lu6 blueprints 2010-11 new
TRANSCRIPT

8/13/2019 LU6 Blueprints 2010-11 New
http://slidepdf.com/reader/full/lu6-blueprints-2010-11-new 1/33
FCH 251 (LU 6) blueprints
Department of Family and Community Medicine
College of Medicine-Philippine General Hospital – UP Manila
Foreword
The Family and Community Medicine Learning Unit 6 (LU 6) rotation is subdivided into three sub
rotations: a two week Supportive, Palliative and Hospice Care (SHPM) rotation, one week Community
Medicine rotation and one week for the Ambulatory Care unit rotation. Each of which has its own
instructional design which will be presented individually in this report.
Supportive, H ospice and Palliative Medicine (SHPM ) Rotation
Course Description: This is a two week rotation which will focus on clinical practice in the provision of Palliative and HospiceCare to patients and their families in the hospital and home care setting.
Pre-requisites: Must have satisfactorily passed LUC 5
Setting of Learning Experience: SHPM ambulatory clinic (3rd floor OPD bldg), Hospice unit at Cancer Institute, Child-Family Supportive
Care Program at the UP-PGH Cancer Institute and Community Home visits
General Objective: “To provide exposure and training in the care of terminally/chronically ill patients and their families in the
context of primary health care”

8/13/2019 LU6 Blueprints 2010-11 New
http://slidepdf.com/reader/full/lu6-blueprints-2010-11-new 2/33
LEARNING OBJECTIVES CONTENT LEARNING
ACTIVITIES
EVALUATION RESOURCES
Given an actual patient, a student
under supervision is expected to
demonstrate the following
competencies:
Apply the principles of Hospice
and Palliative Care in the
management of chronically andterminally ill patients.
Specific objectives
1. Perform adequate assessmentof terminally ill patients and
their families
Hospice and Palliative Care:
the history and concept
Review of:
Trajectory of illness
Impact of illness
History taking
Health beliefs
Family assessment tools
APGAR
Genogram
SCREEM
Physical examination in the
context of terminal/chronic
illness
Biomedical/BiopsychosocialAssessment
Attend orientation
Random interview with
hospice personnel
Small group discussion
Independent reading
Pre-exposure activities
Bedside demonstration
Actual patient exposure
Rounds with
resident in charge
and fellow in charge
Independent reading
(review of previous
lectures/readings OSI I)
Attendance
Global rating scale for
direct observation
Consultant/Resident
evaluation
Reflection paper
Chart review
Patient feedback
End of rotation
examination
Reference c/o
hospice library ,
venue, schedule,
resource persons,
wards
Lecture notes from
OSI I (family
assessment tools)

8/13/2019 LU6 Blueprints 2010-11 New
http://slidepdf.com/reader/full/lu6-blueprints-2010-11-new 3/33
2. Prioritize and manage
common conditions identified.
Clinical
Pain control
Symptom control
Nutrition
Immobilization
Psychosocial
Caregiver fatigue Depression
Co-dependence
Collusion
Dealing with difficult
patient/relatives
Basic pathophysiology
Basic principles in the
management of chronically
and terminally ill patients
Principles of drug use
Symptom management in
palliative care
Evidenced based medicine
Basic communication skills
Active listening skills
Counseling
Family meeting
Ethics in palliative care
Legal medicine
Direct observation
Bedside demonstration
Actual patient exposure
Independent learning
Demonstration
Clip showingRole-play
Lectures
Bedside rounds
Self and peer evaluation
Patient feedback
Formative evaluation Demo tapes
TV. VHSLCD
Laptop
Facilitator(s)
3. Identify the indications foradmission to:
hospice unit at the cancerinstitute
home visit /home care
Guidelines for admission atthe hospice unit/home visit Orientation
Small group discussion
Independent learning
Formative evaluationusing student’s reflection
paper
Examination
Handouts

8/13/2019 LU6 Blueprints 2010-11 New
http://slidepdf.com/reader/full/lu6-blueprints-2010-11-new 4/33
program Bedside rounds
4. Refer patients to the proper
specialty /services
Referral forms
Indication for referral
Health linkages/networking
with other hospices, Madre de
Amor and Bulacan Hospice
Coordinating/Communicating
with other subspecialty in the
care of patient
Preparation and follow up
of referrals
Home visit to madre de
amor and bulacan hospice
Chart review
Progress notes
Feedback from
Specialties/services
5. Maintain complete, legible
and updated patient records
Data recording
Record keeping
Quality assurance
Update chart entries Chart review
Progress notes
Patient charts
6. Provide instructions prior to
discharge or transfer of patients
Transfer of care
Communication skills
Home instructions
Preparation of clinical
abstract and discharge summaries
Patient and caregiver
Feedback from patient
and caregiver
Direct observation using
checklist or Rating scale
Patient charts

8/13/2019 LU6 Blueprints 2010-11 New
http://slidepdf.com/reader/full/lu6-blueprints-2010-11-new 5/33
Discharge PE
Patient/caregiving
Instruction
Networking
training
Actual patient exposure
Patient charts
7. Perform common
tasks/procedures both foradmitted patients and home care
Basic procedures
IV insertion
Administering oxygen
Administeringcommon medicines:
oral, IM, SC
Nebulization NGT insertion
Foley catheter
insertion
Nutrition planning
Blood extraction
Bedsore/colostomy
/tracheostomy care
Family meetings
Demo and return demo
home visit with hospice
team
Actual patient exposure
Independent learning
Self and peer evaluation
Rating scale
Checklist
Video tapes
Dummies for demo purposes
Skills laboratory

