lower targets for weekly weight gain lead to better results in inpatient treatment of anorexia...
TRANSCRIPT

European Eating Disorders ReviewEur. Eat. Disorders Rev. 12, 164–168 (2004)
Lower Targets for Weekly WeightGain Lead to Better Results inInpatient Treatment of AnorexiaNervosa: A Pilot Study
Thomas Herzog1,2*, Almut Zeeck2, Armin Hartmann2
and Thomas Nickel31Department of Psychosomatics and Psychological Medicine,Christophsbad, Goppingen, Germany2Department of Psychiatry and Psychosomatics, Albert-Ludwigs-University Freiburg, Germany3Max Planck Institute of Psychiatry, Munchen, Germany
Objective: To compare the short-term impact of different targetsfor minimumweekly weight gain (MWWG) in inpatient treatmentfor anorexia nervosa.Method: Comparison of weight gain and its maintenance in 16consecutively admitted anorexic patients with MWWG targeted at750 g and in the subsequent 16 patients with MWWG targeted at500 g.Results: Both groups were characterized by severely ill anorexicpatients who were comparable on most measures. A total of 69and 81per cent, respectively, reached target weight (m¼ 18.3(SD¼ 0.4) kg/m2). During the subsequent 10 weeks under standar-dized inpatient conditions, 12 of 13 achievers in the 500 g per weekgroupmaintained or increased their weight compared to only threeof 11 in the 750 g per week group (p4 0.002).Discussion: Lower rather than higher MWWG targets under aclear symptom focus may be advantageous regarding the short-term symptomatic improvement of anorectic patients. The findingsraise important questions regarding weight gain and its regulationon the biological (e.g. leptin system), psychological and sociallevels. Copyright # 2004 John Wiley & Sons, Ltd and EatingDisorders Association.
Keywords: anorexia nervosa; weight gain; target weight; inpatient psychotherapy; quasi-experimentalstudy
INTRODUCTION
Weight restoration is at the heart of the treatment ofanorexia nervosa. It is usually obtained with the help
of treatment contracts setting targets for minimumweekly weight gain (MWWG) and using operanttechniques. The rapid weight restoration aimed atin most inpatient treatment programmes is usuallyreversed soon after discharge, while the slowerweight gain of outpatients tends to be more stable(Herzog, 2000). The issue of what constitutes theoptimal rate of weight gain is of great clinical (andeconomic) importance but has not been studied in
Copyright # 2004 John Wiley & Sons, Ltd and Eating Disorders Association.
Published online in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/erv.424
* Correspondence to: Dr Thomas Herzog, Klinik fur Psycho-somatik und Psychologische Medizin, Christophsbad Faurn-dauer Str. 6, D 73035 Goppingen, Germany.E-mail: [email protected]
detail. A comparison of consecutive admissioncohorts under two behavioral contracts (MWWG630 vs. 960 g) to an integrated adolescent medicinetreatment programme found higher MWWG asso-ciated with faster weight gain but was seriouslyflawed (exclusion of most anorexic patients, obser-vation restricted to the first 4 weeks of treatment)(Solanto, Jacobson, Heller, Golden, & Hertz, 1994).In our own integrated inpatient treatment pro-gramme for severely ill adult anorexics (Herzog,Zeeck, Nickel, Hartmann, & Falk, 2001) we loweredthe MWWG target from 750 to 500 g under theimpression that many patients were overtaxed bythe higher weight target. In the present paper weexamine how these different MWWG targetsaffected the course and outcome of treatment. Ourhypothesis was that the lower MWWG target wouldslow down the process of weight restoration butwould lead to similar overall weight gain.
METHODS
Inclusion Criteria
All consecutive patients admitted for the first timeunder treatment contract, with an ICD-10 diagnosis
of anorexia nervosa (F50.0) (World Health Organiza-tion, 1992), weight at intake at least 0.5 kg/m2 (BodyMass Index (BMI)) below target weight (see below)and who were not admitted exclusively for diagno-sis or crisis intervention, were included in the study.Thirty-two patients fulfilled these criteria, 16 each inthe high and low MWWG target groups, recruitedover comparable time spans (26 vs. 21 months)(Table 1).
