lower back pain management. diagnoses low back pain ddd facet joint syndrome sciatica ...
TRANSCRIPT

Lower Back Lower Back PainPain
ManagementManagement

DiagnosesDiagnoses Low back pain DDD Facet joint syndrome Sciatica Piriformis syndrome Disc herniation Sprain / Strain Muscle spasm

Low Back PainLow Back Pain
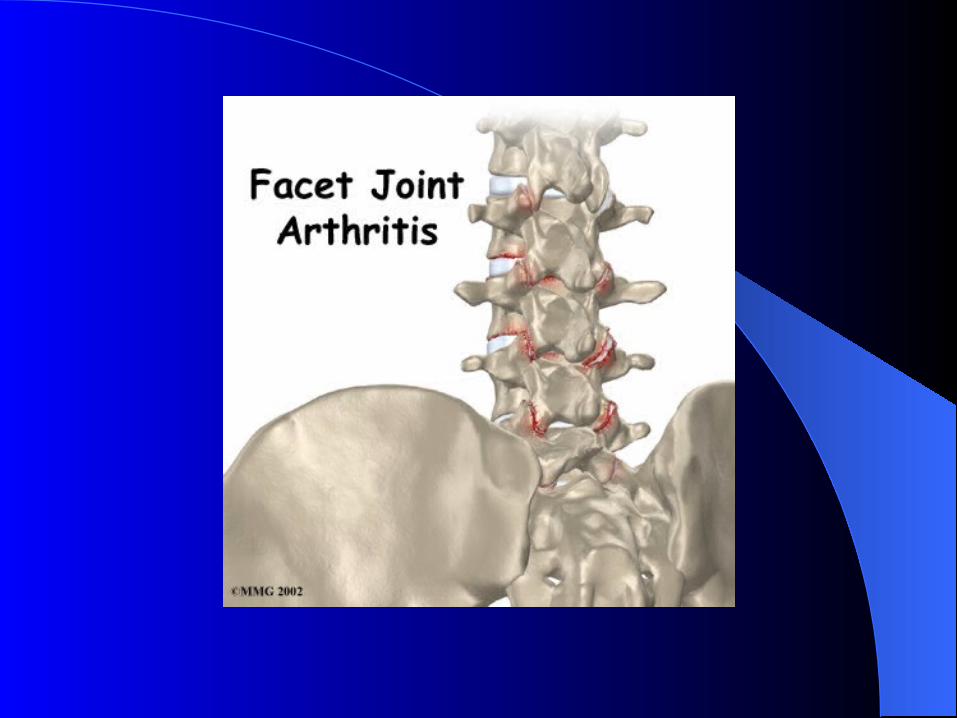
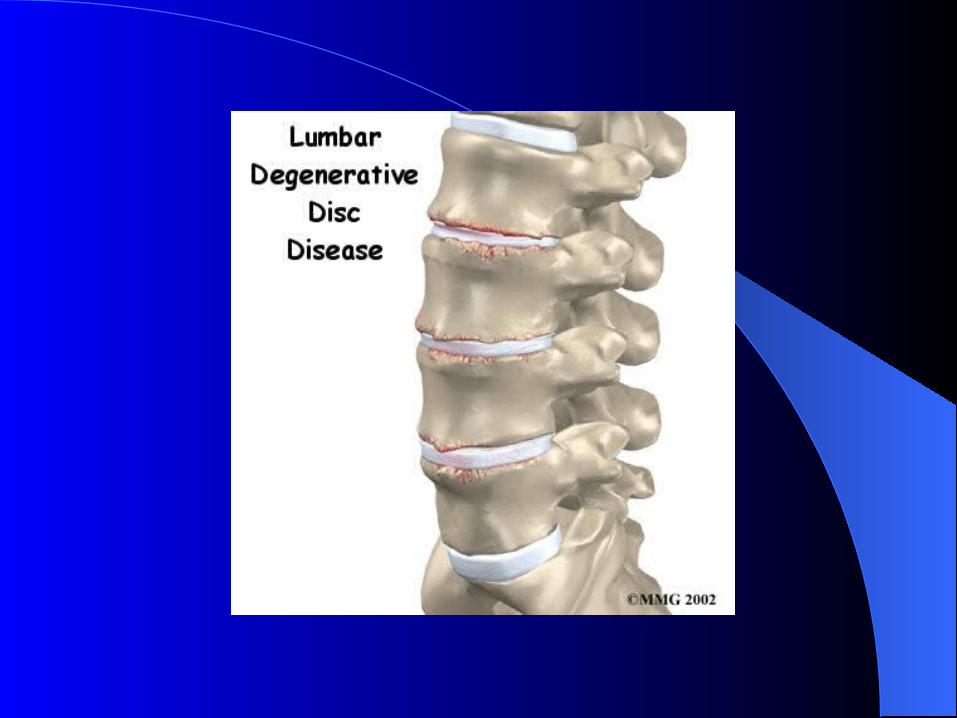
Arthritis/Degenerative Arthritis/Degenerative ChangesChanges
Maintain mobility (ROM) Strengthen +++ Address muscle imbalances Typical radiological finding Symptomatic / Non-symptomatic Anterolisthesis / Posterolisthesis