8/13/2019 LU6 Blueprints 2010-11 New
http://slidepdf.com/reader/full/lu6-blueprints-2010-11-new 6/33
8. Communicate effectively with
other hospice team members
Giving and receiving
feedback
Active listening skills
Role-play
Carry out tasks
Small group discussion
Self and peer evaluation
Formative feedback
Direct Observation usingrating scale
Preceptors
Feedback forms
9. Provide end-of-life care and
comfort to terminally ill patientsand their families
End of life care
Active listening skills
Counseling skills
Bereavement care
Medical ethics
Religion and philosophy
Case discussions
Family meetingsBedside rounds
Actual patient exposure
Independent learning
Debriefing
Patient/family feedback
Self and peer evaluation
Student
logbook/diary/Census
Student logbooks
Patient/clientfeedback forms
Conference rooms
Preceptors
List of must knows and nice to know topics: Hospice and Palliative Care principles
Adequate assessment of terminally ill patients

8/13/2019 LU6 Blueprints 2010-11 New
http://slidepdf.com/reader/full/lu6-blueprints-2010-11-new 7/33
Common signs and symptoms seen in terminally ill patients and basic management
Communication (breaking bad news, counseling skills)
Medicines commonly used in hospice (Morphine myths and fallacies)
End of Life care
Medical Ethics
Class schedule/blueprint of activities:
1st week
Monday Tuesday Wednesday Thursday Friday
A.M. A.M. A.M. A.M. A.M.
General Orientation of the
LU6 course
Orientation with fellow of
the month with consultant
Students hour
Palliative Care team
meeting
DFCM Staff conference Palliative Care team
meeting
Case ManagementMeeting (9am – 10:30) SHPM patient care and
tasks (Home visit/Ward
rounds/OPD
Child-Family Supportive
Care Program rotation)
SHPM patient care and
tasks (Ward rounds/OPD)
SHPM patient care and
tasks (Home visit/Ward
rounds/OPD
Child-Family Supportive
Care Program rotation)
P.M. P.M. P.M. P.M. P.M.
Students hour withconsultant
SHPM patient care andtasks (Ward rounds/OPD at CI 108)
Family counseling/psychodynamics
Junior Journal Club(student evidence based presentation)
SHPM patient care and SHPM patient care and SHPM patient care and

8/13/2019 LU6 Blueprints 2010-11 New
http://slidepdf.com/reader/full/lu6-blueprints-2010-11-new 8/33
tasks (Ward rounds/OPD) tasks (/Ward rounds/OPD) tasks (/Ward rounds/OPD)
2nd week
Monday Tuesday Wednesday Thursday Friday
A.M. A.M. A.M. A.M. A.M.
Palliative Care team
meeting
Students hour: Pain and
common symptoms in
hospice lecture (Dr. Ang)
Palliative Care team
meeting
DFCM Staff conference Palliative Care team
meeting
SHPM patient care and
tasks (Home visit/Ward
rounds/OPD
Child-Family Supportive
Care Program rotation
Case Management
Meeting (9am to 10:30)
SHPM patient care and
tasks (Home visit/Ward
rounds/OPD
Child-Family Supportive
Care Program rotation)
SHPM patient care and
tasks (Ward rounds/OPD)
SHPM patient care and
tasks (Home visit/Ward
rounds/OPD
Child-Family Supportive
Care Program rotation) P.M. P.M. P.M. P.M. P.M.
Students hour : End of Life
(Dr. Bausa)
Students hour with
consultant
Students Didactic session
with Senior Resident
Family counseling
/psychodynamics
Junior Journal Club
(student evidence based
presentation)
SHPM patient care andtasks (Ward rounds/OPD)
SHPM patient care andtasks (Ward rounds/OPD)
SHPM patient care andtasks (Ward rounds/OPD
CI 108)
SHPM patient care andtasks (Ward rounds/OPD)
SHPM patient care andtasks (Ward rounds/OPD)
3rd
week
Monday Tuesday Wednesday Thursday Friday
A.M. A.M. A.M. A.M. A.M.Orientation with fellow of
the month and consultant
Students hour with
consultant
Palliative Care team
meeting
DFCM Staff conference Palliative Care team
meeting

8/13/2019 LU6 Blueprints 2010-11 New
http://slidepdf.com/reader/full/lu6-blueprints-2010-11-new 9/33
Palliative Care team
meeting SHPM patient care and
tasks (Home visit/Ward
rounds/OPD
Child-Family SupportiveCare Program rotation)
SHPM patient care and
tasks (Ward rounds/OPD)
SHPM patient care and
tasks (Home visit/Ward
rounds/OPD
Child-Family SupportiveCare Program rotation)
SHPM patient care and
tasks (Home visit/Ward
rounds/OPD
Child-Family Supportive
Care Program rotation)
Case Management
Meeting (9am – 10:30)
P.M. P.M. P.M. P.M. P.M.
SHPM patient care and
tasks (Ward rounds/OPD)
Students hour with
consultant
Students Didactic session
with Junior Resident
Family counseling
/psychodynamics
Junior Journal Club
(student evidence based
presentation)
SHPM patient care and
tasks (Ward rounds/OPD)
SHPM patient care and
tasks (Ward rounds/OPD
at CI 108)
SHPM patient care and
tasks (Ward rounds/OPD)
SHPM patient care and
tasks (Ward rounds/OPD)
4th
week
Monday Tuesday Wednesday Thursday Friday
A.M. A.M. A.M. A.M. A.M.
Palliative Care teammeeting
Students hour Palliative Care teammeeting
DFCM Staff conference Palliative Care teammeeting
Case Conference/Grand
rounds SHPM patient care and
tasks (Home visit/Ward
rounds/OPD
Child-Family SupportiveCare Program rotation)
SHPM patient care and
tasks (Ward rounds/OPD)
SHPM patient care and
tasks (Home visit/Ward
rounds/OPD
Child-Family SupportiveCare Program rotation)
SHPM patient care and
tasks (Home visit/Ward
rounds/OPD
Child-Family SupportiveCare Program rotation)
P.M. P.M. P.M. P.M. P.M.
Students hour with Students hour with Students Didactic session Family counseling Junior Journal Club