Treatment
The treatment has been described elsewhere (Her-zog et al., 2001). It aimed at the special needs ofthe anorexic patient: weight stabilization at a phy-siological level, normalization of eating behavioursand cognitions, resolving the diverse psychological,familial and/or social problems and conflicts relatedto the illness. Treatment was organized by a contractstipulating its aims and procedures and specifying atarget weight out of the anorectic range as well asMWWG, attendance to therapy components, restafter meals, and leaves of absence contingent uponadherence to the contract. The concept flexiblyallowed for some probationary weeks to gainpatients’ cooperation. At the time of the study theproposed target weight was determined according
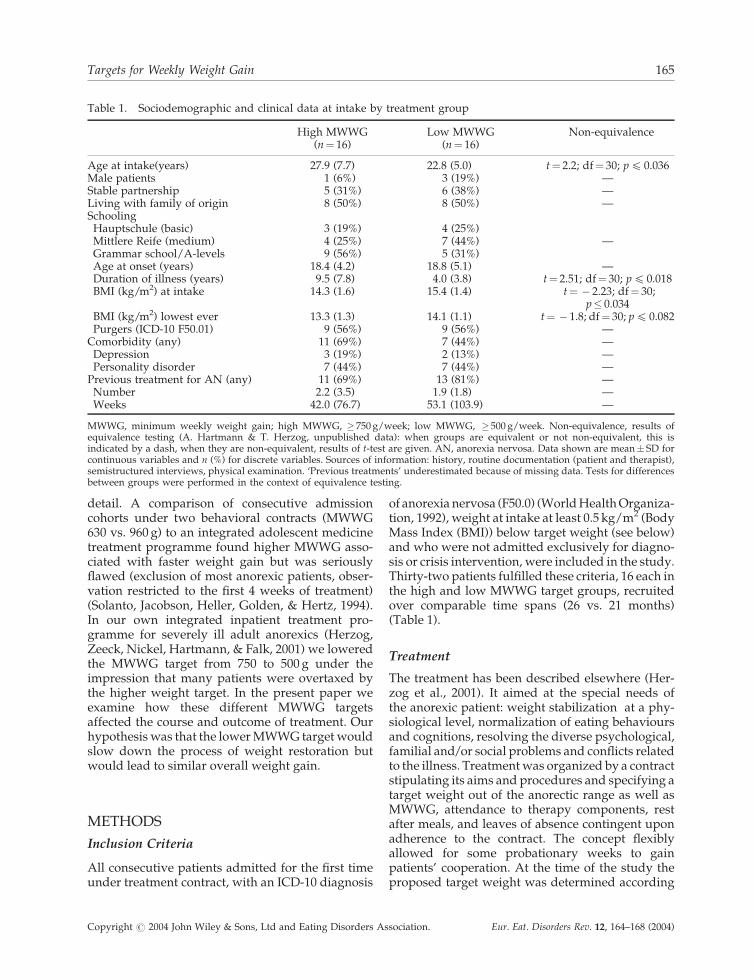
Table 1. Sociodemographic and clinical data at intake by treatment group
High MWWG Low MWWG Non-equivalence(n¼ 16) (n¼ 16)
Age at intake(years) 27.9 (7.7) 22.8 (5.0) t¼ 2.2; df¼ 30; p4 0.036Male patients 1 (6%) 3 (19%) —Stable partnership 5 (31%) 6 (38%) —Living with family of origin 8 (50%) 8 (50%) —Schooling
Hauptschule (basic) 3 (19%) 4 (25%)Mittlere Reife (medium) 4 (25%) 7 (44%) —Grammar school/A-levels 9 (56%) 5 (31%)Age at onset (years) 18.4 (4.2) 18.8 (5.1) —Duration of illness (years) 9.5 (7.8) 4.0 (3.8) t¼ 2.51; df¼ 30; p4 0.018BMI (kg/m2) at intake 14.3 (1.6) 15.4 (1.4) t¼ � 2.23; df¼ 30;
p� 0.034BMI (kg/m2) lowest ever 13.3 (1.3) 14.1 (1.1) t¼ � 1.8; df¼ 30; p4 0.082Purgers (ICD-10 F50.01) 9 (56%) 9 (56%) —
Comorbidity (any) 11 (69%) 7 (44%) —Depression 3 (19%) 2 (13%) —Personality disorder 7 (44%) 7 (44%) —
Previous treatment for AN (any) 11 (69%) 13 (81%) —Number 2.2 (3.5) 1.9 (1.8) —Weeks 42.0 (76.7) 53.1 (103.9) —
MWWG, minimum weekly weight gain; high MWWG, � 750 g/week; low MWWG, � 500 g/week. Non-equivalence, results ofequivalence testing (A. Hartmann & T. Herzog, unpublished data): when groups are equivalent or not non-equivalent, this isindicated by a dash, when they are non-equivalent, results of t-test are given. AN, anorexia nervosa. Data shown are mean� SD forcontinuous variables and n (%) for discrete variables. Sources of information: history, routine documentation (patient and therapist),semistructured interviews, physical examination. ‘Previous treatments’ underestimated because of missing data. Tests for differencesbetween groups were performed in the context of equivalence testing.
