetate 26 16 16 15 13 13 12 12 12 12 8 027 17 16 15 14 13 13 13 12 11 9 027 17 16 15 14 13 13 13 12 12 8 027 17 17 16 15 14 14 13 12 11 9 026 17 16 15 15 14 13 12 12 12 9 0
2.5% diacetate 28 16 16 15 14 14 14 13 12 12 11 1028 17 16 15 15 14 14 14 13 13 11 927 17 17 16 14 14 14 14 14 12 10 928 18 17 16 15 15 14 13 12 12 11 928 17 17 16 14 14 14 14 13 13 11 9
0.5% digluconate 20 17 16 14 12 12 10 8 8 7 0 022 18 16 14 13 11 11 9 8 8 0 020 17 17 15 11 11 10 10 8 0 0 022 18 17 15 13 11 11 9 8 0 0 021 17 16 14 13 13 12 11 9 7 0 0
1.25% digluconate 22 20 18 15 14 13 12 11 11 8 0 023 22 19 16 13 13 13 12 10 8 0 022 18 18 15 13 13 12 11 11 8 0 023 19 19 16 13 12 11 10 9 7 0 022 21 18 15 14 13 12 11 10 8 0 0
2.5% digluconate 26 25 22 18 17 14 13 12 11 10 9 025 24 20 19 16 14 12 12 10 9 8 025 24 20 18 16 14 12 12 10 10 8 026 25 22 18 17 14 12 12 10 9 8 027 26 23 19 18 15 13 13 11 10 9 0
“Day 0” means the immediate antibacterial effect, whereas “day 1” means the 24-hour effects.

36
A N T I B A C T E R I A L E F F E C T S O F A C H L O R H E X I D I N E - C O N T A I N I N G G I C
© 2 0 0 8 , C O P Y R I G H T T H E A U T H O R SJ O U R N A L C O M P I L A T I O N © 2 0 0 8 , B L A C K W E L L P U B L I S H I N G
zones were observed in all the diac-etate groups and the 2.5% diglu-conate-added ChemFil Superior(Figure 1A). For L. acidophilus, thedifference between the groups wasalso significant while compared withthe control (p < 0.05). The 2.5%
diacetate-added ChemFil Superiorgroup had the greatest inhibitionzone against L. acidophilus, fol-lowed by the 2.5% digluconate- and1.25% diacetate-added groups (Figure 1B). None of the testedgroups had an effect on C. albicans.
As the control group of ChemFilSuperior had no effect on the testedmicroorganisms after 24 hours, itwas decided not to include thisgroup in the long-term follow-up ofthe antibacterial effect. Figures 2 and3 show the antibacterial effects ofthe effective groups after 1 week.
For S. mutans, the inhibition zones’diameters diminished after “day 1”and stayed effective until the 70thday for the 0.5% groups and the1.25% digluconate group. Thiseffectiveness lasted until the 80thday for the 1.25% diacetate and the2.5% digluconate groups, and upto the 90th day for the 2.5% diac-etate groups (Table 2). For L. aci-dophilus, the inhibition zones’diameters were similar during thefirst week for all the diacetategroups tested. The antibacterialactivity of the 0.5% and 1.25%digluconate groups was effectiveuntil the 40th day, whereas the2.5% digluconate group had someinhibition effects until day 50. Allthe samples of the 2.5% diacetate-added ChemFil Superior group andone of the 1.25% CHX diacetateshowed effective antibacterial activ-ity until the 60th day (Table 3). Itwas observed that the more CHXconcentration added to the GICs,the more the long-lasting antibacte-rial effect against L. acidophilus.
HardnessThe Vickers hardness was checkedafter 24 hours and after a longer
TABLE 3. LONG-TERM INHIBITION ZONES ( IN MILLIMETERS) OF THE TESTED GROUPS AGAINST L. ACIDOPHILUS (N = 5) .