8/13/2019 LU6 Blueprints 2010-11 New
http://slidepdf.com/reader/full/lu6-blueprints-2010-11-new 10/33
consultant (Dr. Bausa) consultant with Senior Resident /psychodynamics (student evidence based presentation)
SHPM patient care and
tasks (Ward rounds/OPD)
SHPM patient care and
tasks (Ward rounds/OPD)
SHPM patient care and
tasks (Ward rounds/OPD
at CI 108)
SHPM patient care and
tasks (Ward rounds/OPD)
SHPM patient care and
tasks (Ward rounds/OPD)
Course faculty:
Andrew Ang, MD
Agnes Bausa-Claudio, MD
Manuel Medina, MD
Rachel Rosario, MD
Community M edicine Rotation
Course Description: Community Medicine component of FCH 251; a one-week rotation seeking to provide students
with the opportunity to conduct and learn Community Medicine work with vulnerable sectors and
integrate into the health referral system.
Learning Objectives:
At the end of the 1-week rotation, each Year Level-6 student must be able to:

8/13/2019 LU6 Blueprints 2010-11 New
http://slidepdf.com/reader/full/lu6-blueprints-2010-11-new 11/33
I. Demonstrate clinical capacities as a primary care physicians.
1. Perform history taking and physical examination with patients seeking consult at the local health center, NGO clinic, community /
barangay health posts.2. Formulate a diagnosis and a diagnostic & treatment plan with the patients seeking consult at the communities, local outpatient clinic
and a secondary hospital.
3. Demonstrate skills in patient education: Demonstrate skills & attitude in discussing with a patient and her / his caregiver the patient’sillness and the basis for the diagnostic & therapeutic options.
4. Appropriately refer patients for further treatment to better equipped facilities with better skilled health professionals.
5. Appropriately refer patients and their families to community resources and partners in health care.
II. Demonstrate skills & attitude as a health program manager.
A. Analyze local, national, and global determinants / factors that affect the health of a population group and individual patients.
1. Identify gaps in health care
2. Define vulnerable, marginalized population groups
3. Describe why these groups are vulnerable or/and marginalized.
4. Describe the health status of a specific marginalized population.
5. Analyze the social determinants affecting health of populations.
6. Define globalization and its positive and negative effects on health
B. Describe local, national, global efforts to address health and social issues of a specific marginalized population.
1. Describe elements of health programs and systems management
2. Participate in program implementation and management to address health and health-related needs.
3. Analyze how the intervention/s address/es needs of the identified population group/s
8/13/2019 LU6 Blueprints 2010-11 New
http://slidepdf.com/reader/full/lu6-blueprints-2010-11-new 12/33
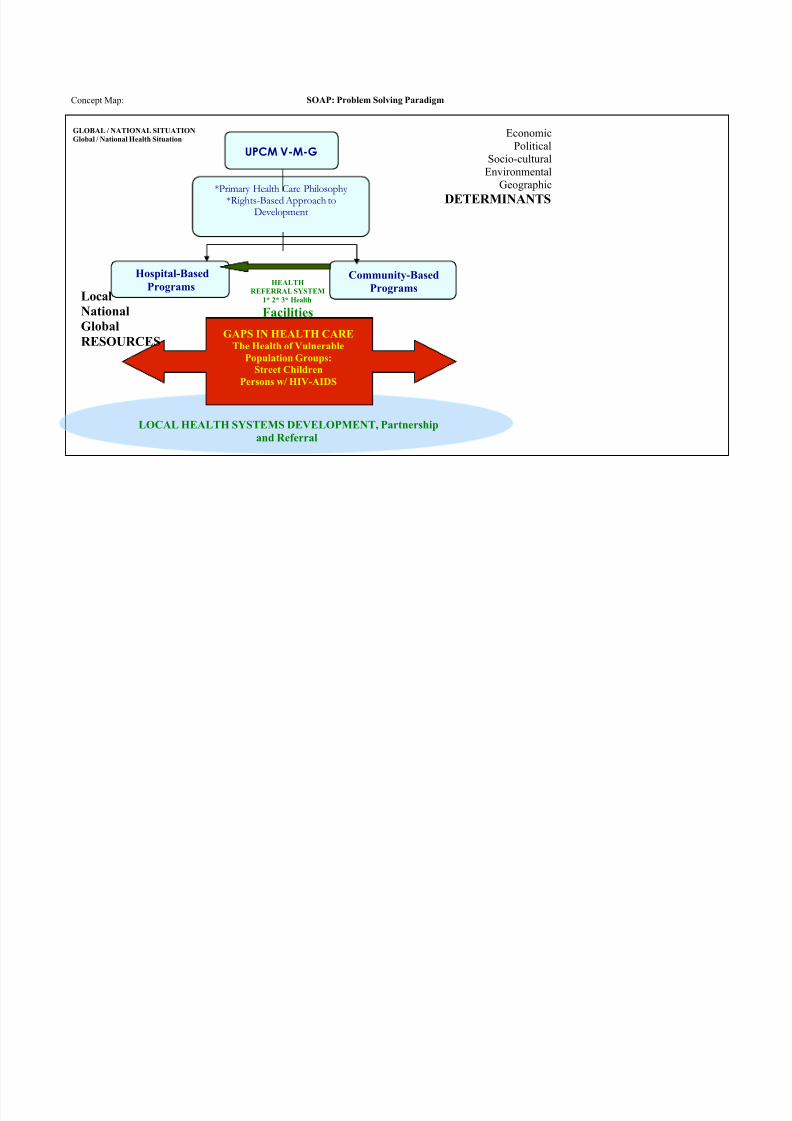
Concept Map: SOAP: Problem Solving Paradigm
GLOBAL / NATIONAL SITUATION
Global / National Health Situation
UPCM V-M-G
Hospital-BasedPrograms Community-BasedPrograms
*Primary Health Care Philosophy*Rights-Based Approach to
Development
LOCAL HEALTH SYSTEMS DEVELOPMENT, Partnership
and Referral
HEALTH
REFERRAL SYSTEM
1* 2* 3* Health Facilities
GAPS IN HEALTH CAREThe Health of Vulnerable
Population Groups:
Street Children
Persons w/ HIV-AIDS
Economic
Political
Socio-cultural
Environmental
Geographic
DETERMINANTS
Local
National
Global
RESOURCES