Targets for Weekly Weight Gain 165
Copyright # 2004 John Wiley & Sons, Ltd and Eating Disorders Association. Eur. Eat. Disorders Rev. 12, 164–168 (2004)

to Crisp, Norton, Jurczak, Bowyer, and Duncan(1985) taking account both of normative populationdata and the individual weight history. The stan-dard treatment protocol included individual andgroup therapy as well as experiential therapies. Dys-functional thoughts were addressed under both psy-chodynamic and cognitive perspectives inindividual and group sessions. Once target weightwas reached, all operant elements were stoppedand patients were allowed full participation in theregular psychotherapy activities of the ward for atleast another 8 weeks of inpatient treatment. Duringthis time they were encouraged to continue to gainweight and to prepare their post-discharge life.
Data Collection and Assessment
During the 4 years of data collection the nursesin charge, the supervisor and the physicalenvironment remained the same. There was slowrotation of other nurses (five, five FTE (Full TimeEquivalent)), ward physicians (one, five FTE,usually in psychoanalytic training), and other teammembers. There were only minor treatmentchanges. All episodes were assessed prospectively.Patients were weighed twice a week under standar-dized conditions. Extensive physical examinations,laboratory work-up and psychometric testing werecarried out at admission and at discharge.
Statistical Analysis
Statistical analysis was undertaken using SAS.JMP.t-Test and�2-tests were used in the context of testingfor equivalence of groups regarding demographicand anamnestic data (A. Hartmann and T. Herzog,unpublished data). ANOVA and ANCOVA wereused to compare differences in weight gain and toexamine the influence of covariates.
RESULTS
Sociodemographic and clinical characteristics of thepatient group at the time of admission are shown inTable 1. Treatment groups were similar on all para-meters except for greater age at admission, greaterduration of illness and lower BMI in the highMWWG target group. The samples were typicalof severely ill adult anorexic patients, most ofwhom had had substantial treatment before(Herzog, 2000).
The weight gain goal (MWWG target of 750 and500 g, respectively) was realized fairly well bythe achievers in both groups. In the high MWWG
target group four patients who began with a verylow BMI (m¼ 13.4 (SD¼ 0.9) kg/m2) failed toreach the MWWG target by, on average 10 per centeven when the probationary time was taken intoaccount.
Table 2 gives details of the treatment and outcomeby treatment group. Target weight was lower in thehigh MWWG target group. It was reached in com-parable proportions in both groups (‘achievers’).‘Nonclinical’ and ‘normal’ weight ranges werereached more frequently in the low MWWG targetgroup. After target weight had been reached, thecourse of weight gain differed between groups. Inthe high MWWG target group weight at discharge(18.0 (0.93) kg/m2) was below weight after reachingtarget (18.4 (0.51) kg/m2). In the low MWWG targetgroup weight at discharge was higher (18.9(0.26) kg/m2 vs. 18.6 (0.17) kg/m2) (ANOVA forrepeated measurement: time effect: F¼ 0.25; df¼ 1;p4 0.62; interaction treatment group� time:F¼ 10.6; df¼ 1; p 4 0.004). Most achievers in thehigh MWWG target group failed to maintain weightcompared to only one in the low MWWG targetgroup. The duration of the entire treatment, ofthe treatment until target weight was achieved andafter target weight were similar in both groups.Achievers (n¼ 24) were treated significantly longerthan non-achievers (25.9 (8.3) vs. 13.8 (12.3) weeks;t¼ 3.18; df¼ 30; p4 0.004) but without differencesbetween treatment groups (interaction of set-ting� achiever status: F¼ 1.23; df¼ 1; p4 0.28).Weight gain in the low MWWG target group wasnot significantly slower than in the other group.However, there was a trend for the overall rate ofweight gain (achievers and non-achievers) to behigher in the low MWWG target group than in thehigh MWWG target group. Duration of illness,weight and age at intake, and duration of treatment,when controlled for by ANCOVAs, showed nogroup differences.