DaysL. acidophilus 0 1 7 14 21 30 40 50 60
0.5% diacetate 24 20 20 14 13 10 10 8 023 22 18 13 12 10 8 8 024 22 19 14 12 9 0 0 023 22 19 14 12 9 8 0 024 23 20 15 13 10 8 8 0
1.25% diacetate 26 24 20 16 14 10 10 8 026 24 22 14 13 11 10 9 825 23 20 14 14 12 11 8 025 23 20 14 13 11 10 8 026 24 22 16 14 12 11 9 0
2.5% diacetate 27 24 22 16 16 14 12 11 828 26 23 18 15 13 12 10 827 24 22 16 15 13 11 10 927 25 22 16 15 13 11 10 928 26 23 17 16 14 12 11 8
0.5% digluconate 22 16 12 9 8 8 8 0 020 15 13 10 9 8 8 0 021 15 13 10 9 8 0 0 022 16 14 11 10 9 8 0 020 15 12 9 9 8 0 0 0
1.25% digluconate 22 17 14 13 9 8 8 0 022 18 15 12 10 9 8 0 023 18 14 12 10 9 8 0 023 18 15 12 10 9 8 0 022 17 14 13 11 10 9 0 0
2.5% digluconate 26 20 16 12 11 10 9 8 026 22 18 14 12 10 8 8 025 21 16 11 10 11 10 0 025 22 18 14 12 10 8 0 026 23 19 15 13 11 9 8 0
“Day 0”‘ means the immediate antibacterial effect, whereas “day 1” means the 24-hour effects.

T Ü R K Ü N E T A L
V O L U M E 2 0 , N U M B E R 1 , 2 0 0 8 37
storing time (10 days) in order toinvestigate if there was a leachingprocess of the CHX, which takesplace mainly at the surface of thespecimens. If CHX was leachedout, this should have a negativeinfluence on the hardness andwould weaken the surface of thespecimens over time. Moreover, if asubstance is leached out of a dentalmaterial (here CHX), it will alwayslead to the weakening of the struc-ture, especially at the surface asthere is a very high mobility of the substance.
The differences between the 0.5 and2.5% digluconate groups and theothers were significant (p < 0.05).At the 24-hour test, the 0.5 and2.5% digluconate-added ChemFilSuperior groups demonstrated sig-nificantly lower hardness than thecontrol GIC (p < 0.05). However, at the 10-day test, all of the testedgroups, except the 2.5% diglu-conate, demonstrated hardnesscomparable to the original ChemFilSuperior group. While comparingthe first hardness value with that atthe 10 days, it can be seen clearlythat the hardness increased signifi-cantly with time for all the diglu-conate groups except the 1.25%group (Figure 4). Furthermore,because we did not see a differencebetween the test groups and thecontrol in the hardness after 10days, we could state that, if anyleaching of CHX took place on thesurfaces of the CHX-added groups,
Antibacterial effect of the tested groups on S.mutans (day 0) A
0
25
26,6
27,8
21
22,4
25,8
0
1,58
0,55
0,451
0,55
0,84
0 5 10 15 20 25 30
ChemFil Sup
0,5% diacetate
1,25% diacetate
2,5% diacetate
0,5% digluconate
1,25% digluconate
2,5% digluconate
Diameter of inhibition zone (mm)Mean
SD
Antibacterial effect of the tested groups on L.acidophillus (day 0)
0
23,6
25,6
27,4
21
22,4
25,6
0
0,55
0,55
0,551
0,55
0,55
0 5 10 15 20 25 30
ChemFil Sup
0,5% diacetate
1,25% diacetate
2,5% diacetate
0,5% digluconate
1,25% digluconate
2,5% digluconate
Diameter of inhibition zone (mm)Mean
SD
e
c, d d
cb
b
a
c
a, b a a
b b
a
B
Figure 1. A, Inhibition zones for S. mutans at baseline (n = 10). B, Inhibition zonesfor L. acidophilus at baseline (n = 10).
0.5% digluconate 0.5% diacetate
2.5% diacetate 1.25% diacetate
1.25% digluconate 2.5% digluconate
Figure 2. Inhibition zones observed for S. mutans after 1 week.

38
A N T I B A C T E R I A L E F F E C T S O F A C H L O R H E X I D I N E - C O N T A I N I N G G I C
© 2 0 0 8 , C O P Y R I G H T T H E A U T H O R SJ O U R N A L C O M P I L A T I O N © 2 0 0 8 , B L A C K W E L L P U B L I S H I N G
original ChemFil Superior glassionomer group (Figure 7).
Working TimeThe working time of all the CHXdigluconate groups and the 2.5%CHX diacetate added ChemFilgroup was longer than the controlmaterial (p < 0.05) (Figure 8).