8/13/2019 LU6 Blueprints 2010-11 New
http://slidepdf.com/reader/full/lu6-blueprints-2010-11-new 13/33
List of must-know and nice to know topics
Session Faculty Topic
1 Portia Marcelo Bridge – review of Community Medicine topics in previous years1. The Philippine Health Care System
2. The Public Sector
3. The Voluntary Sector
Achieving equity in health, the PHCA
2 Edelina DelaPaz,
RPP
Health of Vulnerable Population Groups
Social Determinants of Health, Globalization
3 Alumna/-us Experiences from the Field: Community Medicine as a Career Option
4 * ELEMENTS: Essential/ Basic Health Services / Programs: IMCI {EPI, CARI, CDD, Nutrition}, NTP,
Maternal Health {Antenatal and Post-Partum Care}
*
Portia Marcelo
Edelina Del Paz
Christian Gomez
others
Preceptorials in the Local Health Center, NGO clinic & field sites
1. Clinical case management
2. Clinic management
3. Special Features for emphasis:
1. The Local Health Center
2. Health NGO and Field Sites
5* * Comparative Health Care Delivery Systems and Elements of Health Program / Services Management
ComMed Rotation Evaluation

8/13/2019 LU6 Blueprints 2010-11 New
http://slidepdf.com/reader/full/lu6-blueprints-2010-11-new 14/33
Clinical Clerks Guide to Duties at the Pasay Health Centers
I Introduction
This segment of FCH 251 has the same learning objectives [and evaluation parameters] in a different venue, i.e. a stand-alone public primary care health center. This aims to expose the students to resources and issues related to managing a local primary health facilityand its component public health programs.
II Expected behavior among Clinical Clerks - the bases of your performance evaluation in this rotation.
Courtesy to Health Center Staff and Patients.Introduction to the Health Center Staff: Introduce yourselves to the Doctor-and- Clinic-and Health Programs Manager, and his/her staff [sign in
their logbook]. Get to know the Center Staff, including the BHWs. Observe their assigned duties. Learn about the processes, materials and
activities in running a health center.
Report to Dr. Armand Lee and Ms. Luz Dino {Malibay HC} as well as our DFCM resident physician Dr. __, everyday at 8:00 am.
Take the initiative to set up “your” consultation room – put the room, tables and chairs in order; while totally impossible, try to arrange the
furniture for comfort and privacy. Set up your computer and log into CHITS.
Reminder: Be courteous, every time, every day! Take the initiative to greet all the Health Center staff; you are entering their “home”, their
turf. They do not know you; though they could be busy with the businesses for the day, they expect a greeting with a smile from each of you all
the time. Be respectful to the patients. Observe and immerse into their “lifestyle”; as newcomers, you are EXPECTED to respect their
processes. {There will be another venue for constructive critique.}
Be intellectually prepared. Review
■ Care of well child, pregnant women; health promotion across ages.■ Diagnosis and management of common illnesses among ambulatory patients: IMCI [includes ARI, AGE, EPI, malnutrition, etc
based on WHO-UNICEF protocols]; dermatoses, dyspepsia, hypertension and TB (review the WHO-DOH-NTP/National TB
Program protocol).
■ how to compute for appropriate dosages of common antibiotics and drugs for children

8/13/2019 LU6 Blueprints 2010-11 New
http://slidepdf.com/reader/full/lu6-blueprints-2010-11-new 15/33
■ Your notes on the patient flow in the Health Center, to avoid delays.
■ Your notes on logging into and recording patient transactions in CHITS.
Every morning, check what are the available medicines and preparations in the Health Center pharmacy. Use the list to guide your
choice of drugs and how to compute for correct doses. Remember, prescribing appropriate and available drugs improve patient
adherence to therapy. Be prepared to discuss any of your patients with your resident and/or consultant. Make sure all your patients will be seen by any of
them.
What to bring, what to wear.
ALL THE TIME Bring YOUR OWN basic MD stuff: stethoscope, sphygmomanometer [great if you have a pedia cuff], pen light
[with working batteries], measuring tape, clipboard and pens, neurologic hammer, gloves, calculators and PNDF/ National Drug
Formulary {or MIMS or PDR – commercially available).
ALL THE TIME per pair, Bring YOUR OWN laptop and diagnostic set {ophthalmoscope and otoscope).
Good to have your own set of tongue depressors, they run out fast.
Bring your own personal stuff- water to drink, umbrella to protect you from the rain and sun, candies to stave off hypoglycemia andkeep you smiling.
What to wear: Clean white uniforms and nameplate, closed shoes. Leave unnecessary jewelry and valuables at home. Be
responsible, keep your money / wallet and mobile phones in your pocket at all times.
III Learning Activities
1. Opportunities for Patient Education: 1. Observe the “Pre-con”, pre-consultation lecture [a.k.a. Public Health Lecture in UPCM-PGH parlance], and “Post-con”, post-
consultation discussion to be given by the Center staff. Note also the posters, flyers given to patients and other strategies for patient
education. COMPARE this with how you did these kinds of health education in the past – in LU3, 4, 5 [including your monthly
COME activities teaching the BHWs].2. When assigned in the “Wellness Clinic” - where infant immunization and prenatal care happens, observe the “Post-Con” - how nurses
and midwives iterate the physician's advise (both about medication intake, supportive care, date of follow-up).
2. CHITS – Community Health Information and Tracking System – Data for decision making / Evidence-based decision-making: use