DISCUSSION
To our knowledge, this is the first study to examinethe impact of different MWWG targets in anorexicpatients over the entire course of inpatient treatmentincluding a post-contract follow-up. Lower MWWGtarget did not significantly slow down the process ofweight restoration. During the 10-week follow-upobservation under standardized inpatient condi-tions, only achievers from the low MWWG targetgroup maintained or increased their weight to a sig-nificant extent.
166 T. Herzog et al.
Copyright # 2004 John Wiley & Sons, Ltd and Eating Disorders Association. Eur. Eat. Disorders Rev. 12, 164–168 (2004)

This finding raises a number of intriguing ques-tions concerning both issues of weight regulationand of clinical practice. The good medium-termresults of outpatient treatments with slow weightgain (Herzog, 2000) indicate that while weight gainshould be focused, it should also be slow enough tobe ‘assimilated’ both physiologically and psycholo-gically. Possibly, leptin-mediated (and other)mechanisms prevent weight gain when it is forcedbeyond a (individual) limit and this may explainthe poor medium-term results of enforced weightrestoration (Licinio, 1997). Taken together with thefindings from our systematic review (Herzog,2000), our results caution against forced weightrestoration even under inpatient conditions. It maybe that the optimal rate of weekly weight gain is inthe region of 500 g.
There are some obvious shortcomings to the pre-sent study. First, patient allocation was not by ran-domization. The comparison of groups ofconsecutive admissions on the same ward has pit-
falls (e.g. changes over time including growingexperience of the treatment team) but allows controlof important treatment factors (therapists, milieu,etc.). We decided against a randomized design,because randomization could not be blind (weeklyweight target is part of the explicit treatment con-tract involving the active and informed participationof the patient) and because we therefore expectedunpreventable group interaction on the wardbetween those assigned to different weight targets.
Second, the samples are rather small and nonequi-valent on some potentially important baseline vari-ables. However, sample size is comparable to mostanorexia treatment studies (Herzog, 2000) and ana-lysis of covariance did not reveal any influence ofthose baseline variables to test the stability of ourfindings we have begun treating our current cohortof anorexics admitted for inpatient treatment againwith the higher MWWG target. This will eventuallyallow us to reexamine our findings based on a muchlarger sample and with some control for possible
Table 2. Data on treatment and outcome by treatment group
High MWWG Low MWWG Difference(n¼ 16) (n¼ 16)
‘Target weight’ 18.1 (0.7) 18.5 (0.1) t¼ � 2.7; df¼ 30; p4 0.011(BMI)
Target weight 11/16 (69%) 13/16 (81%) n.s.achieved
Target weight 3/11 (27%) 12/13 (92%) �2¼ 8.16; df¼ 1; p4 0.002maintained
Weight statusat dischargeWeight (BMI) 17.0 (1.8) 18.5 (1.2) t¼ � 2.8; df¼ 30; p4 0.009Percentile MPMW 4.9 (8.2) 12.8 (8.1) t¼ � 2.76; df¼ 30; p4 0.010‘Non-clinical’(> 15% MPMW) 3/16 (19%) 11/16 (69%) �2¼ 8.54; df¼ 1; p4 0.004‘Normal’ (> 15Percentiles MPMW) 2/16 (13%) 8/16 (50%) �2¼ 5.51; df¼ 1; p4 0.012
Treatment timeTime of entire 23.1 (11.3) 21.2 (9.3) n.s.treatment (weeks)Until target 15.9 (8.9) (n¼ 11) 14.0 (6.9) (n¼ 13) n.s.weight (weeks)After target 10.0 (3.3) (n¼ 11) 10.0 (3.3) (n¼ 13) n.s.weight (weeks)
Weight gain(kg/m2)/week
All 0.07 (0.14) 0.13 (0.06) t¼ � 1.7; df¼ 30; p4 0.099Achievers only 0.11 (0.06) 0.14 (0.05) n.s.