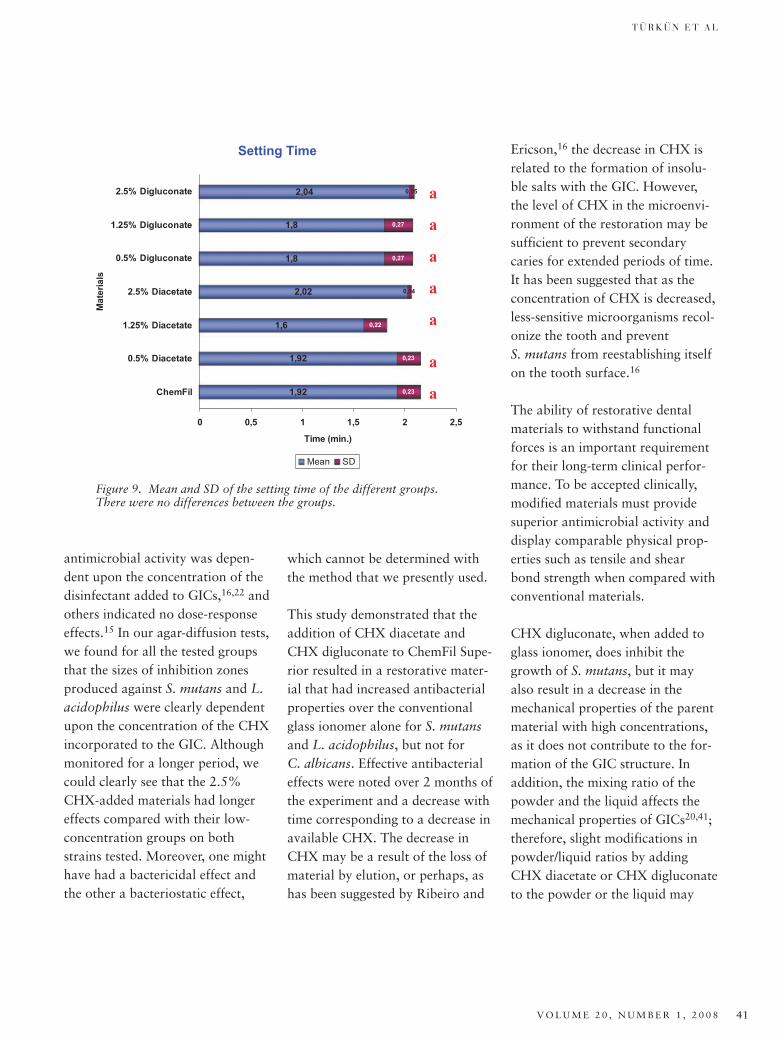
Setting TimeThe setting time of all the experi-mental GICs was not different fromthe original ChemFil Superior material (Figure 9).
Acid Erosion TestThe conventional ChemFil Superiormaterial and all the experimentalgroups had the same acid erosionvalue of 0.17 m.
D I S C U S S I O N
The ability of dental materials toinhibit recurrent caries formation is
0.5% digluconate
2.5% diacetate
1.25% diacetate
0.5% diacetate
1.25% digluconate2.5% digluconate
Figure 3. Inhibition zones observed for L. acidophilus after 1 week.
Vickers Hardness HV3
57,2360,43
50,46
56,21
35,93
58,23
23,55
63,86 63,8 62,7559,7 59,23
63,83
57,46
0
10
20
30
40
50
60
70
ChemFil 0.5%Diacetate
1.25%Diacetate
2.5%Diacetate
0.5%Digluconate
1.25%Digluconate
2.5%Digluconate
Materials
Har
dn
ess
valu
es
24 hours
10 days
SD (24h)
SD (10 days)
a
b
b
aa
aa a
a a a a a b
Figure 4. Mean and SD of the hardness of the different groups.
it was negligible and did not influence the surface hardness ofthe specimens.
Compressive StrengthIn comparison with the controlGIC, 1.25 and 2.5% diacetate-added ChemFil Superior groupshad significantly lower values (p < 0.05), whereas the other groupswere not different (Figure 5).
Diametral Tensile StrengthBoth 2.5% diacetate- and digluconate-added groups tended to have lower tensile values thanthe control GIC, but this differencewas not statistically different (Figure 6).