8/13/2019 LU6 Blueprints 2010-11 New
http://slidepdf.com/reader/full/lu6-blueprints-2010-11-new 16/33
electronic medical records for health information management, i.e. data collection, collation, retrieval, analysis and information for
decision-making
3. Observe / learn about how basic health services subsidized by the government are implemented in a typical health center. Note
the following:1. Division of labor among the different types of health professionals2. Health records/ data management via CHITS
3. EPI {Expanded Program for Immunization, including cold chain management}4. Essential drugs provision
5. Maternal health {Pre- and post-natal care, including vaccinations, breastfeeding advice, nutrition monitoring and family planning
counseling}
6. Malnutrition among children
7. Management of common illnesses / injuries
8. TB case management based on the NTP – visit the UPMASA-supported TB-DOTS Clinic
9. others
4. Patient care: Each day, assign 1-2 students
III. To see sick patients,
IV. To assist wellness consults with nurses and midwives {EPI on MW, Prenatal Care on TTh}. Each patient needs to be presented to the
resident and/or consultant BEFORE you discharge them. Make sure you get to experience both sections of the health center.
V. As in the ER-Ambulatory Section, see all patients seeking consult at the Local Health Center. Keep a log of your patients using the
format initially prescribed during your Course Orientation, similar to the one below:
VI. This will be used in the analysis of case mix,
and over all evaluation of clinic management at the
end of your Community Medicine rotation in FCH260. Be prepared to discuss with the consultant on duty any of the cases of patientsyou attended to. [You need not ask the patients to stay behind unless you think they need further evaluation.]
III HOMEWORK : TO BE SUBMITTED ON MONDAY OF after your FCH 251 rotation. Complete the Comparative Health Care
Systems matrix D, using the basic guide questions listed:
Patient’s
NameAge Sex Bgy Chief
ComplaintDiagnosis Disposition

8/13/2019 LU6 Blueprints 2010-11 New
http://slidepdf.com/reader/full/lu6-blueprints-2010-11-new 17/33
What are the common clinical cases seen in the health center? How do they compare with patients in the PGH? In private practice? What are the activities in the health center? PGH? In the clinic of private practitioners? In the NGOs? What resources does the Health Center have? PGH? Clinic of private practitioners? The NGOs?
What is the experience of a patient seeking consult at the health center? PGH? Clinic of private practitioners? In the NGOs?Characterize the relationships among the clinic staff in the local health center? PGH? Clinic of private practitioners? In the NGOs?

8/13/2019 LU6 Blueprints 2010-11 New
http://slidepdf.com/reader/full/lu6-blueprints-2010-11-new 18/33
Clinical Clerks' Guide to Fieldwork with Health NGOs
Street children and the ChildHope Asia Philippines,
I Introduction: Rationale
This session with Childhope Asia Philippines is an opportunity for a personal encounter with street children in their setting. This provides practical experience of the discussions on health of vulnerable groups, enfleshing issues, putting faces to the problem; it is a first-hand
experience in evaluating the health of street children. Childhope Asia is an international non-profit, non-sectarian, non-political organization
whose primary purpose is to advance the cause of street children throughout the world. Rotary Club of Honolulu, a partner, donated a mobile
clinic with state-of-the-art medical equipment; medical supplies are continuously provided by other partners from the private and voluntary
sectors. Childhope Asia Philippines also works with the national (Department of Social Welfare and Development) and local (city) governments
in order to converge efforts towards ultimately getting the children off the streets.
This learning activity with Childhope Asia Philippines has the same learning objectives and methodology as that of your tour of duty at the
ambulatory clinics in PGH of the Department of Family and Community Medicine, i.e. 2B05 at the OPD and the Ambulatory Care Section of the
ER. However, this is held in a different venue – a mobile clinic amidst where street children amass and run primarily by a private volunteer
organization. It aims to hone your clinical skills, and expose you to social determinants that greatly affect the health of the kids. For the target
children, this would be their (perhaps only) chance to receive proper and thorough care. It provides opportunity for you to critique systems in
order to improve them. The formal health care system, in both government and private sectors, has rendered itself socially, financially and
culturally inaccessible because of the issues that beleaguer street children. In the context of service-learning, this is UP's part in contributing its
capacities to improve health systems, uphold children's rights and make it more responsive to the needs of vulnerable sectors.
II Methodology
Report to the site where the Childhope mobile clinic will set up, noting physical arrangements and available medical supplies that you may need
in patient care. A thorough clinical history and physical examination is expected of you, please note them carefully in your notes. Dr. Harvey
Carpio / Dr. Cheryl Magbanua, UPCM'06, and the assigned DFCM resident and/or consultant will supervise your work, and discharge the
patients from your care with finality. You're expected to be on site from 230-5pm.

8/13/2019 LU6 Blueprints 2010-11 New
http://slidepdf.com/reader/full/lu6-blueprints-2010-11-new 19/33
What to bring: (1) basic MD stuff- stet, sphygmomanometer [great if you have a pedia cuff], flashlight, diagnostic set per group, measuring tape,
neurologic hammer, gloves; (2)clipboard and pen; (3) personal stuff- water to drink, umbrella to protect you from the rain and sun, candies to
stave off hypoglycemia and keep you smiling.
What to wear: Be in uniform, with nameplate, closed shoes [when in the Childhope or RAF clinic].