SciaticaSciatica
Lumbar nerve roots Piriformis Sacro-iliac joint
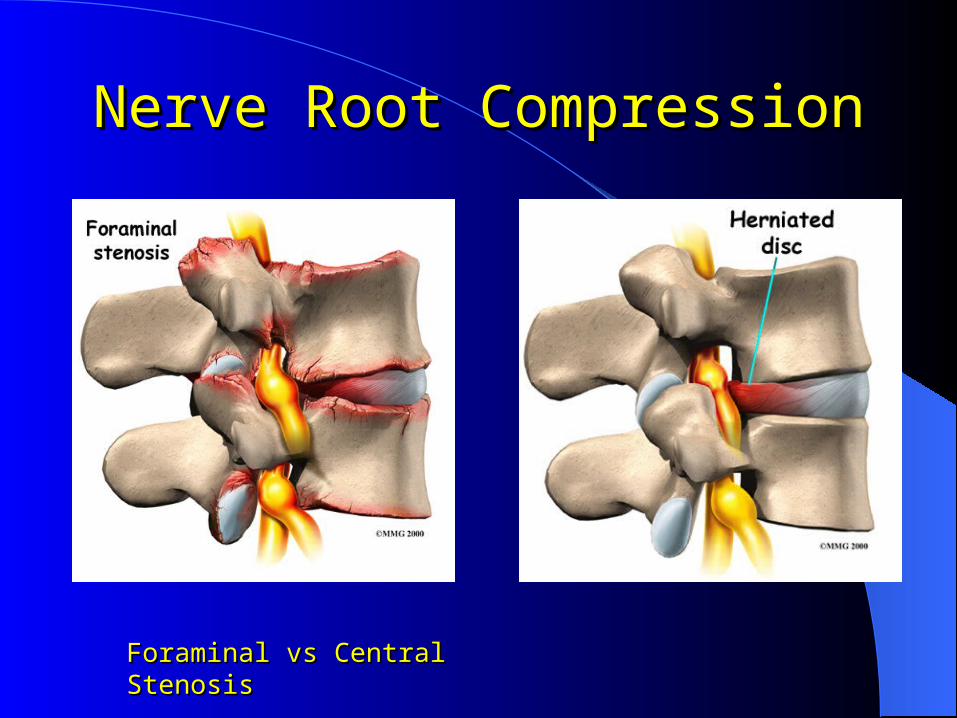
Nerve Root CompressionNerve Root Compression
Foraminal vs Central StenosisForaminal vs Central Stenosis
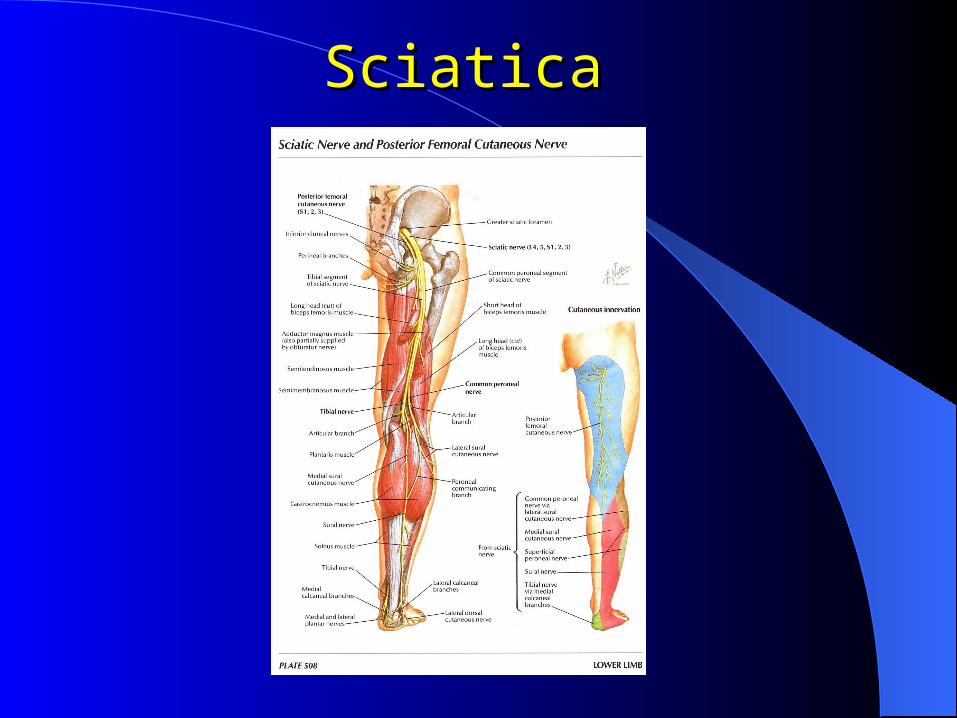
SciaticaSciatica
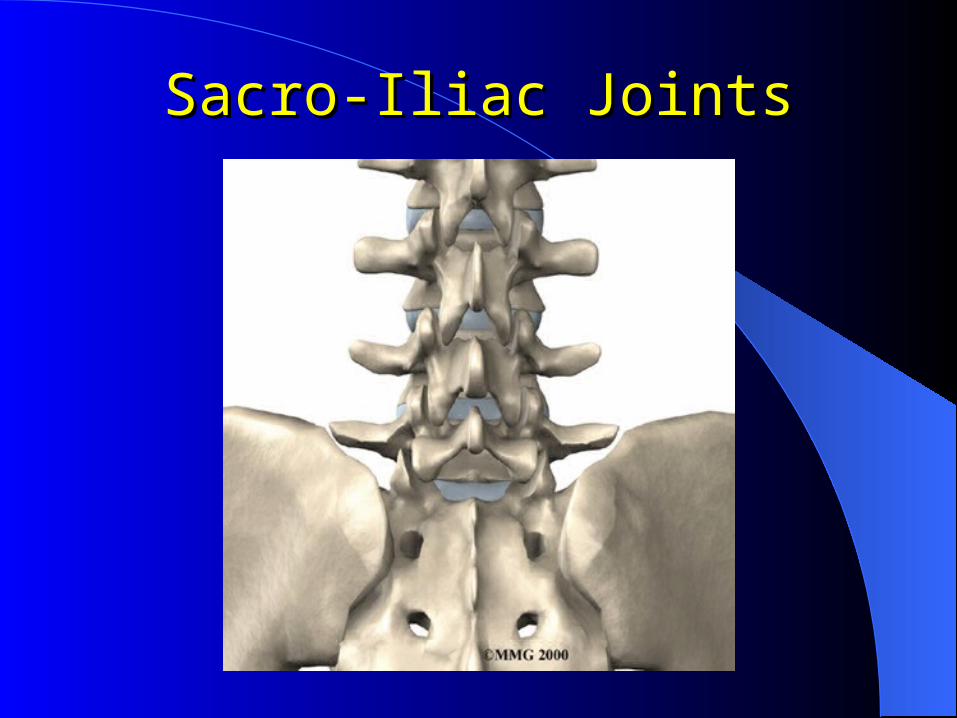
Sacro-Iliac JointsSacro-Iliac Joints
Neurological vs Neurological vs Mechanical OriginsMechanical Origins
Neurological- Pain into the leg
- Pins and needles, burning, numbness in the leg
- Dermatomes/myotomes
- Diminished reflexes
- Lateral shifting, its causes and its relevance
- SLR test