Biaxial Flexural StrengthAll of the tested groups had biaxialflexural strength comparable to the

T Ü R K Ü N E T A L
V O L U M E 2 0 , N U M B E R 1 , 2 0 0 8 39
suggested that GICs may be antimi-crobial because of fluoride releaseand/or acidity. It has been wellestablished that fluoride is releasedfrom GICs26,32,33 and the materialhas a low pH while setting, but theresults of previous investigationsabout the antibacterial effects ofboth fluoride and low pH are con-troversial.31,32 Furthermore, thereduction in bacterial countsobtained by placing conventionalGICs in cavities is not reliable6,8,17;therefore, antibacterial GICs would provide an alternative approach.
The concept of controlled-releasetherapeutic systems to deliver a pre-determined amount of a drug for aspecific period of time is not new,and the combination of antibacterialagents with restorative materialsand, specifically, CHX has beeninvestigated previously.15,16,21,22 In arecent study, Takahashi and col-leagues17 showed with an HPLC testthat there was very little CHXrelease from their experimental GICformulations and concluded that a1% CHX diacetate addition wasoptimal to give appropriate physicaland antibacterial properties to FujiIX (GC Corporation, Tokyo,Japan). Regarding the previousresults, we selected CHX, which isantibacterial against caries associ-ated bacteria,37 as an antimicrobial,in the form of a powder and a liq-uid, to be incorporated into the con-ventional GIC, ChemFil Superior.
Diametral Tensile Strength
12,89
12,77
11,84
9,69
13,74
15,16
9,4
3,24
2,99
4,16
2,17
3,81
2,75
2,9
0 5 10 15 20
ChemFil
0.5% Diacetate
1.25% Diacetate
2.5% Diacetate
0.5% Digluconate
1.25% Digluconate
2.5% Digluconate
Mat
eria
ls
Tensile Strength (MPa)
Mean SD
a
a a
a a
a
a
Figure 6. Mean and SD of the diametral tensile strength of the different groups. There were no differences between the groups.
Compressive Strength
221,1
213,55
175,12
177,91
219,84
207,59
211,62
14,1
10,85
14,47
17,85
24,31
22,59
18,67
0 50 100 150 200 250 300
ChemFil
0.5% Diacetate
1.25% Diacetate
2.5% Diacetate
0.5% Digluconate
1.25% Digluconate
2.5% Digluconate
Mat
eria
ls
Strength (MPa)
Mean SD
b
b
a
a
a
a a
Figure 5. Mean and SD of the compressive strength of the differentgroups. The different letters indicate statistically different groups.
an important clinical property.GICs have been used for more than30 years, and it is well known thattheir major advantage is theirpotential to inhibit caries31 because
of fluoride release17,32,33 and theirclinical adhesion to dental hard tissues. McComb and Ericson,34
DeSchepper and colleagues,35 andVermeersch and colleagues36

40
A N T I B A C T E R I A L E F F E C T S O F A C H L O R H E X I D I N E - C O N T A I N I N G G I C
© 2 0 0 8 , C O P Y R I G H T T H E A U T H O R SJ O U R N A L C O M P I L A T I O N © 2 0 0 8 , B L A C K W E L L P U B L I S H I N G
Agar plate diffusion was themethod of choice for this studybecause it allowed both set andunset materials to be assayed.38
Moreover, the process is relativelyinexpensive and can be performedrapidly and easily with a large num-ber of specimens. However, thereare also some limitations with thistest method.39 One of the mainconcerns is the inability of themethod to distinguish between bac-teriostatic and bactericidal effects,so the test does not provide anyinformation about the viability ofthe test microorganisms within theinhibition zone. Moreover, the testdoes not simulate the clinical condition where multiple species of bacteria will be growing in complex biofilms.
It was observed that the materialshad significantly more antibacterialeffect while setting than whentested completely set.39,40 Thiscould be partially explained by theeffect that most dental materialsseem to be bactericidal while set-ting, and their low pH during thisperiod may also have an effect.Regarding these findings, we choseto use unset materials to be testedwith the agar diffusion method forthe initial antibacterial effects.