8/13/2019 LU6 Blueprints 2010-11 New
http://slidepdf.com/reader/full/lu6-blueprints-2010-11-new 20/33
Community Medicine Discussion Series #2
Health of Vulnerable Population Groups1
I Objectives: At the end of the session, students should be able to
1. Define vulnerable, marginalized population groups from a health and 'power' perspective.(a) Describe why these groups are vulnerable or/and marginalized.(b)Describe local, national, and global determinants / factors
2. Describe the health status of a specific marginalized population.3. Describe local, national, global efforts to address health and social issues of a specific marginalized population.
(a) Analyze how the intervention/s address/es needs of the identified population group.
4. Reflect and describe concept/s previously discussed that is of personal and professional relevance to the students.
II Guide questions:
a) Describe the vulnerable, marginalized population group. Why are they vulnerable, marginalized?
b) What is the health status of this specific population? Why – what factors affect their health?
c) Describe local, national, global efforts to address health and social issues of a specific marginalized population.
d) Do these efforts rationally address the needs of the population concerned? Do the interventions uphold principles of Primary Health Care?
1 Marcelo,PF and EP delaPaz. July 2005. Health of Vulnerable Population Groups. Revised June 2007

8/13/2019 LU6 Blueprints 2010-11 New
http://slidepdf.com/reader/full/lu6-blueprints-2010-11-new 21/33
Community Medicine Discussion Series #3
Social Determinants of Health, Globalization and Health2
References:
1. WHO Commission of the Social Determinants of Health. March 2005. Action on the Social Determinants of Health: Learning fromExperiences
2. Whitehead, M and G Dahlgren. 2006. Leveling up [part1]: Discussion Paper on Concepts and Principles for Tackling Social Inequities
in Health3. Renewing Primary Health Care in the Americas: Position Paper of the PAHO/WHO. March 2007
4. United Nations Millennium Development Goals: Health Related Goals.2000
5. Werner and Sanders, 2000 Chapters 3 and 4. Questioning the Solution: The Politics of PHC
6. Walsh and Warren, 1979. Selective PHC as an Interim Strategy
2 EPDelaPaz, version3_June2007, Poverty, Social Determinants, Globalization and Health

8/13/2019 LU6 Blueprints 2010-11 New
http://slidepdf.com/reader/full/lu6-blueprints-2010-11-new 22/33
Community Medicine Discussion Series #4:
Experiences from the Field: Community M edicine as a Career Option 3
Objectives: At the end of the session, students should be able to
Describe the work of the Community Medicine practitioner1. Describe features of the area where our guest-alumnus/a practices2. List health and health related issues in the area of work of the Community Medicine practitioner
3. Define how these issues were addressed.1. Analyze the intervention/s using the PHC framework
Describe factors that influenced the career choice/s of our guest-alumnus/a
Reflect and describe concept/s previously discussed that is of personal and professional relevance to the students.
Community Medicine Discussion Series #5:
ELEMENTS: Essential Health Services and Programs: [IMCI, TB, Maternal Health]4 Objectives: At the end of the discussion, students should be able to
1. Analyze and diagnose clinical conditions [i.e. TB, childhood illnesses, care of pregnant women] using the ecological model.
1.1. Analyze and diagnose clinical conditions using the force field theory of analysis.
2. Define solutions to clinical issues using an ecological approach to health.
2.1. Describe national government programs [i.e. TB, childhood illnesses, care of pregnant women] as these are implemented in an
urban local health center.
2.2. Describe private sector involvement in these concerns.
3 Marcelo, PF. July 2005. Experiences from the Field: Community Medicine as a Career Option
4 PFMarcelo. June 2004- structured learning materials prepared for TB-- see SIM on TB Modules 1-5; IMCI and Maternal Health discussed during orientation to Pasay HC
duties; updated June 2005. ELEMENTS: Essential Health Services and Programs

8/13/2019 LU6 Blueprints 2010-11 New
http://slidepdf.com/reader/full/lu6-blueprints-2010-11-new 23/33
Community Medicine Discussion Series #6
Comparative Health Care Delivery Systems and
Elements of Health Program / Services Management5
I IntroductionThis discussion is scheduled towards the end of the students' tours of duty at the PGH Family Medicine Clinic - Ambulatory Care Section/ERand the Pasay local health center, a private practice clinic, clinics and field sites of health NGOs, and the Pasay City General hospital.
II Objectives: At the end of the discussion, students should be able to
1. Describe the public and private health care delivery systems
2. Describe the function and rationale of elements of health care delivery: policies / programs systems, people [patient base, health
providers, managers and policymakers], IEC/ Information-education-communications [opportunities for patient education, medical
records management through CHITS], equipment, supplies and facilities [waiting room, clinics, diagnostic, therapeutic supplies],
financing of services.
3. Describe and contrast elements of health care delivery
3.1. in different primary care settings: PGH Family Medicine Clinic - Ambulatory Care Section/ER, the Pasay local health center, a
private family practice clinic, field sites of health NGOs
3.2. in a primary care setting and a public tertiary, teaching hospital
4. Reflect and describe concept/s previously discussed that is of personal and professional relevance to the students.