Neurological vs Neurological vs Mechanical OriginsMechanical Origins
Mechanical- Primary area of pain is in the lumbar area
- There may be pain in the buttock or down the leg, almost always above the knee
- Neurological tests are negative

SciaticaSciatica
Maintain / Improve mobility (ROM) Strengthen +++ Address imbalances / stabilize Monitor pain, weakness

Disc HerniationsDisc Herniations

Disc HerniationsDisc Herniations
Avoid constant and repetitive flexion movements
- Crunches
- Bike
- Reading / TV in bed, counter top use
Favor extension
- Strengthen in this position
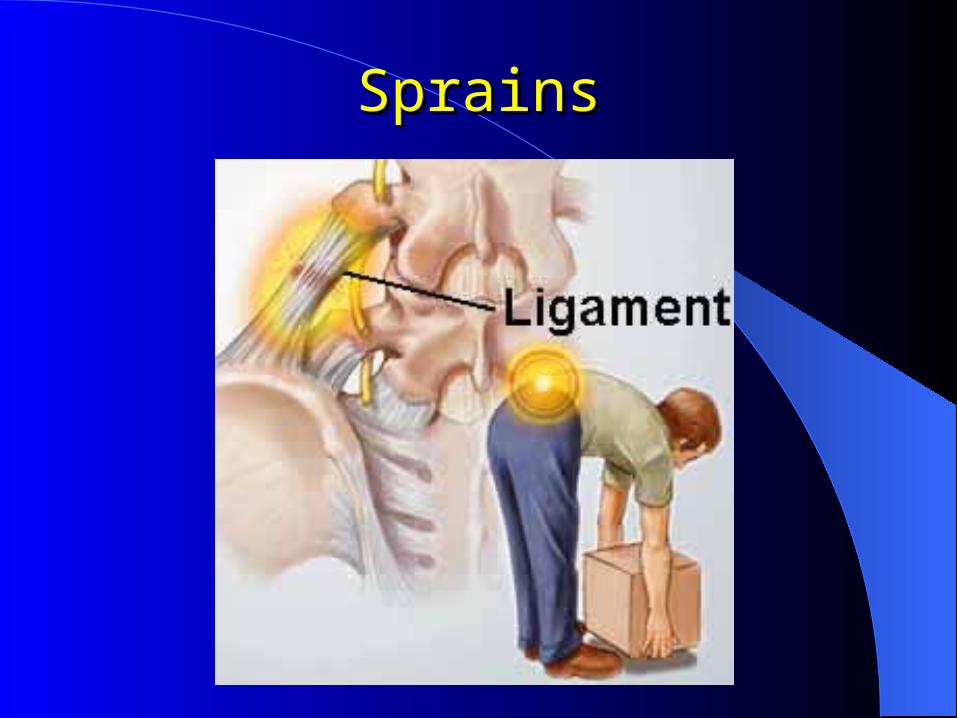
SprainsSprains