Previous studies using conventionalGICs demonstrated conflictingresults about the antibacterialeffects observed by the addition of CHX; some reported that
Biaxial Flexural Strength
43,06
43,39
47,17
45,46
45,22
39,64
37,13
9,92
9,8
7,35
8,16
10,58
8,72
6,66
0 10 20 30 40 50 60
ChemFil
0.5% Diacetate
1.25% Diacetate
2.5% Diacetate
0.5% Digluconate
1.25% Digluconate
2.5% Digluconate
Mat
eria
ls
Flexural Strength (MPa)
Mean SD
a
a
a
a
a
a
a
Figure 7. Mean and SD of the biaxial flexural strength of the differentgroups. There were no differences between the groups.
Working Time
2,4
2,42
2,46
2,54
2,55
2,64
3,16
0,01
0,02
0,03
0,03
0,01
0,21
0,08
0 0,5 1 1,5 2 2,5 3 3,5
ChemFil
0.5% Diacetate
1.25% Diacetate
2.5% Diacetate
0.5% Digluconate
1.25% Digluconate
2.5% Digluconate
Mat
eria
ls
Time (min.)
Mean SD
b
a
b b
c
c
c
Figure 8. Mean and SD of the working time of the different groups.The different letters indicate statistically different groups.
T Ü R K Ü N E T A L
V O L U M E 2 0 , N U M B E R 1 , 2 0 0 8 41
antimicrobial activity was depen-dent upon the concentration of thedisinfectant added to GICs,16,22 andothers indicated no dose-responseeffects.15 In our agar-diffusion tests,we found for all the tested groupsthat the sizes of inhibition zonesproduced against S. mutans and L.acidophilus were clearly dependentupon the concentration of the CHXincorporated to the GIC. Althoughmonitored for a longer period, wecould clearly see that the 2.5%CHX-added materials had longereffects compared with their low-concentration groups on bothstrains tested. Moreover, one mighthave had a bactericidal effect andthe other a bacteriostatic effect,
which cannot be determined withthe method that we presently used.
This study demonstrated that theaddition of CHX diacetate andCHX digluconate to ChemFil Supe-rior resulted in a restorative mater-ial that had increased antibacterialproperties over the conventionalglass ionomer alone for S. mutansand L. acidophilus, but not for C. albicans. Effective antibacterialeffects were noted over 2 months ofthe experiment and a decrease withtime corresponding to a decrease inavailable CHX. The decrease inCHX may be a result of the loss ofmaterial by elution, or perhaps, ashas been suggested by Ribeiro and
Ericson,16 the decrease in CHX isrelated to the formation of insolu-ble salts with the GIC. However,the level of CHX in the microenvi-ronment of the restoration may besufficient to prevent secondarycaries for extended periods of time.It has been suggested that as theconcentration of CHX is decreased,less-sensitive microorganisms recol-onize the tooth and prevent S. mutans from reestablishing itselfon the tooth surface.16
The ability of restorative dentalmaterials to withstand functionalforces is an important requirementfor their long-term clinical perfor-mance. To be accepted clinically,modified materials must providesuperior antimicrobial activity anddisplay comparable physical prop-erties such as tensile and shearbond strength when compared withconventional materials.
CHX digluconate, when added toglass ionomer, does inhibit thegrowth of S. mutans, but it mayalso result in a decrease in themechanical properties of the parentmaterial with high concentrations,as it does not contribute to the for-mation of the GIC structure. Inaddition, the mixing ratio of thepowder and the liquid affects themechanical properties of GICs20,41;therefore, slight modifications inpowder/liquid ratios by addingCHX diacetate or CHX digluconateto the powder or the liquid may
Setting Time
1,92
1,92
1,6
2,02
1,8
1,8
2,04
0,23
0,23
0,22
0,04
0,27
0,27
0,05
0 0,5 1 1,5 2 2,5
ChemFil
0.5% Diacetate
1.25% Diacetate
2.5% Diacetate
0.5% Digluconate
1.25% Digluconate
2.5% Digluconate
Mat
eria
ls
Time (min.)
Mean SD
a
a
a
a
a
a
a
Figure 9. Mean and SD of the setting time of the different groups.There were no differences between the groups.

42
A N T I B A C T E R I A L E F F E C T S O F A C H L O R H E X I D I N E - C O N T A I N I N G G I C
© 2 0 0 8 , C O P Y R I G H T T H E A U T H O R SJ O U R N A L C O M P I L A T I O N © 2 0 0 8 , B L A C K W E L L P U B L I S H I N G
have also contributed to the influ-ences on mechanical strength and setting times.