8/13/2019 LU6 Blueprints 2010-11 New
http://slidepdf.com/reader/full/lu6-blueprints-2010-11-new 24/33
Course Faculty:
Portia Marcelo, MD, MPH (Course Segment Coordinator)
Edelina dela Paz, MDChristian Gomez, MD
Ramon P. Paterno, MD MPH

8/13/2019 LU6 Blueprints 2010-11 New
http://slidepdf.com/reader/full/lu6-blueprints-2010-11-new 25/33
Ambulatory Care Uni t rotation
Course description: This is a 1-week clinical rotation in the Ambulatory Care Unit within the area of the PGH
Department of Emergency Medical Services.
The rotation in the Ambulatory care unit (AMBU) setting covers primarily non-trauma adult
and pediatric ambulatory cases usually triaged as “non-emergency/urgent cases”. Students will
be trained in the context of fi rst-contact care physicians dealing with the more common clinical
conditions found in the general population, delivering basic services and performing simple
interventions usually performed by generalist physicians in an ambulatory setting.
Patients in this area may present with acute medical problems that may be of new onset,
exacerbations of chronic conditions, with either protean manifestations or frank symptoms
pointing to specific organs that may eventually need specialist referral.
In between duty days, students will have opportunities to joi n staff conferences and casepresentations , do independent readings , refl ect on the possible areas of futu re professional
practice and deal wi th personal issues in the context of work-l if e balance.
Pre-requisites: Students must have successfully passed all the requirements of LU5. They are also expected to
know and apply the principles of Family Medicine, the biopsychosocial approach, pharmacology of
medications used in the ambulatory care section, common morbidities seen in the emergency room
(with special note of the Ambu statistics).
Description of training area: The DEMS-Ambu section takes care of adult and pediatric patients initially triaged by the DEMS to
be non-emergency. As such, the cases seen may be considered as urgent or non-emergent. While the
section deals primarily with non-trauma patients, patients needing outpatient procedures (such astetanus prophylaxis) may also be sent to this area.
Required number of duties/student: 5 duties (total of 40 hours)

8/13/2019 LU6 Blueprints 2010-11 New
http://slidepdf.com/reader/full/lu6-blueprints-2010-11-new 26/33
General objective: To provide the LU6 student with the appropriate clinical exposure as first-contact care physician managing
the most commonly encountered acute cases encountered in family practice / generalist setting.
Learning Objectives Content Activities Resources AssessmentGiven actual patients in the
DEMS Ambulatory Care Unit,
an LU6 student should :
1. Conduct primary surveyGeneral assessment:vital signs Patient identification Ambulatory care unit Performance evaluation
of patients with potentially Principles of triaging Taking vital signs Actual patients (adult (to be filled by supervising
life-threatening condition Brief history and pediatric) resident/consultant)
2. Elicit a complete history
History-taking:
Pediatric and History-taking PGH patient records Report of Activities
adult history
(biopsychosocial
Recording PE
findings
history/psychiatrichistory) as indicated Reflection paper /
Feedback form
8/13/2019 LU6 Blueprints 2010-11 New
http://slidepdf.com/reader/full/lu6-blueprints-2010-11-new 27/33
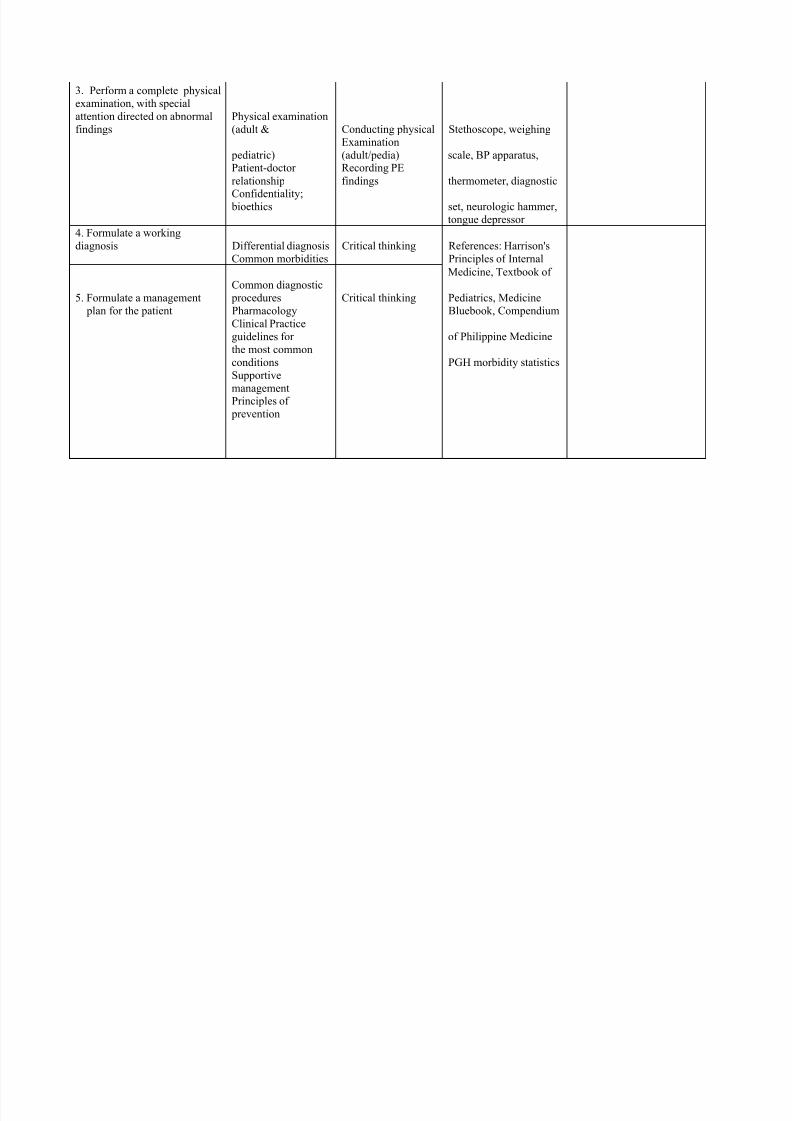
3. Perform a complete physical
examination, with special
attention directed on abnormal
findings
Physical examination
(adult & Conducting physical Stethoscope, weighing
pediatric)Examination(adult/pedia) scale, BP apparatus,
Patient-doctor
relationship
Recording PE
findings thermometer, diagnosticConfidentiality;
bioethics set, neurologic hammer,
tongue depressor
4. Formulate a working
diagnosis Differential diagnosis Critical thinking References: Harrison's
Common morbidities Principles of Internal
Medicine, Textbook of
5. Formulate a management
Common diagnostic
procedures Critical thinking Pediatrics, Medicine
plan for the patient Pharmacology Bluebook, Compendium
Clinical Practice
guidelines for of Philippine Medicine
the most common
conditions PGH morbidity statistics
Supportive
managementPrinciples of
prevention