Until target weight* 0.26 (0.10) 0.23 (0.06) n.s.After target weight � 0.06 (0.10) 0.03 (0.03) t¼ � 3.29; df¼ 22; p4 0.003
Dropout (including 4/16 (25%) 4/16 (25%) n.s.discharge by team)
MWWG, minimum weekly weight gain; high MWWG, � 750 g/week; low MWWG, 5 500 g/week. Data shown are mean � SD forcontinuous variables and n (%) for discrete variables. MPMW, Matched population mean weight according to Hebebrand et al. (1996).*Only patients who achieved target weight after at least 6 weeks (9 vs. 11 weeks).
Targets for Weekly Weight Gain 167
Copyright # 2004 John Wiley & Sons, Ltd and Eating Disorders Association. Eur. Eat. Disorders Rev. 12, 164–168 (2004)

changes associated with the passing of time. Mean-while, we think that our findings merit attention andshould encourage clinicians to reexamine their ownprocedures concerning weight gain.
Longer follow-up times are needed to examine thestability of effects and the possible prognostic rele-vance of different courses of inpatient weight gainfor the post-discharge course of the illness. Moreresearch is needed on the successful assimilation ofweight gain on the biological (e.g. the leptin system),psychological and social levels to provide clinicianswith better guidelines to practical questions such as:what is an appropriate target weight and an appro-priate average weekly weight gain?
ACKNOWLEDGEMENTS
We are grateful to our patients and to the treatmentteam: Maria Gross, Ingrid Hetz (head nurses), Kuan-Yu Chen, Florian Hoffmann, Wolfgang Kupsch,Martin Schatzle, Claudia Spahn (ward physicians),Marie Beyer-Paur, Anemone Carl, Gabriele Kuschel(therapists), Dorothee Jager, Beate Kessen-Scymc-zak (social workers), Werner Weidmann (supervi-sor) and Michael Wirsching (medical director).Amal Treacher provided valuable comments on anearlier draft of the paper.
REFERENCES
Crisp, A. H., Norton, K. R., Jurczak, S., Bowyer, C., &Duncan, S. (1985). A treatment approach to anorexianervosa—25 years on. Journal of Psychiatric Research,19, 393–404.
Hebebrand, J., Himmelmann, G. W., Heseker, H., Schafer,H., & Remschmidt, H. (1996). Use of percentiles for thebody mass index in anorexia nervosa: diagnostic,epidemiological, and therapeutic considerations. Inter-national Journal of Eating Disorders, 19, 359–369.
Herzog, T. (2000). Stand der vergleichenden Therapie-forschung bei Anorexia nervosa—Ergebnisse einersystematischen Literaturubersicht (Comparative treat-ment research in anorexia nervosa—results of asystematic review). In M. Gastpar, H. Remschmidt,& W. Senf (Eds.), Forschungsperspektiven bei Essstorun-gen, pp. 127–155. Sternenfels Berlin: Verlag Wis-senschaft und Praxis.
Herzog, T., Zeeck, A., Nickel, T., Hartmann, A., & Falk, C.(2001). Die stationare psychodynamisch orientiertetherapie bei anorexie und bulimie. In G. Reich, & M.Cierpka (Eds.), Psychotherapie der Esstorungen (2nd ed.),pp. 79–93. Stuttgart, New York: Georg Thieme Verlag.
Licinio, J. (1997). Leptin in anorexia nervosa andamenorrhea. Molecular Psychiatry, 2, 267–269.
Solanto, M. V., Jacobson, M. S., Heller, L., Golden, N. H.,& Hertz, S. (1994). Rate of weight gain of inpatientswith anorexia nervosa under two behavioral contracts.Pediatrics, 93, 989–991.
World Health Organization. (1992). The ICD-10 Classifica-tion of Mental Behavioural Disorders: Clinical Descriptionsand Diagnostic Guidelines. Geneva: WHO.
168 T. Herzog et al.
Copyright # 2004 John Wiley & Sons, Ltd and Eating Disorders Association. Eur. Eat. Disorders Rev. 12, 164–168 (2004)