The most commonly used strengthvalue to characterize dental cementsis compressive strength.42 However,such materials typically fail in flex-ure rather than in compression, andin recognition of this, there hasbeen some work in recent years tocharacterize them in terms of biax-ial flexure strength.26,43 This testwas originally developed for verybrittle materials such as ceramics,but dental cements, including GICs,have been considered sufficientlybrittle for this test to be applied tothem as well.3 Because of its useful-ness as an indicator of flexuralstrength, and also as a straightfor-ward comparison between similarmaterials, we have used it in thepresent study.
In our study, for both types ofCHX-added materials, the diame-tral tensile strength, biaxial flexuralstrength, acid erosion test, and set-ting time results were similar to theoriginal glass ionomer material.Although the hardness values forthe 0.5 and 2.5% digluconate-added ChemFil Superior groupswere lower than the control at 24hours, at the 10-day values, the dif-ference between the materials wasnot significant, except for the 2.5%digluconate group. Regarding com-pressive strength, high concentra-tions of diacetate additions resultedin lower values.
According to Sanders and col-leagues,22 the decrease in the physi-cal properties of the digluconateform of the CHX is related to thefact that it is a liquid and leachesout more rapidly than the powderor diacetate form of CHX. In ourstudy, besides the 24-hour hardnesstest, we did not observe anydecrease in the physical propertieswhile using the low concentrationof the CHX digluconate additive,whereas the decrease was signifi-cant for the 2.5% group at bothtime periods. Another similar studyperformed with CHX-added FujiIX demonstrated that the incorpo-ration of 1% CHX diacetate wasoptimal to provide antibacterialactivities while not affectingmechanical properties, bondingabilities, or setting time.17
Regarding our results on antibacte-rial properties, we found that bothCHX derivates were effective inpreventing the bacteria from grow-ing. However, the CHX diacetatemight be preferable to use for fur-ther development, as it is a morestable material, not prone todecomposition, and can be easilyblended with glass ionomerpowder.44 The CHX digluconatecannot be isolated in substance andcan only be stable in diluted solu-tions. Furthermore, the stability ofCHX solutions is adversely affectedby exposure to higher temperaturesor light, which may happen duringstorage of glass ionomer liquid.45
On the other hand, the amount of
CHX should be kept as low as pos-sible, as the CHX does not con-tribute to the formation of the glassionomer network, and therefore,high amounts of CHX wouldweaken the scaffold and compro-mise the physical properties of theantibacterial glass ionomer. Accord-ing to all these facts and the resultsof the physical and microbiologicaltests, it would be more appropriateto use 1.25% diacetate additionsfor further development in antibac-terial GICs. Furthermore, bothCHX additives are classified asharmful and rather toxic [LD50(mouse, oral) 2,515mg/kg], and itis preferable to keep the amount ofCHX as low as possible. Furtherstudies to examine the benefits ofthe CHX-added antibacterialChemFil in clinical situationsshould be performed.
C O N C L U S I O N S
1. The incorporation of CHXdigluconate into ChemFil Superior glass ionomer liquid orCHX diacetate into the mater-ial’s powder has the ability toprovide a long-term antimicro-bial effect on S. mutans and L. acidophilus.
2. The new material’s immediatecompressive strength for the1.25 and 2.5% groups waslower, whereas the other physical properties of the material obtained were not compromised seriously.
3. The 2.5% diacetate-addedChemFil Superior was found to

T Ü R K Ü N E T A L
V O L U M E 2 0 , N U M B E R 1 , 2 0 0 8 43
be the most effective and longer-lasting antibacterial groupagainst both tested strains.However, from a chemical pointof view, the 1.25% diacetate-added ChemFil Superior wouldbe a more appropriate materialfor further development.
D I S C L O S U R E A N D
A C K N O W L E D G M E N T
The authors, except for StefanBrugger, who is an employeechemist in the research and devel-opment of Dentsply DeTrey, do nothave any financial interest in thecompanies whose products areincluded in this article.
The authors would like to thankDentsply DeTrey for providing thematerials tested and for letting themwork in their research and develop-ment laboratories free of charge.