8/13/2019 LU6 Blueprints 2010-11 New
http://slidepdf.com/reader/full/lu6-blueprints-2010-11-new 28/33
6. Perform simple procedures
usually done in a generalist
setting
Common procedures:
Blood
Obtaining, handling
and transporting
Syringes, gloves,
alcohol,
extraction,
nebulization, intra- specimens, while cotton balls, tourniquet,muscular/intravenousinjections; observing universal KY gel, neb set,
NGT. Foleycatheterization Precautions plaster, gauze
Principles of
universal pre-
Cautions
7. Correctly interpret basic
CBC, basic radiology,
blood chemistries,
EKG
interpreting and
correlating lab tests
laboratory tests
8. Refer appropriatelyManagementguidelines Writing referrals PGH referral forms

8/13/2019 LU6 Blueprints 2010-11 New
http://slidepdf.com/reader/full/lu6-blueprints-2010-11-new 29/33
9. Provide patient and family
Basic
pathophysiology Bedside education Educational materials
education about the illness Basic pedagogy Printed visuals/prompts
Preventive strategies
Basic counselingskills: CEA,
motivational
counseling
10. Address relevant biopsychosocial
Biopsychosocialapproach Bedside education Family medicine lecture
issues that may affect
Family assessment
tools Counseling notes
Adherence
11. Identify community
PGH-community
referral system
Providing referrals
that Listing of health centers,
resources and linkages that DOH programs
include history,
reason hotlines
patients and families may
Philhealth / health
insurance for referral Hospital directory
utilize for the management of
the illness PCSO, NGO

8/13/2019 LU6 Blueprints 2010-11 New
http://slidepdf.com/reader/full/lu6-blueprints-2010-11-new 30/33
12. Demonstrate the
Principles of adult
learning
Perform critical
appraisal Computer with internet Reflection paper
attributes of an ADULT
Evidence-based
medicine of relevant literature access Learner portfolio (report of
LEARNERCommunication andcritical
Participation ingroup Appraisal guides activities, etc)
thinking skills Discussions
13. Demonstrate the desired
Communication
skills
Patient-doctor
consultation Books, hand-outs Performance evaluation
characteristics of aValues and professional ethics Consultant and resident Patient feedback
health professional and Health economics
Readings and
reflection as role models Report of activities
Decent human being Work-life balance
Small group
discussions
Self-careInterpersonalcommunication
Spirituality, EQ. AQ
Giving and receiving
feedback
Organization and
management

8/13/2019 LU6 Blueprints 2010-11 New
http://slidepdf.com/reader/full/lu6-blueprints-2010-11-new 31/33
List of must-know and nice to know topics:
“The Case for a New Philippine Health Referral System”. UP Manila Bagumbayan.
“Real-life drama in the emergency room”. The Philippine Star. July 11, 2000.
“An Evidence-Based Update on NSAIDs”. CM & R. March 2007
“Emergency medical care in developing countries: is it worthwhile?” Bulletin of the WHO, 2002.
“The Occupational Hazards of Emergency Physicians”. Bulletin of the WHO.2002.
“Underestimation of Case Severity by Emergency Department Patients” Implications for Managed Care”. American journal of
Emergency Medicine. May 2000.
“The Short-stay Emergency Observation Ward is Here to Stay”. American Journal of Emergency Medicine. September 2000.

8/13/2019 LU6 Blueprints 2010-11 New
http://slidepdf.com/reader/full/lu6-blueprints-2010-11-new 32/33
Class schedule/blueprint of activities:
A. Ambu duties
Schedule Day 1 Day 2 Day 3 Day 4 Day 5 Day 6 Day 76:00 AM-2:00 PM Orientation 3 2 1 4 3 2
2:00 PM-10:00
PM 1 4 3 2 1 4 3
10:00 PM-6:00
PM 2 1 4 3 2 1 4
Day 8 Day 9 Day 10 Day 11 Day 12 Day 13 Day 14
6:00 AM-2:00 PM 5 8 7 6 5 8 7
2:00 PM-10:00
PM 6 5 8 7 6 5 8
10:00 PM-6:00PM 7 6 5 8 7 6 Off
*Duty
hrs/student: 40 hours
B. Weekday Department Conferences:
7:00 AM -8:00 AM Endorsement conferences (with residents and Interns)
*EBM conference - every Thursday
8:00 AM -9:00 AM Conferences for special topics (TBA)*Department Staff Conference – Thursday (starting 8:00 AM)
1:00 PM -2:00 PM Conferences for special topics (TBA)

8/13/2019 LU6 Blueprints 2010-11 New
http://slidepdf.com/reader/full/lu6-blueprints-2010-11-new 33/33
C. Special conferences
UPCM (TBA) Tuesday 8:00-10:00
Pharmacology modules (TBA)
List of Faculty member/s for Ambulatory care rotation: MARIA CONSUELO BALITA-PUMANES, MD, MHPEd ( Course SegmentCoordinator)
Prepared by: Andrew E. Ang, MD, FPAFP
LU6 Department of Family and Community
Medicine Coordinator