SprainsSprains
Rest / remain active Ice
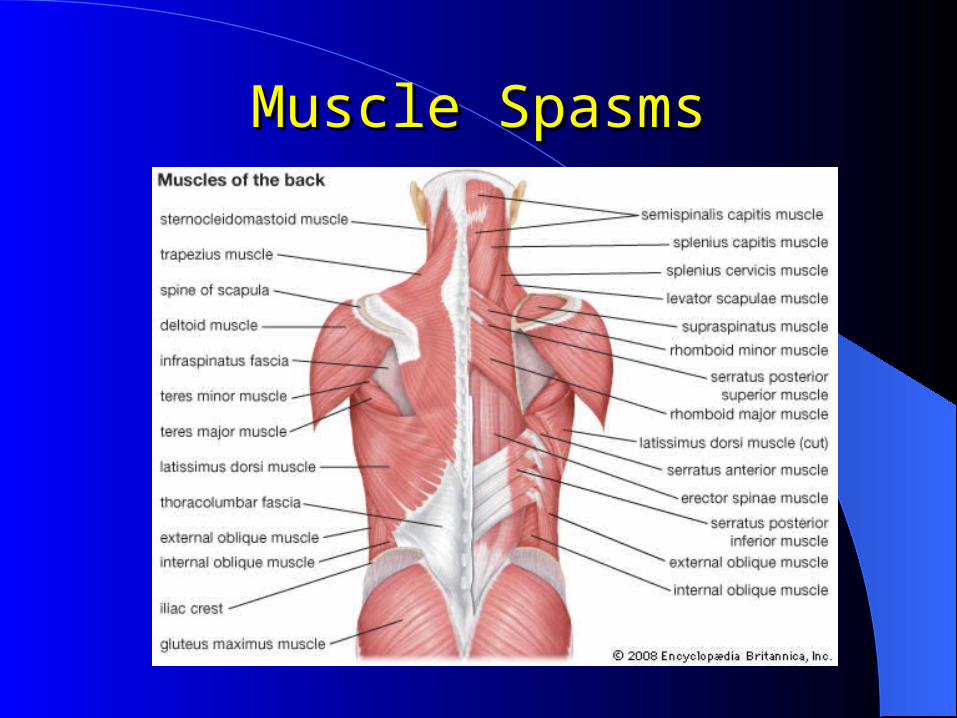
Muscle SpasmsMuscle Spasms

Muscle SpasmsMuscle Spasms
Massage Ice / Heat Light stretching Use of muscle relaxants – When
and Why?
Early Referral to Early Referral to PhysiotherapyPhysiotherapy
Ehrmann-Feldman et al 1996- with early referral, increase chance of return
to work in less than 60 days
Wand et al 2004- increase function, mood, quality of life,
general health
- assess/advise/treat model of care is more beneficial than a assess/advise/wait model for acute lower back pain

Treatment ProtocolTreatment Protocol
pain- treat the cause, not the symptoms
- differentiate the cause of pain
ROM Strengthen / stabilize Educate the patient on dos and don’ts,
ergonomics, lifestyles, sports

Long TermLong Term
Stabilization and Reconditioning exercises
“Core stability” Lifestyle adaptation
(work/sports/leisure) Prevention +++

Our ClienteleOur Clientele
85% Private patients
15%- CSST
- SAAQ
- insurance companies

Multi-disciplinary Multi-disciplinary ApproachApproach
Physiotherapy
Physiotherapy / Occupational Therapy
Rehabilitation- PT
- OT- AT- Osteopathy- Psychology (as needed)

Occupational TherapyOccupational Therapy
Case managers Functional Capacity Evaluations (FCE) Rehabilitation Programs Driving Evaluations PT – OT Splinting Communication +++
CommunicationCommunication
Progress note Avis Motivé

Questions?

Thank youThank you