R E F E R E N C E S
1. Marthaler TM. Changes in dental caries1953–2003. Caries Res 2004;38:173–81.
2. Frencken JE, Makoni F. A treatmenttechnique for tooth decay in deprivedcommunities. World Health1994;1:15–7.
3. Frencken JE, Holmgren CJ. Atraumaticrestorative treatment (ART) for dentalcaries. 1st ed. Nijmegen (the Nether-lands): STI Books; 1999.
4. Phantumvanit P, Songpaisan Y, Pilot T,Frencken JE. Atraumatic restorativetreatment (ART): a three-year communityfield trial in Thailand -survival of one-surface restorations in the permanentdentition. J Public Health Dent1996;56:141–5.
5. Terashima S, Watanabe M, Kurosaki N,Kano A. Hardness of dentin remainingafter clinical excavation of soft dentin.Jpn J Conserv Dent 1969;11:115–8.
6. Weerheijm KL, de Soet JJ, van Ameron-gen WE, de Graaff J. The effect of glass-ionomer cement on carious dentine: an invivo study. Caries Res 1993;27:417–23.
7. Weerheijm KL, Kreulen CM, de Soet JJ,et al. Bacterial counts in carious dentineunder restorations: 2-year in vivo effects.Caries Res 1999;33:130–4.
8. van Amerongen WE. Dental caries underglass ionomer restorations. J PublicHealth Dent 1996;56:150–4.
9. Frencken JE, Phantumvanit P, Pilot T, et al. Manual for the atraumatic restora-tive treatment approach to control dentalcaries. 3rd ed. Gröningen (the Nether-lands): WHO Collaborating Centre forOral Health Services Research, Universityof Gröningen; 1997.
10. Frencken JE, Pilot T, Songpaisan Y,Phantumvanit P. Atraumatic restorativetreatment (ART): rationale, technique,and development. J Public Health Dent1996;56:135–40.
11. Frencken JE, Van’t Hof MA, vanAmerongen WE, Holmgren CJ. Effective-ness of single-surface ART restorations inthe permanent dentition: a meta-analysis.J Dent Res 2004;83:120–3.
12. Smales RJ, Yip HK. The atraumaticrestorative treatment (ART) approach forthe management of dental caries. Quin-tessence Int 2002;33:427–32.
13. Quan DTH, Nga TT, Mc Intyre J. Fluo-ride release from Fuji IX and other fast-setting GICs. J Dent Res 1995;74:440(IADR absract 317).
14. Imazato S. Antibacterial properties ofresin composites and dentin bonding sys-tems. Dent Mater 2003;19:449–57.
15. Jedrychowski J, Caputo A, Kerper S.Antibacterial and mechanical propertiesof restorative materials combined withchlorhexidines. J Oral Rehabil1983;10:373–81.
16. Ribeiro J, Ericson D. In vitro antibacter-ial effect of chlorhexidine added to glass-ionomer cements. Scand J Dent Res1991;99:533–40.
17. Takahashi Y, Imazato S, Kaneshiro AV,et al. Antibacterial effects and physicalproperties of glass-ionomer cements containing chlorhexidine for the ARTapproach. Dent Mater 2006;22:647–52.
18. Botelho MG. Compressive strength ofglass ionomer cements with dentalantibacterial agents. SADJ 2004;59:51–3.
19. Palmer G, Jones FH, Billington RW,Pearson GJ. Chlorhexidine release froman experimental glass ionomer cement.Biomaterials 2004;25:5423–31.
20. Botelho MG. Inhibitory effects onselected oral bacteria of antibacterialagents incorporated in a glass ionomercement. Caries Res 2003;37:108–14.
21. Imazato S, Torii M, Tsuchitani Y, et al.Incorporation of bacterial inhibitor intoresin composite. J Dent Res1994;73:1437–43.
22. Sanders BJ, Gregory RL, Moore K, AveryDR. Antibacterial and physical propertiesof resin modified glass-ionomers com-bined with chlorhexidine. J Oral Rehabil2002;29:553–8.
23. Akdeniz BG, Koparal E, Sen BH, et al.Prevalence of Candida albicans in oralcavities and root canals. ASDC J DentChild 2002;69:289–92.
24. De Carvalho FG, Silva DS, Hebling J, et al. Presence of mutans streptococci andCandida spp. in dental plaque/dentine ofcarious teeth and early childhood caries.Arch Oral Biol 2006;51:1024–8.
25. Zaremba ML, Stokowska W, Klimiuk A,et al. Microorganisms in root cariouslesions in adults. Adv Med Sci 2006;51:237–40.
26. ISO 9917-1. Dentistry-water basedcements, Part 1: powder/liquid acid-basecements. 1st ed. Geneva, Switzerland:ISO copyright office; 2003.
27. Bayindir YZ, Yildiz M. Surface hardnessproperties of resin-modified glassionomer cements and polyacid-modifiedcomposite resins. J Contemp Dent Pract2004;5:42–9.
28. Xie D, Brantley WA, Culbertson BM,Wang G. Mechanical properties andmicrostructures of glass-ionomercements. Dent Mater 2000;16:129–38.
29. Ban S, Hasegawa J, Anusavice KJ. Effectof loading conditions on bi-axial flexurestrength of dental cements. Dent Mater1992;8:100–4.
30. Fleming GJ, Farooq AA, Barralet JE.Influence of powder/liquid mixing ratioon the performance of a restorative

44
A N T I B A C T E R I A L E F F E C T S O F A C H L O R H E X I D I N E - C O N T A I N I N G G I C
© 2 0 0 8 , C O P Y R I G H T T H E A U T H O R SJ O U R N A L C O M P I L A T I O N © 2 0 0 8 , B L A C K W E L L P U B L I S H I N G
glass-ionomer dental cement. Biomateri-als 2003;24:4173–9.
31. Dunne SM, Goolnik JS, Millar BJ, Seddon RP. Caries inhibiton by a resin-modified and a conventional glass ionomercement, in vitro. J Dent 1996;24:91–4.
32. Miller BH, Komatsu H, Nakajima H,Okabe T. Effect of glass ionomer manip-ulation on early fluoride release. Am JDent 1995;8:182–6.
33. Tam LE, Chan GP, Yim D. In vitro cariesinhibition effects by conventional andresin-modified glass-ionomer restora-tions. Oper Dent 1997;22:4–14.
34. McComb D, Ericson D. Antimicrobialaction of new, proprietary liningcements. J Dent Res 1987;66:1025–8.
35. DeSchepper EJ, White RR, von der LehrW. Antibacterial effect of glass ionomers.Am J Dent 1989;2:51–6.
36. Vermeersch G, Leloup G, Delmée M,Vreven J. Antibacterial activity of glass-ionomer cements, compomers and resin
composites: relationship between acidityand material setting phase. J Oral Rehabil 2005;32:368–74.
37. Emilson CG. Potential efficacy ofchlorhexidine against mutants streptococci and human dental caries. J Dent Res 1994;73:682–91.
38. Herrera M, Castillo A, Baca P, CarrionP. Antibacterial activity of glass-ionomerrestorative cements exposed to cavity-producing microorganisms. Oper Dent1999;24:286–91.
39. Tobias RS. Antibacterial properties ofdental restorative materials: a review. Int Endod J 1988;21:155–60.
40. Coogan MM, Creaven PJ. Antibacterialproperties of eight dental cements. IntEndod J 1993;26:355–61.
41. Billington RW, Williams JA, Pearson GJ.Variation in powder/liquid ratio of arestorative glass-ionomer cement used indental practice. Br Dent J1990;169:164–7.
42. McKenzie MA, Linden RW, NicholsonJW. The physical properties of conven-tional and resin-modified glass-ionomerdental cements stored in saliva, propri-etary acidic beverages, saline and water.Biomaterials 2003;24:4063–9.
43. Ban S, Anusavice KJ. Influence of testmethod on failure stress of brittle materi-als. J Dent Res 1990;69:1791–9.
44. Block SS. Chapter 16. In: Block SS, editor. Disinfection, sterilization andpreservation, 4th ed. Malvern (PA): Leaand Febiger; 1991. p. 274–5.
45. Sigma Aldrich [product informationC6143 C9394].
Reprint requests: Dr. L. Sebnem Türkün,Ege University School of Dentistry, Depart-ment of Restorative Dentistry and Endodon-tics, 35100 Izmir, Turkey. Tel.: +90 232 38803 28; Fax: +90 232 388 03 25; e-mail: [email protected] paper was presented as a poster at the84th General Session of the IADR in Bris-bane, Australia, June 28 to July 1, 2006.